
Abstract
Horseshoe kidney deformity with duplex urinary collecting systems is a rare congenital urinary tract defect. Clinically, it is very difficult to visually observe and examine the whole anatomic structure and information with the regular 2D diagnostic imaging tools. Here, we report a case in which a middle age patient has bilateral duplex urinary collecting systems and horseshoe kidney deformity accompanied with right renal ureteral calculi and hydronephrosis. It was diagnosed by magnetic resonance urography with urinary system 3D reconstruction. The imaging and display method provides valuable information about abnormal anatomic structures of the kidneys and the related stone diseases for preoperative planning.
Introduction
About 1/500 of children are born with horseshoe kidney. It occurs while baby is in utero. The kidneys fuse together forming a “U” shape. As urinary system is abnormal, calculi in urinary collecting systemic and hydronephrosis often exist. A rare case with horseshoe kidney deformity with duplex urinary collecting systems, right renal ureteral calculi and hydronephrosis confirmed by magnetic resonance imaging (MRI) scan and magnetic resonance urography (MRU) with 3D reconstruction was reported in this study. Several types of surgeries were performed before and stones were removed by flexible ureteroscopic lithotripsy. We concluded that MRI scan and MRU with 3D reconstruction provide an optimal image tool in its diagnosis, prognosis and in evaluation of treatment for diseases in urinary tract system.
Patient and methods
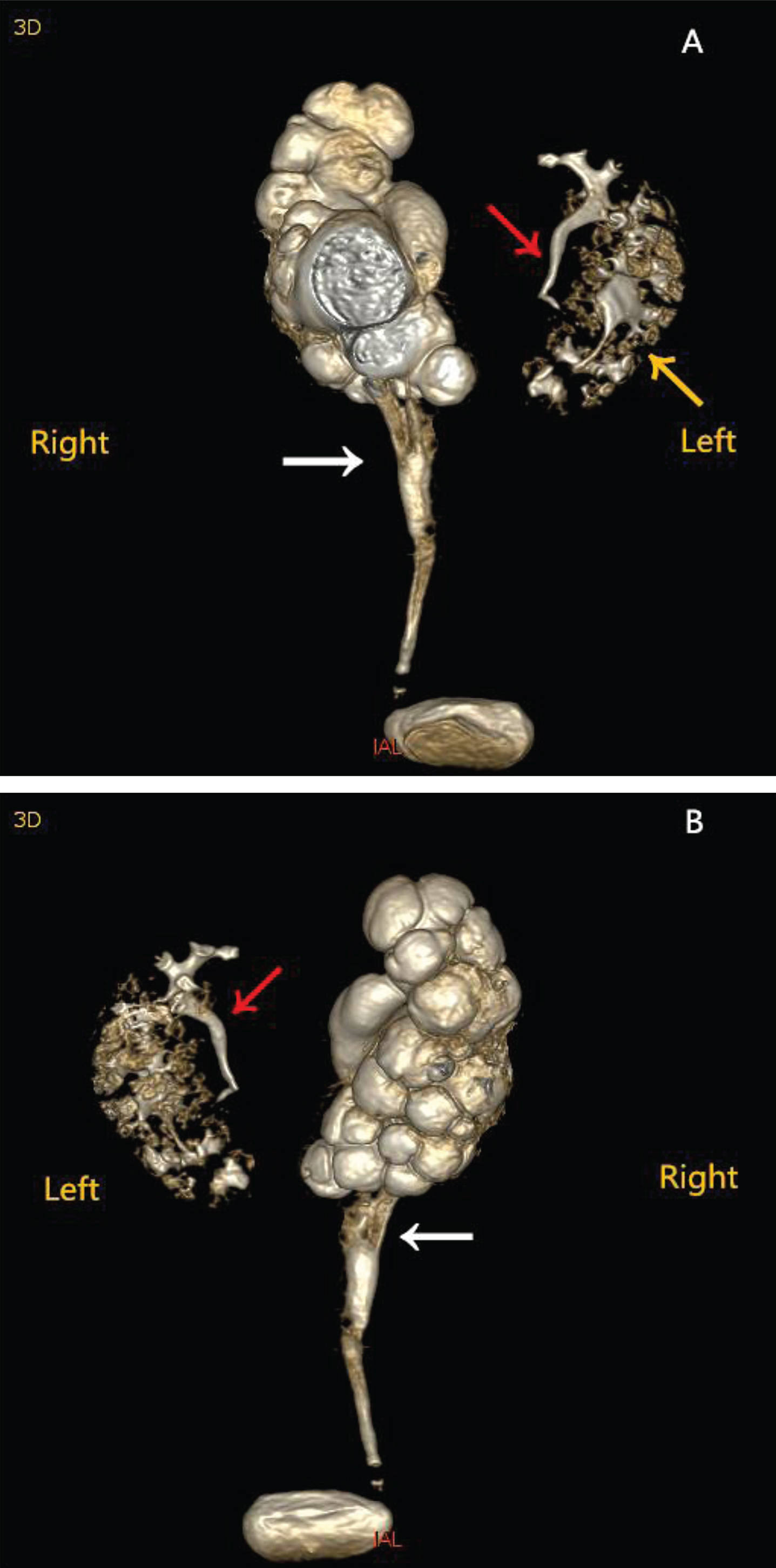
A 41-year-old male patient complained of bilateral renal area painful discomfort for about 20 years. The patient was treated with extracorporeal shock wave lithotripsy and then an open surgery for bilateral duplex kidneys and horseshoe kidney deformity accompanied with recurrent calculi on right ureter and hydronephrosis bilateral renal calculi 20 yeas ago, respectively. Magnetic resonance imaging (MRI) scan and magnetic resonance urography (MRU) with 3D reconstruction (3.0T Signa HDxt, America GE Medical Systems, LLC) showed that bilateral duplex kidneys and horseshoe kidney deformity accompanied with recurrent calculi on right ureter and hydronephrosis (Fig. 1-A, 1-B). The right side double ureters converged into a single one on the umbilical plane, presenting “Y” shape, while the left side the double ureters abnormally went into the urinary bladder directly. The right side of the urinary collecting system where multiple T2WI (T2 weighted image) signals were defected expanded significantly for demonstration, resulting to the renal cortical became thinner. Furthermore, funicular low signal area (1×3 cm) was detected near the end of the cavity of the right single ureter as “calculi street” formed by multiple small stones from the kidney. Compared to the right urinary collecting system, the expansions of left side double renal pelvises were hardly to be detected. Interestingly, the bilateral inferior extremity of kidneys amalgamated together ahead of abdominal aorta, presenting “horseshoe” shape (Fig. 2).
Demonstration of urinary system three-dimensional (3D) reconstruction. Illustration of the anterior position is as (A) showing. When rotating the 3D reconstruction 180 degrees, (B) was obtained, demonstrating the posterior position one. The white arrow indicates the right side “Y” shape converged and expanded ureter from single ones. The left side upper single ureter and lower single ureter are marked by the red arrow and yellow ureter respectively.
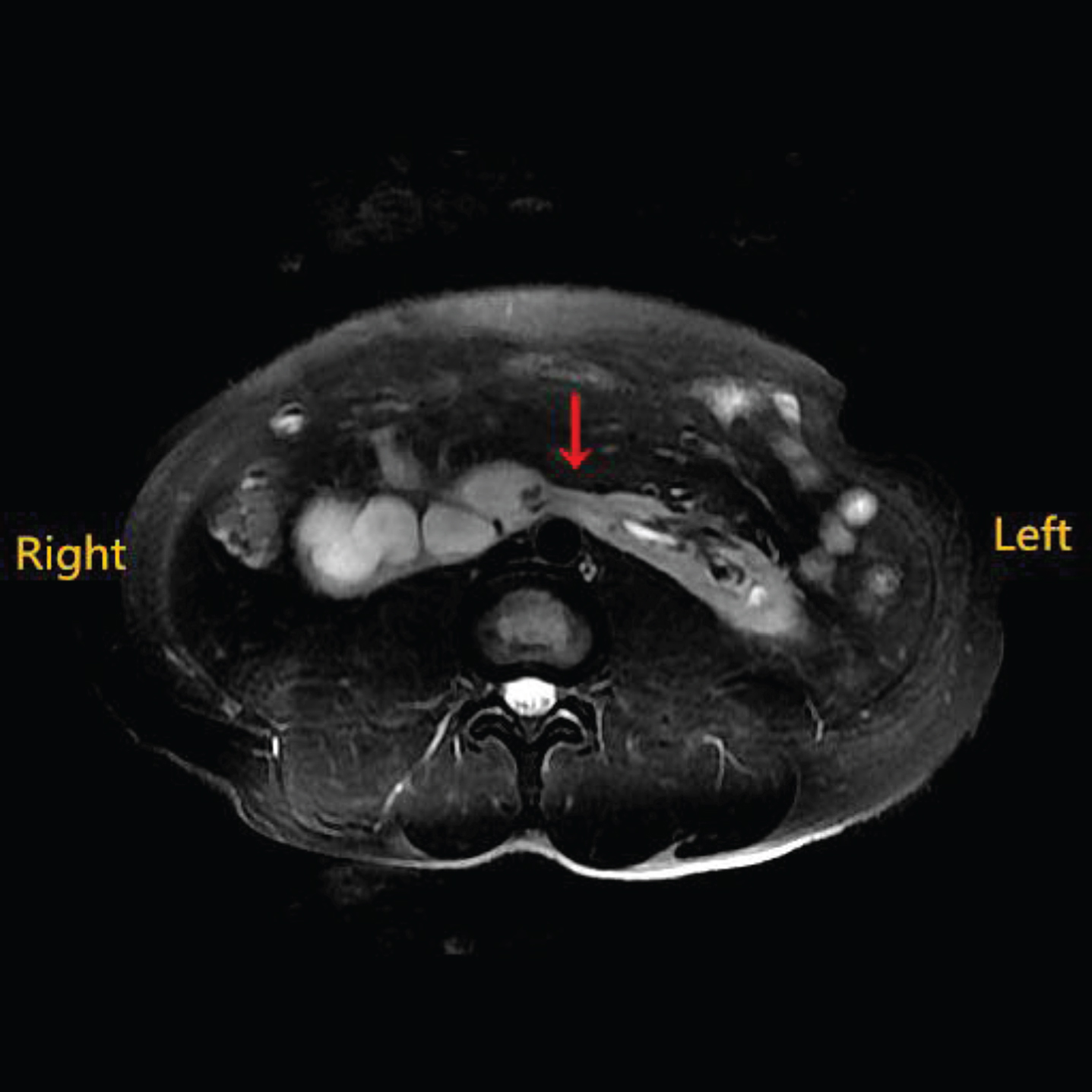
This axial abdominal scan of MRI shows complete fusion of the lower poles of the kidneys with a clear isthmus marked by the red arrow.
Dynamic renography showed that glomerular filtration rate (GFR) of right kidney significantly decreased at 25 ml/min (normal arrange: 40–60 ml/min), compared to 57 ml/min on left kidney. The laboratory urinalysis uncovered that the patient had the presence of a severe infection in the urinary tract, as did the blood cell analysis. Gram-positive organism Enterococcus faecalis was detected in culture urine specimen, which was sensitive to ampicillin. After 7 days’ treatment of sensitive antibiotics, the patient had flexible ureteroscopic lithotripsy. And the right ureteral stone was completely removed. The patient made an uneventful recovery with residual renal function (left: 57 ml/min, right: 38 ml/min) at the 2-year follow-up.
Duplication of the ureter and renal pelvis is the most common upper urinary tract anomaly with a reported incidence of 2% [1]. The duplication is classified as incomplete or complete type [2]. The prevalence of partial duplication is 0.6%, while complete duplication of the ureters occurs in only 0.2% of live births [2]. Partial patients were diagnosed when having clinical performances in adulthood. Horseshoe kidney is another type of urinary congenital defects occurring 1/400 of the general population [3]. Renal parenchyma or fibrous tissue or minority collection system of each lateral kidney fuses at lower poles of kidneys across the midline. Due to the altered anatomy, the urinary drainage is affected and thereby increasing the risk of urinary tract infections and renal stone formation in up to 20% of cases [4], so was the presented case accompanied with duplication of the ureter and renal pelvis. Rare cases of duplication of the ureter and renal pelvis accompanied with horseshoe shaped kidney were reported previously [5, 6]. In the cases, a deformed system was associated with other renal complications such as obstruction, reflux, and infection because of weaken anti-regurgitation urodynamics effects in abnormal shape urinary system.
Duplication of the ureter and renal pelvis or the horseshoe kidney is caused by the factors of genetics and environmental elements. Rodriguez et al. [2] reported that 20 families (66%) had affected first-degree relatives in 30 cases as an incomplete duplication was included as a variant of a duplex system. Usually, only one of the parents was affected, the mode of inheritance was established as dominant abnormal. Bilateral duplex urinary collecting systems accompanied with horseshoe kidney deformity is a rare entity.
Magnetic resonance hydrography (MRU) is a powerful modality without the unique utilization of X-ray radiation. It mainly uses the characteristics of water within long T2 relaxation time and fuses anatomic information data in a single test for evaluating the morphology of the tracts containing water components, such as cerebrospinal fluid, lymph, stomach and intestinal juice, bile and urine [7]. MRU and magnetic resonance cholangiopancreatography (MRCP) are widely utilized to examine and diagnose the correlated anatomic tract systems.
MRU is applied to detect the obstruction which is hardly positioned clearly and congenital malformation of urinary system with high sensitivity and accuracy, particularly in children and adults those who are of poor renal function and pregnancy than computed tomography urography (CTU) [8, 9]. Advantages and disadvantages on imaging diagnostic techniques, including ultrasonography, CTU, MRU and IVU of unary system deformities are summered in Table 1. MRU has advantages over other modalities as it generates tissue contrast from a variety of sources. It also can detect the anatomical consequences of vesicoureteric reflux in terms of dilated ureters, distorted anatomy of the collecting system and renal scarring, and the functional consequences of renal scarring. In addition, MRU creates a 3D T2 urogram with concise and precise to stereoscopically observe the pathologic morphology of urinary collecting system [10, 11]. Therefore, MRU provides a more complete characterization of renal anatomy and pathophysiology in urinary collecting system in this case.
Advantages and disadvantages on imaging diagnostic techniques of unary system deformities
However, the traditional unenhanced MRU is sensitive to urinary tract morphology of obstruction and dilation, but sensitive for renal function evaluation, so was that in this case [11]. The utilization of dynamic contrast-enhanced MRI for the evaluation of renal function has been undergoing development. It shows promise for providing new insights into the evaluation of renal structure and function in relation to important disease processes, including deformity in urinary tract system [12], although it is a relatively complex course and software is proved to be a limiting factor in widespread routine implementation. Whereas, new technological means depicted on functional MRU imaging could be expected in the near future.
Conflicts of interest
There are no conflicts of interest.