
Abstract
Keywords
Introduction
Prostate cancer is a common malignancy in men. For localized stage, standard treatments include active surveillance, radical surgery and radiotherapy. For patient treated with radiotherapy, the option of brachytherapy (either low- or high-dose-rate), conventional external-beam radiotherapy, or altered-fractionation radiotherapy can be applied. With conventional radiotherapy, 1.8∼2Gy per fraction is typically delivered. Dose escalation was shown to improve biochemical disease free survival but have more grade 2+ toxicities. Recently, prostate cancer was reported to have relatively low α/β according to several studies [2, 56]. The estimated α/β value was even suggested to be as low as 1.4Gy [2, 41], thus indicating a greater sensitivity of prostate cancer cells to changes in fraction size. Such α/β value of prostate cancer is lower than the α/β of nearby organs at risk (OARs). Thus hypofractionated radiotherapy is considered to be an alternative way to escalate dose to tumor target without increasing toxicities. Stereotactic body radiotherapy (SBRT), an extreme type of precision-oriented hypofractionated radiotherapy, has potential to achieve excellent tumor control with less radiation-related toxicity over conventional radiotherapy [14, 52].
In previous studies of SBRT for prostate cancer, CyberKnifetrademark (CK, Accuray, Sunnyvale, CA, USA), an image-guided radiation therapy (IGRT) system designed for radiosurgery, was the most commonly used modality. Its compact 6 MV linear accelerator mounted on a robotic arm can deliver beams from non-coplanar and non-isocentric angles. Orthogonal pair of x-ray cameras are used for Image guidance during the treatments. However, as the technology in radiation delivery advances, modalities other than CK were applied in SBRT for prostate cancer in recent years [1, 50]. Helical Tomotherapytrademark (HT, TomoTherapy Inc, Madison, WI), a non-coplanar arc intensity modulated radiation therapy (IMRT) with 64-leaf 0.625 cm multileaf collimator (MLC) and IGRT system with mega-voltage computer tomography (MVCT) guidance which continuously delivered fan-beam in a spiral pattern by rotating gantry and moving couch at the same time, was shown to have greater dose homogeneity and lesser dose to the OARs over conventional IMRT dosimetrically [6, 46].It is thus considered suitable to perform SBRT for prostate cancer.
The aim of this study is to compare the dosimetric properties of SBRT for prostate cancer with HT vs. CK, and evaluate the possible clinical impact by using radiobiological models to mitigate dose heterogeneity and analyze fractionation effect.
Material and method
Patient selection and treatment planning
The cases of 12 patients with clinically localized prostate cancer previously treated with CK for SBRT were selected for analysis. Golden fiducial markers were implanted into the prostate gland for real-time image tracking system of CK. Patients were setup in supine position with rectum emptied before each treatment fraction using rectal laxatives. CT images with slice thickness of 1.25 mm as well as diagnostic MRI were acquired for contouring and planning. The CK plans were generated for SBRT treatment using Accuray Multiplan 4.5 planning system with a cone size of 3 cm. The contours were exported as DICOM-RT files and then imported into the planning system of HT. Subsequently, a HT plan was made for each patient in Hi-Art® 4.2.3 System using a pitch of 0.287, a modulation factor of 2, and a 2.5 cm field width afterwards. All the plans were done by experienced medical physicists and evaluated by the same radiation oncologist.
The clinical target volume (CTV) was defined as the whole prostate gland. The planning target volume (PTV) was created by adding 3 mm in posterior direction and 5 mm margin in other directions to CTV. The setting of PTV margin is based on previous literature [14]. Contours of rectum and bladder were delineated using the whole organ volumes. Urethra was defined as containing both the intra-prostate and membranous segments. Target and OAR contours were manually generated in Multiplan planning system by physicians for the initial CK treatments. Then the CT images and contours were transferred from the CK to the HT treatment planning system. The prescribed dose is 37.5Gy in 5 fractions, assigned to cover more than 95% volume of the PTV. The dose constraints of normal tissues are listed in Table 1.
Normal tissue dose constraints
Normal tissue dose constraints
The plans contained the simulation result of dosimetric distribution for each case, and the dose-volume histograms (DVHs) could be generated by planning systems for further analysis. For each of the CK and HT plans, the DVHs were exported as text files from planning system and then analyzed with Python. Coverage of PTV, normalized conformity index, heterogeneity index and dose gradient index were calculated as per the following equations:
Coverage of PTV
New conformity index
The new conformity index (nCI) is generally used to evaluate the degree of dose conformity for radiosurgery plans. A perfect plan would have a nCI of 1.0.
Heterogeneity index
The heterogeneity index (HI) is a tool to describe the heterogeneity of dose distribution in target volume. The value of HI is always greater than 1. A perfect uniform dose distribution would have a HI of 1.0.
Dose gradient index
Dose gradient index (GI) is used to measure how steep of dose falloff outside the target. The value of GI is always greater than 1. A steeper dose gradient would have a lower value of GI.
The integral dose (ID) to the body (excluding the PTV) was also calculated as
where v i is the ith volume (L) receiving the dose of D i (Gy). The range of i is depended on the bin number of DVH.
The dosimetric indices used in normal tissue constraints were compared between CK and HT plans. Among these organs, rectum is most concerned. So we also compare the relative volume of rectum received 10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90% of prescribed dose to describe the statistic difference over the whole curve of DVH, and D1cc, D2cc, D5cc, and D10cc of the rectum were considered to be significantly associated with rectal bleeding [27].
Radiobiologic evaluation
For radiobiologic evaluation, DVHs were used to calculate the generalized equivalent uniform dose (gEUD, [42]) and normal tissue complication probability (NTCP) by an in-house Python program. The Lyman-Kutcher-Burman (LKB) model used for NTCP calculation [29, 35]. The radiobiological parameters for rectum and bladder toxicities were extracted from previous publications (Table 2). DVH was reduced to gEUD, a single dose value attributed uniformly across the entire volume and is assumed to result in an equivalent biological effect as the originally heterogeneous dose distribution would predict. gEUD is a good tool for comparing the dose-effect relations of target response and normal tissue toxicity amongst varying heterogeneous dose distributions. The formula of gEUD is taken from Niemierko’s phenomenological model [42]. In order to mitigate various SBRT fractionation schemes, the dose bins of DVH were converted to linear quadratic equivalent doses of 2Gy per fraction. This “equivalent dose in 2Gy fractions” (EQD2) wascalculated as
Parameters of biologic model
Parameters of biologic model
where D is the total dose, and d is the dose per fraction. The α/β value for prostate cancer was assumed to be 1.4Gy [41]. The α/β value for late toxicities of rectum and bladder is assumed to be both 3Gy. The formula of gEUD is defined with
where vi is the ith volume receiving biological equivalent dose EQD2i. The empirical parameter n characterizes the dose-volume effect. When n is close to 1.0 then the organ is considered to have a parallel structure, and the value of gEUD will approach the mean dose for the entire volume. When n is close to 0 then the organ is considered to have a serial structure, which means that the volume effect is small and the value of gEUD will be near the maximum dose within the volume. Some studies have used the parameter “a” for EUD calculation, where “a” is equal to 1/n. Parameter n is assumed to be –0.05 (a = –20) for prostate cancer [16].
According to the LKB model, NTCP is calculated using the following equations:
TD50 is the uniform dose causing 50% complication probability, and parameter m characterizes the steepest slope of the sigmoid NTCP curve. The statistical method for comparing the plans was Wilcoxon’ sign rank test using Python programming. If the p value < 0.05, the differences were considered statistically significant.
The mean volume of prostates is 43.47±17.15 cc. Averaged cumulative dose-volume histogram (DVH) of all 12 cases for PTV, rectum, bladder, penile bulb and urethra from CK and HT plans are shown in Fig. 1. Target coverage, homogeneity, conformity and dose gradient of PTV are presented in Table 3. PTV coverage for CK and HT were both adequate by achieving the goal of being greater than 95%. HT plans showed a slightly better coverage of the PTV as compared to CK plans (97.74±0.86% vs. 96.56±1.17%; p < 0.05), along with more homogenous dose distribution as shown by the homogeneity index (1.04±0.01 vs. 1.21±0.02; p < 0.05). There was no significant difference between the GI of HT and CK plans (4.59±0.3% vs. 4.72±0.57%; p = 0.48), which indicated that HT and CK resulted in a comparable drop-off in dose gradient beyond PTV. The nCI was better in HT plans (1.16±0.05 vs. 1.21±0.04; p < 0.05).
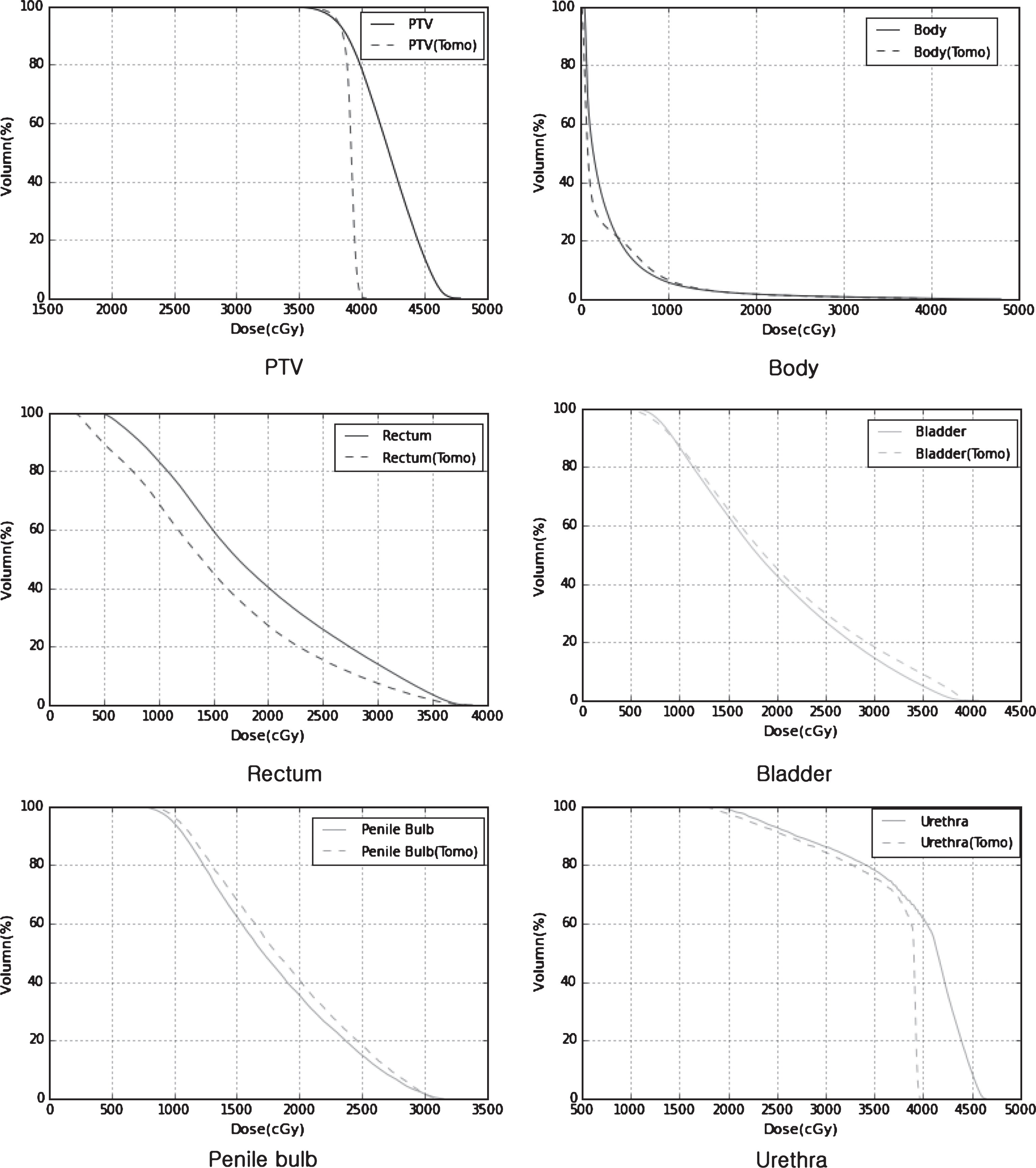
Averaged DVHs.
Dosimetric index of target and organ at risk
Dosimetric indices for OARs are listed in Table 3. Averaged DVH and dosimetric indices for rectum revealed that the volume receiving any dose level of radiation was significantly lower in HT than in CK plans. The dosimetric indices of V37Gy and V37.5Gy for bladder were lower in CK plans. There was no difference in the selected dosimetric index of V49 for urethra and V29.5 for penile bulb. However, averaged DVH for urethra showed that the volume receiving doses higher than prescribed dose was obviously higher in CK plans. The volume of penile bulb exposed to low doses was lower with CK as shown in the corresponding DVH. The integral doses to the body excluding PTV were higher in CK plans (57.05±11.68Gy’L vs. 46.59±6.44Gy’L; p < 0.05). The DVH of body also showed that the volume receiving low dose is smaller in HT plans (Fig. 1).
EUDs of target volume and critical organs are showed in Table 4. The EUD values of CTV were significantly higher in CK plans (119.45±3.69Gy vs. 106.14±1.65Gy; p < 005). EUD values for rectal toxicities with n = 0.12 were lower in HT plans (53.98±2.15Gy vs. 50.04±3.64Gy; p < 005). There was no difference in the EUD value for bladder toxicity with n = 0.5 (p = 0.75). Calculated NTCP for rectal and bladder toxicities are listed in Table 5. HT improved the complication probability for rectal toxicities as compared to CK. However, the complication probability for late genitourinary toxicity was not significantly different between the two techniques.
*p < 0.05.
Calculated EUD for rectal/urinary toxicities and target volumes are compared between CK plans and HT plans
*p < 0.05.
Calculated NTCP for rectal and urinary toxicities are compared between CK and HT plans
*p < 0.05.
With the increased interest in SBRT for localized prostate cancer, more and more institutes began trying IMRT-based treatment technologies other than CK. Volumetric arc therapy such as RapidArcTM was demonstrated to have comparable dose distribution and advantage in faster delivery time as compared to CK [32, 36]. Macias et al. showed that HT is a feasible modality to treat prostate cancer with SBRT according to their initial clinical results [37]. However, as far as we know there has been no publication directly comparing CK and HT SBRT plans.
Target dose coverage, conformity and homogeneity
Our result showed that both CK and HT plans achieved adequate coverage and conformity for PTV with a prescribed dose of 37.5Gy. HT plans have slightly better coverage. The absence of flattening filter makes CK produce a steeper dose gradient. The dose distributions inside target volumes in CK plans are more inhomogeneous. As the DVHs of PTV show in Fig. 1, the PTV has more volume of cold and hot spots in CK pans. The larger proportion of hot spots in the target volumes in CK plans leads to an increase in mean dose and EUD. Dose escalation studies with conventional fractionation had proven that higher doses will improve clinical outcomes [19, 49]. The RTOG 94-06 trial escalated the dose up to 79.2Gy using three-dimensional conformal radiation therapy (3D-CRT) [40]. The escalated dose could be as high as 86.4Gy using 5–7 field IMRT [49]. Further dose escalation using conventional fraction is limited by consideration of increased toxicities. Nevertheless, the prescribed dose of 37.5Gy in 5 fractions used in our study is equivalent to 96∼98.16Gy (using α/β= 1.4∼1.5Gy) for 2Gy per fraction, which is much higher than the escalated doses used in previous studies. The benefit of further dose escalation to such high dose regimen is unknown [33]. Furthermore, toxicity of intra-prostatic urethra should also be taken account into consideration. Cold spots in prostate may raise a concern in compromising tumor control. However, Levegrün et al. showed that cold spots in targets may not be correlated with biopsy outcome in clinical practice [30], probably because the organ motion and setup uncertainties reduce the impact of inhomogeneity.
Normal tissue
We attempted to decrease the volume to rectum irradiated with a dose of 36Gy during planning. Both CK and HT met the constraints. However, HT performed better in its ability to spare rectum at lower doses. The dosimetric indices of D1∼10cc for rectum are suggestive to be correlated with late rectal bleeding from the experience in brachytherapy [21, 27]. Our result showed that D1∼10cc of rectum were significantly lower in HT than in CK plans. Although both modalities achieved the constraint of V36Gy<1c.c. for rectum equally, clinical rectal toxicity was expected to be lower with HT. The dosimetric indices for bladder are better in CK plans but it is probably due to the smaller PTV margin in anterior direction of the prostate as compared to HT plans.
Unnecessary radiation delivered out of target would increase the risk of developing secondary malignancies [18]. Our result showed that the integral dose to the body is higher in CK plans. Moreover, Schneider et al. found that the planning system of CK underestimated the dose out of field, while the accuracy of dose is reliable up to 35 cm form the PTV border in HT planning system [45]. The actual dose delivered out of target with CK may be much higher than we have estimated. Ślosarek et al. compared the integral doses among CK, VMAT, IMRT and HT for prostate cancer treatment with a total dose of 36.25Gy delivered in 5 fractions [47]. The integral dose delivered to the body was higher with HT than CK, which is different from our result. This is probably caused by different objective parameters setup for constraints in the HT planning.
Radiobiological model analysis - EUD
Radiobiological analysis with EUD and NTCP for toxicities was also performed. EUD and NTCP were applied only for conventional fraction size. So the original DVHs were converted to BED2-based DVHs using LQ model [5, 31]. EUDs were then calculated as previously described. The α/β value for late rectal toxicity has been suggested to be as high as 4.6Gy by analyzing the data of RTOG 94-06 trials [55] and 5.4Gy in Brenner’s review [3]. However, we assumed α/β to be a relatively low value of 3Gy in order to prevent underestimating such toxicity [55] using SBRT. In addition to comparing plans, EUD itself could also be an independent prognostic factor for rectal and urinary toxicities. Fleming et al. analyzed the correlation between EUD and toxicities of 180 patients treated with 3D-CRT for prostate cancer. EUD was calculated with parameter n = 0.12 for rectum and n = 0.5 for bladder. They found patients receiving an EUD of >63.1Gy to rectum and >53.4Gy to bladder have higher risk of developing grade 2+ rectal (30%) and urinary (33%) toxicities, respectively [11]. The averaged EUDs of rectum and bladder were much lower in our study, which is considered to be relative safe according to Fleming et al.’s study.
Radiobiological model analysis - NTCP
The respective values of parameters n, m and TD50 using the LKB-model for NTCP calculation vary widely amongst different studies [10, 54], and there is no consensus currently. In this study, we obtained the parameters for rectal toxicities from QUANTEC recommendation [39] and the reports of Gulliford [17], Tucker [54] and Peeters [43]. The end points used in these NTCP parameter studies were not exactly the same. Most previous NTCP parameter studies focus on rectal bleeding or combined rectal toxicities. Gulliford offered NTCP parameters for other rectal toxicities which were less mentioned before [17]. Even with the similar end point of late rectal bleeding, our result showed that NTCP values differed with parameters from different sources. The calculated NTCP is also affected much by the choices of different α/β values. NTCP may not be able to be utilized to predict real toxicity rates precisely. However, it is adequate for comparing different treatment plans. The clinical result of 100 patients treated with similar setting of regimen and constraint using CK as reported by Chen et al. showed that the late GI and GU grade 2+ toxicity rates were 1% and 31%, respectively [7]. In this study, NTCPs for grade 2+ late rectal toxicities were also low. Furthermore, NTCPs for most of the late rectal toxicities are lower with HT than CK. The result agrees with the dosimetric indices of D1cc and EUD. However, the differences of rectal complication probabilities between CK and HT plans are not large.
There was no reliable NTCP model for bladder to estimate the urinary toxicity in the past as mentioned in QUANTEC report. Kole TP et al. recently published a set of LKB-NTCP parameters for late urinary toxicities generated from SBRT treatment [26]. There was no difference in NTCP of both delivery techniques for late urinary toxicity in our study, and this result was compatible with the EUD of bladder [11].
Limitation
Our study has some limitations. Inter-fraction and intra-fraction motions of the prostate have been considered to be important factors [28, 34]. CK is equipped with a kV-image-based tracking system for correcting intra-fraction error during treatment delivery, while HT has MVCT-based image guidance system which can only correct inter-fraction motion. Such difference may result in divergent clinical outcomes. However, this is unfortunately not amenable to be evaluated in our study.
The DVH were generated from different treatment planning system of HT and CK. We could not know the way they calculated DVH in detail inside planning system. However, the calculation of DVH is not complex. If there is difference that will probably be result from the way they dealing with interpretation between dose pixels. However, we believed that the difference could be small because the resolution of dose distribution is fine in modern planning system with adequatesetting.
The LKB NTCP model was designed in the setting of conventional fractionation, thus most of the parameters were not generated from SBRT data. There is a debate on applying LQ model to relatively large dose per fraction. However, a fraction size below 10Gy is still believed to be reliable for clinical application [4, 24]. Current LKB NTCP model might not be applicable with different modalities. Troeller et al. found that the estimated NTCP parameters derived from 3D-CRT and IMRT are different from each other [53]. HT and CK resulted in some differences in dose distribution. The influence of applying the same NTCP parameters to the two different modalities is unknown. It will be interesting to compare calculated NTCP with the actual clinical outcome in SBRT. On the other hand, further study for the feasibility of using LKB NTCP for SBRT should be performed.
Conclusion
In conclusion, HT was shown to provide comparable conformity and coverage for targets as with CK. A slightly better ability in sparing rectum with HT than CK, both dosimetrically and per radiobiologic consideration, could potentially translate into the advantage of lower late rectal toxicity.