
Abstract
OBJECTIVE:
To evaluate the skeletal and dental characteristics in skeletal class III patients with facial asymmetry and to analyse the relationships among various parts of the stomatognathic system to provide a theoretical basis for clinical practice.
METHODS:
Asymmetric cone-beam computed tomography data acquired from 56 patients were evaluated using Mimics 10.0 and 3-Matic software. Skeletal and dental measurements were performed to assess the three-dimensional differences between two sides. Pearson correlation analysis was used to determine the correlations among measurements.
RESULTS:
Linear measurements, such as ramal height, mandible body length, ramal height above the sigmoid notch (RHASN), maxillary height, condylar height, buccal and total cancellous bone thickness, and measurements of condylar size, were significantly larger on the nondeviated side than on the deviated side (P < 0.05). Crown root ratio and buccolingual angle of mandibular first molar were found to be significantly smaller on the nondeviated side than on the deviated side (P < 0.05). A negative correlation was also discovered between the buccolingual angle of mandibular first molar and the ramal height (P < 0.01).
CONCLUSIONS:
In patients with facial asymmetry, asymmetries in the mandible, maxilla and condylar morphology, and skeletal canting served as major components of skeletal asymmetry. Furthermore, a reduced thickness of buccal cancellous bone and a larger crown root ratio were found on the deviated side, indicating that orthodontic camouflage has limitations and potential risks. A combination of orthodontics and orthognathic surgery may be the advisable choice in patients with a menton deviation greater than 4 mm. An important association between vertical skeletal disharmony and dental compensation was also observed.
Introduction
Skeletal class III with facial asymmetry is common in orthodontic clinics and can severely degrade facial aesthetics and oral function. The treatment of skeletal class III patients with facial asymmetry is challenging for orthodontists because of the complicated characteristics of asymmetry. Although various aetiological factors, such as heredity, environmental factors, condylar hyperactivity, etc., have been proposed, the causes of facial asymmetry remain unclear. Investigating the skeletal and dental characteristics in skeletal class III patients with facial asymmetry is helpful in designing orthodontic treatment plans for this malocclusion and for understanding its formation mechanism.
Currently, evaluating facial asymmetry is still challenging because the asymmetry may involve skeletal, dental and soft tissue components. Skeletal (mandible, maxilla, and temporomandibular joint) features are research hotspots in facial asymmetry patients. Because the mandible is a relatively flexible part, and the mandibular growth periods are longer, a deviation of the lower face is more frequent than that of the upper and midface regions [1]. Skeletal asymmetry may involve the mandible only; however, the asymmetry usually also affects the maxilla, which is the antagonist basal bone of the mandible. Many studies [2–9] have characterized maxillomandibular features, but mandibular and maxillary symmetry are still being disputed. The temporomandibular joint (TMJ) is the pivot connecting the maxilla and mandible, and its harmonious function is important for maintaining a normal masticatory system. The symmetry of the TMJ structures helps the TMJ to function normally. Kau CH [10] indicated that skeletal class III patients with facial asymmetry whose skeleton and occlusion are asymmetric may show asymmetric TMJ conditions. While linear, angular, volumetric, and surface area measurements used to assess condylar characteristics have been undertaken by several three-dimensional (3D) research efforts [2, 11–13], a cone-beam computed tomography (CBCT) study of glenoid fossa morphology symmetry is lacking. Further 3D evaluations of skeletal characteristics in patients with facial asymmetry is necessary.
For patients with facial asymmetry, orthodontic camouflage and surgical treatment are the two main therapies. Because surgical treatment causes greater trauma and is associated with higher costs, many patients with facial asymmetry tend to be treated with orthodontic camouflage. When adopting orthodontic camouflage, practitioners should bear in mind its potential limitations and follow basic biomechanical principals; otherwise, iatrogenic sequelae may occur [14]. If facial asymmetry is beyond the scope of correction by conventional orthodontic treatment, a combined orthognathic surgical approach may be required [15]. The dimensions of the alveolus constitute a limiting factor for orthodontic movement [16], and the movement of the posterior teeth plays an important role in the management of facial asymmetry. The dimensions of the posterior alveolus and the position of the posterior teeth in the alveolar bone should therefore be established before treatment. The degree of compensation and the condition of the posterior teeth should also be taken into consideration when selecting treatment options. Investigating the dental characteristics of the posterior teeth (the position of the tooth in the alveolar bone, dental compensation, and tooth condition) in patients with facial asymmetry can provide a reference source for choosing a therapy method.
The maxilla, mandible, TMJ, and dental arches are the major components of the stomatognathic system. Teeth are set in the alveolar fossa of the jaw bones, and the maxilla and mandible are linked together by the TMJ; thus, they are interact with each other affects. Therefore, investigating the relationships among the various components of the stomatognathic system is essential. This study evaluated the skeletal and dental characteristics in skeletal class III patients with facial asymmetry and analysed the relationships among various parts of the stomatognathic system to provide a theoretical basis for clinical practice.
Materials and methods
Study subjects
A total of 56 CBCT images (male 26, female 30, mean age 22±3.46 years) were selected from patients who had undergone a CT scan at the authors’ institution between 2011 and 2015. The inclusion criteria were as follows: 1) angle class III malocclusion and skeletal class III patients (ANB <0°); 2) facial asymmetry (menton deviation ≥4 mm); 3) age ≥18 years; 4) absence of functional mandibular deviations; and 5) full permanent dentition with the exception of the third molar. Patients with 1) abnormally shaped molars; 2) a history of orthodontic treatment; 3) a temporomandibular joint disorder syndrome; 4) noticeable periodontal diseases; 5) a history of facial trauma; and 6) diseases or congenital syndromes accompanied by skeletal disharmony, were excluded from the dataset of this study. The study was conducted according to the recommendations for research involving human subjects and was approved by the authors’ institution (CQHS-IRB-2016-02).
CBCT scans and 3D reconstruction of the CBCT scans
All patients underwent standardized CBCT (KaVo Dental Gmb H, USA) with a setting of 120 kVp, 5 mA, 8.9 sec and voxel size of 0.4 mm. Patients were asked to occlude at maximum intercuspation and relax their lips; in addition, they were positioned with the Frankfort horizontal plane parallel to the floor and the midsagittal plane align with the long axis of the CT machine.
CBCT images were exported in the Digital Imaging and Communication in Medicine (DICOM) format using the iCAT Vision software. DICOM files were imported into the Mimics 10.0 software (Materialise, Leuven, Belgium), and 3D reconstructions were created. The mandible and mandibular first molars were separated from the whole image.
Measurements
The multiplanar visualization was combined with the 3D image reconstructions to locate anatomic landmarks (Fig. 1 and Table 1). Reference planes were established (Fig. 1): The axial plane was defined by passing through the bilateral orbitale and the right porion points; The plane crossing the midpoint of the zygomaticotemporal suture of the two sides and perpendicular to the axial plane was defined as the coronal plane; The plane crossing the most anterior midpoint of the maxillary anterior nasal spine and perpendicular to the axial plane and coronal plane was defined as the sagittal plane. Skeletal and dental measurements were taken using the Mimics (Materialise, Leuven, Belgium) and 3-Matic (version 7.0) software programs.
Description of landmarks
Description of landmarks
L/R, left/right.

Landmarks (as described in Table 1) and reference planes. A and B, lateral and frontal views of maxillofacial region. C, reference planes: a, axial plane; b, coronal plane; c, sagittal plane. D and E, lateral and frontal views of mandible. F, condyle. G, maxillary teeth. H and I, buccolingual and mesiodistal views of mandibular first molar. I is a perspective figure.
Mandibular measurements included an evaluation of menton deviation, mandibular inclination, ramal height, and mandible body length. To further evaluate the mandibular ramus, ramal height above the sigmoid notch (RHASN) and ramal height below the sigmoid notch (RHBSN) were measured. Maxillary inclination and maxillary height were used for evaluating maxillary symmetry (Table 2 and Fig. 2).
Description of measurements
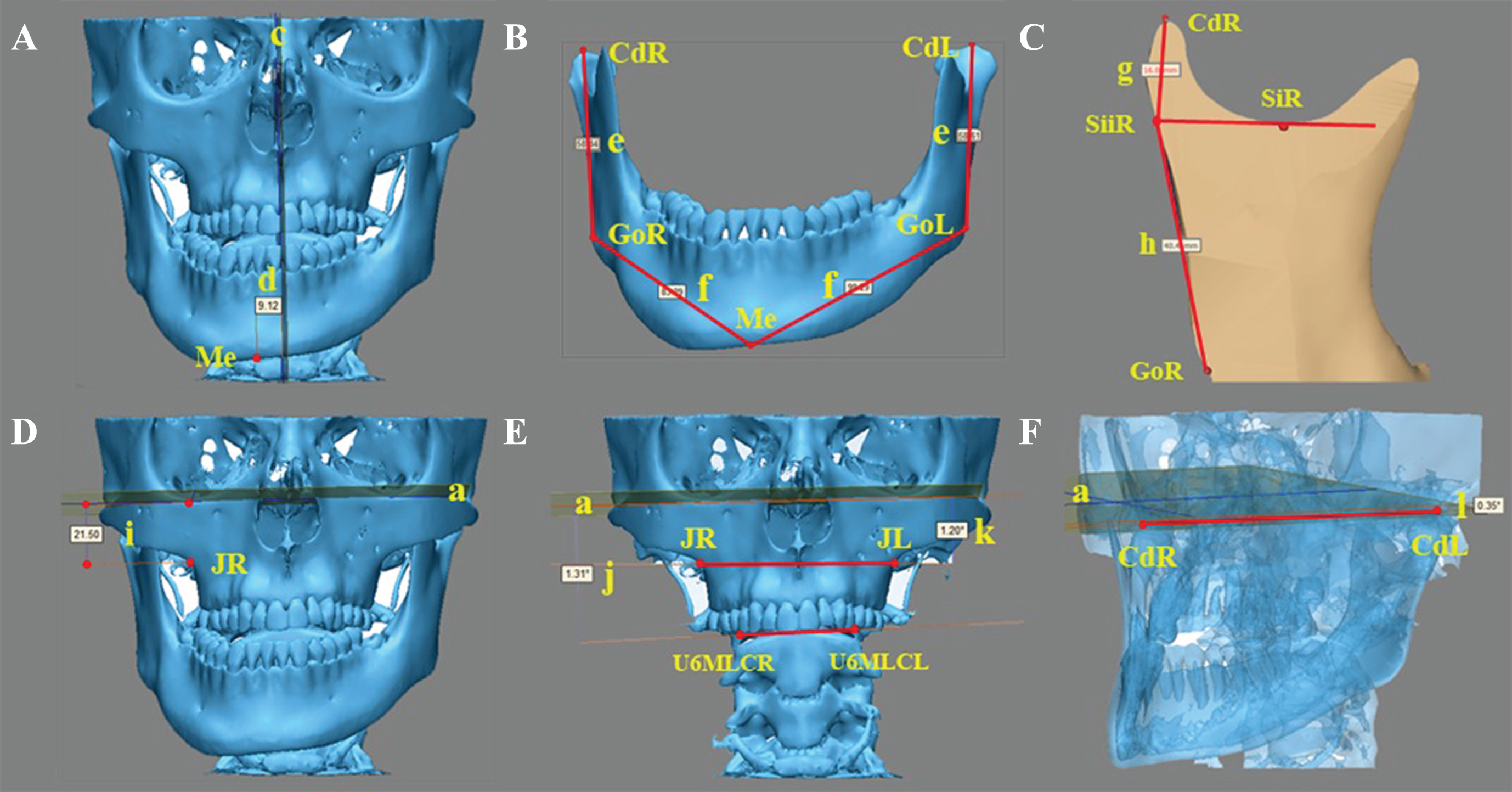
Mandibular and maxillary measurements (The description of measurements is shown in Table 2). A, frontal view of maxillofacial region. c, sagittal plane; d, menton deviation. B, mandibular frontal view. e, ramal height; f, mandible body length. C, section view of mandibular ramus, which was cut along the plane constructed by Cd, Si and Go. g, ramal height above the sigmoid notch; h, ramal height below the sigmoid notch. D, E and F, frontal and lateral views of maxillofacial region. a, axial plane; i, maxillary height; j, occlusal plane angle; k, maxillary angle; l, mandibular angle. F is a perspective figure.
For the TMJ, the symmetry of glenoid fossa and condyle were evaluated. Glenoid fossa width, glenoid fossa height, and tuberculum articulare angle were used to assess the symmetry in the glenoid fossa morphology. The condyle was evaluated from two aspects (morphology and position). Condylar height, condylar volume and condylar surface were used to evaluate the symmetry in the morphology. The symmetry of position included an evaluation of condylar anteroposterior position and axial condylar angle (Table 2 and Fig. 3).
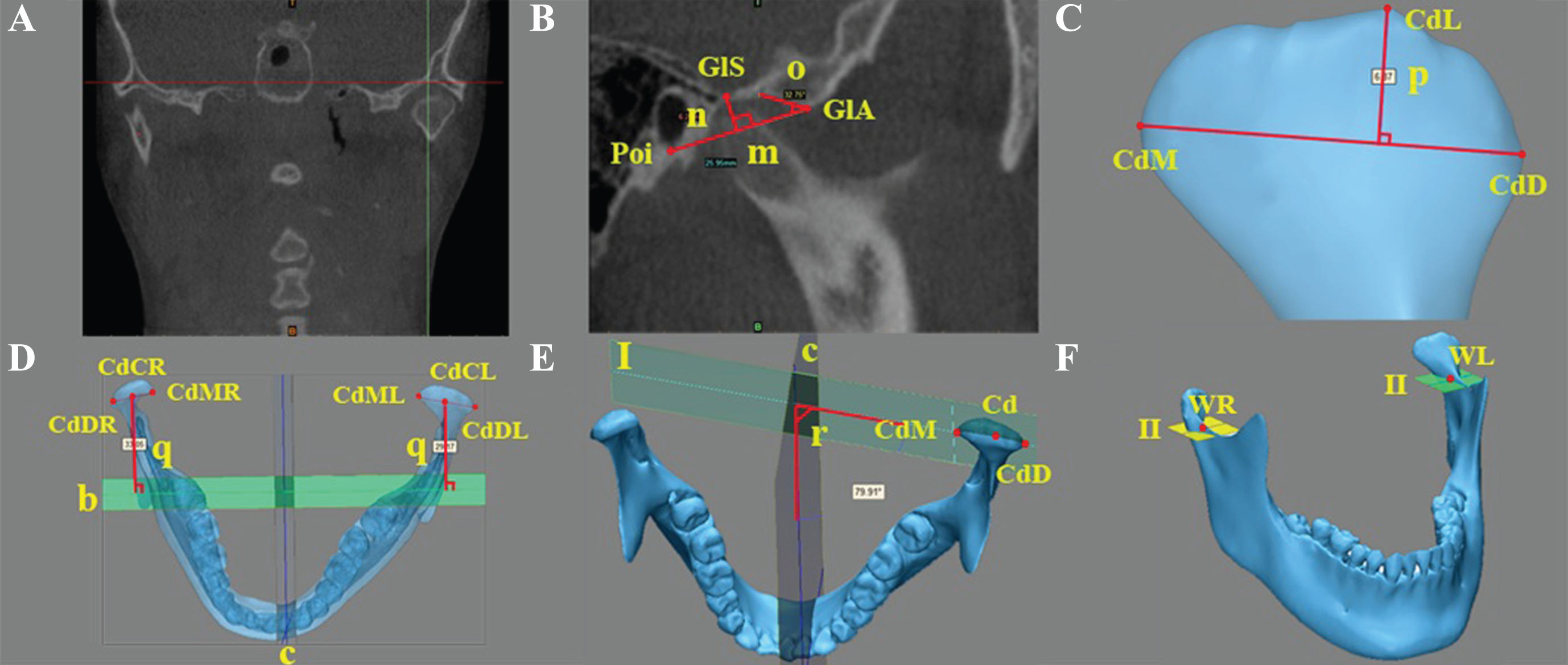
Measurements of temporomandibular joint (The description of the measurements are shown in Table 2). A and B, the coronal and sagittal views at which the curvature of glenoid fossa is the deepest. m, glenoid fossa width; n, glenoid fossa height; o, tuberculum articulare angle. C, condyle. p, condylar height. D, E and F, mandibular upper and lateral views. b, coronal plane; c, sagittal plane; q, condylar anteroposterior position; I, coronal plane of condyle; r, axial condylar angle; II, wing muscle fossa plane.
In this study, the mandibular first molar was used as an example to preliminarily analyse dental characteristics. Dental characteristics were evaluated from three aspects (tooth condition, dental compensation, and the position of the tooth in the alveolar bone). Crown root ratio was used to evaluate the tooth condition. Dental compensation included an evaluation of buccolingual and mesiodistal angles of mandibular first molar. Buccal cancellous bone thickness, lingual cancellous bone thickness and total cancellous bone thickness were used to assess the position of the tooth in the alveolar bone (Table 2 and Fig. 4). Furthermore, occlusal plane inclination was used for assessing the occlusal plane (Table 2 and Fig. 2).

Dental measurements (The description of measurements is shown in Table 2). A, section view of mandibular first molar, which was cut along the plane constructed by L6MBC, L6DBC and L6MA. s, crown length; t, root length. B, section view of mandibular first molar and mandible, which were cut along the plane constructed by L6MRB, L6MRL and L6MA. u, v and w, buccal, lingual and total cancellous bone thickness. C and D, frontal and lateral views of mandibular teeth. c, sagittal plane; III, maxillary occlusal plane; x and y, buccolingual and mesiodistal angles of mandibular first molar. C is a perspective figure.
All measurements were repeated after a two-week interval by the same operator, and the mean of the two measurements was used in the statistical analysis. The intraclass correlation coefficient (ICC) was used in assessing the magnitude of measurement error. The paired t-test was used to compare the differences between the two sides. The Pearson correlation analysis was used to determine correlations among measurements. Statistical evaluations were performed at the 5% level of significance with SPSS (version 17.0; SPSS, Chicago, III).
Results
The ICC results ranged from 0.836 to 0.905, indicating that the method had good reliability. In skeletal indices, ramal height, mandible body length, RHASN, maxillary height, condylar height, condylar volume and condylar surface were significantly greater on the nondeviated side than on the deviated side (P < 0.01). There was no significant difference in RHBSN, glenoid fossa width, glenoid fossa height, tuberculum articulare angle, condylar anteroposterior position and axial condylar angle (Table 3). The mean value of the occlusal plane inclination, maxillary inclination and mandibular inclination were 1.88°, 0.98° and 1.01°. Among subjects of this experiment, the proportion of occlusal canting, maxillary canting and mandibular canting were 63.63%, 54.54%, and 45.45% respectively (Occlusal canting/maxillary canting/mandibular canting was defined as the angle between the bi-U6MLC/bi-jugal/bi-condyle and axial plane exceeding 1°).
Comparison of the differences in measurements between nondeviated and deviated sides (Paired-Samples T Test)
Comparison of the differences in measurements between nondeviated and deviated sides (Paired-Samples T Test)
SD, standard deviation. The Paired-Samples T Test was used to compare the difference between nondeviated and deviated sides. *P < 0.05; **P < 0.01.
In dental indices, crown root ratio and buccolingual angle of mandibular first molar were significantly smaller on the nondeviated side than on the deviated side (P < 0.05). When compared with the deviated side, the buccal and total cancellous bone thickness were found to be significantly larger on the nondeviated side (P < 0.05). The lingual cancellous bone thickness and mesiodistal angle of mandibular first molar were not significantly different between the two sides (Table 3).
Menton deviation was significantly correlated with differences in ramal height (P < 0.01), mandible body length (P < 0.05), RHASN (P < 0.01) and condylar volume (P < 0.05) between the two sides. There were significant correlations between the ramal height with RHASN (P < 0.05). Maxillary height was negatively related to the crown root ratio (P < 0.05). Both condylar volume and condylar surface were correlated with ramal height (P < 0.05) and RHASN (P < 0.01). A negative correlation was found between buccolingual angle of mandibular first molar and ramal height (P < 0.01, Table 4).
Correlation analysis between statistically significant difference measurements (Pearson correlation analysis)
Diff, nondeviated side minus deviated side. *P < 0.05; **P < 0.01.
This study used CBCT for the measurement and analysis of skeletal class III patients with facial asymmetry. CBCT has smaller magnification errors, less radiation exposure, shorter scan times, and lower operating costs compared with traditional radiography [17, 18]. CBCT is an effective tool for clinical examinations and has high accuracy and application value in evaluating TMJ morphology. Take assessing glenoid fossa morphology symmetry as an example to compare the evaluation difference between using old methods and CBCT: Traditional radiograph have magnification errors and the glenoid fossa morphology displayed in these radiograph are not clear. Traditional methods can display the sagittal glenoid fossa morphology, such as the transpharyngeal projection (Fig. 5A) and the transcranial projection (Fig. 5B), but they are difficult to reflect the coronal and transversal glenoid fossa morphology. Utilizing traditional radiograph to assess glenoid fossa morphology symmetry need to take two X-ray photographs. CBCT is able to contrast glenoid fossa morphology symmetry with various sagittal sections (Fig. 5C), coronal sections (Fig. 5D) and transverse sections (Fig. 5E). Furthermore, CBCT can reconstruct the inspected parts and rotate them on the screen to achieve thorough observation (Fig. 5F and G). The frequency of highly reliable values in identifying landmarks was greater in the multiplanar visualization than in 3D image reconstructions [19]. However, previous research [20] has concluded that identifying landmarks with multiplanar visualization may be affected by the reference anatomic structure, visualization of the anatomic plane, and operator training. To improve the accuracy, this study therefore combined multiplanar visualization with 3D image reconstructions to define landmarks.
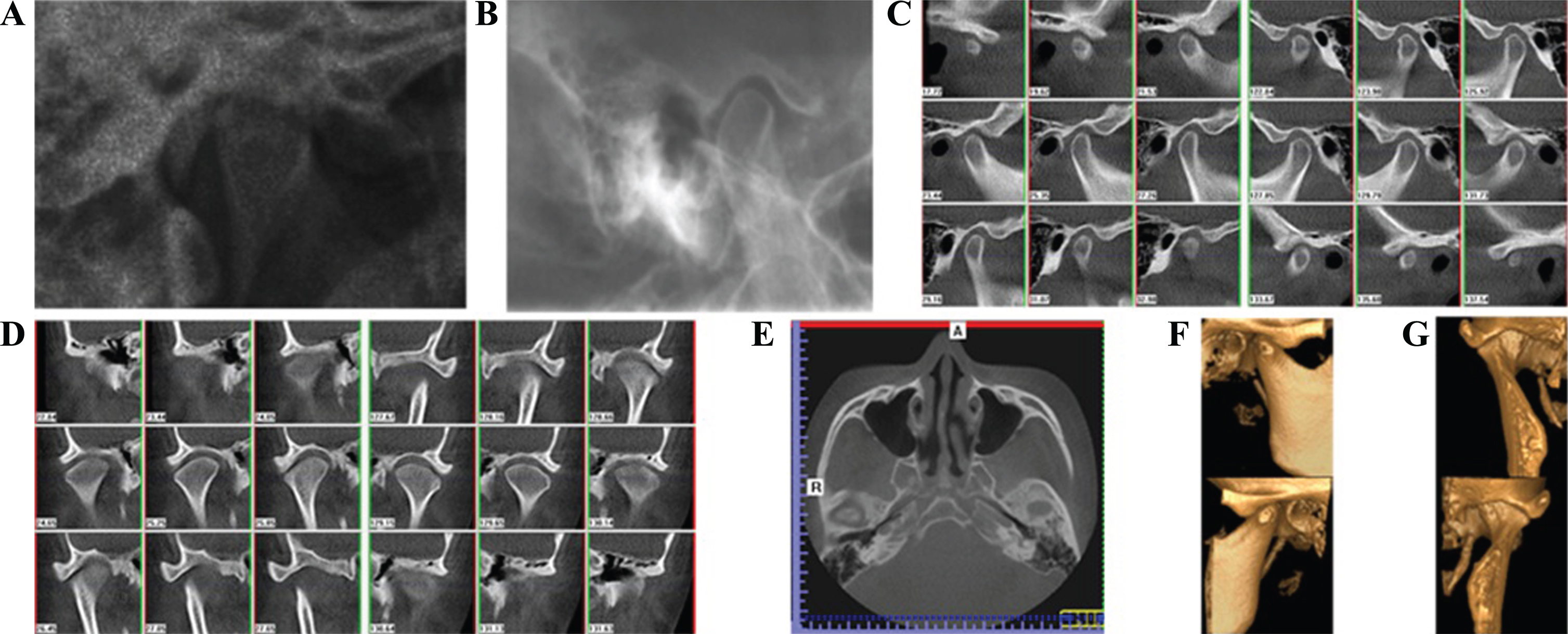
Compared the difference between using old methods and CBCT in assessing glenoid fossa morphology symmetry. A, the transpharyngeal projection. B, the transcranial projection. C, sagittal sections. D, coronal sections. E, transverse sections. F and G, the reconstruct glenoid fossa.
Determining which structures are involved, including the mandible, maxilla and/or another craniofacial region, is important to achieve the correct diagnosis and therapy. Deviations in the lower face are more frequent than those in the upper and midface. The mandibular ramus and body are the basic units of the mandible. In patients with facial asymmetry, their symmetry is still under discussion due to diverse inclusion criteria and measurement methods among experiments. It was concluded by HyoYeon Lee [5] that there was no significant difference in ramal height and body length. Some scholars [2, 3] have insisted that ramal height is asymmetrical, but body length is symmetrical, while others [4] hold the opposite view. This study found that both ramal height and mandible body length were asymmetrical. Anatomically, ramal height can be divided into two parts (RHASN and RHBSN) by the line parallel to the axial plane and tangential to the lowest point of the sigmoid notch. It is amusing to further investigate which part of ramus has significant differences. This study measured RHASN and RHBSN and showed that the difference in ramal height was due to the bilaterally asymmetrical RHASN. We also found that 45% of the subjects in this experiment appeared to have mandibular canting. These findings suggest that facial asymmetry may be caused by the length differences in the mandibular basic units as well as the spatial rotation of the mandible.
The symmetry of the maxilla in patients with facial asymmetry is a controversial issue because inclusion criteria, landmarks and reference planes are diverse in the current research. While the maxillary asymmetry has been reported in some studies [4, 6], experiment published by Lee et al. [5] did not report the same outcomes. This study showed that maxillary height was significantly different between the two sides. Moreover, among the subjects in our experiment, the proportion of maxillary canting was 54.54%, suggesting that maxillary canting was common in patients with facial asymmetry. In facial asymmetry, asymmetric maxilla and maxillary canting can be assumed to be adaptations of the asymmetric functional condition, which was caused by existing mandibular asymmetry. The significance of a maxillary cant is that this feature will require correction with surgery if the mandibular asymmetry is to be corrected. To summarize, in the diagnosis and treatment of facial asymmetry, both mandible and maxilla should be considered from at least two aspects: asymmetrical morphology and skeletal canting.
The symmetry of the structures in the TMJ is important for maintaining normal function. In this study, the results of condylar morphology were consistent with the outcomes of previous experiments [11, 21] that reported that condylar height, volume and surface were smaller on the deviated side. In patients with facial asymmetry, the deviated side exhibited bigger medial pterygoid volumes [22], and the percentage of fast muscle fibers was increased in the deep masseter muscle on the deviated side [23]. These suggest that the bilateral condyle may be subjected to asymmetrical forces during mastication. Some animal experiments [24] have confirmed that the asymmetrical force can lead to asymmetric condylar remodelling. Asymmetry in condylar morphology may be caused by asymmetric condylar adaptive reconstruction. Bishara [25] claimed that if the posterior crossbite was not treated for a long time, adaptive remodelling would occur in TMJ and the condylar position would become more symmetrical. This finding supports the experimental result in our study that there was no obvious difference in bilateral condylar positions. Therefore, in the clinical treatment of adult facial asymmetry patients, adjustments in jaw positions should have a limit. Although the condylar morphology was asymmetrical, the morphology of glenoid fossa did not show asymmetry, possibly because, when compared with the glenoid fossa, condylar adaptive reconstruction is more active. In brief, an asymmetry in condylar morphology was the major component of TMJ asymmetry in patients with facial asymmetry. Yanez-Vico had indicated that condylar morphology asymmetry was a common feature of temporomandibular disorders (TMD) [26]. Accordingly, facial asymmetry patients have the potential risk of appearing to have TMD. In the treatment of facial asymmetry, orthodontic specialists should pay more attention to TMJ, especially in performing intermaxillary traction and mandible backward movements. These specialists should use caution to prevent TMJ from being damaged.
The present study used the intersection angle of two planes to assess transverse dental compensation, which is more precise than the measurements used in previous studies [27–30]. This experiment and previous studies [27–30] indicate that buccolingual angle of mandibular first molar was significantly smaller on the nondeviated side than on the deviated side. This was attempt to compensate the lateral skeletal disharmony by causing dental changes. When patients undergo surgical treatment, asymmetric torque control should be adopted in the deviated and nondeviated side to eliminate dental compensation. However, if patients undergo non-surgical treatment, the compensatory inclinations should be maintained or produced. This research also demonstrated that the deviated side had smaller buccal cancellous bone thickness. Accordingly, the roots of the deviated side may make contact with the cortical plate when producing compensatory buccolingual inclination, which can inhibit orthodontic movements to a great degree and may lead to dehisences, fenestrations or root resorption [31]. Furthermore, the crown root ratio on the deviated side proved worse than that of the nondeviated side. The above results suggest that producing compensatory inclinations has limitations and potential risks. However, from the perspective of health and stability, a combination of orthodontics and orthognathic surgery are perhaps a better choice in cases of menton deviation ≥4 mm. An important discovery was that the total cancellous bone thickness on the deviated side was found to be smaller. Therefore, clinicians should be aware that in patients with facial asymmetry, the range of mandibular first molar movement on the deviated side was limited compared to the nondeviated side. In the subjects of this study, the proportion of occlusal canting was 63.63%, indicating that facial asymmetry was usually associated with an occlusal canting. Preoperative measurement of the occlusal plane inclination in all patients with facial asymmetry will ensure that the orthognathic surgery is properly planned.
The stomatognathic system is indivisible and interactive, making it important to further investigate the relationships among them. The differences in ramal height, mandible body length, RHASN and condylar volume are found to have a significant correlation with menton deviation, indicating that the mandibular [2, 9] and condylar incoordination between the two sides are the factors causing mandibular asymmetry. However, the masticatory muscles, facial soft tissues and occlusal factors may influence the occurrence and development of mandibular deviation. Further study is needed to analyse these factors. Transverse dental compensation has been confirmed to be closely related to sagittal and transverse skeletal discrepancy [30]. In this experiment, ramal height was significantly related to buccolingual angle of mandibular first molar, suggesting that vertical skeletal discrepancy is also correlated with transverse dental compensation.
This study has several limitations. Combined with the results of the previous studies [19, 20], the method for determining landmarks in this experiment is deemed reliable. Therefore, the linear and angular measurements based on landmarks are accurate. However, using smoothing algorithms in 3D surface reconstruction can eliminate holes in areas with low voxel threshold, which can cause measurement errors in condylar volume and condylar surface. Because the elimination holes of the two sides are approximately equal for the same research object, this should not affect the comparison results of condylar size between the two sides. Nonetheless, we still reduced the frequency of using smoothing algorithms. Future studies that consider this aspect in larger sample sizes are needed.
This research concluded that facial asymmetry may be caused by length differences in mandibular basic units as well as the spatial rotation of mandible and these will probably cause maxillary asymmetry. Second, an asymmetry in condylar morphology served as the major component of TMJ asymmetry in skeletal class III patients with facial asymmetry. Furthermore, a smaller buccal cancellous bone thickness and a larger crown root ratio were found on the deviated side, indicating that orthodontic camouflage has limitations and potential risks, and a combination of orthodontics and orthognathic surgery may be the advisable choice in patients with a menton deviation of greater than 4 mm. Importantly, a vertical skeletal discrepancy was proved to have a significant correlation with transverse dental compensation.
Footnotes
Acknowledgments
This work was supported by Program for the Natural Science Foundation of China (81470772); the Natural Science Foundation of Chongqing (cstc2015jcyjA10028, cstc2016jcyjA0238); the Medical Scientific Research Project of Chongqing (20141013, 2015HBRC009, 2016MSXM051); the Program for Innovation Team Building at Institutions of Higher Education in Chongqing (CXTDG201602006); the Chongqing Municipal Key Laboratory of Oral Biomedical Engineering of Higher Education.