
Abstract
Cone beam computed tomography (CBCT) has obvious advantages over regular radiography in diagnosis of complex diseases. Objective of this study is to report a case of a mandibular jaw ameloblastoma recurring cyst, which represents a benign tumor of odontogenic epithelium, using CBCT imaging technology. CBCT examination of the patient suffering with recurrent lower jaw cyst (relapsing four years after surgery) showed a decrease in irregular bone density and appearance of a honeycomb pattern (3.5 cm×2.5 cm×1.8 cm) in the right lower jaw. This suggests that the lesion is more likely to be an ameloblastoma. Preoperative tissue biopsy and pathological examination of surgical sample confirmed the diagnosis. Surgical resection of the diseased tissue and autogenous bone grafting in the mandible was performed. Postoperative CBCT examination showed that the bone defect healed well, without recurrence of the tumor 22 months postoperatively. In conclusion, the rotated 3D CBCT images clearly displays the exact size, location, borders and internal changes of the tumor in the jaw cyst itself and the adjacent tissues. Thus, the dental CBCT allows clinicians to better evaluate lesions, leading to better treatment outcomes.
Introduction
Ameloblastoma is a benign odontogenic tumor with a predilection for the mandible. It represents approximately 1% of oral tumors and usually occurs in the third to fourth decades without gender predilection [1, 2]. This tumor originates from the remnants of dental laminas and odontogenic epithelium. It leads to loosening and shifting of teeth and destruction of the surrounding anatomical structures [3]. Ameloblastoma is currently classified into four types: solid/multicystic, extraosseous/peripheral, desmoplastic and unicystic ameloblastomas [4]. Histopathologically, the lesion can be classified as follicular, acanthomatous, granular, basal, desmoplastic and plexiform. Ameloblastoma usually demonstrates a slow growth tendency without any symptoms; it is characterized by cortical bone expansion, perforation and soft tissue infiltration [5].
The preoperative planning of oral tumors is based on its pathological type, biological behavior and clinical presentation [2, 6]. The cystic ameloblastoma can be treated with decompression; the non-cystic type requires removal of the epithelial tissues within the tumor [7–10]. Therefore, accurate preoperative diagnosis is essential. Cone beam computed tomography (CBCT) scans provide more details of ameloblastoma in 3-dimensional (3D) structure than traditional plain radiographic images [11, 12]. It is able to reveal the precise internal structures, changes of the tumor and its adjacent tissues [13].
At present, various radiographic diagnostic imaging techniques, including panoramic radiograph, computed tomography (CT) and magnetic resonance imaging (MRI) are commonly used in the diagnosis of oral and maxillofacial diseases. Panoramic radiographs can differentiate between pathological lesions and surrounding structures. However, the limitations of panoramic radiographs, including inherent magnification and resolution may lead to fuzzy images and disturb diagnosis. As stated by Koong, only 25% of doctors believe panoramic radiographs provide enough information for diagnosis [14]. Spiral CT has the advantage of showing the lesion area in multiple directions and cross sections with a higher accuracy. This becomes necessary to completely evaluate jaw cysts, especially for proopiomelanocortin [15, 16]. However, the cost and the radiation dose of spiral CT is higher than other imaging diagnostics and poses a concern. Magnetic resonance imaging (MRI) also provides imaging solutions in multiple directions with enhanced ability to show soft tissues. Some cystic contents under MRI register as heterogenous, non-uniform signal, which can further contribute in the diagnosis [17, 18]. Nevertheless, as compared with the panoramic radiographs, MRI is more expensive and time-consuming with higher amount of the radiation dose [19].
CBCT with significant clinical reference value has been widely used in radiotherapy of pancreatic cancer, esophageal cancer and head and neck cancer [20–22]. It provides images with the scanning of cone beam in contrast to the fan-shaped beam CT uses [23]. It accurately calculates 3D direction of translational displacement error in the course of radiotherapy. It reflects the anatomical position, changes of organizations and structure in the irradiated zone [24, 25]. It is also able to reveal the adjacent relationship, size, border of tumors and the situation of surrounding tissues [26–28]. With CBCT the 3D information of the mandiblular defect can be well obtained [29, 30]. In addition, the range, borders and the amount of bone destruction associated with the mandiblular lesion can be precisely observed in each direction [31].
Thus, in this paper, we aim to report a case of a mandibular ameloblastoma. In this case, the static image and 3D rotation image formed by CBCT played a crucial role in the diagnosis and management of the disease.
A Case Report
Patient information
A 31-year-old female patient presented with pain in her right lower jaw for 3 months and aggravation of the pain over one week. The patient had a dental surgery for a single cyst with the approximate size of 1.0 cm×1.0 cm 4 years ago. The cyst relapsed 3 months postoperatively with no symptoms and no further intervention.
Extra-oral physical examinations indicated facial asymmetry with a slightly elevated right side of the lower jaw. Moreover, a 1.5 cm×1.5 cm lump on the mandibular anterior vestibular region was observed. On intraoral palpation, the borders of the mass were nuclear, with the mucosal surface intact. The texture of the mass was hard and non-fluctuating without wave motion. No loosening of the teeth in the affected area was noted. There was an obvious pain on percussion in the right mandibular first premolar. About 1 mL of brown transparent fluid was aspirated via a fine needle biopsy.
CBCT Examination
CBCT examinations were performed utilizing a device with a flat panel detector (aSi) in size of 20×25 cm (KaVo 3D exam; KaVo, Biberach, Germany) and reconstructed through i-CAT Vision software (Imaging Sciences International, Hatfield, Pa). The CBCT images showed a low-density lesion with an ill-defined border in the middle mandible extending from the left mandibular lateral incisor to the right mandibular canine with suspected apical absorption but no obvious lamina dura invasion. Close to the low-density lesion a honeycomb mixed lesion with a clear border in the right mandible was observed. The bony cortex of right mandible was not continuous. Displacements of the right mandibular canal and the root of right mandibular second premolar were seen (Fig. 1).

The CBCT images before surgery. A, A low-density lesion with an ill-defined border was detected in the middle mandible (white dotted line) and the absorption and displacement of teeth. Honeycomb mixed lesion with a clear border (red dotted line). B, The sagittal image shows the swelling of the honeycomb mixed lesion (arrow). C, The coronal image shows the displacement of mandibular canal (green dots and arrow). D, The horizontal image shows the lesion with disordered bone trabecula structure and cortical discontinuity (arrow). E-F, The anterior and lateral views of the 3D reconstruction of the preoperative CBCT views.
Histopathological examination via tissue biopsy confirmed the right mandibular ameloblastoma. After consulting with the patient and her family, a surgical plan that included reconstruction of the resected jaw bone with autologous iliac bone graft was decided upon. We completely resected of the lesion and the affected tissues of the mandible along with the simultaneous removal of teeth in the line of the lesion constructing a 13-cm continuous defect. Then we harvested two iliac bone grafts and combined them with titanium plate to restore the mandiblular defect.
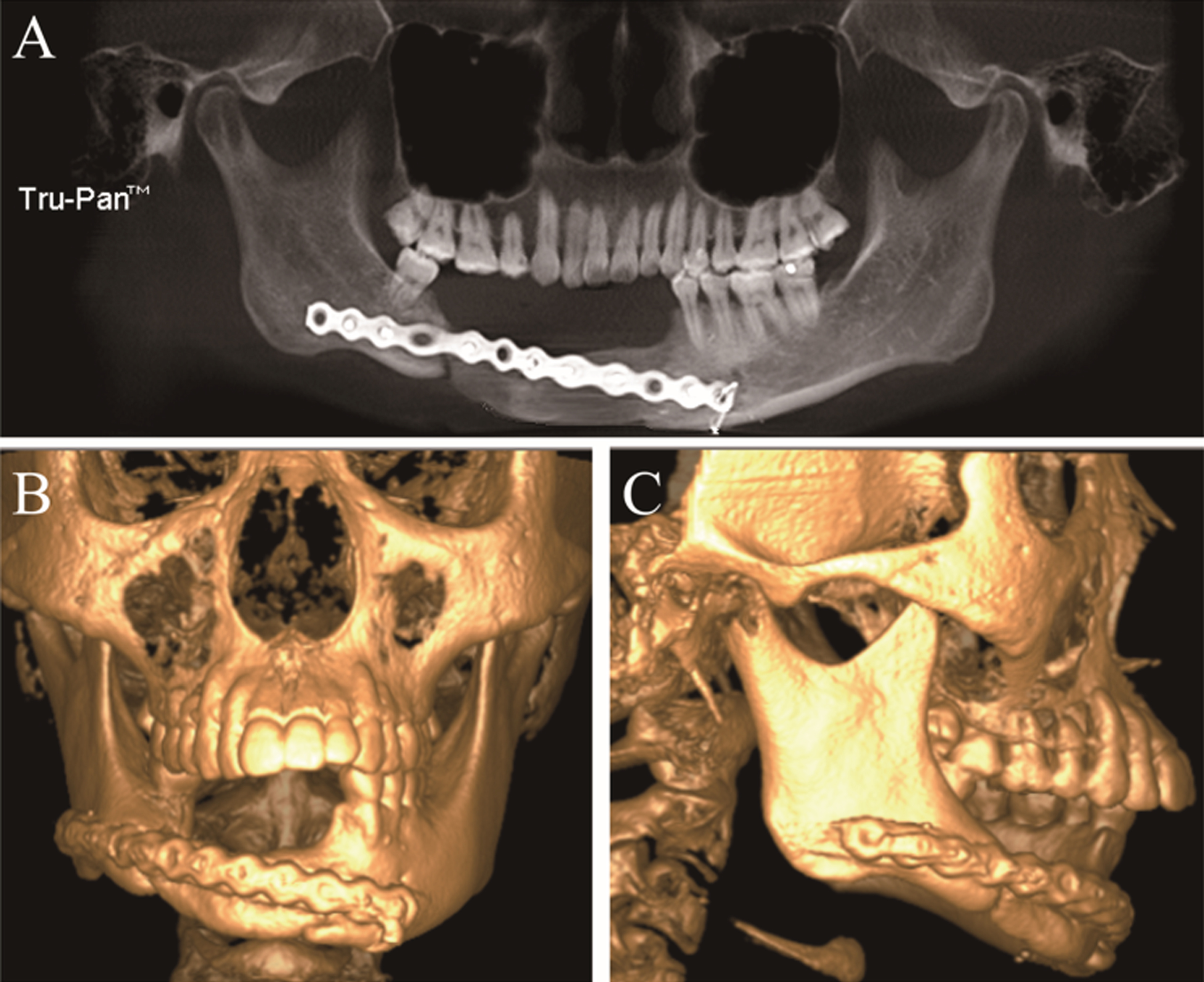
CBCT images scanned one week after the surgery showed that the lesion was completely removed, the free iliac bone and titanium plate were stable, and the defect of mandibular bone was mainly repaired (Fig. 2). CBCT images scanned twenty-two months postoperatively showed that the implanted titanium plate was in good position. In addition, the transplanted iliac bone showed partial absorption but the whole mandible retained its structure and function (Fig. 3). While some amount of resorption was noticed at the healing site, the patient had no evidence of relapse. Adequate mandibular bone height and width remained with good facial form. As per the surgical plan, rehabilitation of the reconstructed part with dental implants was planned in the next phase of treatment.

CBCT images and 3D reconstruction 1 week postoperatively: A, Panoramic view shows the lesion was replaced by the iliac bone grafts and firmly combined with the titanium plate. B-C, The anterior and lateral views of the 3D reconstruction of the CBCT views.
CBCT images and 3D reconstruction 22 months postoperatively: A, Panoramic view shows the firm restoration of the mandible and partly marginal absorption of the grafts. B-C, The anterior and lateral views of the 3D reconstruction of the CBCT views.
The mandibular cystic lesion was removed completely, with no signs of recurrence 22 weeks after surgery. At the same time, the grafted iliac bones fused considerably; however, the height of the right side of the grafted iliac bone was found to be reduced by approximately 2 mm.The trabecular bone image in this region was clear. There was no significant change in the coronal and sagittal planes of temporomandibular joint bilaterally.
Overall perspective obtained by 3D rotated images
The pre- and post-treatment 3D rotated images were obtained by Dolphin Software (version 11.0; Dolphin Imaging Systems, Chatsworth, CA). These images showed that good bone fill was obtained through the grafted iliac bone. The Titanium plate fastened the grafted bones well. A new and continuous bone was formed between the grafted iliac bone and the original mandibular bone. In addition, functional occlusion and physiologic condition of the remaining teeth was restored (Fig. 4).
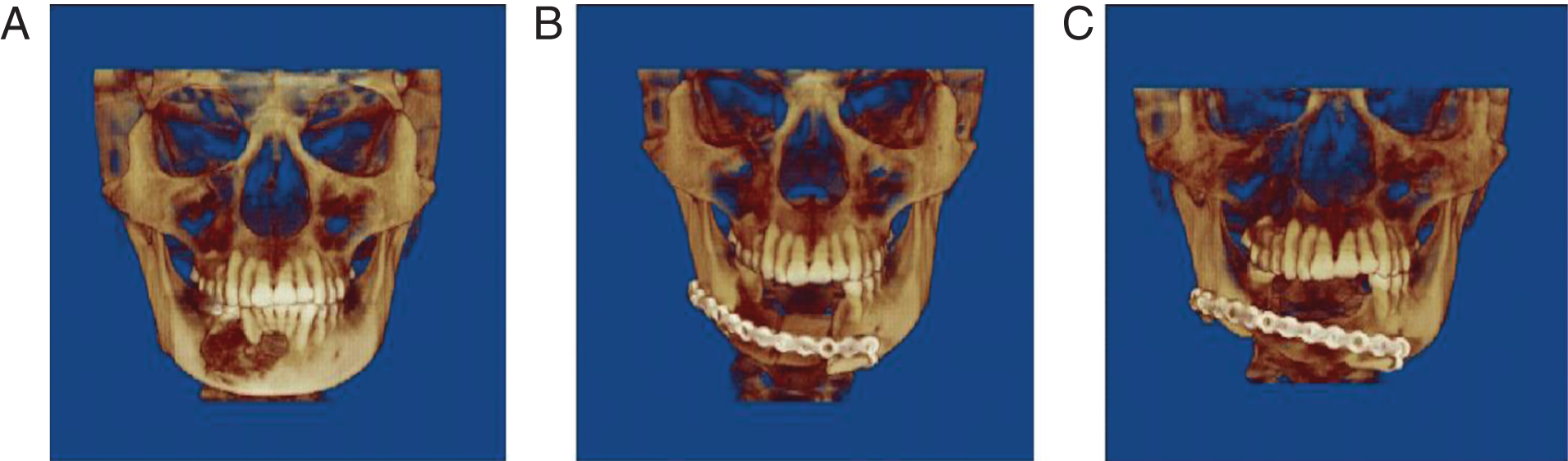
A: 3D rotated images of pre-operative; B: 3D rotated images of 1 week post- operative; C: 3D rotated images of 22 months post-operative.
Rotational 3D panoramic radiography provides a highly efficient imaging methodology in the diagnosis of maxillary and mandibular diseases, including in ameloblastomas. Jaw ameloblastomas are often located in the adjacent teeth and surrounding tissue [32]. Therefore, in some cases, it is hard to determine the specific location of the edge of the cyst, true involvement of the teeth and the adjacent anatomic relationship between the maxillary sinus and the mandibular canal. This makes it difficult to determine preoperative plans.
To evaluate jaw cyst lesions in 3D, multi slice spiral CT (MSCT) is often used. However, MSCT is not clear enough for development of the subtle anatomical structures, especially for jaw bone imaging [33]. MSCT imaging is performed by medical imaging personnel; clinicians only passively read the films and sometimes cannot get the necessary information for decision making. In contrast, CBCT achieves less distorted 3D image data through volumetric scanning in the axial, sagittal and coronal planes. This results in a 3-dimensional image reconstruction with different imaging principles [34, 35]. In addition, clinicians can read CBCT data through the computer software. More comprehensive and accurate information of the target area (in any direction) can be obtained by just a drag of computer mouse [36]. Moreover, patients reported a more comfortable scanning experience because of positioning and lower radiation doses [35, 37]. However, some images could be hindered by artifacts and image noise [38]. The advantages and disadvantages of CBCT and other imaging techniques are summarized on Table 1.
Comparison of the advantages and disadvantages of Panoramic Radiograph, traditional CT, MRI and CBCT
Although ameloblastoma is a benign tumor, it has a malignant tendency with aggressive, invasive behavior. This enhances the significance of early diagnosis and prompt treatment. Surgical resection of the lesion and surrounding area of the mandible reduces the risk of malignant changes or recurrence [39]. In the presented case, the changes in root morphology, uneven bone and a honeycomb appearance were visible in CBCT image. The preoperative biopsy and pathological examination both confirmed ameloblastoma, which is the same as pre-surgical CBCT image indicated.
In conclusion, 3D imaging of CBCT provides accurate diagnosis for ameloblastoma in the jaw bone. CBCT is reliable and effective in differential diagnosis, preoperative planning and the evaluation of postoperative efficacy.
Disclosure
None of the authors have a conflict of interest.