
Abstract
21-hydroxylase deficiency is a rare kind of autosomal recessive disorders, which can result in congenital adrenal hyperplasia and/or testicular adrenal rest tumors. 21-hydroxylase deficiency with TARTs is prone to be misdiagnosed as Leydig cell tumors. Although the sonographic characteristics of TARTs have been summarized in previous reports, its features in computed tomography images were rarely reported. In this study, we presented and summarized the clinical and imaging data of a special case suffering this disease, aiming to improve the imaging diagnosis performance.
Introduction
21-hydroxylase deficiency is a rare kind of autosomal recessive disorders and also the most common cause of congenital adrenal hyperplasia (CAH) [1]. It refers to the partial or complete deficiency of 21-hydroxylase in adrenocortical hormone synthesis, which results in the decline of cortisol synthesis and the continuous secretion of adrenocorticotropic hormone (ACTH), as well as the further congenital adrenal hyperplasia (CAH) and/or testicular adrenal rest tumors (TARTs). 21-hydroxylase deficiency with TARTs is prone to be misdiagnosed as Leydig cell tumors (necessitating surgical treatment) in an imageological examination. Although the sonographic characteristics of TARTs have been summarized in previous reports, its features in computed tomography (CT) images were rarely reported. In this study, we have summarized the clinical and imaging data (including ultrasonography and CT images) of a case suffering 21-hydroxylase deficiency with TARTs in 2017, aiming to improve the imaging diagnosis level.
Case report
A 20-year old male was found suffering the bilateral testicular swelling, with no sperm. As shown in ultrasonography (Fig. 1), there were multiple solid masses in his bilateral testicles, which were diagnosed as testicular tumors subsequently. Hence, the patient was hospitalized for suffering from “bilateral testicular tumors”.
Relevant medical history and laboratory examinations were further provided after his admission into our hospital. As a full-term newborn, he was born weighing 3 kilograms. Subject to the mixed feeding, he began to vomit frequently 20 days after his birth, in an interval of 4–10 days. Such symptoms were relieved after he was injected with normal saline, and it finally disappeared after he was one year old. Despite his larger scrotum and penis than his peer, this patient had normal stature and weight during his 6 months old. When he was 5-year old, his penis and scrotum began to grow, together with pigmentation and pubic hair (but without armpit hair). At the age of 12, he stopped growing, with his stature ceased at 1.5 meters. Examinations revealed his normally developed perineum and obviously swelling bilateral testicles, with a hard handfeel and palpable nodules. Relevant laboratory results were summarized in Table 1. Computed tomography (CT) images also showed nodular enlargement of his bilateral adrenal glands, with uniform and obvious enhancement (Figs. 2, 4A), and his bilateral testicles were found with significantly enhanced masses (Fig. 3).
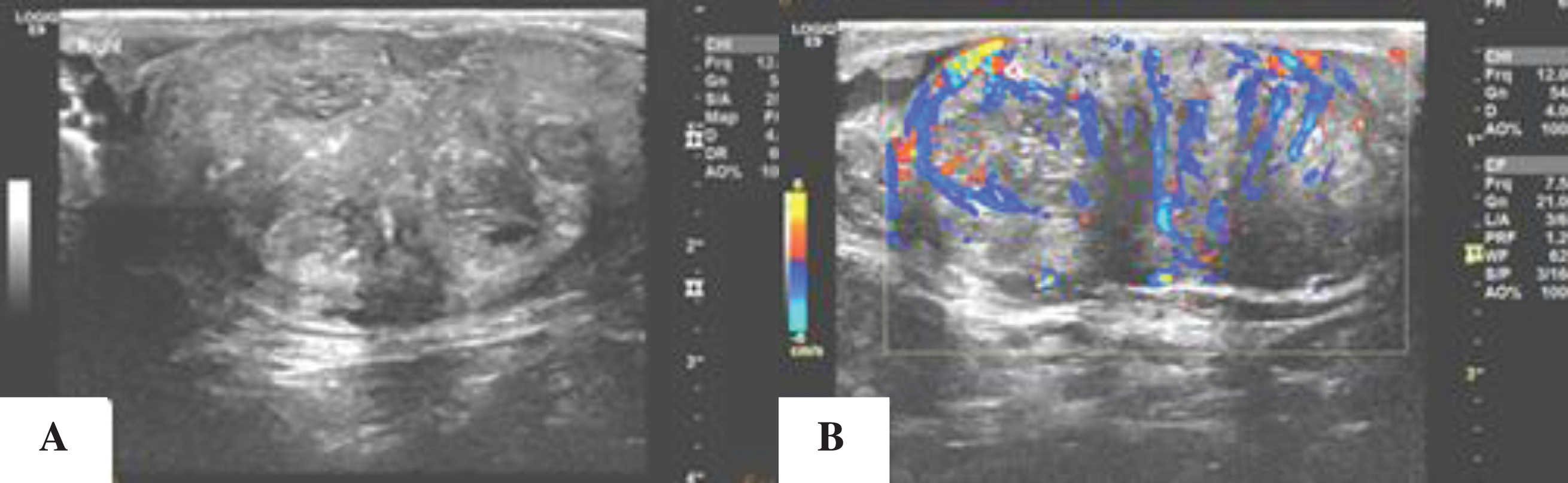
The enlarged testicle, with solid hypoechoic masses. Their boundaries were still clear, but the boundary of normal testicular tissue was unclear (1A). A rich blood supply was shown in the lesions (1B).
Relevant laboratory tset results

Bilateral adrenal glands having obvious nodular hyperplasia, with obvious and uniform enhancement (2A: CT non-contrast image; 2B: CT enhanced image).
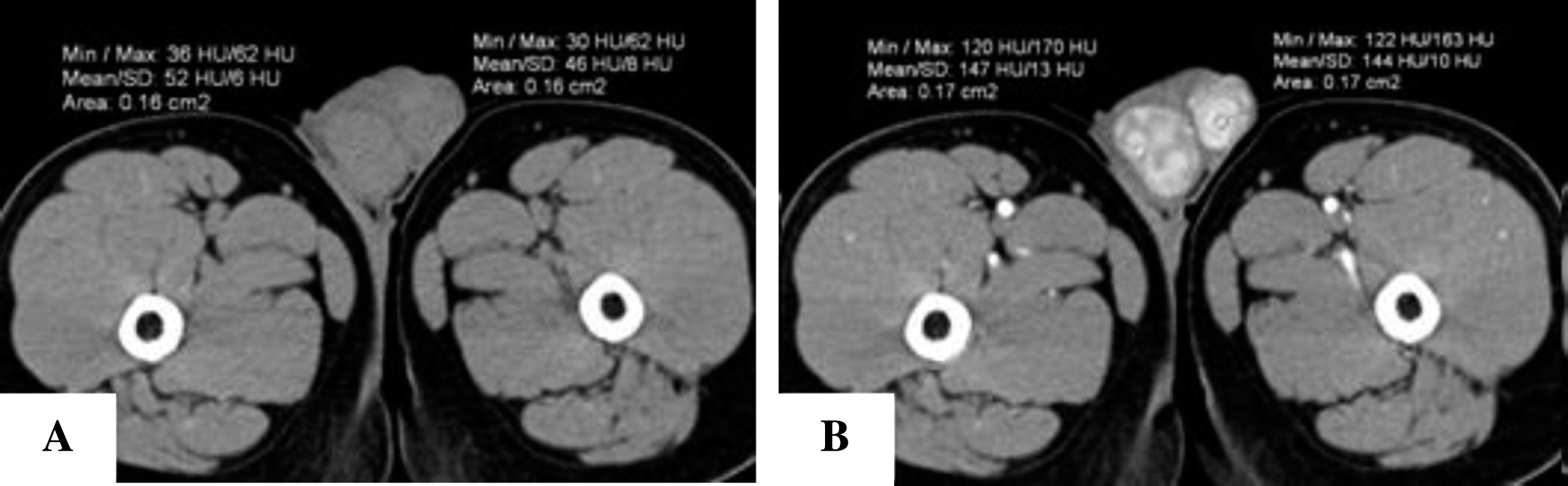
Bilateral testicles with multiple masses, which were also significantly enhanced (3A: CT non-contrast image; 3B: CT enhanced image).
This patient suffered sexual precocity. His ACTH, progesterone and precusor substance of androgen were all enhanced. The CYP21A2 gene was detected to be positive in 21-hydroxylase deficiency, and one homozygosis pathogenic mutation was detected via Sanger sequencing. Finally, he was diagnosed as congenital adrenal hyperplasia with TARTs caused by 21-hydroxylase deficiency. Both his AFP and HCG were normal. After the glucocorticoid replacement therapy, his testosterone and 17-OHP levels declined, and his testicular tumors shrank. Hence, his symptoms were further confirmed as TARTs.
Description of 21-hydroxylase deficiency
21-hydroxylase is an enzyme necessary in adrenocortical hormone synthesis. Its deficiency accounts for more than 90% of CAH cases [1]. Specifically, such deficiency causes the lack of glucocorticoid and mineral corticoid, as well as the accumulation of 17-OHP, together with an excessive secretion of adrenal androgen. According to the severity of its clinical symptoms, CAH is divided into the classical and non-classical types. Based on the lack of 21- hydroxylase, such classical type is further divided into the salt wasting (SW) and simple virilizing (SV) types.
Salt wasting CAH is the severer type, accounting for 75% of classical cases [2] as estimated, and its enzymatic activity is less than 2% of the normal. Patients suffering salt wasting CAH are deficient in their cortisol and aldosterone. The female often shows masculine symptoms caused by hyperandrogenism, such as the labium closure resembling scrotum, and the clitoris hypertrophied like penis. At the same time, relevant symptoms often occur within 1-2 weeks after birth, such as feeding difficulties, vomiting, diarrhea, weight loss, dehydration, acidosis, low sodium, hyperkalaemia, adrenal crisis, etc., all of which are difficult to be corrected. In case of failure to receive timely treatment with glucocorticoids during postnatal development, both male and female could, along with the development of classical CAH, show signs of androgen excess, including precocious pubarche, acne, rapid linear growth, and advanced bone age leading to an underdeveloped final height [3, 4].
Compared to SW CAH, SV CAH is resulted from about 1-2% increase of the enzyme activity. It accounts for around 25% of all the classic CAH cases. In this disease, cortisol secretion is normal or slightly decreased, and aldosterone secretion is roughly normal. Hence, it is possible to maintain physiological functions, and it may only be presented as different virilism levels of female vulva caused by hyperandrogenism. The male suffering SV CAH is often born with normal or slightly enlarged genitalia, exhibiting scrotal pigmentation. Absence of a timely treatment could result in peripheral precocious puberty caused by the enlarged penis.
Non-classical congenital adrenal hyperplasia (NCAH) is caused by a partial 21-hydroxylase deficiency, typically resulting in decline of normal function to 20–50% approximately [5]. Compared to classical CAH, NCAH‘s clinical presentation shows later and dissimilar. Cortisol and aldosterone secreted by the adrenal cortex prevent clinical deficiencies necessitating hormone replacement therapy. Although the need for such therapy is relieved, cortisol produced by the adrenal glands is insufficient to suppress the over secretion of ACTH, while the shunting of precursor steroids results in hyperandrogenemia. Most children with NCAH are asymptomatic in prepubertal years, who have normal genitalia at birth. They tend to be undiagnosed while experiencing normal growth, puberty, and reproduction, who may be finally diagnosed in kindred studies [6]. Clinical presenting signs of NCAH in children may include accelerated growth, premature pubarche, cystic acne, and/or bone age advancement. Later in life, common presenting features including hirsutism, acne, menstrual cycle disorders and decreased fertility can be presented. These features are likely secondary to excess androgens in circulation. Features in male are less evident, and they may remain asymptomatic or present with acne and/or impaired fertility.
Causes and diagnosis of TARTs
Testicular adrenal rest tumors (TARTs) were firstly described by Wilkins et al. in 1940 [7]. They are benign intratesticular masses, also a potential complication in males with CAH [2, 8]. According to the studies performed on children, it is found that TARTs can be detected in childhood, with a prevalence of 18.3%–29% [9–10]. Among male patients, its prevalence is nearly 94% [11]. The causes of TARTs are still unclear. Both the adrenal cortex and testicles are believed to derive from the mesoderm body cavity epithelium. During the embryonic development, a small amount of adrenal gland cells descend with testicles, and that’s why they are called as adrenal gland rest cells. There is a hypothesis that, chronic overstimulation of adrenal tissue remnants in testicles (which normally regresses before a baby’s birth) can lead to TARTs [12, 13]. TARTs impair spermatogenesis and testicle‘s endocrine function. As a result, poor hormonal control leads to the enlarged TARTs, which further affects fertility [14, 15]. In this case, the patient also suffered from aspermia symptom.
Pathologically, TARTs resemble the adrenocortical tissue [16]. Compared to Leydig cell tumors (LCTs), TARTs lack the symptoms as cytological atypia, lymphoid aggregates, adipose metaplasia, low mitotic activity, prominent lipochrome pigment and dense fibrous septa [17]. Reinke crystals are absent in TARTs, which can, however, be found in 25–40% of LCTs. About 10% of LCTs are malignant, while there is almost no report on the malignance of TARTs [18, 19]. Immunohistochemically, TARTs display focal or diffuse strong reactivity for synaptophysin, diffuse and strong positivity for CD56. In contrast, LCTs show focal weak or negative reactivity for synaptophysin and focal weak to moderate or negative reactivity for CD56. In addition, TARTs show negative reactivity for the androgen receptor, compared to which the LCTs display positive reactivity [20, 21].
Imaging findings
In this case, the patient‘s bilateral adrenal glands exhibited obvious nodular enlargements, as well as obvious and uniform enhancements, which were different from the signs exhibited in other adrenal tumors. Hence, they were diagnosed as adrenal hyperplasia.
Both LCTs and TARTs can be presented as mass lesions in testicles. According to the previous reports, more than 80% cases of TARTs were bilateral, compared to which only 3% cases of LCTs were bilateral [18]. In this case, the patient’s bilateral testicles were both found with multiple masses. As shown in the ultrasound images, such TARTs were adjacent to the mediastinum testis and enjoying a rich blood supply, which was consistent with previous reports [22]. Compared to LCTs, TARTs‘ enhancement was shown more obviously in the CT enhanced image, to the same extent with that enhancement of hyperplastic adrenal glands. This may be an evidence revealing their same origin. Besides, we also found thick and circuitous testicular arteries and veins around the lesions (Fig. 4B), which were uncommon in LCTs.
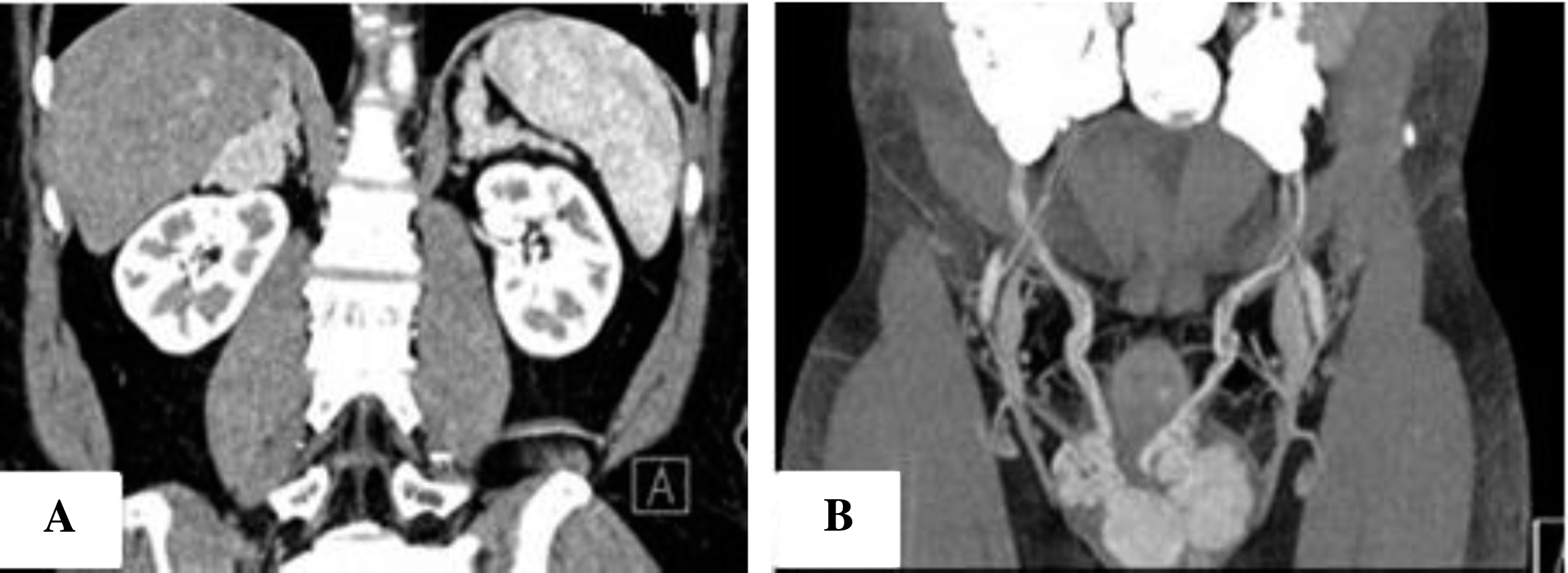
Bilateral adrenal glands (as shown in CT coronal image) having obvious nodular hyperplasia (4A). As shown in the maximum intensity projection (MIP) image, there were thick and circuitous testicular arteries and veins around the lesions (4B).
In general, when features of adrenal hyperplasia accompanied with testicular masses are detected in the imaging examination, we shall dwell on the possibility of such disease, with relevant laboratory examinations recommended to avoid the misdiagnosis of such disease as Leydig cell tumors and consequent orchidectomy.