
Abstract
BACKGROUND:
Percutaneous coronary intervention (PCI) is the recommended treatment for high risk patients with non-ST-segment elevation myocardial infarction (NSTEMI).
OBJECTIVE:
To investigate the application of three dimensional-speckle tracking imaging (3D-STI) on patients diagnosed with NSTEMI undergoing PCI.
METHODS:
Forty-four NSTEMI patients and 20 healthy subjects that received basic clinical and laboratory examinations were included in our study. NSTEMI patients were divided into three groups: heart failure (HF) with normal ejection fraction (HF-NEF group, n = 19), heart failure with preserved ejection fraction (HF-PEF group, n = 14) and heart failure with a reduced ejection fraction (HF-REF group, n = 11). The global longitudinal peak systolic strain (GLS), global circumferential peak systolic strain (GCS), global radial peak systolic strain (GRS) and left ventricular (LV) torsion of all subjects were measured by 3D-STI before PCI and 1 month, 3 months after PCI. The high-sensitivity troponin T (hs-TNT), high-sensitivity C-reactive protein (hs-CRP) and N-terminal pro-brain natriuretic peptide (NT-pro BNP) were measured in each group. Correlations between these parameters and LV ejection fraction (LVEF) were tested by Pearson correlation analysis.
RESULTS:
GLS, GCS and torsion were significantly decreased in the 3 NSTEMI groups compared with control group (P < 0.05). GLS, torsion were significantly improved in the three NSTEMI groups at postoperative 1 and 3 months (P < 0.05). HF-REF group showed improved GCS on postoperative 1 and 3 month compared with preoperative data, and improved GLS at 3-month follow-up compared with 1-month follow-up (P < 0.05). The hs-TNT, hs-CRP and NT-pro BNP increased in the three NSTEMI groups before PCI (P < 0.05), and decreased at postoperative 1 and 3 month (P < 0.05). LVEF has the positive correlations with LV endsystolic volume (LVESV) and torsion, as well as the negative correlations with LVGLS, LVGCS, NT-pro BNP (P < 0.05).
CONCLUSIONS:
The combinative detection of 3D-STI and NT-pro BNP is an efficient way to assess the cardiac function in patients diagnosed with NSTEMI undergoing PCI.
Keywords
Introduction
Myocardial infarction, which defines as myocardial cell death caused by prolonged ischemia [1], is classified into ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI). Due to the electrocardiogram (ECG) results without ST-segment elevation or normal, it was often difficult to diagnose NSTEMI [2]. However as the presence of multiply sensitive biochemical markers, the diagnosis of NSTEMI has been gradually improved [3]. Currently, percutaneous coronary intervention (PCI) is the recommended treatment for high risk patients with NSTEMI according to guidelines [4]. Abundant researches indicated that a r96–+eduction in the incidence of cardiovascular death and myocardial infarction (MI) in the medium to long term. Therefore it is crucial to efficiently monitor the myocardium viability and cardiac function during periprocedural period in patients undergoing PCI.
The newly-developed three dimensional-speckle tracking imaging (3D-STI) is potential to track global and regional strain parameters in all dimensions simultaneously, circumventing the shortcomings of 2D-STE caused by plane-dependency. It also can accurately detect subclinical myocardial dysfunction. Previous study has presented the application of 3D-STI on patients with STEMI [5]. However 3D-STI has not reported with the predict value for left ventricular (LV) function changes in NSTEMI. This aim of the study is to investigate the application of 3D-STI on LV function changes of patients with NSTEMI undergoing PCI.
Materials and methods
Patients
The study was approved by the research ethics committee of Tianjin Chest Hospital and the consent forms were obtained from all the patients. Patients with NSTEMI undergoing PCI in Tianjin Chest Hospital from January 2016 to June 2016 were investigated in the study. The flow diagram of the participants was shown in Fig. 1. 44 NSTEMI patients and 20 healthy subjects that received basic clinical and laboratory examinations were included in our study. NSTEMI patients were divided into three groups: heart failure (HF) with normal ejection fraction (HF-NEF group, n = 19), heart failure with preserved ejection fraction (HF-PEF group, n = 14) and heart failure with a reduced ejection fraction (HF-REF group, n = 11). The basic characteristics are shown in Table 1 and there was no significant difference among the four groups (P > 0.05). All the patients were suffering from the first MI and first PCI. PCI would be conducted within 2–72 h after they were admitted to hospital. Patients with age >75 or <40 years old, ECG results with ST-segment elevation or pathological Q wave, severe hepatic and renal insufficiency, autoimmune disease, non-ischemic heart disease, valvular heart disease were excluded.
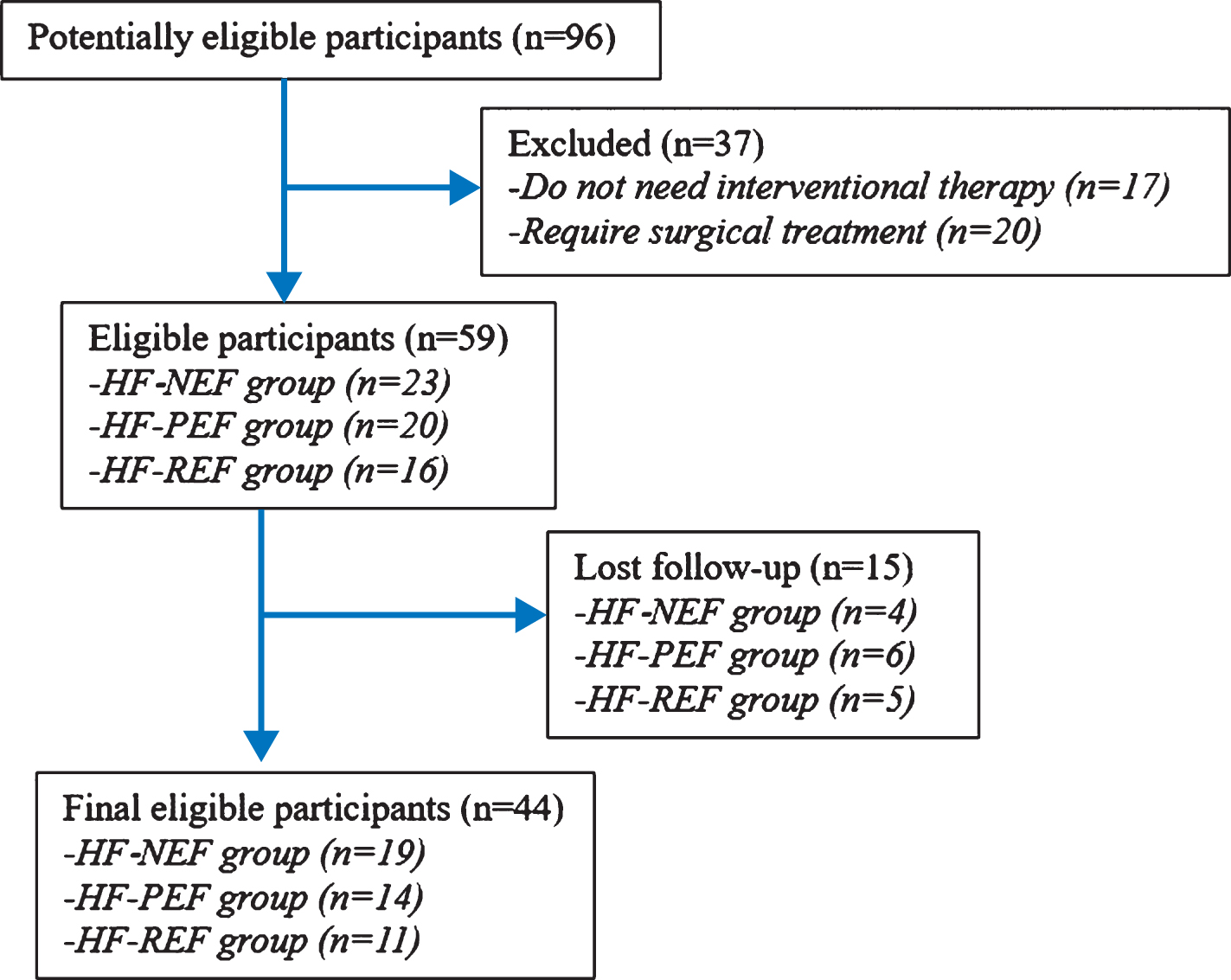
Flow diagram of the participants.
Basic characteristics in control and NSTEMI groups
Note: Data are presented as mean±standard deviation or number (percentage) as appropriate. TC: Serum total cholesterol; HDL: high density lipoprotein; LDL: low density lipoprotein.
The diagnosis of NSTEMI was based on American College of Cardiology/American Heart Association (ACC/AHA) guidelines [6]. The patients were retrospectively divided into normal ejection fraction (NEF) group, heart failure with preserved ejection fraction (HF-PEF) group, heart failure with reduced ejection fraction (HF-REF) group according to ESC guidelines [7]. Twenty healthy subjects were selected as the controls. They met the following inclusion criteria: no history of heart disease; normal physical examination, normal electrocardiogram and echocardiography results and no use of medication.
All subjects had a complete transthoracic echocardiogram to determine cardiac structure, chamber size, wall thickness and cardiac function according to the recommendations of the American Society of Echocardiography [8–10]. All studies were performed at rest without sedation. A commercially available system (iE33, Philips Medical Systems, Andover, MA) was used with S5, S8, or S10 broadband phased-array transducers, depending on the age of the subject. Subsequently, all subjects underwent 3D echocardiographic study using the same system with X5-1 transducer. Images were optimized to obtain the entire left ventricle in a full-volume data set in the apical four-chamber view. Data sets were acquired using a four heartbeat acquisition setting. End-expiratory breath holding was performed when feasible. A minimum of four data sets were acquired for each subject, and three best quality data sets were selected for offline analysis. Data sets that missed a portion of the left ventricle, had indistinct endocardial borders, or had significant stitch artifacts were excluded.
The software generates time-domain LV volume curves, from which the LV end-diastolic volume (LVEDV), endsystolic volume (LVESV) and LV ejection fraction (LVEF) were automatically determined. For 3D strain analysis, the left ventricle was divided into 16 segments using standard segmentation schemes. The software provided averaged longitudinal, circumferential, and radial strain time curves from each segment, from which peak global strain values [LV global longitudinal strain (LVGLS), and LV global circumferential strain (LVGCS), LV global radial strain (LVGRS) and LV torsion] were automatically obtained [11].
Three-dimensional echocardiographic full-volume data sets were stored on a hard disk for offline analysis. Offline 3D STI analysis was performed by two experienced investigators using vendor-independent 3D speckle-tracking software (4D LV Analysis version 3.1.2; TomTec Imaging Systems, Unterschleissheim, Germany) [12, 13]. Measurements were made using the dataset with the best image quality, which was selected by consensus of the two readers.
Assessment and follow-up
The basic clinical, laboratory indexes, 3D-STI parameters were observed on healthy subjects, and patients before PCI. High-sensitivity C-reactive protein (hs-CRP) was detected by automated immunoturbidimetric assay using the ADVIA Chemistry system (Siemens Healthcare Diagnostics Inc.) and high-sensitivity troponin T (hs-TNT) and N-terminal pro-brain natriuretic peptide (NT-proBNP) were assessed by electrochemiluminescence immunoassay using the Elecsys 2010 Immunoanalyzer (Roche Diagnostics, Indianapolis, IN, USA).
The patients would receive comprehensive medication treatments after PCI. At 1-month, 3-month follow-up, 3D-STI examination was repeated, hs-TNT, hs-CRP and NT-proBNP were reassessed. Typical preoperative and postoperative 3D-STI images obtained from a NSTEMI patient was shown in Fig. 2.
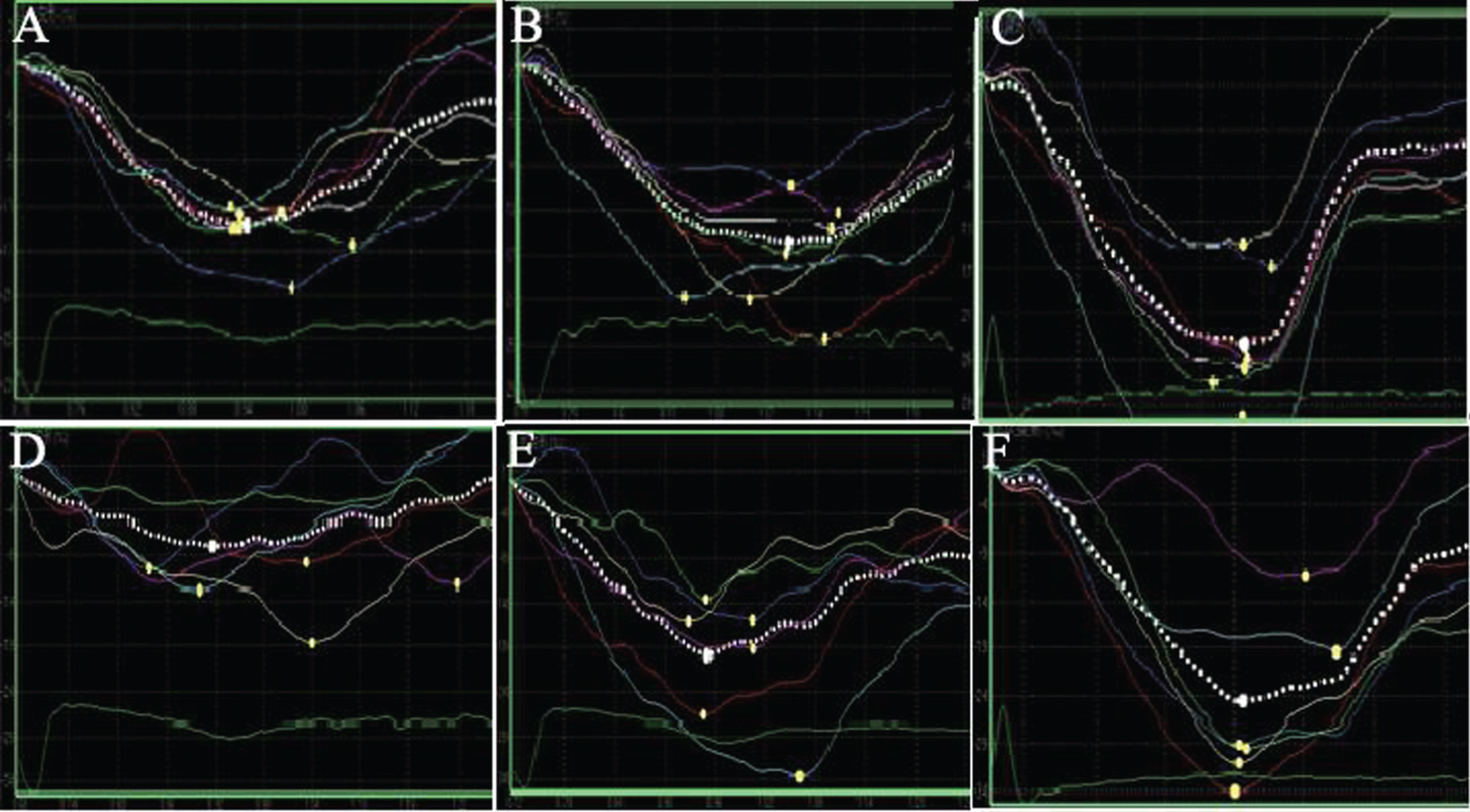
Preoperative and postoperative 3D-STI images obtained from a NSTEMI patient. A: Preoperative GLS curves; B: GLS curves one month after operation; C: GLS curves three months after operation; D: Preoperative GCS curves; E: GCS curves one month after operation; F: GCS curves three months after operation.
All acquired data were performed using SPSS statistical software (version 16.0; SPSS, Inc., Chicago, IL, USA). Continuous data were expressed as means±standard deviation. Continuous variables were statistically analyzed by Student’s t-test. Categorical variables were assessed by chi-square analysis. Correlations between the parameters and LVEF were tested by Pearson correlation coefficients. The P-value (P < 0.05) was used as a criterion to be considered as a statistically significant difference of the comparison between the NSTEMI group and control group in preoperative and 1-month follow-up data analysis.
The conventional parameters are summarized in Table 2. LVESV and LVEF showed markedly differences in NSTEMI groups including HF-PEF group and HF-REF group at 1-month, 3-month follow-up compared with control group, and preoperative data (P < 0.05). LVEF was significantly increased in HF-PEF group and HF-REF group at 3 month follow-up compared 1 month follow-up (P < 0.05).
The conventional parameters of 3D-STI in NSTEMI and control groups
The conventional parameters of 3D-STI in NSTEMI and control groups
Note: a,bNSTEMI vs control group, aP < 0.05, bP < 0.01; c,dpreoperative data of two groups, cP < 0.05, dP < 0.01; e1-month follow-up data of two groups, P < 0.05.
The 3D full-volume parameters are presented in Table 3. GLS, GCS and torsion were obviously decreased in the three NSTEMI groups compared with control group before and after PCI (P < 0.05). However GLS, torsion were distinctly improved in the 3 NSTEMI groups at postoperative 1 and 3 months compared with preoperative data (P < 0.05). HF-REF group was also showed improved GCS on postoperative 1 and 3 month compared with preoperative data, and improved GLS at 3-month follow-up compared with 1-month follow-up (P < 0.05).
Left ventricular strain parameters in NSTEMI and control groups
Note: a,bNSTEMI vs control group, aP < 0.05, bP < 0.01; c,dpreoperative data of two groups, cP < 0.05, dP < 0.01; e1-month follow-up data of two groups, P < 0.05.
Compared with control group, the hs-TNT, hs-CRP and NT-proBNP were obviously increased in the three NSTEMI groups before PCI (P < 0.05), and were markedly decreased in the 3 groups at postoperative 1 month and 3 month compared with the preoperative data (P < 0.05, Table 4). As shown in Table 5, LVEF has positive correlations with LVESV, torsion and negative correlations with LVGLS, LVGCS, NT-pro BNP in the three NSTEMI groups (P < 0.05).
Laboratory indexes in control and NSTEMI groups
Note: a,bNSTEMI vs control group, aP < 0.05, bP < 0.01; c,dpreoperative data of two groups, cP < 0.05, dP < 0.01; e1-month follow-up data of two groups, P < 0.05.
The correlations between LVEF and relevant parameters
Identification of patients with left ventricular function (LV) recovery after PCI has crucial prognostic implications. In our study, 3D-STI, as accurately to observe the LV deformation in patients with NSTEMI, is preferable for detecting abnormalities in cardiac structure and function for NSTEMI. LVEF is the most common echocardiographic parameter for evaluating LV function in clinical applications. In our study, the decreased value of 3D-LVEF in patients with NSTEMI before PCI was reversed after PCI treatment, indicating that PCI helps the recovery of cardiac function.
Basing on cardiac anatomy, the longitudinal fiber is the major element of subendocardial myocardium. Therefore the change of contractility on longitudinal axis is a sensitive indication for subclinical myocardial damages [14, 15]. Kalam et al. [16] demonstrated that LVGLS was superior on predicting major adverse cardiac events. Xu et al. [17] proved that LVGLS could be superior in the evaluation of myocardial function. In our study, the increased value of LVGLS in patients with NSTEMI after PCI, is also indicated as a sensitive index for evaluating the subclinical myocardial damage. LV twisting is described as the wringing motion of the ventricle around its long axis in the LV wall [18, 19]. Torsion, as the parameter for LV twisting function, is a significant predictor of LV remodeling [20]. Nucifora et al. [21] observed that LV torsion was significantly impaired early after AMI. Our study has the consistent results with the impaired twisting function before PCI and improved function after PCI in NSTEMI groups. GRS mainly reflects the thickening of the ventricular wall during the systolic phase, Zhu et al. [22] demonstrated that the reduced GRS may be multiply affected by the presence of injuries of 3 myocardial layers. While the NSTEMI patients without obvious thickened ventricular wall in our study were showed with no significant difference of GRS compared with control group. Cardiovascular biomarkers play important roles in the diagnosis of cardiac diseases, including the use of hs-TnT to detect myocyte injury and NT-proBNP to detect myocardial cell necrosis [23, 24]. And NT-proBNP has a strong prediction of morbidity and mortality [25]. Hs-CRP is a representative marker for systemic inflammation. In our study, the decreased levels of hs-TnT, NT-pro BNP, hs-CRP in patients with NSTEMI after PCI, are consistent with the 3D-STI results, which further proved the 3D-STI as a sensitive detection method for patients with NSTEMI.
According to the parameters, the HF-REF group was found to have more distinctly improvement in cardiac function after PCI treatment in the study. We speculated that the larger damage area in HF-REF group would accelerate myocardial injury. The early revascularization would be crucial for them with better prognosis. Our study demonstrated that the parameters of LVESV, LVGLS, LVGCS, torsion and NT-proBNP had well correlation with LVEF, and LVGLS, torsion showed strong correlations with LVEF. Shetye et al. [26] showed similar correlations between LVEF and LVGLS, LVGCS in patients with STEMI (r = 0.64, r = 0.71). And patients with heart failure had a negative correlation between NT-pro BNP and LVEF (r = –0.602) in the research of Duan et al. [27]. Fujiwara et al. [28] also observed the strong correlation between LV dyssynchrony and torsion. However hs-CRP had no correlation with LVEF in our study. A possible explanation for this is that hs-CRP is generated by multiply inflammatory responses and affected by various factors with lack of specificity.
Our study also has some limitations. First, the retrospective analysis might affect the results due to unmeasured confounder. And the small sample size might lead to a lack of statistically significant differences. Second, we used semi-automated software to quantify LV mechanics and the results will depend on image selection and the ability of parameters. Third, we haven’t detect or identify one best parameter or several optimal parameters to accurately assess cardiac function in patients, so further investigation by using a mathematical model was needed. Last, the accuracy of using the automated software to detect so many parameters was not investigated in our current study. Thus, using the automated software with the quantitatively big data processing and analysis capability [29] will be explored and applied in our future study to improve accuracy and robustness of the study and assessment results.
Conclusion
In this study, we demonstrated that the combinative detection of 3D-STI and NT-pro BNP was an efficient approach to assess the cardiac function during the periprocedural period and the follow-up in patients diagnosed with NSTEMI undergoing PCI.
Declaration of interest
The authors report no conflicts of interest.
Footnotes
Acknowledgments
This research was supported by a grant from Tianjin Health Care Industry Program for Tacking Key Problems (No.15KG127).