
Abstract
Introduction
Endometriosis is a benign estrogen-dependent inflammatory disorder characterized by the presence of endometrial-like tissue outside the uterus (ectopic) [1], which has been classified as a tumor-like condition by the World Health Organization Histologic Classification of Ovarian Tumors, affecting 6% –10% of women of childbearing age [2]. 40% –60% of patients with endometriosis are infertile and display low pregnancy rate [3]. This is mainly caused by inadequate receptivity of ectopic endometrium, i.e. embryos fail to adhere or anchor to the endometrial basal lamina and stromal extracellular matrix in women with endometriosis. However, the etiopathology of endometriosis remains elusive. Hence, identification of molecular differences between the endometrium of women with endometriosis and that of disease-free women is an important step toward understanding the pathogenesis of this disease and developing novel strategies for diagnosis and treatment.
MicroRNAs (miRNAs) are short non-coding RNA molecules, usually consisting of 18–30 nucleotides, generally acting as negative gene regulators by mRNA cleavage or translational repression. It has been demonstrated that all these mechanisms responsible for endometriosis development can be regulated by miRNAs including proliferation [4, 5], matrix remodeling [6–10], cell survival [11, 12] and angiogenesis [13–16]. miRNA expression differences between endometriotic lesions and eutopic endometrium from women with endometriosis have been reported [17, 18]. miRNA are potent regulators in a broad array of cellular processes that occur in endometriosis and are emerging as potent biomarkers and therapeutic agents for this condition. Therefore, it would be interesting to know the differentially expressed miRNAs in endometriosis and their associations with the reduced endometrial receptivity in these patients.
In this study, we compared the miRNA expression profiling between women with endometriosis and endometriosis-free women to screen for abnormally expressed miRNAs in endometriosis. Eight women with endometriosis were enrolled for the study and the control group consists of 6 infertile patients who are endomteriosis-free but with defects from fallopian tubes. DNA from endometrium of midluteal phase (MLP) were sequenced with 20M each sample. Bioinformatic analysis revealed the differentially expressed miRNAs and identified their downstream target genes and pathways that are likely contribute to the pathogenesis of endometriosis. Hence our finding shed new lights on future research into the role of miRNAs in this disease. Ultrasound is a widely used imaging modality in the clinical practice [19] including the evaluation of the endometrial receptivity [20]. This study aims to investigate the microRNA expression profiling in endometriosis-associate infertility, and the relationship between the microRNA expression and endometrial receptivity evaluated by ultrasound.
Patients and methods
Patients and tissue samples
A total of fourteen infertile patients were recruited from Shenzhen Second People’s Hospital (Shenzhen, Guangdong, China) during June 1, 2015 to August 31, 2015. All patients have provided informed consent for participation in this study. Authors had access to information that could identify individual participants during or after data collection. The research protocol was approved by the ethics committee/institutional review board of the Shenzhen Second People’s Hospital. All the patients of control group, in which infertility is only caused by fallopian tube occlusion, and they were surgically confirmed endometriosis-free. Eight patients, namely Case-1, 2, 3, 4, 5, 6, 7 and 8, were diagnosed as endometriosis with normal fallopian tube. Endometium tissues were collected at surgery, frozen in liquid nitrogen and stored at –80 °C. Fourteen women with endometriosis and 10 women with non-endometriotic infertility as controls between September 1, 2015 and December 31, 2015 were selected for the validation of different expression miRNAs. And then we evaluated the endometrial receptivity by ultrasound for other 20 infertility patients. And divided the 20 patients into two groups: 12 endometriosis-free patients with high endometrial receptivity, in which infertility is caused by fallopian tube occlusion, and 8 endometriosis patients with low endometrial receptivity (Fig. 1). Compare the endometrial miRNAs expression between the 2 groups, and evaluated the relationship between the endometrial miRNAs expression and the endometrial receptivity. In this study, the choice of all endometriosis patients was belong to mild or moderate type.
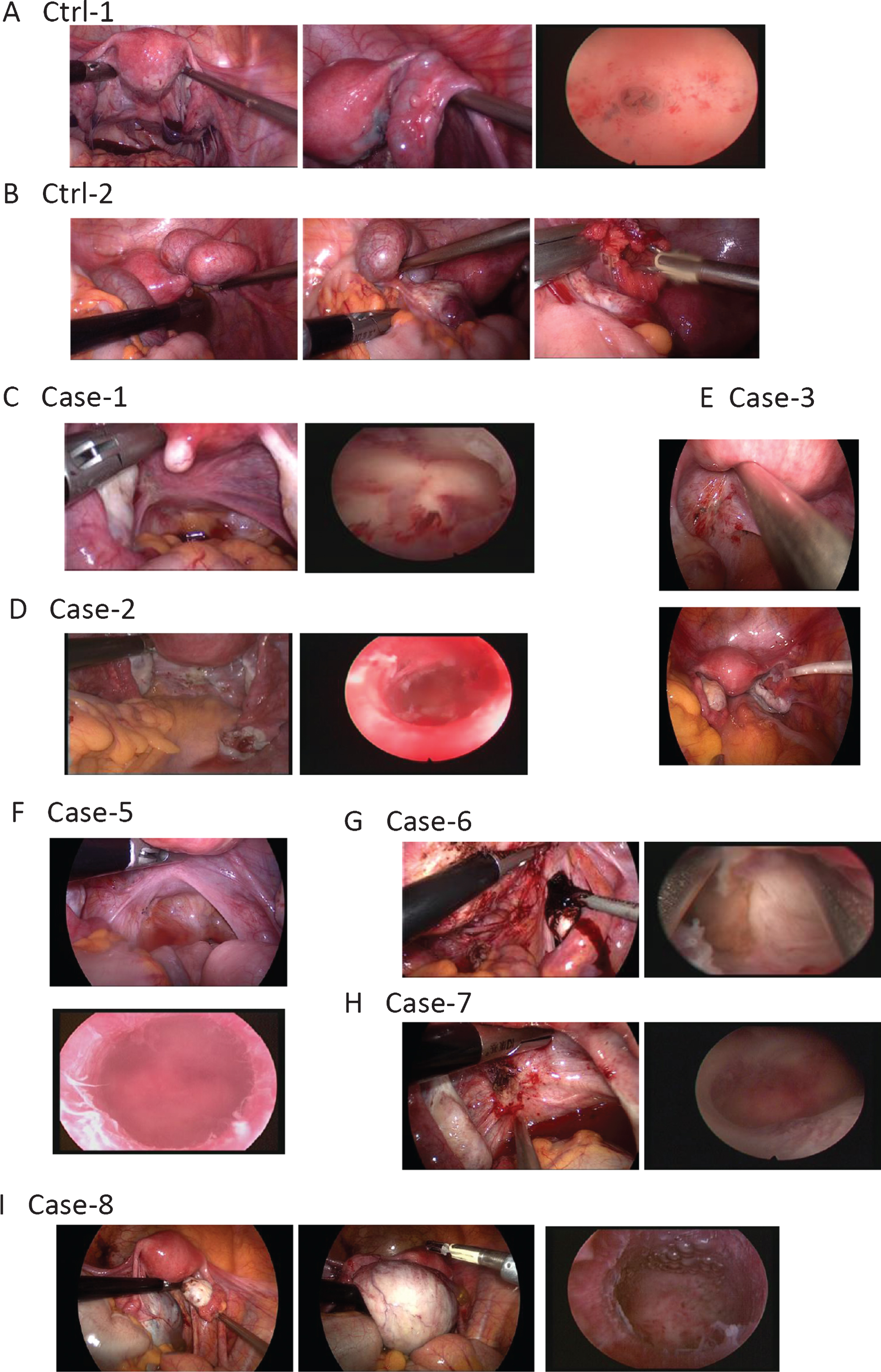
Representative photos of ectopic endometrial lesions taken at surgery. (A) Infertility in Ctrl-1 patient was caused by fallopian tube occlusion at the left side. The left and middle pictures are laparoscopic photos showing the uterus and bilateral adnexa. The right picture is a hysteroscopy photo showing endometrium. (B) Infertility of Ctrl-2 patient was caused by bilateral hydrosalpinx. (C) Endometriosis in Case-1 patient. Left picture shows endometriosis lesions scattered around uterosacral ligaments. The right picture is a photo of the endometrium in the luteal phase of the menstrual cycle of the patient. (D) Case-2 patient had endometriosis. The black spots in the left picture shows lesions of pelvic endometriosis. Right picture shows the endometrium in the luteal phase of the menstrual cycle of the patient. (E) Case-3 patient had mild endometrial endometriosis. Pelvic lesion spots of endometriosis were shown in the upper picture. The lower picture is an overview of uterine adnexa after endometriosis burning treatment. (F) Case-5 patient was diagnosed with pelvic endometriosis. Ectopic endometriosis had migrated to Douglas lacuna. Lesions were seen as the dark spots. (G) Endometriosis in Case-6 patient. Left picture shows chocolate cyst of ovary. Right picture is a photo of the endometrium in the luteal phase of the menstrual cycle of the patient. (H) Case-7 patient had pelvic endometriosis, which had migrated to Douglas lacuna. Dark brown spots in the left pictures shows lesions of endometriosis. (I) Case-8 patient had multiple endometriosis. The left and middle pictures show the lesion spots of the endometriosis in bilateral ovaries. The right picture is a photo of the endometrium in the luteal phase of the menstrual cycle of the patient.
Total RNA was extracted using Trizol Reagent (Invitrogen, CA) from ten samples, and passed the RNA QC for sequencing. The quality and integrity of total RNA was assessed with Agilent 2100 Bioanalyzer (Agilent Technologies, USA) [21]. RNA segments of different sizes were separated using PAGE gel and strips between 18 and 30 nucleotides were cut out. Lastly, library quality was assessed by Agilent 2100 Bioanalyzer using DNA High Sensitivity Chips. These libraries were then sequenced on an Illumina Hiseq 2000 platform (Illumina, BGI, Shenzhen) and 50nt single-end reads were generated.
Data analysis
High quality clean read sequences were screened by the alignment to NCBI GenBank data UCSC hg19 (ftp://ftp.ncbi.nlm.nih.gov/genbank/) and miRBase 21.0 (http://www.mirbase.org/ftp.shtml) for the further analysis. The raw data was submitted to NCBI under BioProject accession No.SRP076962. DEGseq [22] was applied to identify miRNAs differentially expressed between two groups. Q-value ≤ 0.001 and | log2 fold change | ≥ 1 were set as the cut-offs to screen out differentially expressed miRNAs.
The expression levels of differentially expressed miRNAs screened by the above experiment were determined by reverse transcription-polymerase chain reaction (RT-PCR) in the two groups (14 in the endometriosis group and 10 in the control group, respectively). The miRNA microarray were selected to check the results.
Ultrasonographic evaluation of endometriosis endometrial receptivity: recorded the endometrial thickness in the expected ovulation time, which will be divided into two types according to the endometrial morphology: A-type and B-type. In the type A, 3 clear hyperechoic line (three-line sign) was visible in endometrium, which suggested high endometrial receptivity; the endometrial midline of the B-type was less clear or homogeneous, the lack of intermediate high-echo line, which suggested that endometrial receptivity was low. (Fig. 2).
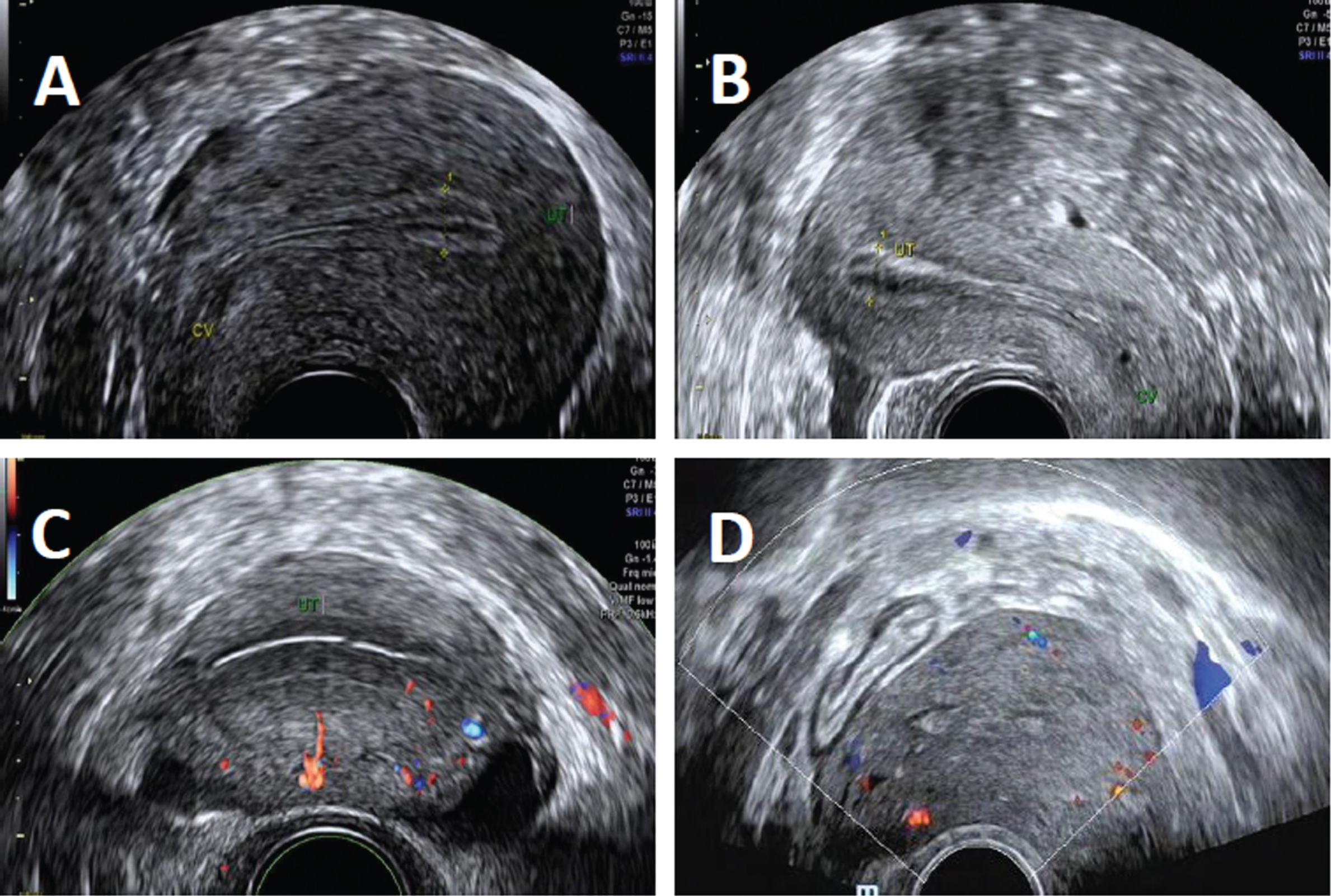
A (Longitudinal section) and C (Cross section): 3 clear hyperechoic line was visible in endometrium, which suggested high endometrial receptivity; B (Longitudinal section) and D (Cross section): the endometrial midline was less clear, the lack of intermediate high-echo line, which suggested low endometrial receptivity.
To screen out the possibility of endometrial receptivity related miRNA from the differentially expressed miRNA, at the same time 20 patients were selected, of which the endometrial receptivity was assessed and divided into two types by ultrasonography detecting the morphology of the endometrium (12 patients with good endometrial receptivity, in which infertility is caused by fallopian tube occlusion as control group, and 8 endometriosis patients with bad endometrial receptivity as experimental group). To detect the different expression levels of the expressed miRNA by RT-PCR in the endometrium in the luteal phase of the two types of patients, high or low endometrial receptivity. According to the results, to analysis the possible that endometrial receptivity may be related to miRNA, and further explore the mechanism of endometriosis infertility. Especially, all the clinical samples data are store in remote medical cloud database for retrieving and analyzing.
First, endometrial biopsy specimens were obtained from eight midreproductive-aged infertile women with endometriosis and six endometriosis-free infertile women, which are the controls. The ages of these women ranged from 30 to 36 yr in the control group (mean age, 33.05±4.24) and 27 to 41 yr in the patient group (mean age, 32.88±4.52) (Table 1). Statistical analysis revealed no significant difference between these two groups. All the 8 patients in the endometriosis group have regular menstruation except case-4. Case-2, 5, 6 and 8 have pelvic endometriosis. Ctrl-1, 2 and 3 patients had polycystic ovary syndrome, uterine and pelvic adhesion and fallopian tube occlusion. Ctrl-4, 5 and 6 patients had primary sterility, displaying hydrosalpinx, pelvic adhesion and mesosalpinx cyst. Review of pathology reports revealed no evidence of inflammation or abnormality within the endometrium of women without endometriosis.
Patient characteristics in two groups
Patient characteristics in two groups
Second, the study found that in the top ten affected known miRNAs (Table 2), 6 are up-regulated (miR-1304-3p, miR-544b, miR-3684, miR-494-5p, miR-4683 and miR-6747-3p) and 4 are down-regulated (miR-3935, miR-4427, miR-652-5p and miR-205-5p). Three up-regulated miRNAs hsa-miR-1304-3p, hsa-miR-544b and hsa-miR-3684 are not expressed in the control group and two down-regulated miRNAs hsa-miR-3935 and hsa-miR-4427 are not detected in the patient group, suggesting that these five miRNAs are likely associated with endometriosis. Interestingly, these top ten DE miRNAs, which are changed by at least four folds, have not been reported associated with endometriosis [23–25]. miR-483-5p [23], miR-20a-5p and miR-17-5p [23] are slightly down-regulated by log2 fold change > –1 compared with controls, which is different to previous reports. Notably, miR-9-5p and miR-34c-5p [23] were found down-regulated in endometriosis patients, however they are slightly up-regulated in our findings, indicating that they are less likely associated with endometriosis.
Differentially expressed known miRNAs (|log2Ratio (Case/Control) |>2)
Third, expression level of endometrial tissue on Luteal phase was checked by RT-PCR, as shown in Table 3. The expression level of miR-1304-3p, miR-544b, miR-3684, miR-494-5p, miR-4683 and miR-6747-3p in endometriosis group were higher than that in control group. The difference between the two groups was statistically significant (P < 0.05). The expression level of miR-3935, miR-4427, miR-652-5p and miR-205-5p in endometriosis group were lower than that in control group. The difference between the two groups was statistically significant (P < 0.05).
miRNA level differences between endometriosis and control group checked by RT-PCR
Last, miRNA level differences between high endometrial receptivity group and low endometrial receptivity group, as shown in Table 4. The expression levels of miR-1304-3p, miR-494-5p, and miR-4427 were different between the two groups. Suggesting that these miRNAs may be associated with changes in endometriosis receptivity, but for the miR-544b, there was no statistical difference between the two groups.
miRNA level differences between high endometrial receptivity group and low endometrial receptivity group
Endometriosis is an emerging public health problem of reproductive-age women. It is associated with persistent pelvic pain and/or infertility, but the pathogenesis of this condition remains elusive. Previous studies have raised miRNAs as important regulators of genes and pathways involved in the development of endometriosis. Endometriosis is a common gynecological disorder, but its exact eptiopahtogenic mechanism remains unsolved. Nowadays, as research continues, the most accepted theory is Sampson’s retrograde menstruation proposal, which proposed that during menstruation, endometrial fragments could migrate through fallopian tubes and reach the peritoneum, being capable to attach, survive, and implant at different locations [1, 26]. Endometriosis is very difficult to diagnose without surgical assessment, as the symptoms of reduced fertility and the variety of associated pain are not specific for endometriosis itself. The current gold standard for the diagnosis of endometriosis is laparoscopic examination with histological confirmation of glands and/or stroma in the excised lesions [27]. Non-invasive nor a minimally invasive test has not been achieved, and an ideal test for diagnosis of endometriosis should diagnose patients at initial stages with high sensitivity and specificity. Considering that endometrium can be easily and non-invasively collected, searching for biomarkers of endometriosis becomes a hotspot of research interests nowadays.
Next Generation Sequencing (NGS) was initially developed for sequencing human genome faster, cheaper and deeper. The ability to read millions of short fragments of DNA soon prompted the generation of a new methodology, RNA-seq, which includes RNA sequencing and quantification. Accompanying with the further development of bioinformatic software and sequencing cost reduction, miRNA sequencing projects are performed widely and deeply, including ENCODE (http://www.genome.gov/encode/), focusing on defining RNA transcripts, transcriptional regulator binding sites, and chromatin states in many cell types by different approaches, ncRNAPain (http://www.ncrna-pain.eu/) for personalized pain medicine, CORDIS (http://cordis.europa.eu/project/rcn/110362_en.html) for studying on ncRNA-derived diagnostic and therapeutic tools, etc. Here, through RNA-sequencing of endometriotic endometrium and eutopic endometrium of non-endometriosis patients, we screened abnormally expressed miRNAs in endometriosis patients and did functional analyses of their targets and the downstream pathways.
Previously genome-wide studies have identified a large number of miRNA transcripts differentially expressed in the eutopic endometrium of women with and without endometriosis [28, 29] and between ectopic and eutopic endometrial samples from the same women [30], including miR-200a/b/c, miR-34c-5p, miR-9, miR23a, miR-23b etc. miRNA-200 family showed the highest potential as noninvasive biomarker for endometriosis, since they are significantly downregulated in evening plasma samples of patients compared with that of surgically confirmed disease-free patients [31]. Shen et al. demonstrated that compared with normal endometrium, miR23a and miR23b were down-regulated in ectopic endometrium, leading to the aberrant SF-1 expression in endometriotic stromal cells [32]. In our study, we have found a total of 57 novel miRNAs and 61 known miRNAs that are differentially expressed in the ectopic endometriosis. We did not observe overlapped DE miRNAs between our sample and previous samples [18], which could owes to many factors, such as heterogeneity of endometriosis among the recruited patients and their clinical treatments, as well as the patient population size, etc. Furthermore, future work would focus on validation of these differently expressed miRNAs by quantitative PCR in patients with endometriosis and disease-free patients.
Recent studies have indicated that the embryo implantation barrier based on the decreased endometrial receptivity is one of the important reasons of endometriosis infertility. Endometrial receptivity (ER) refers during the pre-implantation of embryo period, the endometrium experiences a series of changes under the regulation of hormones, cytokines, adhesion molecules and glycoproteins and other factors and reaches to the state of the embryo implantation, including the thickness of the endometrium, luminal epithelium, interstitial development, glandular epithelium and endometrial blood supply status. The evaluation of endometrial receptivity has an extremely important role. Ultrasound imaging can measure the endometrial thickness, endometrial type, uterine artery and endometrial blood flow of endometrial blood flow to detect the endometrial receptivity.
The literatures show that miR-199a, miR-135a, miR-135b, and miR-21 are all associated with endometrial receptivity, which was possibly associated with endometriosis. As a regulator of post-transcriptional level, miRNAs regulate the degradation of target genes and inhibit the translation of proteins in endometrial receptivity. It has been demonstrated that many target genes of some miRNAs are markers of endometrial receptivity including leukemia inhibitory factor, signal transducer and activator of transcription 3, cyclooxygenase 2, prostaglandins; cognate box gene AIO, prolactin, transforming growth factor p1, matrix metalloproteinase, Kazal motif containing reversal induced cysteine-rich protein and tissue inhibitor of metalloproteinase 3 and so on. These genes interact through complex regulatory pathways to participate in the establishment and maintenance of endometrial receptivity.
Combined with the results of this genetic sequencing, Targetscan database prediction results and related literature research, it was predicted that miR-544b, miR-494-5p and miR-4427 can act on the gene corresponding to HOX10, LIF, ITGB3, OPN, ESR, PGR, ITGAV, CDH1 and MMP and other receptors of endometrial markers. In this study, we selected the following miRNA as the research object namely, miR-544b, miR-494-5p, miR-4427. Ultrasonography was used to evaluate the endometrial receptivity, and then the differences of expression level of these miRNAs in the luteal phase were analyzed. The statistical results were significant, suggesting that these miRNA may be involved in endometrial receptivity changes of endometriosis in the mechanism, which is one of infertility reasons.
Conclusions
Taken together, our findings in this study constitute a comprehensive foundation for future research into the role of miRNAs in endometriosis, and the relationship between it and the endometrial receptivity. Nevertheless, considering the heterogeneity of endometriosis, it would be of great interest to screen for DE miRNAs of endometriosis in a larger patient cohort and perform functional studies to confirm their specific targets, which will facilitate the understanding the pathogenesis and development of novel strategies for the clinical diagnosis and treatment of endometriosis. The combination of ultrasound and miRNAs detection will be better for the diagnosis of infertility in the future. The other future work is to further explore the mechanisms and roles of miRNAs in altering endometrial receptivity. In a word, the result of this study will be helpful for the research about infertility in the future.
Conflict of interest
None of the authors have potential conflicts of interest to be disclosed.
Footnotes
Acknowledgments
This study received financial support from Shenzhen Science and Technology Project (project number JCYJ20140414170821311 and JCYJ20140414170821323).