
Abstract
Purpose:
To evaluate the clinical efficacy of percutaneous trans-hepatic integrated 125I seed stents implantation for malignant lower biliary tract obstruction.
Methods:
Thirty-two patients with malignant lower biliary obstruction were randomly divided into two groups. One group underwent the therapy with integrated 125I seed stents (Test group, n = 13), and another group received conventional metal stents implantation for treatment (Control group, n = 19). The pre- and post-operative changes in biochemical indices, white blood cell count, IgG level, stent patency, survival time, tumor size and complications were compared between the two groups. RECIST 1.1 (Response Evaluation Criteria In Solid Tumors) was used to evaluate therapeutic effects. The average follow-up time was 12.3 months.
Results:
The differences between pre- and post-operative (30 days) intragroup biochemical indices had statistically significant difference (P < 0.05), but there were no significant differences (P > 0.05) in leukocyte counts and IgG levels. As to the median time of stent patency and patients’ survival, there were significant differences (P < 0.05) between Control and Test groups (3.9 months vs. 8.1 months, 139 days vs. 298 days, respectively). Three months after the operation, the average tumor size was reduced in the Test group, but was increased in the Control group (P < 0.05). There was no significant difference in the incidence of complications between the two groups. The evaluation results using RECIST 1.1 showed that there were statistically significant differences between the two groups in terms of the rates of remission, control, and progression (χ2 = 17.5, P < 0.05).
Conclusions:
The study indicates that integrated 125I seed stents are effective in reducing jaundice symptoms, inhibiting tumor growth, improving stent patency and prolonging patient survival, which may serve as a safer and more feasible method in treating malignant lower biliary obstruction with minimal invasiveness.
Introduction
Percutaneous transhepatic biliary stents (PTBS) have become the most common palliative therapy for malignant biliary tract obstruction [1–5]. However, stents only play a role in drainage with no inhibitive effect on tumors, and might induce an in-stent restenosis or obstruction in a long run, which has been a key factor affecting the therapeutic efficacy [6–9]. Some scholars treated malignant biliary tract obstruction with stent combined with radiotherapy or chemotherapy, but the effect has not been ideal [10, 11]. In the recent years, it has been reported that the stent implantation combined with percutaneous puncture implantation of 192Ir, 125I, or other radioactive isotopic particles, can be used in treating malignant biliary tract obstruction by relieving obstruction with stent and resisting the tumor with brachytherapy, showing a better efficacy in extending the patient survival period [12–15]. Nevertheless, this therapy is greatly restricted by the location and morphology of lesions. In fact, 125I radions are hard to be evenly distributed at lesion locations through the percutaneous implantation, which may impact the therapeutic effect [16]; besides, patients have to undergo many puncture surgeries, which increases the treatment cost and risk.
To date, a few animal experiments and clinical studies with internal radiation biliary stents have shown preliminary efficacy and safety of particle stent [17–20]; however, these nonintegrated radiation stents usually require two interventional operations, and there are still many internal radiation biliary stent-related issues to be solved. To further study the feasibility, safety and effectiveness of integrated internal radiation biliary stents in clinical application, we conducted a prospective study for the clinical value of integrated 125I particle stents in the treatment of malignant low biliary tract obstruction, as well as comparative study with ordinary metal stents in terms of biliary drainage, liver function, complications, stent patency period, tumor size and survival period. Our study shows that the integrated 125I seed stents are more effective in reducing jaundice symptoms, inhibiting tumor growth, improving stent patency and prolonging patient survival than the conventional metal stents.
Materials and methods
Information of patients
From September 2014 to November 2016, a total of consecutive 78 patients with malignant obstruction of the lower biliary tract were included for the prospective study, and all of them had clinical manifestations including yellowish skin and mucosa, dark yellow urine, abdominal distention, poor appetite and weakness. The laboratory examination showed significant increases in serum total bilirubin and direct bilirubin. Their preoperative jaundice lasted for 9 to 78 days, with an average of 36 days. According to the imaging examinations (abdominal CT and MRI), all patients showed lower biliary tract obstruction below the porta hepatis, dilated biliary tract above the obstruction, and linear sign or beak sign at the obstruction, while some of them presented sudden truncation. Inclusion criteria for eligible patients in the trial were, (1) any case shows malignant lesion that should be patho-histologically or cytologically confirmed; (2) any case diagnosed as lower biliary tract obstruction by type-B ultrasound, CT or MR, has clinical symptoms directly related to biliary obstruction; (3) any case which has no surgical indication but willing and able to receive this study procedures; and (4) any case that has no absolute contradiction for this interventional operation. Exclusion criteria were: (1) any case having biliary tract obstruction caused by benign lesions; (2) any case that was treated through surgery, endoscopic stent implantation or drainage tube; (3) any case having widespread liver lesions; (4) any case having so stiff and tough biliary tract obstruction that cannot be dilated and penetrated by stent; and (5) any case having incomplete follow-up data.
This study was approved by the Hospital Ethics Committee. Before the treatment, all patients were informed about the potential benefits and risks involved in the therapy and they signed the informed consent. The patients were divided into two groups in accordance with the randomization table; one group was implanted with ordinary bare metal stents (control group), while the other group was implanted with 125I particle stents (test group).
Therapeutic method
The ordinary stent group
All cases were given antibiotics to prevent infection and other necessary supportive treatments for protecting the liver and reliving the jaundice 3 days prior to the surgery. All cases received 50 mg dolantin intramuscular injection 30 minutes before the surgery. All surgical procedures were performed under the guidance of DSA. Basically, a 21 G micro-puncture needle (Cook, USA) was delivered percutaneously and transhepatically into the intrahepatic bile duct. A small amount of contrast agent was injected to confirm the needle tip inside the intrahepatic bile duct. Then, a 0.014in micro-guide wire (Cook, USA) was inserted into the bile duct, with a 6F expanding sheath (Cook, USA) along the micro-guide wire. Next, the micro-guide wire was replaced with a super-slip guide wire (Terumo, Japan), which was placed into the duodenum along the common bile duct obstruction section. Finally, the catheter was sent along the guide wire, and the guide wire was pulled out. DSA also showed the specific obstruction location and length to help select an appropriate stent. Afterwards, efforts shall be made to replace with a super-hard guide wire, send the stent pushing system along the guide wire, anchor the stent location under DSA, and slowly implant the stent (produced by Mirco-tech, Nanjing, China). Please notice that the stent shall be 1-2 cm longer than the obstruction section.
The particle stent group
(1) 125I particles: 125I sealant particles produced by China Institute of Atomic Energy (Reactor Engineering Research and Design Institute) are cylindrical and 4.8 mm long, with a diameter of 0.8 mm and half-life period of 59.6d; their energy is 27.4–3l.5kev X ray and 35.5kev γ ray, with the effective irradiation range between 1.7 and 2.0 cm; (2) 125I particle stent: The treatment planning system (Beijing Astro Technology Co., Ltd., China, registration No.: the same as SYJ (Z) [2009] No. 3700398) was used to calculate the dosage required by the tumor focus area and its adjacent tissues, and to draw the isodose curve and the particle distribution diagram. Subsequently, as per the treatment plan, accurate number of particles were implanted into the hollow biliary tract stent made of polytetrafluoroethylene membrane to make the particle stent (Fig. 1a); (3) 125I particle stent implantation: the same basic steps as with ordinary stents were followed and was shown in Fig. 1b-e.
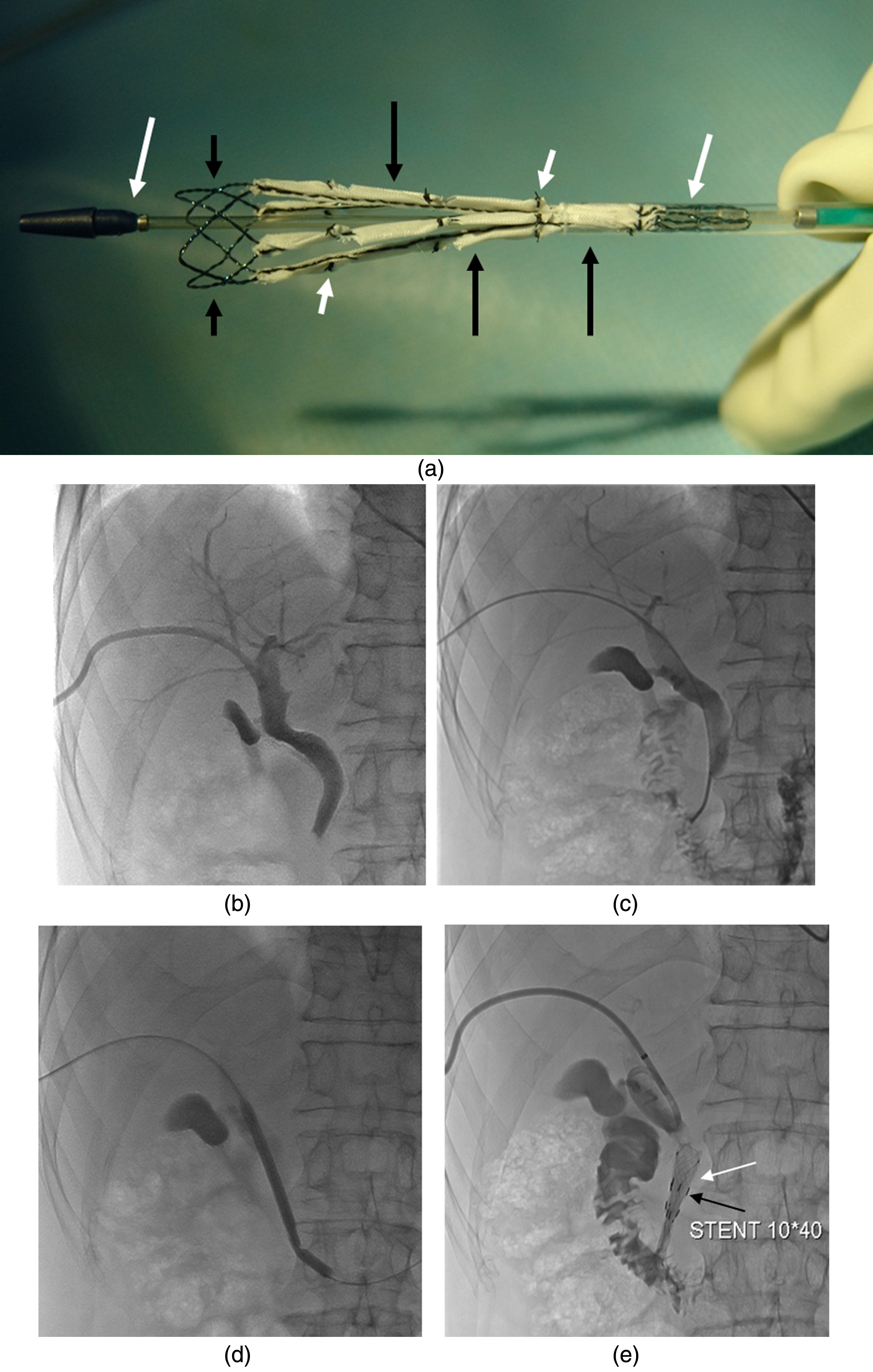
The procedure of radioactive 125I particle biliary stent and radioactive particle stent implantation. Fig. 1a The long white arrows refer to the stent conveyer, the short black arrows refer to stent (made of nickel titanium alloy), the long black arrows indicate the pouch (made of polytetrafluoroethylene) for loading particle, the short arrows refer to ligature, which is used to tie the pouch. Fig. 1b Percutaneous transhepatic cholangiography (PTC) shows lower biliary obstruction. Fig. 1c The catheter enters the duodenum through the obstructed section. Fig. 1d Balloon dilates narrow segment. Fig. 1e The 125I particles stent is implanted into bile duct stenosis segment, the white arrow refers to the stent, the black arrow to 125I particle.
After the surgery, both groups shall be fasting for solids and liquids, receive medicines for preventing infection, protecting the liver and to control bleeding, somatostatin and other supportive treatments. Efforts shall be made to observe vital signs, abdominal signs and body temperature, reexamine blood, urine amylase and liver function, and regulate water-electrolyte balance. The cases can take liquid diet in case of normal urine amylase and no abdominal sign. The ordinary stent group was given symptomatic and supportive treatment, without anti-tumor treatment.
Therapeutic effect evaluation
(1) postsurgical liver function of the patients, serum total bilirubin, direct bilirubin, alanine aminotransferase and alkaline phosphatase were recorded one month after the surgery and compared with pre-surgical results. (2) Their complications were observed. (3) Leukocyte count and serum IgG index before the surgery and one month after the surgery were recorded and compared. (4) The follow-up visit recorded the stent patency period from the stent implantation to the stent obstruction or the patient death. (5) Measurements of the maximum and minimum tumor size were made before and after (3 months later) ordinary and particle stent implantation with contrasted CT images. (6) The follow-up visit also recorded the patient survival period from the stent implantation to the patient death. The follow-up visit was conducted by telephone or through outpatient review, started at 2d after the surgery and ended on Dec 31, 2016, with the average duration of 12.3 months. (7) Based on the response evaluation criteria in solid tumors (RECIST 1.1), the therapeutic effects were divided into CR (complete response), PR (partial response), SD (stable disease) and PD (progressive disease). Remission rate (RR) = (CR+PR)/total patients in each group; disease control rate (DCR) = (CR+PR+SD)/total patients in each group; disease progression rate (DPR) = PD%.
Statistical processing
The data was processed by using SPSS 17.0 statistical software (SPSS for Windows; Chicago, IL, USA). The measurement data was represented with (
Results
Grouping and stent implantation
Among 78 patients, 30 were willing to abandon palliative treatment due to variety of reasons such as economic condition, medical insurance, risk, effect, determination, etc. And the rest were randomly and equally divided into two groups. All of the 48 patients were successfully implanted with ordinary metal stents and 125I particle stents, with the success rate of 100%. However, five patients from control group and eleven from test group were lost to follow-up. As a result, the ultimate grouping was following: (1)control group: 19 cases in total, including 12 males and 7 females aged between 48 to 86 years old, with an average age of 68 years. They included 11 cases of pancreatic head carcinoma, 5 cases of bile duct carcinoma, 2 cases of gallbladder carcinoma and 1 case of ampullary carcinoma. (2)test group: 13 cases in total, including 8 males and 5 females aged between 49 to 88 years old, with an average age of 66 years. They included 7 cases of pancreatic head carcinoma, 4 cases of gallbladder carcinoma and 2 cases of bile duct carcinoma.
The two groups had no statistically significant difference in patient age, gender and type of lesion (P > 0.05), and thus were comparable (Table 1). There were no significant complications, such as massive hemorrhage, acute liver damage, falling and loss of 125I particle or death during peri-operative period.
Baseline demographic and disease characteristics of patients
Baseline demographic and disease characteristics of patients
CHA = cholangiocarcinoma, GA = gallbladder carcinoma, AA = ampulla carcinoma, PHA = pancreatic head carcinoma.
In comparison between the two groups, serum total bilirubin, direct bilirubin, alanine aminotransferase, alkaline phosphatase, leukocyte count and IgG index one month after the surgery were significantly alleviated compared to pre-operative levels (Table 2). The maximum and minimum tumor diameters three months after the surgery showed obvious differences from pre-surgical levels (Table 3). The control group showed significant increase in tumor size from before the surgery (P < 0.05), whereas test group showed remarkable decrease in tumor size from before the surgery (P < 0.05); the two groups showed no statistically significant difference in tumor size before the treatment (P < 0.05) but significant difference after the treatment (P < 0.05). In terms of the median time of stent patency and patients’ survival, there were significant differences (each P < 0.05) between control and test groups (3.9 months vs. 8.1 months, 139 days vs. 298 days, respectively).
Laboratory values pre- and post-operation of stent implantation (
±s)
Laboratory values pre- and post-operation of stent implantation (
Changes of tumor size pre- and post-operation of stent implantation (
To the expiration date of follow-up, the RR, DCR, PD% in control group were 0, 15.8%, 84.2%, respectively, but those in test group were correspondingly 53.9%, 84.6% and 15.4%, showing a significant difference (χ2 = 17.5, P < 0.05) between the two groups (Table 4). In terms to drainage patency time (χ2 = 10.21, P < 0.05) and patient survival rate (χ2 = 10.04, P < 0.05), the comparisons showed significantly different by the line graphs (Fig. 2a, 2b).

Kaplan-meier stent patency time and overall survival time. Fig. 2a Kaplan-meier stent patency time with Control group versus Test group (OSG = ordinary stent group, PSG = particle stent group). Fig. 2b Kaplan-meier overall survival time with Control group versus Test group (OSG = ordinary stent group, PSG = particle stent group, CSF = cumulative survival function).
Comparison of evaluation results by RECIST 1.1
Note: χ2 = 17.5, P < 0.05; RECIST = response evaluation criteria in solid tumors.
In control group, 5 of the 19 cases suffered short-term complications, with the incidence of 26.31%, including 2 cases of biliary hemorrhage, 1 case of mild pancreatitis and 2 cases of severe pain. In test group, 3 of the 13 cases suffered short-term complications, with the incidence of 23.08%, including 1 case of hemorrhage, 1 case of pancreatitis and 1 case of pain. All of the cases of biliary hemorrhage featured puncture channel bleeding; after the puncture channel bleeding was blocked with gelatin sponge, the cases were observed to show stable vital signs. The cases of pancreatitis and pain got better after expectant treatments. There were no serious or lethal complication and surgery-related death. The two groups showed no statistical difference for complications (Table 5, Fisher’s exact probability test, p > 0.05).
Complications after ordinary and particle stent implantation
Complications after ordinary and particle stent implantation
The 125I particles, as a type of efficient low-energy radions, have been used in the treatment of liver cancer, brain cancer, rectal cancer and other tumors, and proven to effectively inhibit the proliferation of tumors in practice [13, 21–23]. Under this inspiration, some scholars [12–14] treated malignant biliary tract obstruction through stent implantation combined with percutaneous puncture implantation of 192Ir, 125I and other radioactive isotopic particles by relieving obstruction with stent and resisting the tumor with brachytherapy, showing a better efficacy in extending the patient survival period. On the basis of many literatures [24–26], the brachytherapy for malignant obstructive jaundice through the intraluminal implantation of a self-expandable metallic stent combined with 125I and other radioactive isotopic particles can help extend the stent patency period and the patient survival period. Nevertheless, the percutaneous implantation of 125I and other radioactive isotopic particles is greatly restricted by lesion locations and morphology. In fact, 125I radions are hard to be evenly distributed at lesion locations through the percutaneous implantation, which may impact the therapeutic effect [16].
Can a biliary stent and 125I particles be combined and implanted in vivo to relieve the biliary tract obstruction symptom and achieve effective internal radiotherapy for local lesions? Currently, the efficacy and safety of 125I particle stent in treating obstructive jaundice have been preliminarily proven in a few clinical studies and animal experiments for the implantation of 125I particle stent via endoscope [17–20]. Guo et al. [17] treated 1 case of gallbladder carcinoma through the implantation of 125I particle plastic stent via endoscope; two and half years after the successful surgery, the review showed normal liver and kidney functions and no increase in tumor size. Liu et al. [18] treated 11 case of pancreatic head carcinoma through the implantation of 125I particle stent via endoscope; the results showed a median survival period of 150 days, and 8 cases with stable tumor burden (72.7%) and 3 cases with worsening conditions (27.3%) in the 2nd month after the surgery. According to our preliminary findings, the 125I particle stent group showed a median survival period of 298 days, which not only is significantly longer than that of the ordinary metal stent group (139 days), but also superior to the 99–175 days reported in literatures [27, 28]. The reason for the extension of the survival period may be that the implantation of radioactive particles stent inhibits the tumor growth, extends the stent patency period, and fully drains the obstructed bile, so as to improve the patients’ liver function and overall conditions, delay the progress of the disease, and extend the survival period.
The 125I carrying quantity is decided based on tumor size and relevant recommendations through the treatment planning system. In this study, the single activity of radioactive particles ranges between 0.5 and 0.7 mCi, and the radiological dose is controlled between 40 and 50 Gy, which conforms to the requirements of effective brachytherapy for adenocarcinoma, and is proven to be safe in some animal experiments and clinical trials [20]. Some literature [29, 30] reported that long-time, low-dose radiotherapy with radioactive particles can cause reduction in leukocyte count and relevant immune globulins. However, in this study, the particle stent group showed no significant difference in leukocyte count and IgG test results before the surgery and in 1 month after the surgery (P > 0.05). This may be because particles stents feature local irradiation and small dosage and have a smaller impact on tissues and organs beyond the irradiation area, and proved the safety of the particle stents again.
In this study, the ordinary stent group showed 5 short-term complications out of the 19 cases, with the incidence of 26.31%; the particle stent group showed 3 short-term complications out of the 13 cases, with the incidence of 23.08%. The complication incidence basically conformed to that reported in literatures (8% – 42) [31]. The two groups showed no statistical difference in complication incidence (p > 0.05), suggesting the implantation of particle stents will not increase the complication incidence.
The cause of stent obstruction is correlated with in-stent tumor growth, hyperplasia, biliary sludge or gallstones. According to our findings, particle stents had a median patency period of 8.1 months, which was significantly longer than that of ordinary stent (3.9 months). According to the evaluated results by RECIST 1.1, RR and DCR in test group were significantly better than those in contrast group (Table 4). We believe that particle stents’ longer patency period is attributed to the short-distance irradiation effect of radioactive particles carried by the stents. Brachytherapy with 125I can inhibit or delay tumor growth and hyperplasia, so as to extend the stent patency period.
The 125I particle stents adopted in this study were 8 mm in diameter, and can pass through 9.0F sheath and can be released via endoscopic or percutaneous transhepatic puncture. In addition, the stent structure can help firmly fix radioactive particles on the stent wall, and prevent them from being displaced and falling off. Compared with the stent implantation combined with percutaneous puncture implantation of radioactive isotopic particles, particle stents integrate particles and stents, which guarantees the efficacy and helps reduce surgical frequency and surgical risks although particle stents were a little more expensive than conventional stents [32], which may be the main disadvantage, an impact on patients’ will for further treatment. In most of cases, it’s not a big problem for patients with medical insurance. In addition, the particle stents adopted in this study were metal stents, which were different from plastic stents via endoscope; the latter has the disadvantages of shorter stent patency period and easy displacement [33]. Compared with plastic stents, metal stents have a larger diameter, which therefore helps greatly extend the stent patency period [5, 35]. This study showed a success rate of 100% for the stent implantation technology. The follow-up visit recorded no stent or particle displacement or falling off, and particle stent design and release-related complication, such as bile duct perforation and bile duct bleeding, indicating the easy operability, feasibility and safety of particle stents. In short, the integrated 125I seeds stents denoted a promisingly clinical value in the conservative therapy of malignant lower biliary tract obstruction though it’s a bit expensive.
In conclusion, the results for preliminary clinical application showed that the percutaneous puncture implantation of 125I particle stent in the treatment of malignant low biliary tract obstruction is safe and effective. However due to the small sample size in this study, particularly for the particle stent group, we could not make a conclusion for differences in the efficacy of this type of stents for different pathological tumors. Therefore, further large-scale, multicenter and long-term studies shall be conducted to confirm the clinical efficacy of 125I particle stents.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (No. 81101043), 333 High-level Talents Training Project of Jiangsu (No. 2016III-0603), Sci.&Tech. Achievements and Suitable Technology Extension Project in Wuxi (No.T201722), and Youth Talents Program of Science-education Rejuvenating Healthy in Jiangsu Provincial Commission of Health and Family Planning (No. QNRC 2016181).