
Abstract
Rosai-Dorfman disease (RDD) is a rare histiocytic disorder of unclear etiology, which commonly presented with the enlargement of lymph nodes of the neck and the head. Here, we report an unusual case of 77-year-old male patient presenting with left kidney lesion with several small enlarged lymph nodes around the abdominal aorta. The diagnosis of left kidney cancer was suspected and the patient underwent left laparoscopic exploration and lymph node biopsy. Only saponification of the renal surrounding fat and enlargement of the left renal pedicle and 5 abdominal aortic lymph nodes were found; no kidney cancer was found. Surrenalectomy and lymphadenectomy dissection were then performed and the left kidney was retained. Intraoperative frozen and postoperative pathology indicates Rosai-Dorfman disease. RDD with kidney involvement is uncommon, and its x-ray imaging appearances are atypical, and often resemble kidney cancer leading to kidney loss. A systematic literature review was also performed to investigate the x-ray imaging and treatment features of this disease.
Case report
A 77-year-old male patient with 3 weeks of repeated left flank pain presented. A left kidney lesion (3.0 cm×3.5 cm) was detected by 64 rows of abdominal computed tomography (CT) and enhanced uneven scaning. The patient had a history of hypertension, cerebral infarction, and chronic hepatitis B virus. Ten years ago, he was diagnosed with Rosai-Dorfman disease (RDD) by lymph node biopsy due to neck and inguinal region lymphadenopathy. He was treated with an interferon dose of 1×106 units/time for 12 cycles during one month with no effect. He was then converted to chemotherapy with 1 cycle of COP (vincristine + ifosfamide + dexamethasone) and 2 cycles of CHOP (vincristine + ifosfamide + pirarubicin + dexamethasone). The enlarged lymph nodes initially shrunk and eventually disappeared. This admission, the physical examination revealed tenderness of the left flank without superficial lymph node enlargement. Laboratory examination showed globally normal values with normal renal function.
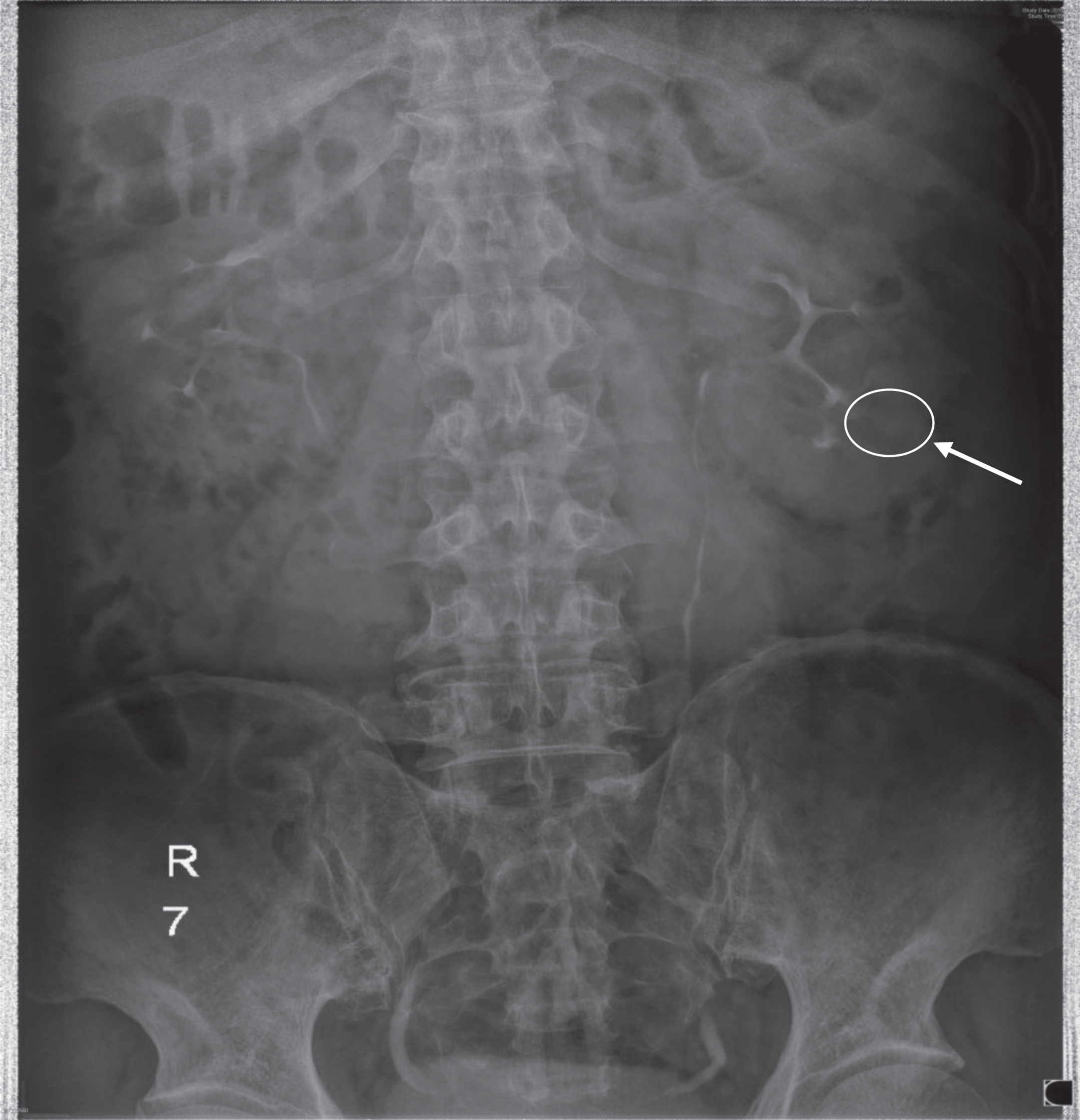
X-ray image examination with intravenous pyelography showed normal morphology of the right kidney and a sharp renal calyx was clearly observed without filing defect. The morphology of the middle and lower calyx of left kidney was unclear. This imaging suggested that the lesion occupied the left kidney (Fig. 1). The abdominal CT scan with 64 rows showed the lesion was in the middle and lower poles of left kidney measuring 3.5 cm of diameter with heterogeneous contrast enhancement. For further diagnosis, abdominal CT with 256 rows and three dimensional reconstruction (Video 1) was performed, confirming the location of the lesion in the left kidney and 5 enlarged retroperitoneal lymph nodes were found between the abdominal aorta and left renal hilum. (Fig. 2). Diagnosis of left renal cancer with abdominal aortic lymph node metastases was suspected. Left laparoscopic abdominal exploration and lymph node biopsy was further performed. Only saponification of the surrounding renal fat and enlargement of left renal pedicle and five lymph nodes (1.5 cm×1.2 cm to 2.0 cm×1.5 cm) was noted. Intraoperative frozen pathology indicated Rosai-Dorfman disease. Surrenalectomy and lymphadenectomy dissection were performed, and the left kidney was preserved. The patient recovered quickly and the lumbago symptoms disappeared 7 days postoperatively. The postoperative pathology showed lymph follicles that included an enlarged lymphatic sinus, plasma cells, cell hyperplasia, and tissue hyperplasia with multinucleated cells was formed (Fig. 3). Immunohistochemical results showed a positive S100, positive CD68, partially positive CD1a, negative CK, FDC net positive CD21, partially positive Ki-67, partially positive CD20, partially positive CD3, negative acid-fast stain, which are typical characteristics of RDD distinguishing it from other diseases (Fig. 4).
Morphology of middle and lower calyx of left kidney was unclear in the intravenous pyelography, which suggested kidney cancer.

Adominal CT with 256 rows showed left kidney lesion with 3.5 cm in diameter (white arrow) and 5 enlarged retroperitoneal lymph nodes (white circle) between abdominal aorta and left renal hilar area.
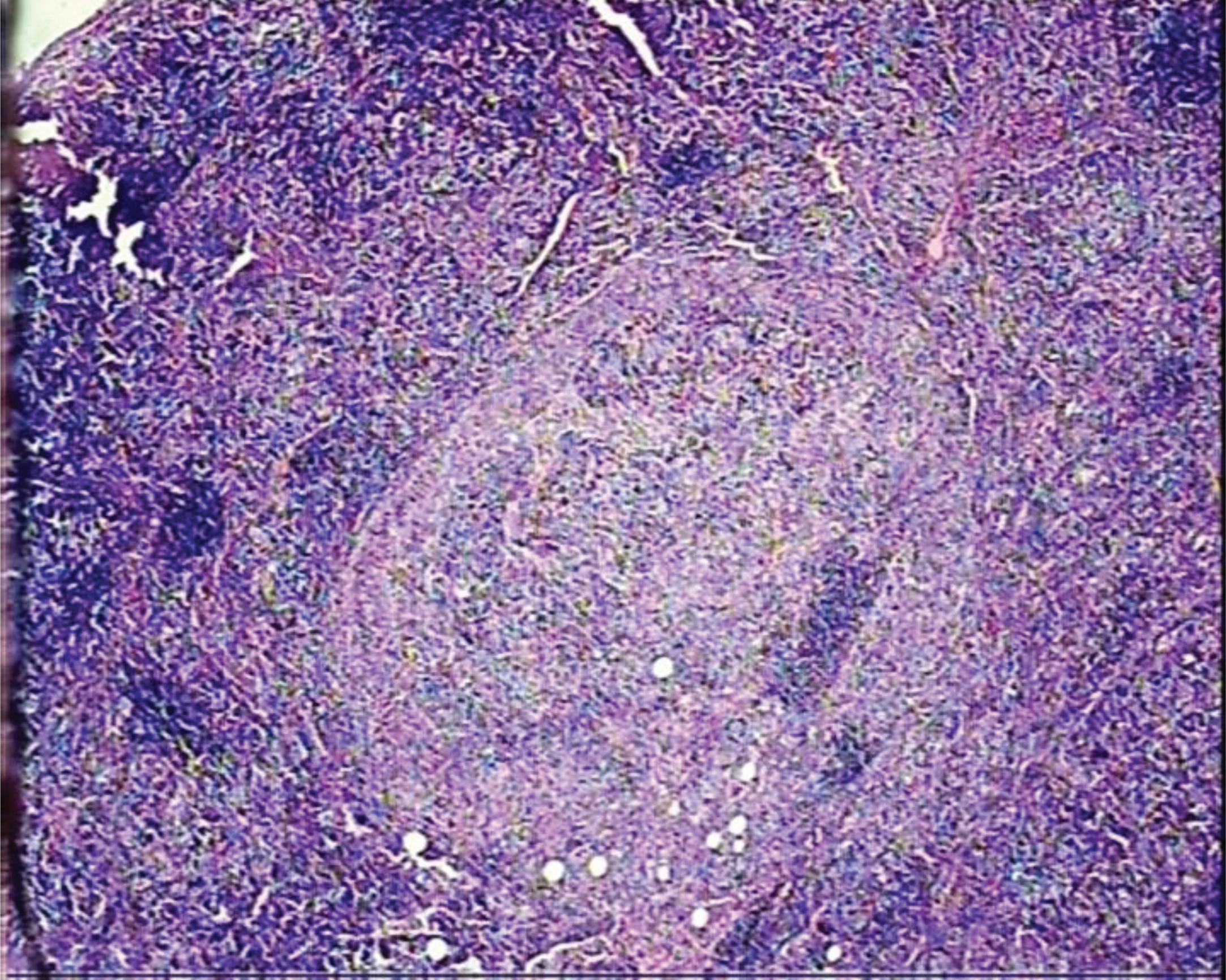
Postoperative pathology showed that lymph follicles and enlarged lymphatic sinus, plasma cells, and cell hyperplasia, and tissue hyperplasia with multinucleated cells were formed. HE x 40.
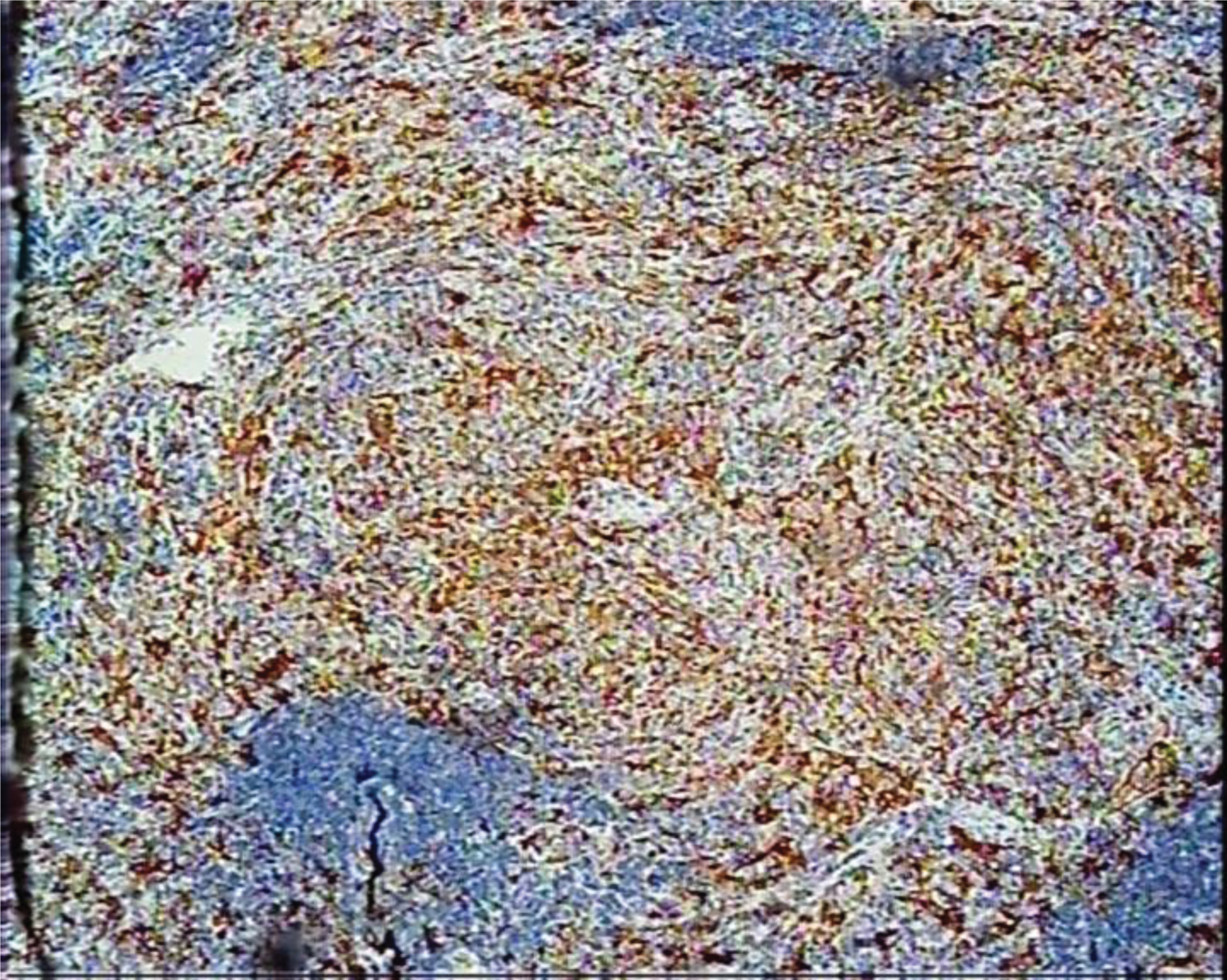
Typical characteristics in scattered foci of lymphocytic aggregation cells (Bowen color) of S100+ for Rosai-Dorfman disease distinguished from other diseases. Immunohistochemical staining, HE x 40.
Rosai-Dorfman disease, also known as sinus cell hyperplasia with giant lymphadenopathy of unknown etiology, has histiocytosis lesions with obvious pathological features, which was first proposed by Rosai and Dorfman in 1969 [1]. Currently, RDD etiology is still unknown, but may be associated with viral infection [2], or induced by a long-term use of immunosuppressive agents [3].
CT imaging is the mainstay for diagnosis of kidney tumors. With the development of additonal imaging techniques, three-dimensional (3D) reconstruction images based on CT and MRI has played a more important role in the differential diagnosis of kidney tumors [4, 5]. The 3D reconstructed images often provide more detailed information about anatomic relationship and morphological features of normal and diseased kidney tissues. Additionally, it provides a more accurate and insightful illustration of kidney tumors. With the aid of 3D reconstruction technology, tumor tissue can be precisely evaluated to aid in preoperative preparation, decrease injury to neighbor organs, reduce surgical complications, and lead to improved surgical outcomes [6, 7].
RDD is characterized by lymphadenopathy, with fever and leukocytosis, which often has increased erythrocyte sedimentation rate (SED rate) and gamma globulins on laboratory examination [8]. It is rare and often misdiagnosed as a malignant tumor with multiple metastases due to its vague clinical manifestations and depiction on imaging [9]. Currently, the diagnosis of RDD depends on the histopathology. Its typical characteristic is “movement into the histiocyte,” which is manifested as single or multiple morphological intact lymphocytes and/or plasmacytoid cells into the proliferation of the cytoplasm. However, basic hematoxylin and eosin (H&E) stains do not always demonstrate enough, further need to perform immunohistochemistry S100 marker for macrophages and Langerhans cells in inflammatory diseases is necessary. For three cases of RDD with kidney involvement in Brown’s report, there was no typical movement phenomenon in H&E staining but immunohistochemistry was more enlightening [8]. In this case, the postoperative pathology showed hyperplastic tissue with multinucleated cells and positive S100 and CD68 +, negative acid-fast stain typical of RDD.
RDD with kidney involvement is uncommon and is often misdiagnosed as renal malignancy often leading to kidney loss [9–11]. To our knowledge, there were no more than 20 reported cases of retroperitoneal RDD with kidney involvement. Almost all cases were misdiagnosed as renal cancer, and radical nephrectomy was performed. In this case, the patient was first suspected to have kidney cancer with abdominal aorta lymph node metastases due to atypical x-ray imaging. In light of the past history of RDD involving neck and inguinal lymphadenopathy, we did not perform radical nephrectomy but laparoscopic exploration and lymph node biopsy were performed. This eventually leads to retention of the kidney. From this case, our experience of identification of RDD with kidney involvement from renal malignant tumors is as follows: (1) history: most RDD with kidney involvement patients have immune system diseases or long-term use of hormones, while most renal malignant tumors do not have that relevant past history; (2) clinical manifestations: RDD with kidney involvement mainly involves the neck, retroperitoneal and inguinal lymph nodes with a long duration and without obvious clinical symptoms. Regional back pain would be caused by invaded lymph nodes outside the kidney. Renal malignant tumors do not show any obvious clinical symptoms at an early stage but back pain, hematuria and blood dyscrasias would appear with the development of cancer [12]. (3) Imaging manifestations: Intravenous pyelography or CT image examination of RDD with kidney involvement have no specificity, while most renal malignant tumors have their own features and imaging changes, such as low or isodensity signal in normal CT and fast in and out signals in enhanced CT [13]. On the basis of X-ray imaging, we could not differentiate RDD with kidney involvement from renal malignancy, so the lymph node biopsy was recommended to get the final pathological diagnosis.
As a result, there is no unified standard for the therapy of RDD with kidney involvement to date. Usual treatment options are surgery [14], radiotherapy [15], chemotherapy and hormone therapy [16]. Some scholars consider RDD with kidney involvement a benign lesion. Classically, surgery often requires nephrectomy which lead to kidney loss. Over-treatment is probably unnecessary and observation is recommended [17]. However, some think that RDD with renal involvement is associated with poor prognosis with 40% mortality and the remainder having persistent involvement [18]. Therefore, surgery in combination with comprehensive treatment appears to be most effective [19]. According to our own experience, laparoscopic exploration and lymph node biopsy were recommended to make the differential diagnosis from renal malignant tumors and avoid the loss of kidney.
Conclusion
Rosai-Dorfman disease with kidney involvement, although rare, its x-ray imaging appearances are atypical, and often resemble kidney cancer, and lead to kidney loss. High attention should be taken and laparoscopic exploration and lymph node biopsy are recommended for the differential diagnosis of renal malignant tumors and kidney reserve.