
Abstract
BACKGROUND:
Differences often exist in the dose calculation accuracy caused by using different dose calculation algorithms in non-uniform tissues.
OBJECTIVE:
To evaluate the accuracy of dose calculation with inhomogeneity correction in intensity-modulated radiation therapy (IMRT) by comparing dose calculated in Monaco with measurements in lung-chest phantom for esophagus cancer treatments.
METHODS:
Finite size pencil beam (FSPB) and X-ray voxel Monte Carlo (XVMC) were used respectively for IMRT dose recalculations. Ten IMRT plans were recalculated and measured in the chest-lung phantom. The dose measurements using the Gafchromic ® (EBT3) dosimetry films were validated with open fields in the interfaces of materials with various physical densities. The accuracy of dose calculations was then evaluated by both point dose comparison and Gamma analysis against the film measurements.
RESULTS:
For regular open fields, the discrepancies of the point doses were less than 3.0% and 2.0% between measurement and calculations by FSPB and XVMC, respectively. For 6 MV IMRT plans, the average passing rates based on 3% /3 mm Gamma criteria were 82.8±1.0% and 96.4±0.7% for FSPB and XVMC, respectively.
CONCLUSIONS:
The XVMC algorithms more accurate in IMRT dose calculations with inhomogeneity correction for esophagus cancer.
Keywords
Introduction
The accurate dose calculation is one of the most important steps needed to be examined in the radiotherapy. The tissue heterogeneity and beam intensity modulation bring a challenge for dose calculation accuracy. The calculation time is also a critical factor in clinical practice. Therefore, various dose calculation algorithms have been developed to solve this issue. The finite size pencil beam (FSPB) and X-ray voxel Monte Carlo (XVMC) are two clinical dose calculation algorithms used in Monaco treatment planning system (Elekta, Stockholm, Sweden). While FSPB is a fast dose calculation algorithm, the XVMC has been proved to be more accurate but less efficient in dose calculation.
The esophagus cancer is one of the major cancer types in the rural areas of China. Due to the location of the treatment targets, intensity-modulated radiation therapy (IMRT) is a commonly used modality for esophagus cancers treatments. The employment of IMRT can achieve the planning goal more easily to provide enough dose to the tumors while sparing the critical organs. However, the dose calculation is more complicated in IMRT. The accuracy of dose calculation affects the dose distribution in both tumor volume and normal tissues, and, therefore, plays a critical role in the outcomes of radiotherapy. For esophagus cancer patients, IMRT beams pass through chest and lungs. The anatomical inhomogeneity results in more uncertainties of dose calculation that has become a key problem of radiotherapy treatment [1–4].
Our clinic has used FSPB and XVMC to plan esophagus cancer treatments. As mentioned in several publications, Monte Carlo algorithm is capable of dealing with the tissue inhomogeneity well in dose calculation, but requires more computation time [5–7]. Fipple has presented that the XVMC algorithm for photon beams speeds up the dose calculation and makes XVMC much more timing efficient while keeping the satisfactorily low uncertainty in the photon beam dose calculation [8]. The FSPB algorithm still have a certain error when the tissue electron densities change significantly in heterogeneous medium [9]. This study evaluated the accuracy of dose calculations of two algorithms, FSPB and XVMC, for esophagus cancer treatments with IMRT by comparing the dose calculated in Monaco TPS with the dose measured in tissue inhomogeneity phantoms.
Material and methods
An Anthropomorphic Chest-Lung Phantom (ACLP) shown in Fig. 1 and an Inhomogeneous Tissue Phantom (ITP) shown in Fig. 2 were scanned in a large bore CT simulator (GE, Fairfield, CT) with 2.5 mm thickness. We constructed the ITP phantom by inserting several pieces of solid water to ACLP phantom to build the interfaces of materials with different physical densities. The ACLP was scanned from the neck to abdomen. Other scanning parameters used for phantom scanning were 0.75 pitch, 120 kVp for the voltage, and 160 mAs for the current. The equivalent tissue density of soft tissue, lung, and bone inside both phantoms were 1.06 g/cm3, 0.28 g/cm3, and 1.68 g/cm3, respectively. During the simulation, the dummy films were inserted into the phantoms at the same positions as the measurements. We then imported the images into the Monaco TPS through the DICOM communication, and saved ACLP phantom as a quality assurance (QA) patient and ITP phantom a regular patient.

The Anthropomorphic Chest-Lung Phantom (ACLP) with a dummy film inserted.
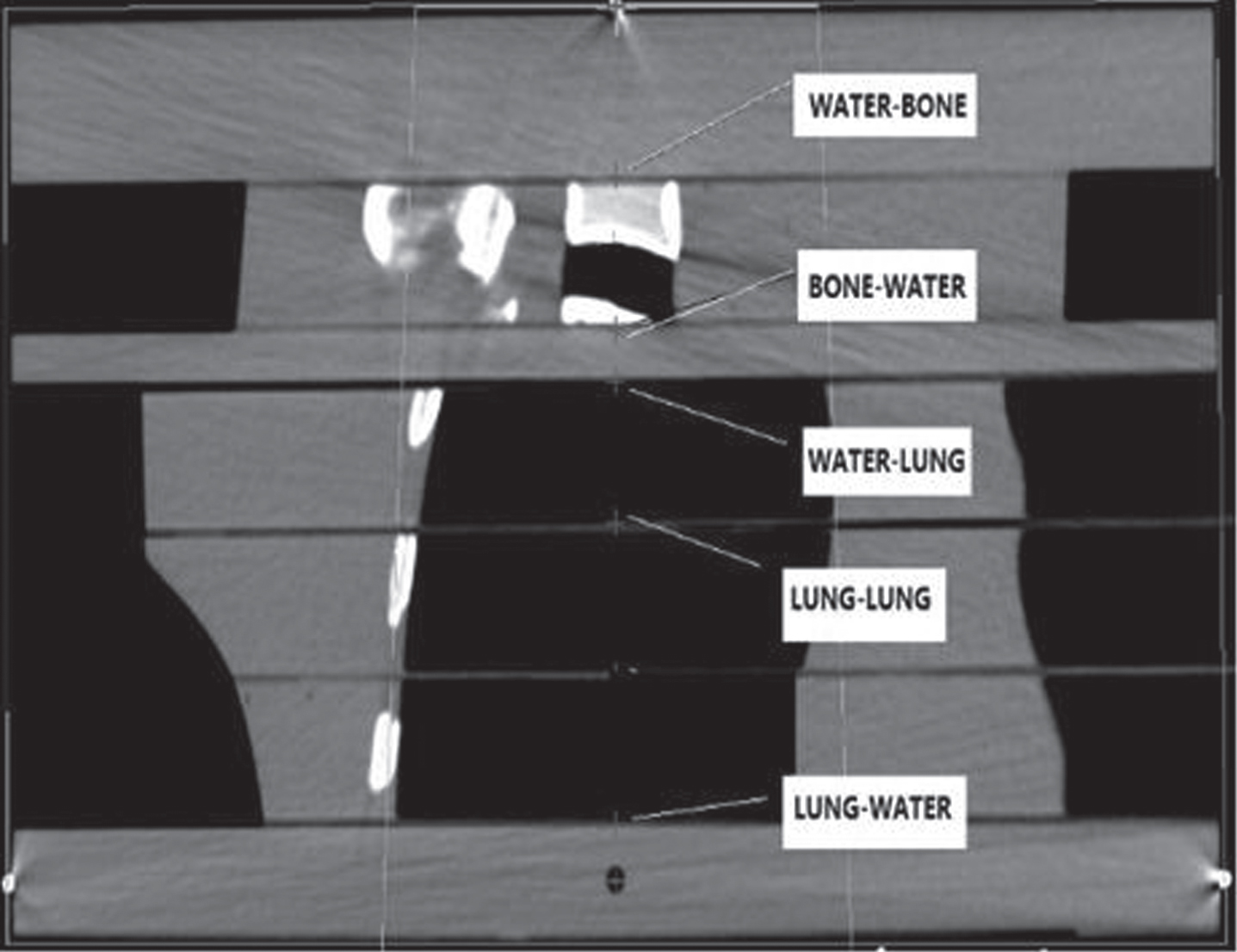
The measurement points shown in Inhomogeneous Tissue Phantom (ITP). The WATER-BONE, BONE-WATER, WATER-LUNG, LUNG-LUNG, and LUNG-WATER indicate the interface of two tissues, respectively, water and bone, bone and water, water and lung, lung and lung, and lung and water.
In order to validate the accuracy of the phantom measurement with filming, we generated several regular open fields in ITP phantom. The beam energies were 6 MV and 15 MV, the gantry angles were zero, and the field sizes were 10 cm×2 cm and 10 cm×10 cm. For each field, 100 MU was delivered with SSD setup. The doses were calculated in these single open field plans by both FSPB and XVMC algorithm. The doses at five interesting points shown in Fig. 2 were calculated. They were located, respectively, in the interface between water and bone, bone and water, water and lung, lung and lung, and lung and water. We measured the dose by use of the EBT3 films in the same ITP phantom location. The irradiation beams were aligned either to be perpendicular to films from superior direction or to be parallel to films. The measurements were repeated three times for each plan. The point doses were measured at the interface of various densities and compared to the values calculated with the regular open fields.
The beams with the field sizes of 10 cm×2 cm were setup at 25 degree of gantry angle for the dosimetrical validation in the ACLP phantom. The beam energies were 6 MV and 15 MV. For each field, 100 MU were delivered with SAD setup and were calculated by both FSPB and XVMC algorithm. The ACLP phantom was set up by the alignment of three BBs with lasers after having EBT3 films inserted. In the ACLP phantom measurement, 2D dose analysis were performed. The films were parallel to each beam and recorded as a 2D dose distribution. Films were marked on the phantom surface to align the measured dose distribution to the calculated dose distribution. The 2D dose comparison was executed in FilmQA Pro V3.0 by checking the dose using the Gamma analysis. The horizontal and vertical dose profiles are also compared quantitatively.
The evaluation of dose calculation employs ten randomly selected clinical IMRT from those used for esophagus cancer treatments. Each IMRT plan has five co-planner beams and all beams used 6 MV. All IMRT plans were optimized with the minimum MU of 4MU and the minimum segment area of 2 cm×2 cm. After copying the plans to the ACLP phantom, the doses were re-calculated by setting the same MUs for each plan using two algorithms, FSPB and XVMC, respectively. The dose grid was 3 mm×3 mm×2.5 mm for both recalculations. Each plan was exported individually to the treatment machine, Varian 23Ex (Varian, Palo Alto, CA, USA) for dose measurement. The measurements were performed in the same ACLP phantoms which had GafChromic films inserted to record the dose. In the ACLP phantom measurement, Fig. 4 shows the interesting points doses were measured in each IMRT plan using the EBT3 film.
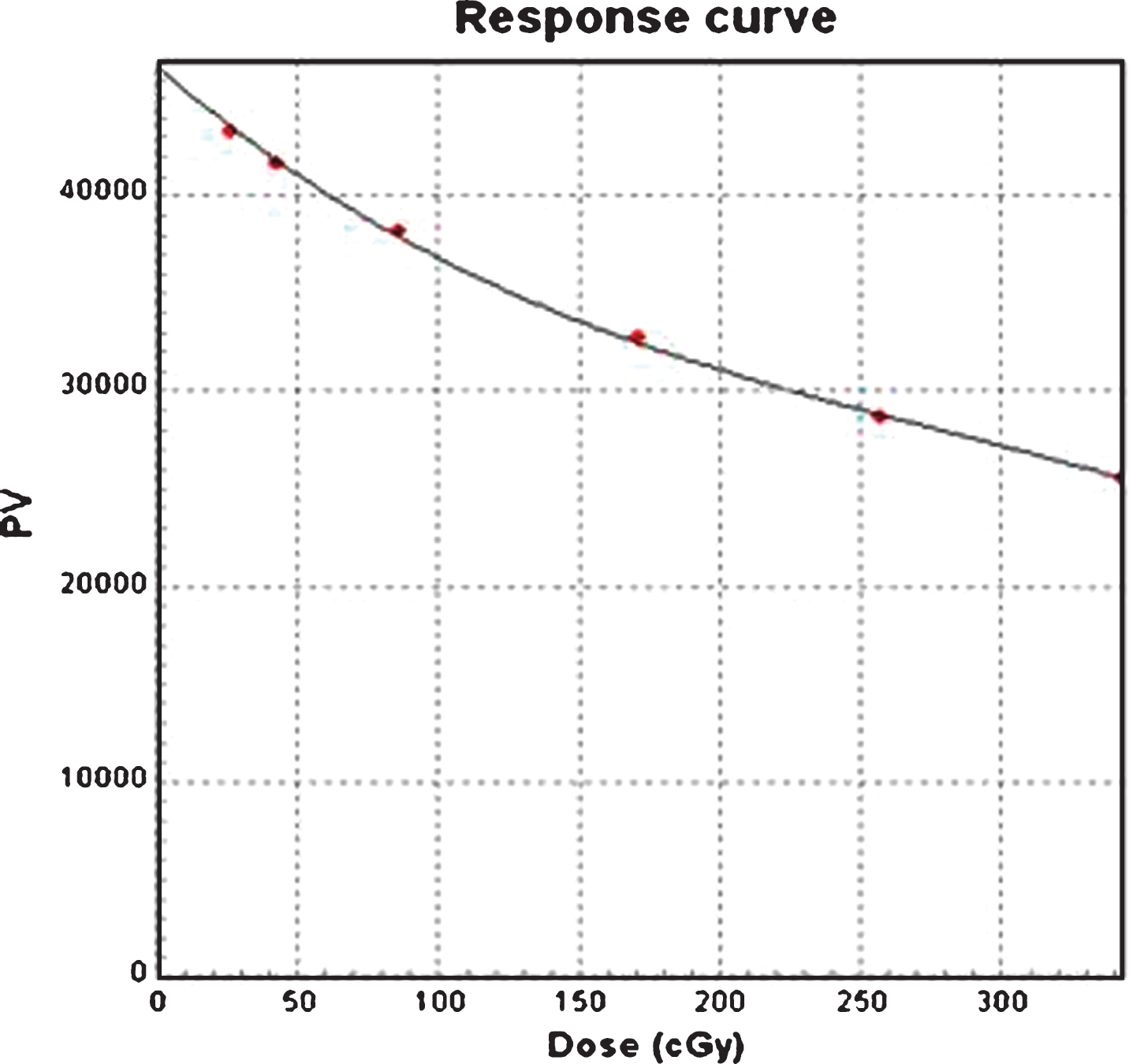
EBT3 film calibration response curve. PV stands for the Pixel Value that was measured from the calibration films.
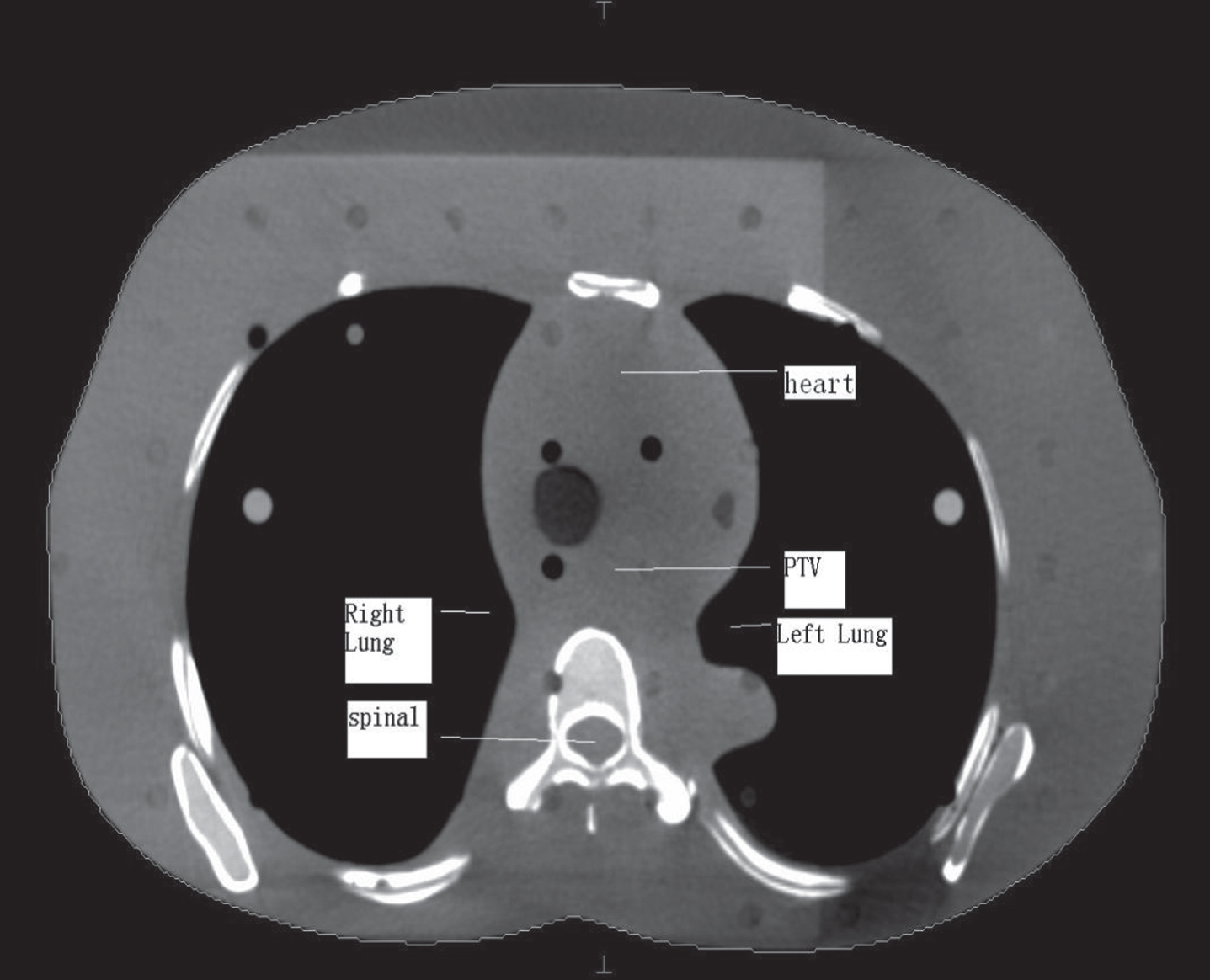
The interesting points related to in the phantom the target and critical structures shown in the ACLP phantom.
The film dosimetric calibration utilized an EPSON flat panel film scanner, Perfection v750 Pro, (EPSON, Seiko Group, Japan) and a film dosimetry analysis software, FilmQA Pro V3.0, (PEO Radiation Technology, Wijchen, Nederland). The film calibration procedure follows the guideline stated in the papers [10, 11] A series of films were exposed to certain amount of radiation under standard beam calibration condition. After exposure, each film was kept in the dark room for 2 hours before scanning and an unexposed EBT3 film was scanned too as the background dose correction. The films were scanned and the images were saved as TIF files with imaging resolution of 48 bits and 75 dpi. The film dosimetric response curve was generated by giving each film a value that was identical to absolute dose to the center of the film exposure field. As shown in Fig. 3, the film dose response ranged from 0 to 350 cGy. The response curve was verified through a measurement of an EBT 3 film to which the given dose was delivered.
The results of the point dose measured in the ITP phantom for the open fields are shown in Table 1. The discrepancies of the point doses between film measurement and TPS calculation using XVMC algorithm were less than 2% at all points for two photon energies and two open fields in the heterogeneous environment. The discrepancies between measurements and FSPB algorithm calculation could be more than 2% and 3% for 6 MV and 15 MV photon beams, respectively. Obviously, the calculation error of XVMC algorithm was less than FSPB algorithm. On the other hand, the point dose discrepancies were small in the 10 cm×10 cm field for FSPB algorithm, while this tendency was not shown in XVMC algorithm calculations. The maximum point dose discrepancies for FSPB algorithm were at the interface of lung to water and up to 6% for the smaller field using 15 MV beam.
The average percentage discrepancies of point doses between the film measurements and the Monaco calculations in open field
The average percentage discrepancies of point doses between the film measurements and the Monaco calculations in open field
Note: X— ray voxel Monte Carlo (XVMC); Finite Size Pencil Beam (FSPB).
The Gamma passing rates of 2D dose analysis for the 10 cm×2 cm open field
Note: DTA means Distance to Agreement.

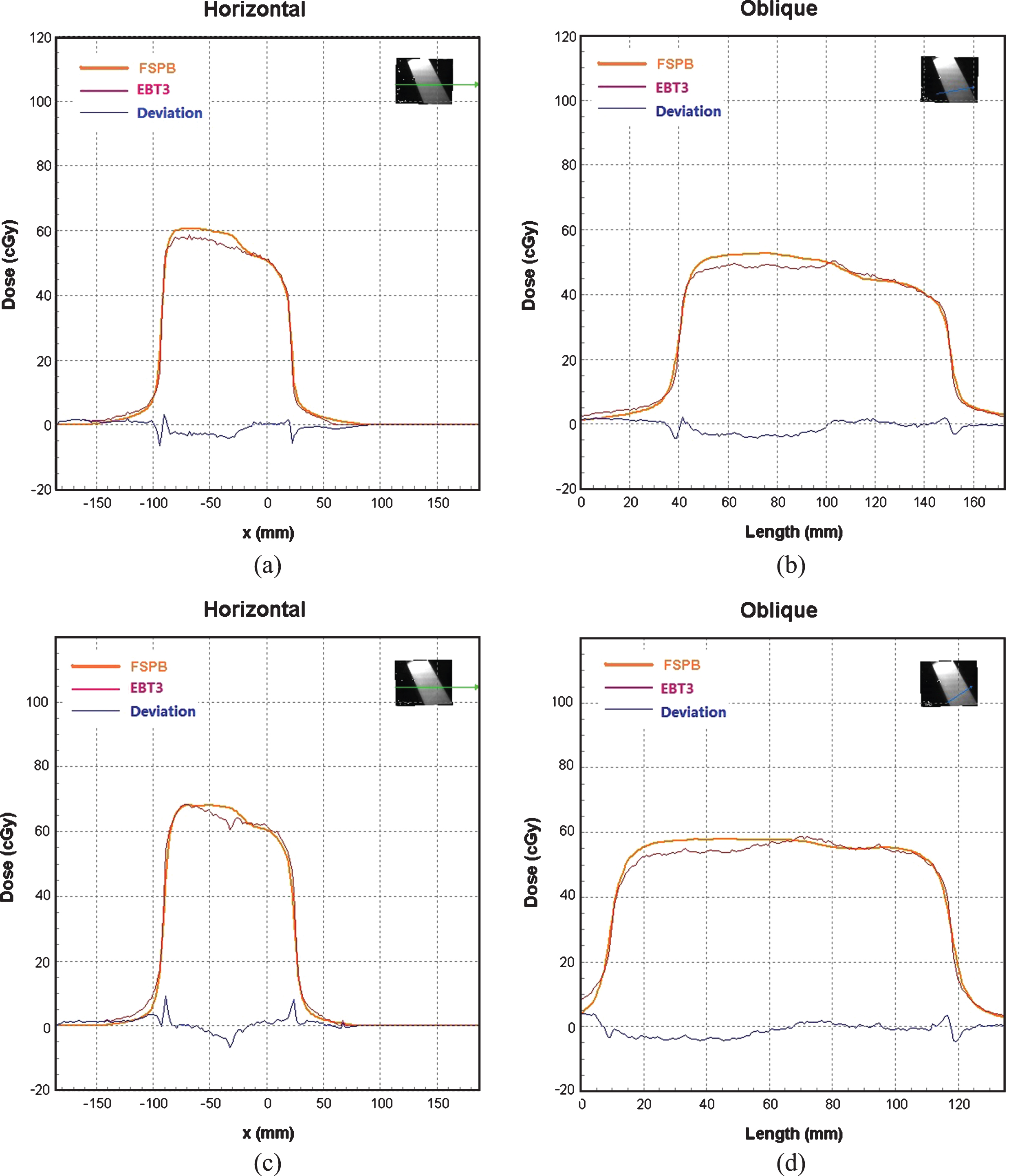
The profiles of 2D dose comparison between the film measurement and XVMC calculations. The measurement made by 6 MV beam are shown the results in (a) and (b) and by 15 MV in (c) and (d).
Table 3 shows the Gamma passing rates of 2D dose analysis for 10 IMRT film measurements in ACLP phantom. The passing rates were 96.41±0.71% and 82.81±1.01% for comparing the measured doses to XVMC and FSPB calculated doses, respectively, using 3% /3 mm gamma index. The passing rate was 91.77±0.98% for comparing to the FSPB dose if gamma index increased to 4% /4 mm. For comparing the doses calculated with two algorithms, XVMC and FSPB, the average passing rate was 60.1±5.4% using 3% /3 mm gamma index. The passing rate increased to 85.2±4.6% with 4% /4 mm. Table 4 shows the average doses calculated using the algorithms of FSPB and XVMC and measured using EBT3 films for 5 points of interest. The percentage discrepancies of point doses between the XVMC calculation and the film measurement are less than 0.3% for all point measurements. However, between the FSPB calculation and the measurement they could be more than 2.5%. These results are consistent to the results of 2D dose comparisons using the ITP phantom.
The Gamma passing rate of dose comparison for 10 IMRT plans using Gamma index Analysis
Average point doses calculated in TPS and measured by films in 10 IMRT planning and measurements
According to ICRU report [12], the error of 3% in dose calculation might lead to a total uncertainty of 4.3% in radiotherapy delivery or even higher. As an inversely planning, IMRT has more complicated dose calculation procedures. It is even more challenging to ensure the correctness and accuracy of IMRT dose calculation with inhomogeneity correction. Film dosimetry has been widely used in clinic due to its high resolution and reliability [13–15]. However, the film dosimetry may depend on several factors and the film dose calibrations have to be verified. In this study, the EBT3 films were carefully calibrated before the dose measurements to eliminate the potential uncertainty caused from film itself and post-measurement processing.
Tables 1 shows the results of the point dose comparisons. The discrepancies resulted from comparing the measurements of 6 MV small open fields and IMRT to FSPB calculations are obviously larger than to XVMC calculations in the interface of lung to lung inside the ITP phantom. More interesting is the results shown in the Fig. 5: The right half of profile matches well between the FSPB calculation and the measurement but the left half was not. The mismatch is due to the location of the right half of films in water equivalent tissues and the location of the left half of films in lungs. In the comparison of the FSPB calculations and the measurements for IMRT plans, most of the point pairs which did not meet the 3% /3 mm Gamma criteria were also found to be located in lung areas. It is no doubt that the FSPB algorithm used in Monaco system do not calculate the dose accurately in low-density tissues such as lungs. In another hand, as shown in the results of the comparison of XVMC calculation with the measurements in ACLP phantom, all measurements of IMRT for esophagus treatment had a 3% /3 mm Gamma passing rates more than 95%. Similar results have been seen in the comparisons of the XVMC calculation with the ITP phantom open field measurements.
Table 2 shows an increase of Gamma passing rates from about 82% using the index of 3% /3 mm to 95% using 4% /4 mm in 2D dose comparison with FSPB calculations. The similar Gamma passing rate increase with the index change from 3% /3 mm to 4% /4 mm indicates that certain amount of points had the dose calculation difference from 3% to 4% in 2D dose comparisons.
The profiles of 2D dose comparison between the film measurement and FSPB calculations. The measurement made by 6 MV beam are shown the results in (a) and (b) and by 15 MV in (c) and (d).
In IMRT planning for esophagus treatment, the dose calculated in low density tissues by FSPB algorithm is higher than the measurements. This phenomenon can be explained by the results shown in Table 1. The discrepancies of doses between the FSPB calculation and the measurements were larger for the smaller open field of 10 cm×2 cm and the higher energy beams. FSPB is one of the algorithms in which the local dose distribution function called as Kernel does not work accurately inside the low density tissues such as lung [8]. Our results verify the previous reports that the calculation error was large to high-energy rays when the larger changes of density was occur in heterogeneous medium [16, 17]. The range of the secondary electrons which were created by photons interactions within the ITP phantom is larger when the energy of incident photon was higher and the part of the side scattering of secondary electrons could be missed in the inhomogeneity environments. The larger field size of beams, the less scattering dose is lost. As shown in Table 1, the beams delivered with open fields of 10 cm×10 cm had a smaller difference of point doses between the measurements and FSPB calculations.
Another study also emphasized that the dos calculation error could be up to 18% when the pencil beam algorithm was used in treatment planning of lungs [18]. From this study, it shows that the FSPB dose calculation is not accurate either for the esophagus treatment planning, but the dose overestimation in FSPB calculation is not as high as more than 7% if treated by 6 MV IMRT. The IMRT plans having higher energy beams could produce higher calculation errors using FSPB algorithm and certainly should be avoided in esophagus cancer treatments.
The esophagus cancer IMRT should use XVMC dose calculation algorithm in Elekta Monaco system. The FSPB algorithm in Monaco has a dose calculate error more than 3% in chest-lung areas in IMRT planning and should not be used for esophagus treatments.
Footnotes
Acknowledgments
The study was supported by Science and Technology Department of Fujian Province (NO.2016Y0044) and Fujian Provincial Health and Family Planning Commission(NO. 2016-CX-19).