
Abstract
OBJECTIVE:
To evaluate the relationship of microhemorrhage on susceptibility-weighted imaging (SWI) with the severity of clinical symptoms and the prognosis of viral encephalitis.
MATERIALS AND METHODS:
Thirty patients with clinically diagnosed viral encephalitis were divided into three groups according to the Glasgow Coma Scale (GCS) and the condition of recovery namely, Group I (n = 12): Glasgow Coma Scale (GCS)≥13 and recovered with no sequelae; Group II (n = 11): GCS 9–12 and recovered with some sequelae; Group III (n = 7): GCS 3–8 and recovered with more severe sequelae. The microhemorrhage detectability on SWI and conventional MR imaging in these three groups was compared and their correlations with different seriousness of clinical symptoms and prognosis were analyzed.
RESULTS:
There was a significant difference in microhemorrhage volume among different MR sequences (p < 0.05). SWI was more sensitive to detect microhemorrhage than conventional MR imaging techniques. Microhemorrhages on SWI were significantly different among the three groups (p < 0.01). The volume of microhemorrhage on SWI was well correlated with the degree of clinical symptoms and the prognosis of viral encephalitis.
CONCLUSION:
SWI can be used to detect microhemorrhage in patients with viral encephalitis. Assessment of microhemorrhage with SWI can provide useful information for the prognosis evaluation of viral encephalitis.
Keywords
Introduction
Viral infections of the central nervous system and adjacent structures are often life-threatening conditions. Herpes simplex encephalitis is the most common type of non-epidemic encephalitis and accounts for 5–10% of all encephalitis cases. HSV-1 encephalitis is mostly found in adults, often with localized lesions in the temporal and frontal lobes. HSV-2 infection is more common in neonates and the brain involvement is more generalized. Other herpes viruses may cause viral encephalitis in a lower frequency than herpes simplex virus. In addition, cytomegalovirus (CMV) encephalitis should be considered in patients with immunodeficiency, e.g., those using immune suppressive drugs or chemotherapy [1, 2]. Clinical diagnosis of viral encephalitis is suggested by fever and general symptoms of infection, encephalopathy, and focal neurological signs. Patients usually present with malaise, headache, nausea, and vomiting, which could be followed by acute or subacute onset of altered consciousness, focal and generalized seizures, and features of raised intracranial pressure and microhemorrhage, including papilloedema, psychiatric aberrations, and behavioral abnormalities such as confusion and delirium.
Common sequelae among survivors of viral encephalitis include learning disability, motor deficits, memory loss, ataxia, dysphasia, seizures, and cranial nerve lesions. Retrograde memory and language ability can be impaired. A majority of survivors will have significant residual neurological deficits even with aggressive therapy. Patients experiencing a shorter delay between presentation and treatment have a better cognitive outcome. If treatment is delayed, permanent neurological deficits may occur in survivors. Thus, early and accurate diagnosis is considered a key factor for the successful treatment of viral encephalitis patients, and immediate resuscitation is applied following diagnosis. All adults with suspected encephalitis are given anti-viral therapy while waiting for confirmation of the diagnosis.
The diagnosis of viral encephalitis is usually established by a combination of clinical and laboratory findings [3]. Imaging, especially MR imaging, plays an important role in the diagnosis and follow-up of viral encephalitis. Visualization of typical lesion patterns often allows a rapid diagnosis and subsequent therapeutic decisions [4, 5]. Susceptibility weighted imaging (SWI) is a novel imaging method that maximizes susceptibility difference among various tissues by combining a long echo time (TE), high spatial resolution, fully flow compensation, and three dimensional gradient echo sequence. It consists of using both magnitude and phase images, and is very sensitive in the detection of extra vessels blood products [6]. The goal of this study is to evaluate the correlation of microhemorrhage on SWI with the severity of clinical symptoms and the prognosis of viral encephalitis.
Materials and methods
Patients
The study population was recruited from the patients receiving MR examination for suspected encephalitis. A total of 30 patients (17 males and 13 females) were enrolled with a median age of 14.3 years (range 7 months-65 years). All adult patients or the parents of under-aged patients’ signed informed consent forms, and the institutional review board approved the study. The final diagnosis was established on the basis of clinical manifestations, electroencephalographic (EEG) findings, cerebrospinal fluid (CSF) analysis, and serologic tests. On the basis of the CSF and serum findings, the causative viral agents were herpes simplex type I in 9 patients, cytomegalovirus in 5 patients. Types of viral infection were unspecified in the remaining 16 encephalitic patients. The patients were divided into three groups according to the Glasgow Coma Scale (GCS) and the condition of recovery namely, Group I (12 patients): Glasgow Coma Scale (GCS)≥13 and recovered with no sequelae; Group II (11 patients): GCS 9–12 and recovered with some sequelae; Group III (7 patients): GCS 3–8 and recovered with more severe sequelae. Table 1 summarizes the detailed information of the patients in three groups.
Acquisition of imaging data
All examinations were performed using Signa HD 3.0T MRI scanner (GE Healthcare, Little Chalfont, United Kingdom) with 8-channel head array coil. The scanning sequences included the conventional MR sequence and SWI sequence. The parameters of conventional MR sequence were as follows: T1-weighted spin echo fluid attenuated inversion recovery (FLAIR) images (TR 2580 ms, TE 23 ms, TI 860 ms), T2-weighted fast spin echo images (TR 4600 ms, TE 110 ms), T2-weighted FLAIR images (TR 9602 ms, TE 117 ms, TI 2400 ms), and contrast-enhanced T1 weighted spin echo FLAIR images. Slice thickness was 5.0 mm and the slice interval was 1.5 mm. Field of view (FOV) was 240 mm×240 mm. Gadopentetate dimeglumine (0.1 mmol/kg; Bayer HealthCare, Berlin, Germany) was injected through an antecubital vein with 2 mL/s injection rate. Then, 20 mL of saline was injected via a 24-gauge catheter using an MR power injection system (Spectris Solaris EP MR Injection System, Medrad, Volkach, Germany).
All patients received T2 star weighted angiography (SWAN) scanning. The parameters were as follows: TR 32 ms; TE 22 ms; flip angle (FA) 150; slice thickness 2 mm; matrix 320×384; FOV 230 mm×170 mm. Scanning range kept clear of the air-containing regions such as bilateral petrous pyramid, frontal sinus, and sphenoid sinus. Pre-saturation slabs were used to avoid the structure. Minimum intensity projection (MinIP) of SW images (SWI-MinIP) were reconstructed with Advantage Windows (AW sdc 4.3) workstation. The SWI images were reconstructed with slice thickness, position and section number similar to conventional MR sequences.
Image analysis
Two neuroradiologists (Xin-jiang Liu and Chong-xiao Zheng with 10 and 5 year experience in neuroradiology) independently evaluated all imaging data of patients. Irregular low-signal region was assumed to represent hemorrhage, and their distribution was recorded. If the two neuroradiologists had different views, the consensus was researched after the joint reading. The number and volume of microhemorrhage was measured on T1WI, T2WI, T2FLAIR, and SWI images on AW sdc 4.3 workstation. One well-experienced neuroradiologist (Chong-xiao Zheng with 5 year experience in neuroradiology) carefully measured microhemorrhage three times on all MR sequence images, and the average values were regarded as the final results.
Statistical analysis
Statistical package for social science (SPSS) 16.0 software was used for statistical analysis. Quantitative variables were expressed as mean±SD, while categorical variables as frequency or percentage. The differences of microhemorrhage number between SWI and conventional MR sequences in different groups were analyzed with Kruskal-Wallis test. Further comparisons were carried out among those sequences with Mann-Whitney test. Correlation analysis was performed between the micro hemorrhage on SWI and the degree of clinical symptoms and the prognosis of viral encephalitis. P < 0.05 were considered as the level of statistical significance.
Glasgow Coma Scale (GCS) and age of the patients
Glasgow Coma Scale (GCS) and age of the patients
Location and distribution of brain lesions
In 30 patients with viral encephalitis, the locations of brain lesions were as follows: frontal lobe, 16 cases; temporal lobe, 17 cases; parietal lobe, 6 cases; occipital lobe, 4 cases; basal ganglia, 4 cases; thalamus, 2 cases; cerebellar hemispheres, 6 cases; and brain stem, 3 cases. There were 23 patients with multiple brain lesions, and 7 cases had single brain lesion.
The distribution of the brain lesions was also analyzed. Lesions were involved in the cortex in 17 cases, cortex and medulla in 7 cases; subcortical and deep brain white matter in 9 cases; basal ganglia, thalamus and gray matter nuclei in 21 cases. The lesions were asymmetric distribution in 21 cases, and the lesions were in symmetrical distribution in 9 patients with involvement of basal ganglia, thalamus, frontal lobe, and temporal lobe.
Microhemorrhage on SWI and conventional MR sequences
In 30 patients with viral encephalitis, there were 12 patients GCS≥13 and recovered with no sequelae (Group I); 11 patients GCS 9–12 and recovered with some sequelae (Group II); 7 patients GCS 3–8 and recovered with sequelae (Group III). The microhemorrhage number and volume detected on conventional and SWI sequences are summarized in Table 2. There was a significant difference in microhemorrhage volume among different MR sequences (p < 0.05). Inter-class analysis showed that microhemorrhage was not well defined on T1WI (Figs. 1a and 2a). An improvement was seen on T2WI and T2 FLAIR (Figs. 1b, 1c, 2b, 2c). There were statistically significant differences (p < 0.05) among the three conventional MRI sequence groups. SWI was more sensitive than conventional sequences in delineating microhemorrhage in viral encephalitis (p < 0.01). Figures 1d, 1e, 2d, 2e are the two representative images which show SWI was superior to all other sequences in defining microhemorrhage.
Microhemorrhage shown on SWI among three groups of patients with viral encephalitis
The microhemorrhage volumes as measured by SWI in three groups of patients with viral encephalitis are shown in Table 2. Patients in Group I had significantly lower microhemorrhage volumes than those in group II, and the microhemorrhage volumes were the highest in group III (P < 0.01). The microhemorrhage on SWI closely correlated with the degree of clinical symptoms and the prognosis of viral encephalitis (r = 0.694, p < 0.05).
Microhemorrhage on conventional and SWI sequences
Microhemorrhage on conventional and SWI sequences

MR images of a 15-year-old female with viral encephalitis (group I). Transverse T1WI (a), T2WI (b), T2-FLAIR (c), SWI (d) and SW phase image (e). The lesions in bilateral temporal and frontal lobes are hypointensive on T1W image (a), while they are hyperintensive on T2W image (b) and T2-FLAIR image (c). No microhemorrhage is shown on all images including SWI (d) and SW phase images (e).
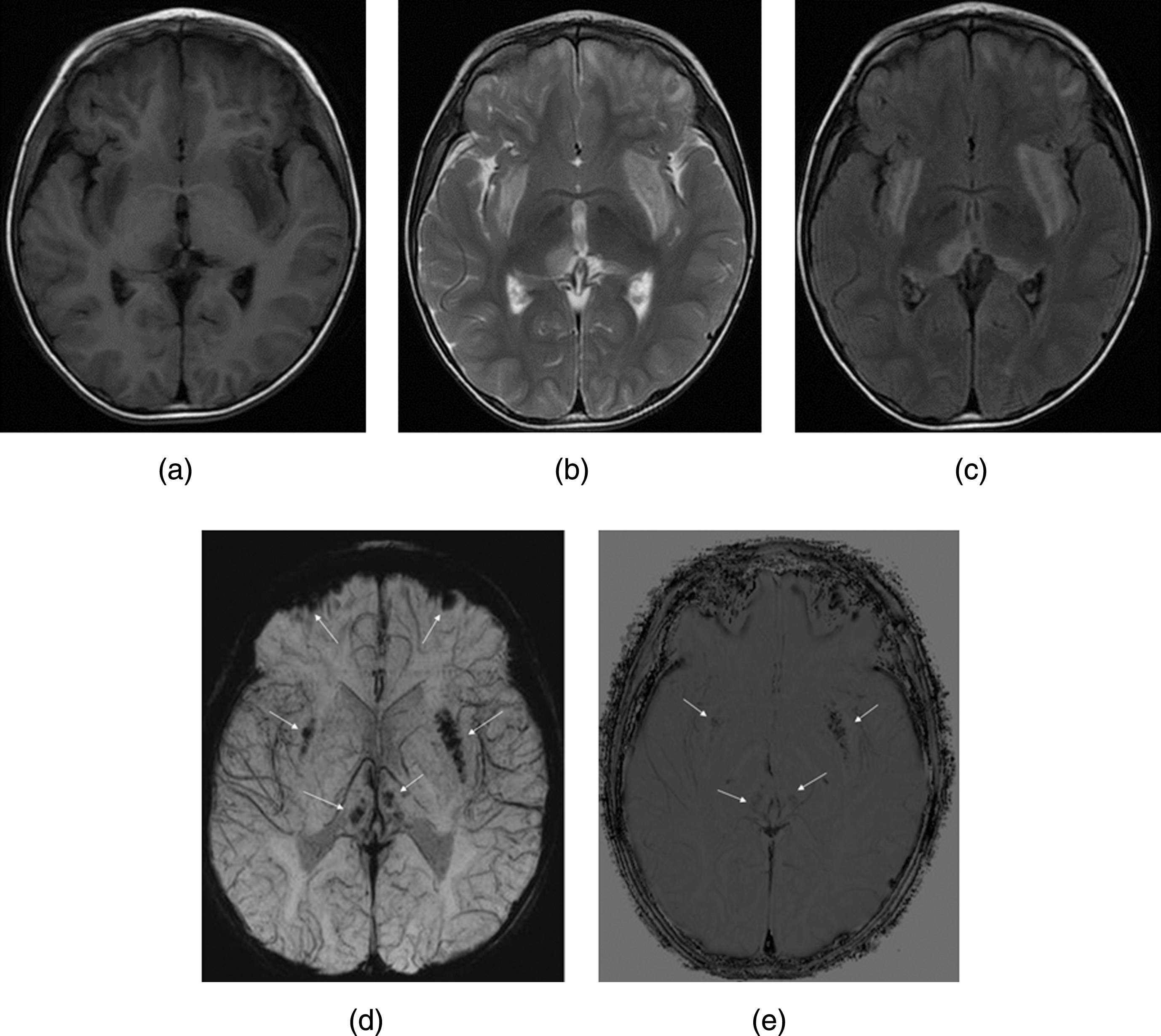
MR Images of a 9-year-old boy with viral encephalitis (group II). Transverse T1WI (a), T2WI, (b) T2-FLAIR, (c) SWI, (d) and SW phase image (e). The lesions in bilateral thalami, bilateral lentiform nucleus and bilateral frontal lobes are hypointensive on T1W image (a), while these lesions are hyperintensive, which can easily be seen on T2W image (b) and T2-FLAIR images (c). Multiple microhemorrhage foci are detected in SW image (d) and SW phase image (e) (arrows).
Viral encephalitis is a life-threatening inflammatory disease of the brain that can occur at any age and is caused by herpes simplex and other types of viruses. The prognosis of viral encephalitis is usually poor, but early treatment with antiviral agents has been proven to be efficacious. These patients usually end up with focal or diffuse neurological symptoms with temporal lobe symptoms. The brain lesions are often hemorrhagic, and a rare complication is a large intracerebral hematoma which usually carries a poor prognosis. MRI is widely accepted as a sensitive imaging technique for detecting early changes in viral encephalitis. Conventional MR sequences including T1-weighted, T2-weighted, and T2 FLAIR were used to identify abnormal areas involved in viral encephalitis. MRI shows encephalitic lesions as areas with prolonged T1 and T2 relaxation times, appearing hypointense on T1-weight and hyperintense on T2-weight images. FLAIR imaging has been reported to be more sensitive than T2-weight spin-echo sequences in detecting encephalitic lesions [7, 8].
SWI uses paramagnetic deoxyhemoglobin as an intrinsic contrast agent. Deoxyhemoglobin causes a reduction in T2* as well as a phase difference between the vessels and their surrounding brain parenchyma. The susceptibility-weighted images are displayed using the minimum intensity projection, thus highlighting the signal from the vein and minimizing the signal of adjacent brain tissues. Microhemorrhages contain various kinds of blood products (deoxyhemoglobin, methemoglobin, ferritin, and hemosiderin), and deoxyhemoglobin within a clotted hemorrhage has a marked hypointense signal and decreased T2*. With the destruction of red blood cells, the susceptibility effects of both deoxyhemoglobin and methemoglobin disappears, leading to increased signal intensity on SW images. In later stages, when ferritin and hemosiderin are formed, strong signal cancellation occurs and high susceptibility effects (manifested as reduced signal) return. This well-known T2* sensitivity to hemorrhage is enhanced with SWI [9, 10]. The advantage of high-resolution, 3D gradient-echo, high signal-to-noise ratio (SNR) makes it possible to demonstrate the microhemorrhage and small vessel at size smaller than one pixel [11–13]. The results of our study showed that SWI is more sensitive than fast spin echo sequence and FLAIR sequence for the detection of microhemorrhage in patients with viral encephalitis.
The 3.0T MR imaging equipment was used in our study. Theoretically, SNR of a 3.0T MR scanner will be doubled compared to that of a 1.5 T scanner. This higher spatial resolution can provide more precise anatomical information for viral encephalitis. High-field (3.0T) SW imaging allows for optimal susceptibility effects at shorter measurement times, therefore 3.0T MR imaging equipment has advantages for obtaining detailed, high spatial resolution images of viral encephalitis [14, 15]. There are limited reports about the application of 3.0T MR susceptibility weighted imaging for the diagnosis of viral encephalitis.
An intracranial hemorrhage may occur in viral encephalitis by different mechanisms. Some infectious agents directly promote the inflammatory reactions in the cerebral vessels resulting in vessel injury and cerebral bleeding [16, 17]. Others cause a vasculitic reaction resulting in aneurysmal formation, which rupture and bleed in the subarachnoid space. Some infectious agents produce a hypercoagulable condition, coagulopathy, thrombosis, or thrombocytopenia, leading to vessel wall disruption and intracranial hemorrhage. In adolescents and adults, herpes simplex encephalitis typically leads to focal, necrotic-hemorrhagic process within the frontal and temporal lobe. Disturbances of the microvascular circulation and breakdown of the blood-brain barrier are associated with ischemia and hemorrhage. These complications develop and determine the clinical outcome of herpes simplex encephalitis. Our results showed that microhemorrhage on SWI among the three groups of viral encephalitis was significantly different. The microhemorrhage on SWI correlated well with degree of clinical symptoms and the prognosis of viral encephalitis. The patients with large amount of microhemorrhage had lower GCS and tended to recover with more sever sequelae. These data indicated that SWI could provide useful information for the diagnosis and prognosis evaluation of viral encephalitis.
It should be pointed out that the current study is limited by a small sample size. In addition, virus detection in serum and CSF was not performed in all subjects, making it impossible to evaluate the efficacy of SWI technique in encephalitis caused by different types of viruses. Future studies with a larger sample size, more viral infection and clinical data, and follow-up SWI assessment of hemorrhage could help us to better evaluate the role of SWI sequences in viral encephalitis. Nevertheless, by demonstrating the potential of SWI technique in assessing the severity of viral encephalitis, the current study has laid a solid foundation for future studies.
Advances in knowledge
Assessment of microhemorrhage with SWI can provide useful information for the prognosis evaluation of the patients with viral encephalitis.
Conflict of interest
None.
Footnotes
Acknowledgments
This work is supported by research grants from the National Natural Science Foundation of China (No. 31271065, No. 81171385, to Q Gao).