
Abstract
BACKGROUND
Cognitive and environmental parameters are among the most important influencing factors in the prevalence of WRMSDs, which have been studied less compared to physical ergonomic in automobile industry.
OBJECTIVE
This study was conducted with the aim of investigating the relationship between environmental and cognitive ergonomics with the prevalence of WRMSDs in an automotive industry.
METHODS
This study was conducted in 2023 in an automobile company. The sample size was 740 workers. The prevalence of WRMSDs was assessed using the Cornell Musculoskeletal Discomfort Questionnaire. Occupational stress, mental workload, sleep quality, and cognitive failure were assessed by Job Content Questionnaire, NASA-TLX Questionnaire, Pittsburgh Sleep Quality Index, and Cognitive Failure Questionnaire, respectively. Noise were measured by KIMO-DB300 sound analyzer. The intensity of lighting was measured using a Hanger Screen Master illuminance meter. Heat stress was measured by Wet Bulb Globe Temperature (WBGT).
RESULTS
72.58% reported the musculoskeletal disorders in at least one of their body parts during the past 12 months. The average values of occupational stress, mental workload, sleep quality, and cognitive failure among workers with WRMSDs were higher than the participants without WRMSDs (p-value < 0.05). There was a significant difference between the values of all studied physical harmful factors between the two investigated groups, except thermal stress (p-value < 0.05).
CONCLUSION
Findings from this study highlight the critical need for a holistic approach that considers both the external work environment and internal cognitive processes to effectively prevent and manage WRMSDs among automobile industry workers.
Introduction
Ergonomics is the modification and optimization of the environment, tools, equipment and machines from two physical and cognitive dimensions in order to improve the level of physical, mental and social health and well-being through the interaction of people with each other and other components of the system or environment. In general, any incompatibility of the job requirements and the physical and mental ability of the worker with the assigned job duties can lead to the creation of inappropriate and non-ergonomic conditions, and this causes human error, accidents, injuries, and ultimately a decrease in productivity and effectiveness [1, 2].
In general, four main areas of ergonomics including physical (micro ergonomics), environmental, cognitive and organizational (macro ergonomics) have been proposed by the International Ergonomics Association (IEA). Physical ergonomics is mainly related to concepts such as anatomy, anthropometry, work physiology, improper posture, workstation analysis and occupational biomechanics. Environmental ergonomics mainly includes the impact of physical harmful factors of the work environment such as noise and vibration, lighting and thermal stress on human performance and the application of this information in the design and redesign of the human activity environment. Cognitive or perceptual ergonomics is related to thought processes such as perception, memory, stress, mental workload and body reaction to these stressors. The scope of study and performance of this field is from of the stages of understanding to action, which is called cognition. Finally, organizational ergonomics is also related to the optimization of technical-organizational systems such as structures, policies and processes, which somehow can involve all the people of the organization at all levels in accordance with their job duties with ergonomic issues, and lead the organization to study ergonomic goals and improve organizational productivity [3–5].
One of the most important complications caused by non-observance of ergonomic principles in the workplace is the increase in the prevalence of work-related musculoskeletal disorders (WRMSDs) in various workplaces [6]. WRMSDs may arise as a result of long-term exposure to the factors that cause them and during a long process, or they may arise suddenly due to a large impact on a part of the musculoskeletal system. These injuries are often multi-factorial phenomena [7]. WRMSDs begin with fatigue and pain and progress to the disease in which the range of motion of the organs is limited or the strength and power of the muscles are reduced. Studies conducted in England have shown that 55% of the occupational diseases caused in this country were related to musculoskeletal disorders [4]. In Iran, musculoskeletal disorders are the main source of disability and related costs. Based on the available statistics, nearly 48% of work-related illnesses are accumulated injuries that are caused by physical or mechanical factors and are considered a form of WRMSDs [5, 8, 9]. The consequences of WRMSD can affect individuals and society and lead to a large financial burden. In Europe, absenteeism has been reported in more than 50% of workers with WRMSDs, which is significantly higher than in workers infected with influenza virus (10–12%). In addition, WRMSDs are responsible for permanent disability in 60% of all reported cases. Statistics show that the financial costs of WRMSDs in Europe are estimated at 240 billion euros, which is 2% of the EU-15 GDP [9].
There are many risk factors in each of the four components of ergonomics that can lead to the increase of the prevalence of WRMSDs. One of the important dimensions of ergonomics, which has been studied and evaluated so far, is physical ergonomics. Previous studies have made it clear that one-dimensional evaluations in the field of ergonomics (physical ergonomics) are not effective and conducting effective studies in this field requires comprehensive attention to all aspects of ergonomics (physical, environmental, cognitive, and organizational). Cognitive risk factors and physical harmful factors in the work environment are among the most important risk factors in the prevalence of WRMSDs [4, 10–12].
Cognitive concepts such as oral workload, occupational stress, burnout, sleep quality, etc. are among the most important risk factors affecting the prevalence of WRMSDs in the workplace. In working environments, if the physical and mental capabilities of people are not in accordance with their job needs, it can have various negative consequences such as increasing dissatisfaction and absenteeism, creating stress, reducing physical ability, fatigue and reducing job efficiency. Among these, one of the most important negative consequences is the increase in the prevalence of WRMSDs. One of the effective cognitive factors in occupational injuries such as WRMSDs is the disproportion between the mental workload imposed on workers and their abilities and limitations [13–15]. In these situations, people work in non-ergonomic and unsafe conditions, and their mental and psychological balance is disrupted, leading to ergonomic disorders and also various types of occupational accidents [1, 16]. Occupational stress is generally recognized as an important risk to the health of the workforce. Excessive job stress may cause physical and psychological harm to people, such as anxiety or burnout. It can also negatively affect the effectiveness, productivity and job satisfaction of workers. Previous studies have also determined that working under the risk of many psychological and cognitive factors, such as high mental workload and severe work stress, significantly increases the risk of WRMSDs [17].
In addition to cognitive factors, another important risk factor in the prevalence of WRMSDs and related disability is exposure to harmful physical factors in the work environment such as noise and vibration, unfavorable lighting, and thermal stress (cold and heat stress). Previous studies show that occupational stress caused by high-intensity work, irregular work-rest schedule, and exposure to harmful factors such as high temperature, vibration and noise, may lead to various health problems such as high blood pressure, cardiovascular disorders and WRMSDs [18, 19]. Exposure to noise and vibration in the work environment can impose many physiological and psychological effects on the body. Among them, we can mention mental effects, irritability, changes in nerve and brain waves, changes in blood pressure and heart rate, disorders in the digestive system, and changes in some hormones such as adrenaline and cortisol. In addition to the mentioned cases, noise pollution along with exposure to vibration can aggravate musculoskeletal disorders [20–23]. It has been found that workers exposed to vibrations are often simultaneously exposed to other ergonomic stressors such as poor posture and manual materials handling (lifting). Previous studies have shown a dose-response relationship between exposure to whole body vibration (WBV) and low back disorders. The researchers concluded that occupational WBV exposure is associated with an increased risk of low back pain (LBP), sciatica, and degenerative changes in the spinal system [24].
Optimum lighting can improve health, comfort, sleep quality, work speed, reduce errors and reduce absenteeism, and increase productivity. Improper lighting is one of the potential risk factors for the prevalence of WRMSDs. Improving lighting can help improve posture and prevent ergonomic disorders associated with inappropriate lighting in the workplace [25].
Exposure to thermal stress in the work environment can also affect people physically and psychologically, including disorders such as heat exhaustion, heat stroke, muscle cramps and heatstroke, ergonomic disorders, decreased physical and mental performance, reduced productivity and increased absenteeism. Previous studies show that environmental parameters such as temperature complaints can affect significantly on the prevalence and exacerbation of WRMSDs [26, 27].
In the dynamic setting of the automobile industry, the intricate interplay between environmental factors and cognitive ergonomics has been increasingly recognized as a crucial determinant in the prevalence of WRMSDs among workers. Understanding the relationship between these two domains and their impact on the occurrence of WRMSDs is essential for developing effective prevention strategies and improving overall workplace health and safety in the automobile sector. By probing into how environmental and cognitive ergonomics intersect to influence musculoskeletal health, this study not only sheds light on the multifaceted nature of ergonomic risks but also paves the way for tailored interventions geared towards reducing occupational injuries and enhancing productivity in this pivotal industry.
All the mentioned cases show that cognitive and environmental parameters are among the most important influencing and root cause factors in the prevalence of WRMSDs, which have been studied less compared to physical ergonomic parameters such as improper posture, manual material handling, etc. Therefore, according to the existing research gap in this field, especially among the statistical population of automotive industry workers, as one of the occupations with high and varied manual activity, the present study was conducted with the aim of investigating the relationship between environmental and cognitive ergonomics with the prevalence and severity of WRMSDs in an automotive industry.
Methods
Study design
This cross-sectional study was conducted in 2023 in an automobile company. The statistical population of the present research included all employees working in the operating jobs (800 employees). Therefore, the sample size was 800 employees. Before starting the study, all employees were screened for the presence or absence of musculoskeletal disorders (MSDs). In order to determine the prevalence of MSDs among the studied personnel, self-report questionnaires, and their medical records were used. Finally, it was found that 450 workers had MSDs in at least one of their organs and 350 workers did not experience any MSDs and were studied during the present study.
After deleting confounded questionnaires and considering the response rate of employees, 740 subjects were finally studied (response rate: 92.5%). The number of remaining and studied subjects in the workers with and without WRMSDs groups were 380 and, 360 respectively.
Inclusion criteria included at least one year of work experience in operational jobs, and exclusion criteria was included the history of systemic diseases of the musculoskeletal system like the history of surgery in musculoskeletal system, the history of fractures in musculoskeletal system, osteoporosis, lack of sufficient consent to participate in the study. Before conducting the study, sufficient information about the purpose of the research was provided to the participants to maximize their participation, and participants were assured that their information would remain confidential. The ethics committee of the University approved the methodology of the study.
Finally, in the present study, the relationship between the risk factors related to cognitive, and environmental ergonomics with the prevalence and severity of musculoskeletal disorders was investigated and the ergonomic risk levels of the studied subjects were extracted. Demographic data were extracted using a self-administrated questionnaire and to examine main variables, the following questionnaires were applied.
Cognitive ergonomics
In the present study, four indicators including occupational stress, mental workload, sleep quality, and cognitive failure were used to evaluate this component.
Occupational stress
Job content questionnaire (JCQ)
To evaluate occupational stress in this study the Persian version of the Job Content Questionnaire (JCQ) were applied. The components of this questionnaire include: three items to assess the components of decision-making or control, five items to assess the psychological demands of the job, eight items to assess the social support components, five items to assess the physical demands of the job, and three items to assess the components of job insecurity. The scoring method was in Likert scale format, from 1 ‘strongly disagree’ to 4 ‘strongly agree’. The criteria recommended in the job content questionnaire guidelines were applied to make the model of demand-control houses. The validity and reliability of this tool have been confirmed in previous study (Cronbach’s alpha 0.85) [28].
Mental workload
NASA-TLX questionnaire
The NASA-TLX is a multidimensional tool that provides an overall value of workload according to a weighted average of six dimensions of mental demand, physical demand, temporal demand, effort, overall performance, and frustration level. The participants score each of the six mentioned dimensions based on their working situation from zero to 100. applying the analytical hierarchic method, the importance of each dimension compared to other dimensions is investigated two by two. In this case, people choose the one that is more related to their activity from the two options. Each choice is equal to a weighted score. By multiplying the weight of each dimension of workload (which is between 0–1) by the scale score of each dimension (between 0–100), the total workload is calculated numerically between 0 and 100. In fact, the overall score obtained is expressed as a weighted workload. According to this tool, if the total workload score is less than 50, the risk level is low and if it is above 50, the risk level is high. The validity and reliability of this questionnaire have been confirmed in previous studies (Cronbach’s alpha: 0.897) [29, 30].
Sleep quality
Pittsburgh sleep quality index (PSQI)
The Pittsburgh Sleep Quality Index is a self-report tool that evaluate sleep quality and disturbances over a 1-month time period. This tool uses seven scales that include subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency (ratio of sleep duration to elapsed time), sleep disturbances, use of sleeping medication, and daytime dysfunction. The score of each scale is between 0 and 3, and the score of 3 in each scale indicates the maximum negative value. The total score of this questionnaire is between 0 and 21, and the total score of 6 and above indicates inappropriate sleep quality. The validity and reliability of this questionnaire has been confirmed in various studies (Cronbach’s alpha: 0.83) [8, 31].
Cognitive failure
Cognitive failure questionnaire (CFQ)
In order to evaluate cognitive impairment, Cognitive Failure Questionnaire (CFQ) was used. This tool contains 25 items in 4 subscales of distraction, memory problems, inadvertent mistakes and failure to remember names (forgetfulness). The memory factor includes questions that measure memory deficits and forgetfulness. The distraction factor refers to the perceptual aspects of tasks in which there is diverted attention. The factor of inadvertent errors refers to errors that are made in the execution of work and is related to physical accidents. Each item is answered on a five-point Likert scale from “never” to “always”. The total score of cognitive impairment for each person is obtained from the sum of the scores of the subscales. Higher scores in the present instrument indicate greater cognitive impairment. The good validity and reliability of this tool has been reported in previous studies (Cronbach’s alpha: 0.81) [32, 33].
Environmental ergonomics
This component is actually the physical harmful factors of the work environment. Previous studies have made it clear that the physical harmful factors of the work environment are among the important risk factors in the prevalence of musculoskeletal disorders in the work environment [4]. In the present study, four indicators including noise, vibration, lighting, and thermal stresses were used to evaluate this component.
In this study, the results of annual measurements were used to evaluate the exposure of people to physical harmful factors.
Noise
In order to measure the noise in this study, a KIMO-DB300 sound analyzer model was used. Before the measurement, the sound meter was calibrated using TENMARS-TM100 calibrator at a sound intensity of 94 dB. All measurements were performed in the A frequency weighing network and Slow speed mode.
Vibration
In this study, occupational exposure to vibration was determined qualitatively and using a question with a three-mode answer in the questionnaire with the options, including: “I do not experience any vibration during work shifts”, “I have occupational exposure to vibration during work shifts (at least once a week and or more)” and “I have occupational exposure to vibrating devices continuously and every day during the work shift” were measured.
Lighting
In this study, the intensity of public lighting was measured using a regular grid method with Hanger Screen Master illuminance meter.
Thermal stresses
During the current study, Wet Bulb Globe Temperature (WBGT) was measured at different hours based on the ISO7243 standard [34]. Considering that the type of work processes in the studied industry mainly did not include heat-generating activities and also considering the homogeneity of temperature conditions at different heights, the measurement was carried out in the waist area of people. In each measurement, the device was fixed in its place for 30 minutes to be at the same temperature as the environment.
Evaluation of the prevalence and severity of musculoskeletal disorders
Cornell musculoskeletal discomfort questionnaire (CMDQ)
To determine and evaluate the prevalence, severity and disabilities caused by MSDs in all studied job tasks, Cornell Musculoskeletal Disorders Questionnaire (CMDQ) was applied. This tool is arranged in three sections: the frequency of discomfort, the intensity of discomfort, and the effect of discomfort on work capacity. It has a body map and examines 12 body parts, which are a total of 20 body areas. The findings of the three parts of the questionnaire are multiplied together for each member, and the final result is a number between 0 and 90, which is the product of the repetition value (never = 0, 1 to 2 times a week = 1.5, 3 to 4 times a week = 3.5, every day = 5 and several times a day = 10), discomfort score (1, 3, 2) and work interference score (1, 3, 2). The validity and reliability of this tool has been confirmed in previous studies (Cronbach’s alpha: 0.986) [35, 36].
Evaluation of environmental and cognitive component risk index
During the present study, the model developed by Sadeghi-Yarandi et al. under the title of TUGA ergonomic management and analysis (TEMA) was used to determine the values of environmental and cognitive parameters in the form of a number. This model consists of eight steps, and in the third step, a novel evaluation method has been developed to estimate the ergonomics risk index (ERI) of jobs using the Delphi method as well as Fuzzy analytic hierarchy process (FAHP). The mean CVI and CVR values were reported as 0.92 and 0.80, respectively. Moreover, Cronbach’s alpha values for each of the physical, environmental, and cognitive components and the entire model were reported as 0.91, 0.87, 0.85, and 0.89, respectively. The schematic of the proposed model is presented in Fig. 1 [1]. It should be noted that the investigated parameters were selected according to the model proposed in the study by Sadeghi-Yarandi et al. [1].
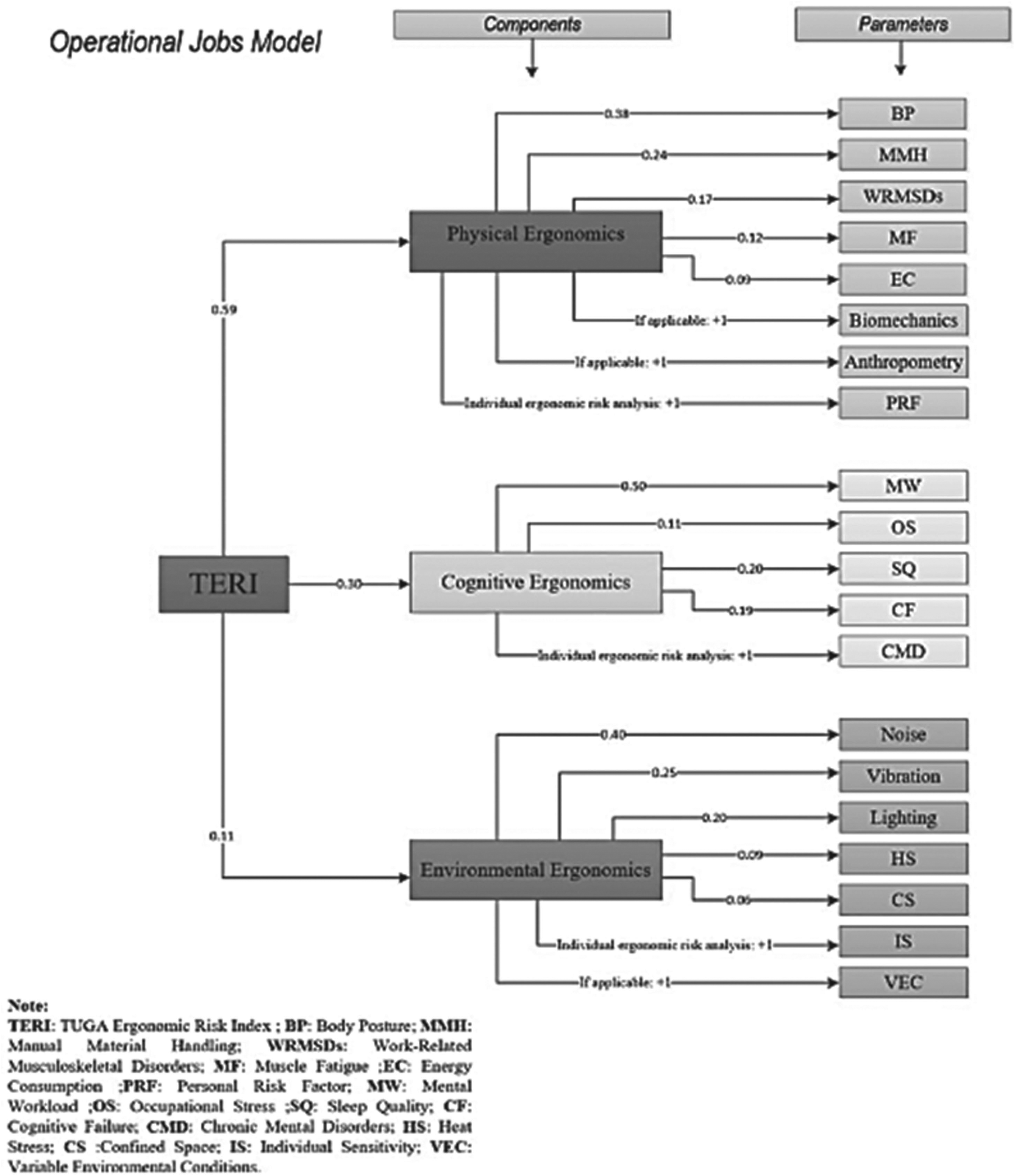
Evaluation model of ergonomic risk index in operational jobs in TEMA model [1].
During the present study, Kolmogorov-Smirnov test was applied to investigating the normality of the data distribution. Descriptive statistics were presented by mean, standard deviation and, frequency. Data analysis was performed using independent sample t-test, one-way ANOVA, chi-square, and multiple logistic regression model. Backward elimination method was applied to make the final regression model. All statistical analyzes were done in IBM SPSS version 25.0 software, and in all statistical tests, a value of 0.05 was accepted as a significant level (p-value < 0.05).
Results
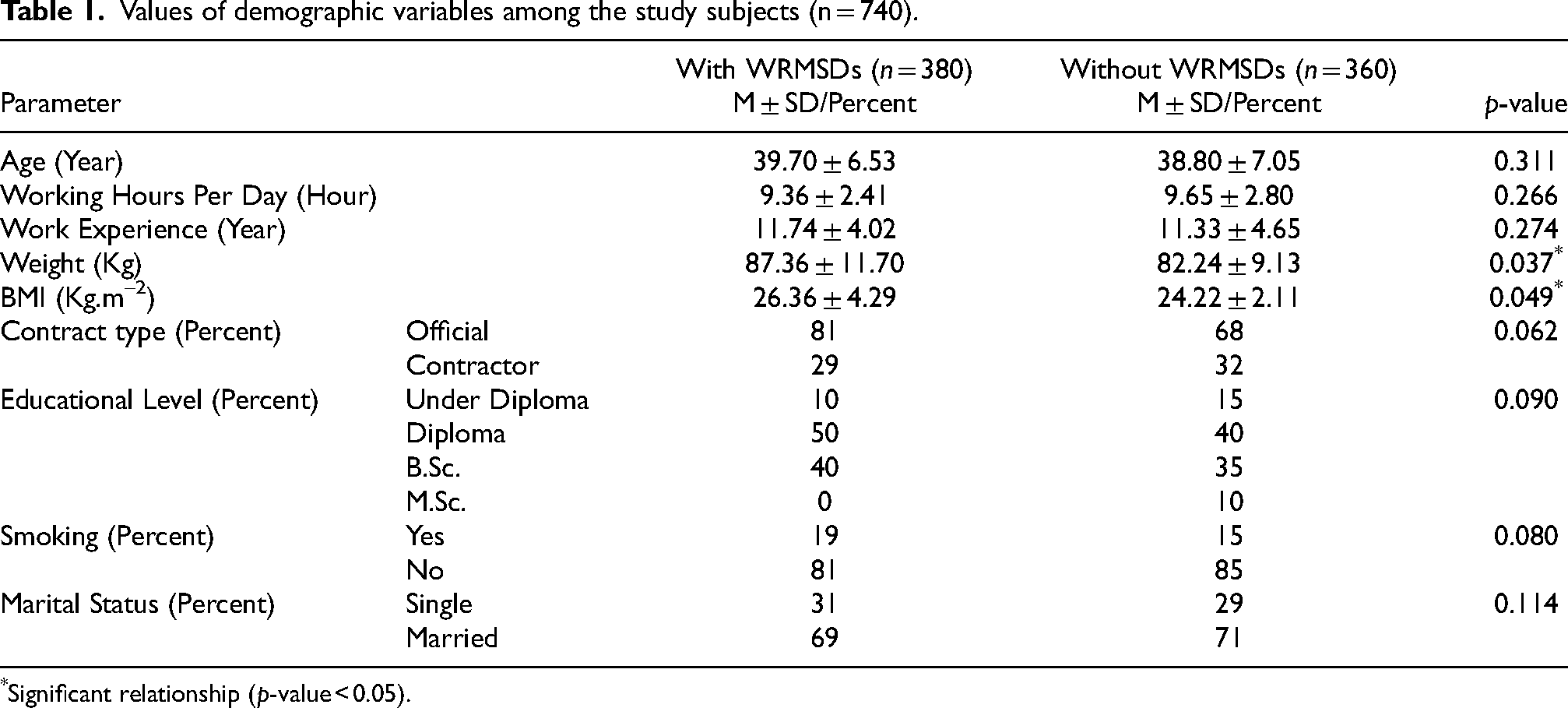
The results revealed that the average age in the workers with, and without WRMSDs groups were 39.70 ± 6.53, and 38.80 ± 7.05 years, respectively. Moreover, the average work experience in the workers with, and without WRMSDs groups were 11.74 ± 4.02, and 11.33 ± 4.65 years, respectively. The average value of body mass index between these two groups were 26.36 ± 4.29, and 24.22 ± 2.11 kg/m2, respectively. It was found that there was a significant difference between the weight and body mass index between these two groups (p-value < 0.05). According to the matching of the two groups, no significant relationship was observed between other demographic variables in the two investigated groups. Other results related to demographic information are presented in Table 1.
Values of demographic variables among the study subjects (n = 740).
Values of demographic variables among the study subjects (n = 740).
*Significant relationship (p-value < 0.05).
Analyzing the prevalence of WRMSDs revealed that 27.42% of the studied subjects didn’t experience any musculoskeletal disorders and 72.58% reported the musculoskeletal disorders in at least one of their body parts during the past 12 months. The highest prevalence of WRMSDs was reported in the neck, left knee, right shoulder, upper back, left foot, and waist with values of 69.6, 60.5, 60.5, 59.7, 59.2, and 56.8 percent, respectively. Moreover, the lowest prevalence of WRMSDs was reported in the right arm, left thigh, and left arm with the values of 34.6, 38.2, and 39 percent, respectively (Table 2).
Prevalence and severity of WRMSDs in different body parts of study subjects (n = 740).

Prevalence and severity of WRMSDs in different body parts of study subjects (n = 740).
The results of the evaluation of cognitive parameters demonstrated that the average values of mental workload, sleep quality, and cognitive failure among the workers with WRMSDs were 50.88 ± 10.36, 14.59 ± 2.14, and 21.32 ± 4.51, respectively. Furthermore, the average values of mention parameter among the workers without WRMSDs were 42.78 ± 11.13, 8.46 ± 3.81, 16.70 ± 3.56, respectively.
Also, the results showed that the cognitive ergonomics score in the workers with, and without WRMSDs groups were 3.14 ± 0.90, and 1.97 ± 0.31, respectively. It was found that the score of all cognitive parameters among the workers with WRMSDs was higher than other group and there was a significant relationship between the mentioned values (p-value < 0.05) (Table 3).
The values of cognitive parameters among the study subjects (n = 740).

The values of cognitive parameters among the study subjects (n = 740).
*Significant relationship (p-value < 0.05).
The obtained values of occupational stress dimensions based on job content questionnaire were presented in Table 4. It should be noted that the higher score of the dimensions of decision making and social support in this tool, demonstrates the low level of stress in these dimensions. The higher value of the dimensions of job psychological demands, job physical demands, and job insecurity, demonstrates high level of stress.
The values of cognitive ergonomics components among the study subjects (n = 740).

The values of cognitive ergonomics components among the study subjects (n = 740).
*Significant relationship (p-value < 0.05).
The results revealed that the mean score of decision-making and job insecurity in employees with WRMSDs was significantly higher than those without any WRMSDs and there was a significant relationship between decision-making values of two groups (p-value < 0.05). Investigating other dimensions of occupational stress revealed that the mean score of job psychological demands, social support, and job physical demands in employees with WRMSDs was significantly higher than those without any WRMSDs and there was a significant relationship between job psychological, and physical demands values of two groups (p-value < 0.05) (Table 4).
The results of the evaluation of different dimensions of mental workload revealed that the mean score values of all dimensions of mental workload including mental demand, physical demand, temporal demand, efforts, overall performance, and frustration level were at higher levels among employees with WRMSDs. There was a significant relationship between the score values of all mental workload dimensions between the workers with, and without WRMSDs groups, except temporal demand (p-value < 0.05) (Table 4).
Sleep quality assessment
The average sleeping hours per day between workers with, and without WRMSDs groups were 5.58 ± 1.04, and 6.76 ± 1.89 hours, respectively. The results of the evaluation of different dimensions of sleep quality among the participants showed that the average scores obtained in subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction dimensions were higher among the workers with WRMSDs and this participant experienced more unfavorable sleep quality compared to the other participants. There was a significant relationship between the score values of all sleep quality dimensions between the two study groups, except habitual sleep efficiency (p-value < 0.05) (Table 4).
Cognitive failure assessment
The results of the evaluation of cognitive failures among the participants showed that the mean score values of all dimensions of cognitive failures were higher among people with WRMSDs, except name dimension. A significant difference was observed between the scores of distraction, memory problems, and blunders components between the two study groups (p-value < 0.05) (Table 4).
The values of environmental parameters
The results of examining the physical harmful factors of the work environment affecting ergonomics, including the parameters of noise, vibration, thermal stress and lighting among the participants showed that the noise exposure values among the workers with, and without WRMSDs groups were 70.36 ± 10.07, and 67.42 ± 7.14 dB, respectively. The average light intensity in the work environment of workers with, and without WRMSDs groups were 157 ± 13, and 183 ± 9 lux, respectively. The average WBGT index (heat stress) in the working environment of workers with, and without WRMSDs groups were 28.32 ± 5.86, and 27.44 ± 3.93C, respectively. The occupational exposure of the participants to vibration was evaluated qualitatively and it was determined that 16% of the participants with WRMSDs and 42% of the participants without WRMSDs did not exposed with vibration in their work shift. Ultimately, the mean environmental ergonomics score value was calculated between workers with, and without WRMSDs groups, with the values of 2.45 ± 1.13, and 2.11 ± 0.88, respectively. It was found that there was a significant difference between the values of all investigated physical harmful factors in the work environment between the two study groups, except thermal stress (p-value < 0.05) (Table 5).
The values of environmental parameters among the study subjects (n = 740).

The values of environmental parameters among the study subjects (n = 740).
*Significant relationship (p-value < 0.05).
Table 6 shows the most important risk factors affecting the prevalence of WRMSDs according to the multiple logistic regression model. The results obtained from the final logistic regression revealed that the most important parameters affecting the prevalence of WRMSDs were mental workload final score, cognitive ergonomics score value, work environment lighting, environmental ergonomics score value, occupational stress final score, sleep quality score and noise exposure with regression Coefficient (B) of 0.25, 0.23, –0.23, 0.22, 0.21 and 0.19 (Table 6).
Evaluation of the effect of individual, cognitive and environmental parameters on the prevalence of WRMSDs using logistic regression.

Evaluation of the effect of individual, cognitive and environmental parameters on the prevalence of WRMSDs using logistic regression.
**Significant correlation at 1% significance level (p < 0.01). aOccupational stress component. bMental workload component. cSleep quality component. dCognitive failure component.
The present study was conducted with the aim of investigating the relationship between environmental and cognitive ergonomics with the prevalence and severity of WRMSDs in an automotive industry. The automobile industry in Iran and the world is one of the major industries in which many people work. Despite the automation of many work processes in this industry, many heavy and repetitive activities are still done manually. Previous studies have shown that the prevalence of musculoskeletal disorders in this industry is very high in Iran and the world, and people perform various job duties in this industry under non-ergonomic conditions [37, 38], so the study of the relationship between different physical, environmental and cognitive risk factors with the prevalence and severity of these disorders in the automotive industry, it is of great importance to conduct proactive studies and plan control measures in order to adjust ergonomic risk levels.
Analyzing the prevalence of WRMSDs revealed that 27.42% of the studied subjects didn’t experience any musculoskeletal disorders and 72.58% reported the musculoskeletal disorders in at least one of their body parts during the past 12 months. The highest prevalence of WRMSDs was reported in the neck, left knee, right shoulder, upper back, left foot, and waist with values of 69.6, 60.5, 60.5, 59.7, 59.2, and 56.8 percent, respectively. As it was mentioned before, due to the variety of manual activities as well as the exposure of employees to a wide range of ergonomic risk factors, the prevalence of musculoskeletal disorders in the automotive industry is high. A systematic review and meta-analysis study in automobile industry in China revealed that the overall 12-month prevalence of WRMSDs among workers in this industry was 53.1%, and the lower back/waist was the body region affected most, which is consistent with the results of the present study [38]. The study conducted by Chen et al showed that the highest prevalence of disorders in the automotive industry is related to the neck and shoulder organs, which is consistent with the results of the present study [39]. In another study, the prevalence rate of WRMSDs in this industry was reported as 70.7%, which is in line with the results of the present study [40].
The results of the evaluation of cognitive parameters demonstrated that the average values of mental workload, sleep quality, and cognitive failure among the workers with WRMSDs were 50.88 ± 10.36, 14.59 ± 2.14, and 21.32 ± 4.51, respectively. Furthermore, the average values of mention parameter among the workers without WRMSDs were 42.78 ± 11.13, 8.46 ± 3.81, 16.70 ± 3.56, respectively.
Also, the results showed that the cognitive ergonomics score in the workers with, and without WRMSDs groups were 3.14 ± 0.90, and 1.97 ± 0.31, respectively. It was found that the score of all cognitive parameters among the workers with WRMSDs was higher than other study group and there was a significant relationship between the mentioned values (Table 3).
The results showed that the amount of mental workload among people with WRMSDs was higher than other study group. Among the factors for the high mental workload in this study, we can mention reasons such as the need for high intellectual and mental activities while performing job tasks and sub-tasks, variety of body movements in unfavorable ergonomic conditions, high volume of activities and the need to perform job duties in the short and limited time frame as well as the continuous effort to maintain optimal job performance. Previous studies have also shown that mental workload is an important risk factor in the prevalence and severity of WRMSDs in automobile industry [40, 41]. Examining the six dimensions of mental workload showed that the average scores of all dimensions in workers with WRMSDs were higher than participants without WRMSDs. It was found that due to the sensitivity of the automotive industry as well as the high variety of job duties and the need to perform a wide range of physical (static and dynamic) and mental activities, the studied subjects needed more physical and mental effort to perform their occupational tasks and time is more important in their job and they should have done their duties in a short and specific time period. The study conducted by Ghasemi et al. also revealed that mental workload is an important parameter in the prevalence of WRMSDs and the mean scores of the dimensions of mental demand, physical demand, temporal demand, effort, and frustration level in individuals with WRMSDs were higher. Their study also reported that there was a significant relationship between the scores of physical demand, temporal demand and effort dimensions and WRMSDs, which is in line with the results of the present study [42].
The results of job stress assessment also showed that the occupational stress level of subjects with WRMSDs was much higher than those without any WRMSDs. It should be noted that the higher score of the dimensions of decision making and social support in this tool, demonstrates the low level of stress in these dimensions. The higher value of the dimensions of job psychological demands, job physical demands, and job insecurity, demonstrates high level of stress.
The findings revealed that the mean score of decision-making and job insecurity in employees with WRMSDs was significantly higher than those without any WRMSDs. These results show that the freedom of decision making was less among people with WRMSDs and these people felt more insecure in their jobs, which can affect their ergonomic disorders. Investigating other dimensions of occupational stress revealed that the mean score of job psychological demands, social support, and job physical demands in employees with WRMSDs was significantly higher than those without any WRMSDs. It was also found that the physical and psychological demands of work are an important parameter in the prevalence of musculoskeletal disorders. Previous studies have also shown that higher physical demands as well as higher demands of the job to perform mental, and cognitive activities make the worker more prone to suffering from various ergonomic disorders [43, 44].
High mental workload and chronic stress are known to impact musculoskeletal health by increasing muscle tension, reducing recovery time, and impairing cognitive function. In the automobile industry, workers often face demanding and cognitively challenging tasks, leading to increased mental workload and stress levels. Prolonged exposure to such conditions can contribute to fatigue, reduced attention, and musculoskeletal strain, thereby elevating the risk of WRMSDs. Exploring the relationship between mental workload, stress, and the prevalence of WRMSDs in the automobile industry requires comprehensive assessments of task demands, cognitive stressors, and psychological well-being among workers. Implementing stress management programs, workload optimization strategies, and promoting work-life balance can help mitigate the negative impact of mental workload and stress on musculoskeletal health, ultimately reducing the incidence of WRMSDs among workers.
The results of the evaluation of the sleep quality of the studied workers revealed that workers with WRMSDs had less sleep duration per day, experienced more unfavorable sleep quality, experienced more sleep disturbances and used more sleeping medication compared to the other study group. The results of the recent study demonstrate that sleeping hours of patients with musculoskeletal disorders were shorter than control group [8]. The mean total score of sleep quality among workers with WRMSDs was higher than other study group, which shows poor sleep quality among them and can create more psychological and physical stress and as a result, the prevalence of musculoskeletal disorders can be increased. Previous studies have also revealed that the sleep quality among people with low back pain was significantly lower than other people, and sleep is one of the effective factors in the prevalence of musculoskeletal disorders, that is in line with the present research [8, 45]. Sleep plays a critical role in musculoskeletal recovery, tissue repair, and overall health. Inadequate sleep quality, disrupted sleep patterns, and sleep deprivation can compromise the body’s ability to recover from daily strain and increase susceptibility to musculoskeletal injuries. In the automobile industry, shift work, long working hours, and irregular schedules can disrupt sleep patterns and lead to sleep disturbances among workers. Investigating the relationship between sleep quality, shift work, and the prevalence of WRMSDs in the automobile industry requires monitoring sleep patterns, assessing sleep quality, and identifying factors that may affect sleep duration and efficiency. Implementing fatigue management strategies, promoting healthy sleep practices, and considering scheduling adjustments can help improve sleep quality, enhance musculoskeletal recovery, and reduce the risk of WRMSDs associated with sleep disturbances.
Finally, the assessment of cognitive failure among the studied subjects showed that the values of cognitive impairment components including distraction, memory problems, and blunders among the individuals with WRMSDs were higher than other group. This means that people with cognitive failures such as forgetfulness, distraction, etc. need to repeat many physical and mental processes while doing their work during the work shift, which can increase their mental and physical workload, and subsequently can lead to an increase in the prevalence of WRMSDs. The results of the study by Sadeghi-Yarandi et al. showed that cognitive failure is an important parameter in the ergonomic risk index of people in work environments [4].
Environmental factors such as noise, lighting, and vibration can also impact musculoskeletal health and contribute to the prevalence of WRMSDs in the automobile industry. Prolonged exposure to high noise levels, inadequate lighting conditions, and excessive vibration can increase stress, fatigue, and physical discomfort among workers, leading to musculoskeletal strain and injuries. It was found that there was a significant difference between the values of all investigated physical harmful factors in the work environment such as noise, vibration, and lighting between the workers with, and without WRMSDs groups, except thermal stress (Table 5).
Exposure to noise in the workplace has many negative effects on people’s health, the most important of which are noise induced hearing loss (NIHL) and cardiovascular problems such as blood pressure [19]. Previous studies have shown that noise and vibration can reduce the capacities and threshold of physical and cognitive tolerance of people in the work environment and act as a risk factor in the prevalence of various WRMSDs [26]. In previous studies, it has been determined that exposure to vibrations (whole body and hand-arm), especially when it is accompanied by an inappropriate posture, can lead to various musculoskeletal disorders locally or systemically. Each organ and tissue of every worker’s musculoskeletal system has its own tolerance. When the physical loads exceed the load tolerance, the tissue can be damaged [20].
Lighting is also one of the most important environmental factors that can lead to the development of musculoskeletal disorders. In addition to causing psychological disorders and eye and vision problems, improper lighting can lead to improper posture in people during the work shift and accelerate the prevalence of WRMSDs [26].
Finally, previous studies revealed that heat and cold stress have negative effects on employee’s health, and job performance, creating irritability, fatigue, and burnout. Heat is a physical hazard that can pose a problem in almost any workplace. Working in hot environments can increases workers’ thermal stress, and decrease their performances and efficiency [26]. The results of the present study also showed that the amount of people’s exposure to physical harmful factors in the work environment in all parameters was higher in the workers with WRMSDs, which is consistent with the findings of previous studies.
Investigating the relationship between noise, lighting, vibration, heat stress and the prevalence of WRMSDs in the automobile industry necessitates conducting ergonomic assessments, environmental monitoring, and risk evaluations to identify potential hazards and their impact on musculoskeletal health. Implementing engineering controls, noise reduction measures, ergonomic lighting solutions, and vibration damping technologies can help mitigate the adverse effects of environmental factors on musculoskeletal health, thereby reducing the incidence of WRMSDs in the workplace.
Ultimately, the findings of logistic regression demonstrated that the most important parameters affecting the prevalence of WRMSDs were mental workload final score, cognitive ergonomics score value, work environment lighting, environmental ergonomics score value, occupational stress final score, sleep quality score and noise exposure with regression Coefficient (B) of 0.25, 0.23, –0.23, 0.22, 0.21 and 0.19 (Table 6). These results show the necessity of comprehensive attention to the aforementioned risk factors in ergonomic intervention programs.
The results of the present study showed that along with physical risk factors, cognitive and environmental risk factors are also important parameters in the prevalence of WRMSDs in the automotive industry, and conducting effective studies in the field of reducing the levels of ergonomic risk factors with proactive approach requires comprehensive attention to all ergonomic components, including physical, environmental and cognitive.
By studying the relationship between environmental and cognitive ergonomics, researchers and industry professionals can gain insights into the synergistic effects of these factors on the musculoskeletal health of automobile industry workers. Findings from this study highlight the critical need for a holistic approach that considers both the external work environment and internal cognitive processes to effectively prevent and manage WRMSDs. Strategies that integrate both environmental and cognitive ergonomic considerations can lead to comprehensive interventions that holistically address the root causes of WRMSDs. Through interdisciplinary collaboration and evidence-based approaches, it is possible to create a safer and healthier work environment that promotes employee well-being, productivity, and long-term sustainability in the automobile industry.
Strengths and limitations of the study
Among the strengths of the present study, we can point out the simultaneous study of the most important cognitive and environmental risk factors affecting the prevalence and severity of musculoskeletal disorders in the automotive industry as one of the most important and largest industries in Iran. The results of the present study can lead to the creation of a novel scientific perspective for the implementation of control, preventive, and proactive programs in the field of ergonomic risk management in similar industries.
Among the limitations of the present study, we can mention the impossibility of studying the risk factors in the field of organizational ergonomics, impossibility of evaluating exposure to vibration quantitatively, as well as the impossibility of conducting an interventional study due to time and economic constraints. Therefore, it is suggested that in the future researchers in this industry conduct interventional studies and also assess the risk factors at the level of organizational ergonomics and evaluate the effectiveness of the results of their study in order to create the basis for the implementation of preventive and proactive measures in the framework of the ergonomics management system. It is also worth mentioning that all tools used in the cognitive ergonomics section were self-reported and subjective. Therefore, it is suggested that researchers use objective methods to evaluate this component in the future. Considering that this study was conducted in Iran as a developing country, it is suggested to use its results with caution in similar industries in developed countries due to the different nature of working processes and ergonomic management programs.
Implications for future research
Understanding the complex interplay between physical, environmental and mental parameters and the prevalence of WRMSDs in the automobile industry is essential for developing holistic interventions that address multiple ergonomic risk factors. Integrating ergonomic principles, occupational health strategies, and environmental management practices can help create safer, healthier, and more ergonomic work environments that support musculoskeletal health and well-being among workers.
Future research directions may include longitudinal studies to assess the long-term effects of interventions targeting physical, environmental and mental parameters on reducing WRMSDs prevalence, ergonomic interventions tailored to specific job roles within the automobile industry, and the development of personalized health promotion programs to support musculoskeletal health and prevent work-related injuries.
Conclusion
The investigation into the relationship between cognitive and environmental risk factors such as mental workload, occupational stress, sleep quality, cognitive failure, noise, lighting, vibration, heat stress and the prevalence of WRMSDs in the automobile industry underscores the multifaceted nature of occupational health risks and the interconnectedness of various ergonomic factors. Findings from this study highlight the critical importance of considering not only physical ergonomics but also psychological and environmental factors in preventing WRMSDs and promoting musculoskeletal health among automobile industry workers.
Addressing these interconnected ergonomic risk factors through tailored ergonomic interventions, occupational health programs, and environmental modifications can play a vital role in reducing the prevalence of WRMSDs, improving worker well-being, and enhancing overall productivity and safety within the automobile industry.
Footnotes
Acknowledgments
This research project was supported by Behbahan University of Medical Sciences (Approval code: 402100). Therefore, the authors express their gratitude to the Behbahan University of Medical Sciences as well as participants of the present study.
Ethical approval
The present study was approved by the ethics committee of Behbahan University of Medical Sciences (Ethics code: IR.BHN.REC.1403.003).
Informed consent
Before conducting the study, an informed consent form was obtained from all participants.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
None to report.