
Abstract
Mixed epithelial and stromal tumor of the kidney (MESTK) is a rare renal tumor composed of epithelial and stromal cells. In this study, we report a rare case of MESTK, which was pathologically benign but complicated with renal vein and inferior vena cava tumor thrombus. The 50-year-old female patient was admitted to hospital for a mass on the left kidney. Computed tomography showed a 32 mm×18 mm mass with slight delayed enhancement in the left renal sinus, and neoplastic thrombus was detected in left renal vein and inferior vena cava. A preoperative diagnosis of renal leiomyoma was made by needle biopsy and a laparoscopic radical nephrectomy with thrombectomy was performed. Histologically, the tumor and thrombus were composed of proliferative spindle cells and a small amount of tubular structures. Both kinds of the cells were well differentiated with no atypia or mitosis of nuclei. Immunohistochemical staining showed positive for CK, Ki-67 in the tubular cells and desmin, actin, estrogen receptors, progesterone receptors in the spindle cells. Finally, the diagnosis of MESTK was established. No recurrence or metastasis was found in the patient with a followed-up period of 12 months after the surgery. Due to the difficulty in diagnosis of MESTK, documentation with more cases of MESTK is needed to further understand its pathogenesis, biological behavior, preoperative diagnosis and optimal management of patient treatment.
Keywords
Introduction
Mixed epithelial and stromal tumor of the kidney (MESTK) is a rare renal tumor, which is composed of epithelial and stromal components with solid and cystic architecture. It was first described by Michal and Syrucek in 1998 [1], and had been reported under various names such as cystic hamartoma of renal pelvis, adult mesoblastic nephroma, cystic nephroma, cystic partially differentiated nephroblastoma, or solid and cystic biphasic tumor of the kidney. In the 2004 World Health Organization Classification of Tumors of the Kidney, MESTK was adopted as an official name [2], accounting for 0.2% –1.6% of all renal neoplasms [3, 4]. During the past decades, emerging features of MESTK have been explored, leading to an increased awareness of this type of renal tumor.
MESTK occurs almost exclusively in perimenopausal women, especially those having a history of long-term oral contraceptive use. To date, only 5 male cases of MESTK have been reported [5–9], and 2 of them had a history of prostate cancer treated with anti-androgens [7, 9]. The chief complaints of MESTK are palpable abdominal mass, flank pain, hematuria and urinary tract infections. Approximately 25% of the patients are asymptomatic, detected incidentally during a work-up for other unrelated disorders [4]. The tumors range in size from 1 cm to 21 cm in diameter (mean 6 cm to 9.7 cm) [9–11]. The mostly described imaging features of MESTK are single, centrally located, well-circumscribed masses with cystic architecture, and a delayed enhancement of the solid component during the nephrographic phase on contrast-enhanced computed tomography (CT).
MESTK is confirmed by pathological and immunohistochemical examination, and mostly proved to be benign. Microscopically, MESTK has a mixture of epithelial and stromal components, with the former generally predominating. The epithelial component can display tubules, microcysts or macrocysts, and cells lining the tubulo-cystic architecture show a variety of different morphologies, such as flat, cuboidal, tall, and hobnail-like cells. The stromal component consists of a spindle cell proliferation that resembles ovarian stroma, showing a differentiation towards smooth muscle cells. Immunohistochemically, epithelia of MESTK are positive for CK, vimentin, EMA, and the stromal cells are positive for desmin, SMA, vimentin. Some tumors cells, especially the stromal cells, also express ER and PR, but it is not specific to MESTK [9, 11–14]. MESTK used to be considered a benign tumor at first, while a small number of cases with malignant transformation have been published in the literature. In the reported 15 cases of malignant MESTK (13 females and 2 males), 13 cases showed sarcomatous transformation in the stroma, including leiomyosarcoma, rhabdomyosarcoma, synovial sarcoma, chondrosarcoma and unclassified sarcoma [6, 15–25]. Malignant transformation of the remaining 2 cases was in the epithelium, classified as renal papillary carcinoma [17] and endometrioid adenocarcinoma [20] respectively. Hemorrhage and necrosis are common in malignantcases.
The pathogenetic mechanism of MESTK remains hypothetical and several theories have been proposed [10, 25]. The most widely accepted is hormone-induced pathogenesis. The preponderance in perimenopausal females with a history of long-term estrogen replacement and the frequent expression of ER and PR suggest that the hormonal milieu plays an unneglectable role in the evolution of MESTK.
To our best knowledge, this is the first case being diagnosed as benign MESTK complicated with renal vein and inferior vena cava tumor thrombus, and treated with laparoscopic nephrectomy and thrombectomy. Our pathology department colleagues has described the pathological morphology of this special case [26]. Here we provide detailed information on its imaging data, diagnosis and treatment methods. Meanwhile, we review the related literature and make somesummaries.
Case report
A 50-year-old female patient was admitted to hospital for a mass on the left kidney with inferior vena cava thrombus identified incidentally in a routine physical examination. No clinical symptoms or accompanying diseases were present. She had regular menstruation and had no history of receiving hormones or contraceptive agents. A family history of renal tumor was denied and physical examination was unremarkable.
All of her laboratory data were within normal ranges. A contrast-enhanced CT of the abdomen revealed a well-marginated mass measuring 32 mm×18 mm in the left renal sinus (Fig. 1). The mass showed uniform density without necrosis, calcification or cystic lesion, and showed slight delayed enhancement. Filling defect was detected in left renal vein and inferior vena cava with slight enhancement and considered as neoplastic thrombus. There was no evidence of involvement of lymph nodes or distant metastasis. On magnetic resonance imaging (MRI), the mass showed isointense on T1-weighted images, mixed iso-hyperintense on T2-weighted images, and no obvious enhancement on contrast-enhanced MRI. 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) did not show abnormal metabolism of the tumor and thrombus. Urine exfoliative cytology was negative for malignancy. Fluorescence in situ hybridization (FISH) didn’t detect abnormalities of chromosomes 3, 7, 17 and the p16 (9p21) gene. Flexible ureterorenoscopy was also carried out but detecting nothing abnormal. It was difficult to distinguish the nature of the mass and thrombus on the basis of the examinations above. On the one side, the mass was not enhanced distinctly on CT and did not show abnormal metabolism in PET, appearing to be benign, but on the other side, the mass was complicated with neoplastic thrombus, which is usually a sign of aggressive behavior. The diagnosis was puzzled, and further, we conducted a needle biopsy of the mass for pathological diagnosis. Microscopically, the biopsy tissue was composed of proliferative spindle cells without fat or vascular components. There was no significant cytological atypia or mitosis of nuclei, and no areas of necrosis. Immunohistochemical staining of the spindle cells showed diffusely positive for desmin and actin, while negative for HMB-45, CD34 and S-100. Pathological findings of biopsy supported the diagnosis of leiomyoma, and the thrombus was presumed to be intravascular leiomyomatosis, which can be histologically benign but biologicallymalignant.
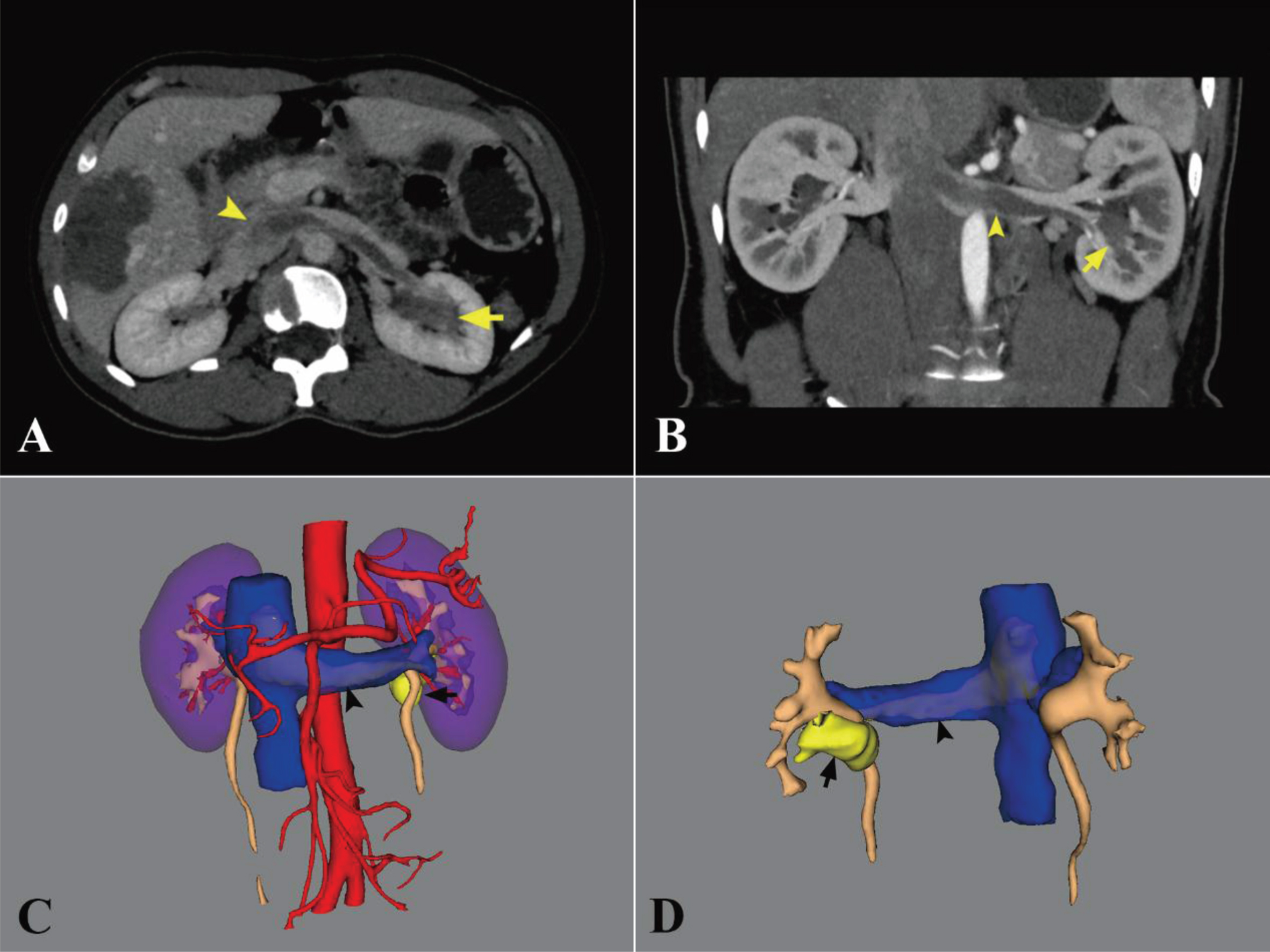
Axial (A) and coronal (B) contrast-enhanced CT revealed a well-marginated mass in the left renal sinus, showing slight delayed enhancement. Filling defect in left renal vein and inferior vena cava was considered as neoplastic thrombus. (C) (D) Three-dimensional CT reconstruction images. (The arrows indicate the mass and the arrow-heads indicate the thrombus.)
Given the tumor was in the renal sinus and complicated with thrombus, we opted for a laparoscopic left radical nephrectomy with inferior vena cava thrombectomy. On the postoperative gross examination, the solid tumor arose from the renal parenchyma and bulged into the renal pelvis, not encapsulated but well circumscribed, measured 35 mm×25 mm on maximum section and appeared yellow (Fig. 2). The tumor thrombus was 9 cm in length and connected to the tumor. It didn’t infiltrate the vascular wall and presented smooth surface. Microscopically, the tumor and thrombus were mainly composed of proliferative spindle cells. A small amount of tubular structures were distributed among the spindle cells (Fig. 3). Both kinds of the cells were well differentiated with no atypia or mitosis of nuclei, and there was no hemorrhage or necrosis. Hyaline change was noticed in focal hypocellular areas. By immunohistochemical investigations, the tubular cells were positive for CK with Ki-67-positive cells occupying about 1%, and the spindle cells were positive for estrogen receptors (ER) and progesterone receptors (PR) (Fig. 3) besides the staining result of biopsy tissue. Finally, the diagnosis of benign mixed epithelial and stromal tumor of the kidney with renal vein and inferior vena cava tumor thrombus was established. The patient was followed up for 12 months after the surgery with contrast-enhanced CT and no recurrence or metastasis was found.

Grossly, the solid tumor arose from the renal parenchyma and bulged into the renal pelvis. Tumor thrombus was connected to the tumor and it didn’t infiltrate the vascular wall.
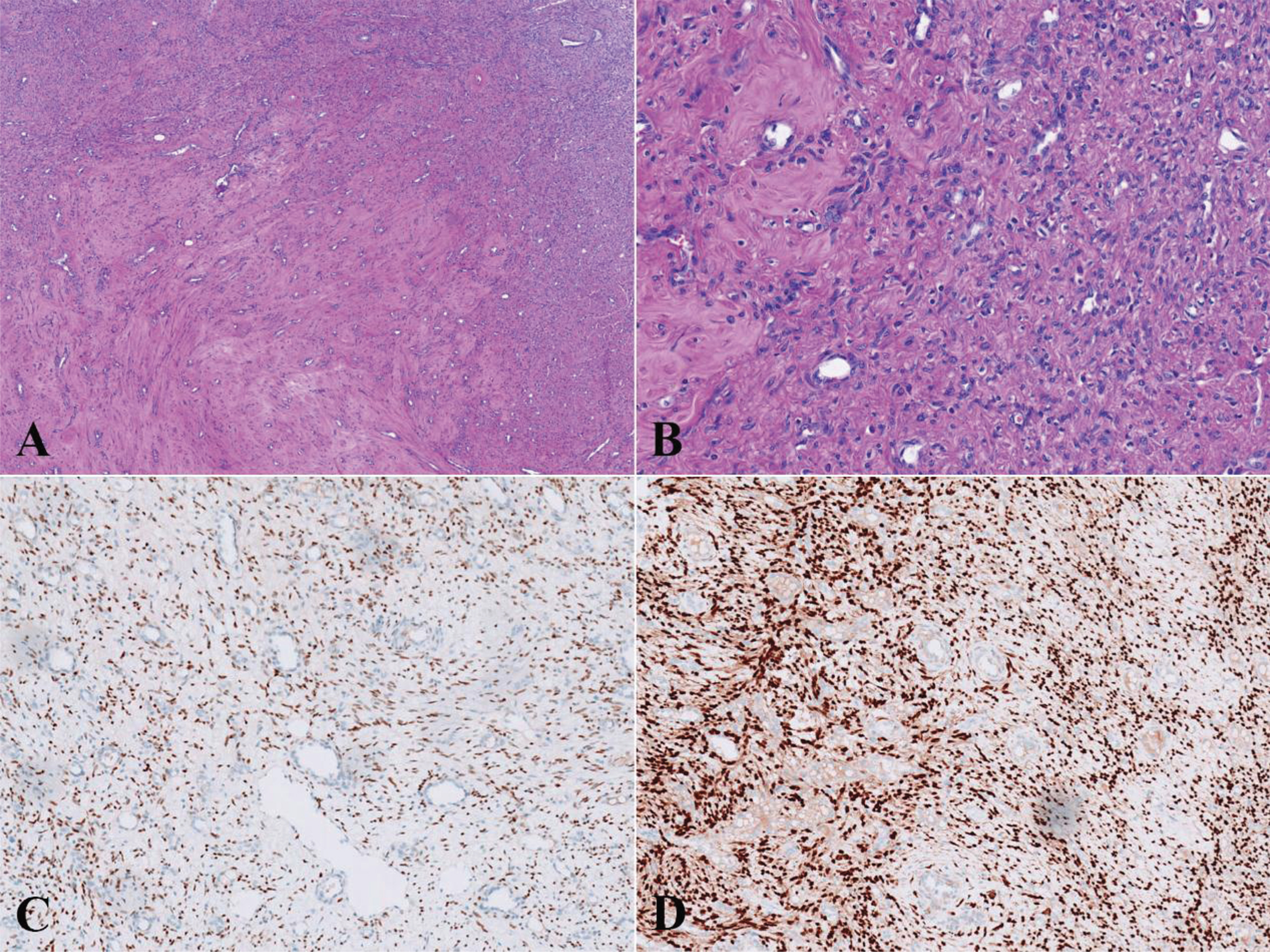
Microscopically, the tumor and thrombus were composed of proliferative spindle cells with tubular structures distributing among the spindle cells (A, hematoxylin and eosin×4; B, hematoxylin and eosin×20). Immunohistochemically, the spindle cells were positive for ER (C, immunohistochemistry×10) and progesterone receptors PR (D, immunohistochemistry×10).
In our case, the patient was a perimenopausal women belonging to the high-risk groups of MESTK, and the tumor possessed the typical cellular morphology and immunohistochemical characteristics of MESTK. What makes it distinct is that the tumor appeared to be grossly solid and was predominately composed of stroma. In addition, it was complicated with renal vein and inferior vena cava tumor thrombus, which is unusual for benign tumors. We presume the thrombus was the result of the predominance of stromal component, which consisted of a marked cell proliferation, but further studies are needed to testify this assumption.
It is difficult to establish a precise diagnosis of MESTK preoperatively due to lack of any distinct clinical and imaging findings. MESTK must be differentiated from several entities. For most MESTK has cystic architecture, other cystic lesions of the kidney should be considered, such as multilocular cystic renal cell carcinoma, cystic partially differentiated nephroblastoma and pediatric cystic nephroma. When composed of stroma predominantly, similar to our case, METSK should also be distinguished from other renal solid tumors, including renal cell carcinoma, urothelial carcinoma of the renal pelvis, liomyoma, angioleiomyolipoma, epithelioid angiomyolipoma, congenital mesoblastic nephroma, and metanephric adenofibroma. The differential diagnosis of malignant MESTK includes leiomyosarcoma, synovial sarcoma and sarcomatoid renal cell carcinoma. In the diagnostic process of this case, the most important and difficult part is to exclude the urothelial carcinoma of the renal pelvis, for the mass was located in the renal sinus, and the operation scope and adjuvant treatment are quite different from that of renal tumors. Urine exfoliative cytology, FISH and flexible ureterorenoscopy detected nothing abnormal, so we conducted a needle biopsy. However, the pathological findings from the needle biopsy misled us to an incorrect preoperative diagnosis as liomyomaand, as a result of the tumor’s predominance of stromal component.
Partial or radical nephrectomy according to the patient’s condition is the suggested treatment of MESTK. No matter which surgical method is chosen, complete resection of the tumor must be emphasized, as positive surgical margins and tumor spillage during resection are presumably risk factors for local recurrence. Farias et al. [27] reported a case of benign MESTK that locally recurred complicating peritoneal seeding 3 years after the initial surgery because of incomplete resection. Another case has been reported that a complex renal cystic mass treated with robotic decortication recurred 2 years later, which then underwent a partial nephrectomy and turned out to be benign MESTK [28]. In a case of malignant MESTK, the tumor ruptured during surgery and was removed in fragments, and extensive recurrence was confirmed just 4 months later [23]. Thus, when a partial nephrectomy is performed, an intraoperative frozen section is helpful to exclude a positive margin. Additionally, preoperative biopsy should be conservative, which was conducted in our case though, for it may cause the cysts to rupture and increase the risk of recurrence.
If the tumors are resected completely and confirmed to be benign, patients can achieve favorable prognosis. In the largest reported series by Michal et al. [11], they followed up 22 cases of benign MESTK for 3–8 years postoperatively, and all patients were alive and well without evidence of local recurrence or distal metastasis. However once the pathological diagnosis is malignant, the prognosis is poor even leading to a fatal outcome. All the 15 patients of malignant MESTK mentioned above received radical nephrectomy, but 7 patients recurred afterwards (recurrence rate: 46.7%, disease-free survival: 2–24 months and 9.5 months average), including three patients with distal metastasis. 4 of the recurrent died with postoperative survival time ranging from 5 to 43 months (18 months average). There are no established guidelines on the treatment of recurrent or metastatic MESTK, and adjuvant chemotherapy or radiotherapy might be needed in selected cases. In our case the tumor was resected completely and confirmed to be benign pathologically, but it was complicated with neoplastic thrombus. Although no recurrence or metastasis was found 12 months after the surgery, more longitudinal follow-up is required to determine whether it possesses aggressive behavior.
Conclusion
MESTK is a rare renal tumor, which should be considered as a possible diagnosis in cases of cystic renal mass, especially in perimenopausal women or those having a history of long-term oral contraceptive use. Our report demonstrates that MESTK can also appears solid in imaging in some uncommon cases, which means the tumor is composed of stroma predominately. And it is possible to be complicated with renal vein and inferior vena cava tumor thrombus, even though the tumor is benign. Documentation with more cases of MESTK is needed to further understand its pathogenesis, biological behavior, preoperative diagnosis and optimal management of patient treatment.
Footnotes
Acknowledgments
The authors received no financial support for the research, authorship, and/or publication of this article.