
Abstract
BACKGROUND:
The Accreditation Council for Lung Cancer CT Screening of Japan established guidelines for the certification of Radiological Technologists in 2009.
OBJECTIVE:
To analyze the trends in examination pass rates of the Radiological Technologists and discuss the reasons.
METHODS:
The cohort comprised 1593 Radiological Technologists (as examinees) based on 10-year of data (with a total of 17 examination runs). First, the examinees’ written test results were analyzed. Second, an abnormal finding detection test was conducted using >100 client PCs connected to a dedicated server containing low-dose lung cancer CT screening images of 60 cases. The passing scores were correct answer rate >60% and sensitivity (TP) of >90%, respectively.
RESULTS:
Overall, 1243 examinees passed with an overall rate of 78%. The average pass rate for the written test was 91%, whereas that for the abnormal findings detection test was 85%. There was a moderate correlation between the test pass rate and average years of clinical experience of the examinees for the abnormal findings detection test (R = 0.558), whereas no such correlation existed for the written test (R = 0.105).
CONCLUSIONS:
In order for accredited Radiological Technologists to serve as primary screeners of low-dose computed tomography, it is important to revise the educational system according to current standard practices.
Introduction
Low-dose computed tomography (LDCT) for early detection of lung cancer was first reported in 1996 [1]. The results of a 2006 study reported that the 10-year survival rate of stage 1 lung cancer, as identified by LDCT, was approximately 90% [2]. Lung cancer screening by low dose CT is more effective than that by conventional X-ray radiography in terms of lung cancer detection rate, miniaturization of the tumor diameter of the found lung cancer, and resection rate [3–6]. A randomized controlled trial conducted by National Lung Screening Trial in the National Cancer Institute in 2011 revealed that a lung CT screening reported approximately 20% mortality reduction effect to chest radiograph [7]. Physicians and Radiological Technologists require extensive training and experience for the accurate screening of lung cancer by LDCT.
In Japan, a meeting of six academic committee members was held in March 2007 to establish certification guidelines for screening of lung cancer by LDCT. In April 2009, the Accreditation Council for Lung Cancer CT Screening was established to accredit doctors and Radiological Technologists. In addition, to ensure the accuracy and consistency of CT examinations, the guidelines suggest that the first reader (usually a physician), as a member of team in a double reading system, should be a Radiological Technologist. And then, the Accreditation Council for Lung Cancer CT Screening approved 1243 Radiological Technologists, “license in low-dose lung cancer CT screening” in approximately 10 years based on the test results (Fig. 1) [8]. The aim of this study was to assess changes in the certification rates of Radiological Technologists over a 10 year period for screening of lung cancer by LDCT to guide future educational requirements.
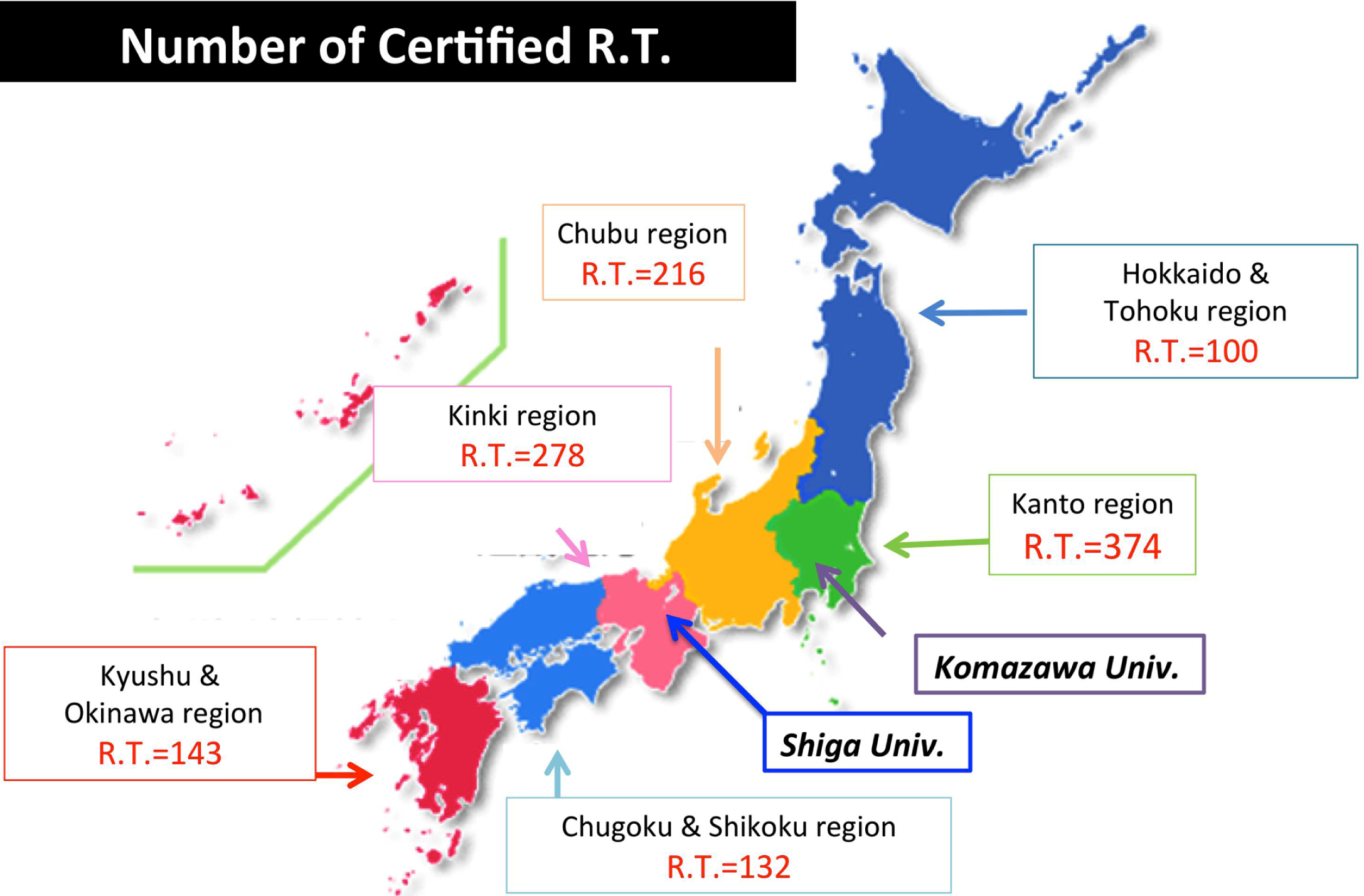
Prefectural distribution of Radiological Technologists certified for screening of lung cancer by LDCT in Japan. Komazawa University (purple frame) and Shiga University of Medicine (blue frame) were used as test facilities.
Examination sites
Komazawa University (1-23-1 Komazawa, Setagaya-ku, Tokyo, Japan) and Shiga University of Medicine (1-1-1 Banba Hikone, Shiga, Japan) were used as testing venues for certification of radiologists for screening of lung cancer by LDCT. The following three items were set as conditions for facility selection: (1) accommodations for more than 100 examinees, (ii) availability of personal computers (PCs) to conduct the examinations, and (iii) a central location in the southern or northern half of Japan with adequate traffic access.
Study population and qualifications for examination
The examination results of 1593 examinees that based on 10 years of data (number of exam runs: a total of 17 times) conducted by the certification committee for screening of lung cancer by LDCT were assessed. The average duration of work experience of the examinees was 12.7±7.11 (range, 2–38) years. The basic requirements for Radiological Technologists to perform the examination were licensure and at least 2 years of clinical experience as a Radiological Technologist.
Examination method and system
The certification exam was conducted twice per year, but at different venues. The certification test comprised two sections: a written test (25 questions, 60 min) (Table 1) and an abnormal finding detection test (60 cases, 120 min) (Fig. 2). The focus of the written test was the knowledge of safety, dose management, and image quality of a CT system. The abnormal findings detection test included normal cases, and then all examinees read the same cases. In the preliminary guidelines established for this study, the detection point of abnormal findings was determined as “a nodule with a diameter of ≥5 mm thought to be necessary for a detailed examination.” In the abnormal finding detection test, one server system was accessed by more than 100 PCs of the examinees. For the examination, a CT image viewer was installed on all PCs in advance. The image displayed by the viewer can be altered by scrolling the mouse, and answers were recorded by marking (clicking) the area judged as an abnormal finding (Fig. 3). Then, by clicking the “Next patient” tab for each case, the image of the next case was automatically loaded. It was possible to return to any case for modification within the examination time. After completion of the detection test, answers were automatically collected, and the results calculated.

The examinees were tested on their ability to detect lung nodules suspected as lung cancer on CT images tested within a specified time under controlled conditions. First, the abnormal findings detection test was conducted with 100 client systems connected to one server system. Second, suspicious lung nodules were detected by the examinee. Lastly, counting and analysis were performed immediately after the test was completed.

CT image viewer for the abnormal finding detection test imitates the operation screen of the existing CT apparatus and has excellent operability. A window adjustment function was installed to arbitrarily adjust the image.
Standard questions of written test
The acceptance or rejection of the certification test was based on the sensitivity and Az value of the written test and the results of the abnormal finding detection test. For certification, a score of >60% is needed for the written examination, a detection sensitivity of “true positive” (TP) must be >0.90 for the abnormal finding detection test, and an Az value in the area under the receiver operating characteristic (ROC) curve of >0.90 for the abnormal finding detection test.
Statistical analysis
Regression analysis using the ordinary least squares method was performed to assess the passing rate of the written and abnormal finding detection tests against the average number of years of experience. The statistical significance of the TP value and average number of false positives (FPs) against the written test and abnormal finding detection test was determined using Welch’s t-test. A two-sided probability (p) value of <0.05 was considered statistically significant. All data were analyzed using the Tokei-Kaiseki version 2.0 and Tahenryo-Kaiseki version 2.0 for Mac software packages (Esumi Co., Ltd., Tokyo, Japan).
Results
In the 10 years (total number of trials: 17), among the 1243 examinees, the passing rate was 78%. In the tests, writing tests and abnormal findings detection tests were conducted, and the passing rates were 91% and 85%, respectively. The correlations between the average number of years of experience and the passing rates of the written and abnormal finding detection tests are shown in Fig. 4 (left and right, respectively). The results of the regression analysis for the written and abnormal detection tests were as follows: slope value = –0.004/0.039; intercept = 0.965/0.355, and correlation coefficient (R) = 0.105 (p = 0.71)/0.558 (p = 0.03), respectively.

Showing the results of the evaluated correlation between the average number of years of experience and pass rates in the written test (Left) and the abnormal finding detection test (Right).
As shown in Fig. 5, the average scores of the written test, as classified into four groups according to the years of experience of the examinees were 77.1 for 2–5 ears, 76.4 for 6–10 years, 74.2 for 11–20 years, and 73.0 for >20 years. There were significant differences in the scores between combinations of groups other than 2–5 vs. 6–10 years and 11–20 vs. >20 years (p < 0.01).
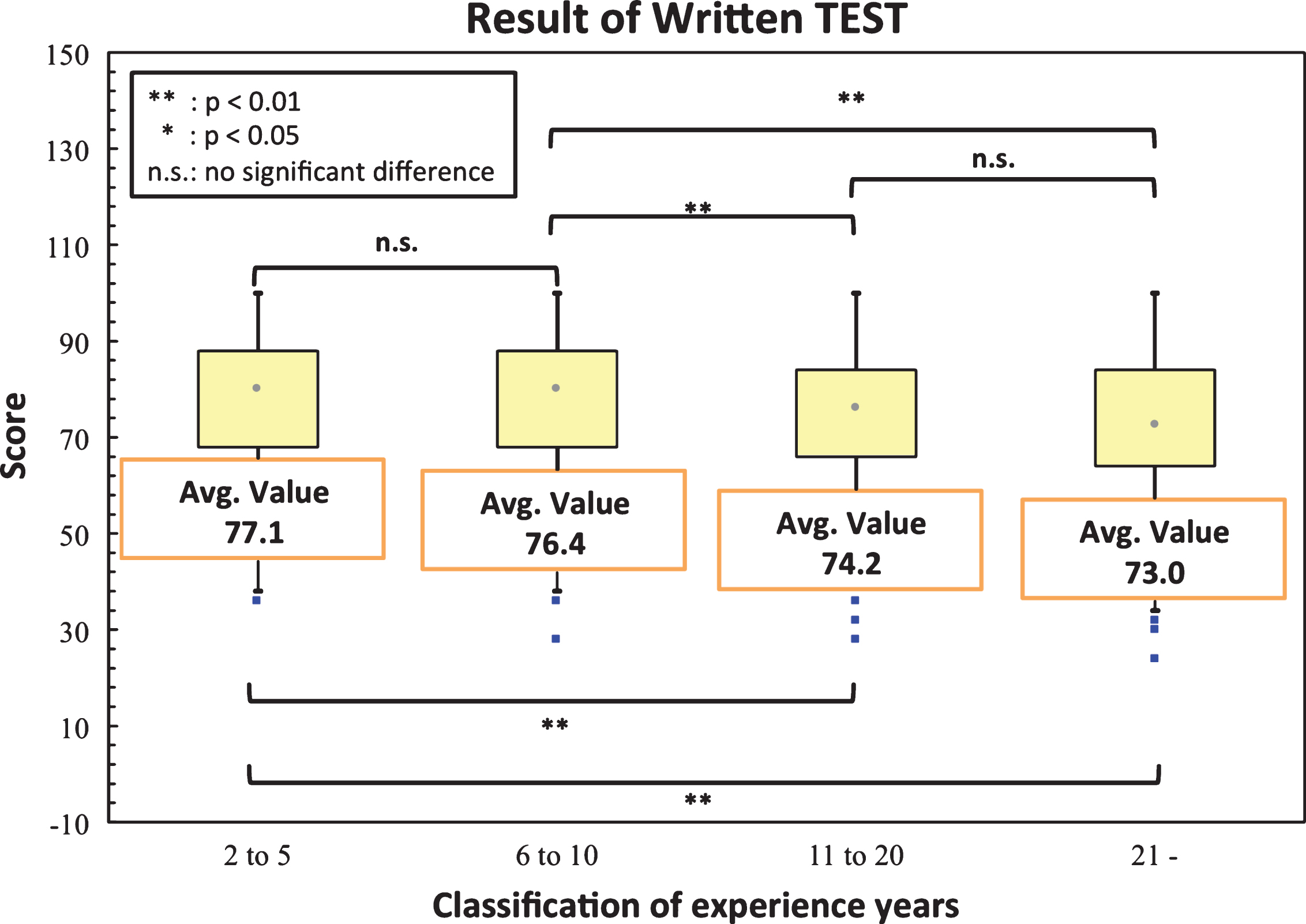
Results of written test were classified according to the years of experience: 2–5, 6–10, 11–20, and ≥21 years, and the scores were evaluated.
As shown in Fig. 6, as in Fig. 5, the average TP values of the abnormal finding detection test according to years of experience were 0.922 for 2–5 years, 0.930 for 6–10 years, 0.937 for 11–20 years, and 0.937 for >20 years. There were significant differences in the average TP values as comparing 2–5 vs. 11–20 years, 2–5 vs. >20 years, and 6–10 vs. 11–20 years (p < 0.01, 0.01, and 0.05, respectively).
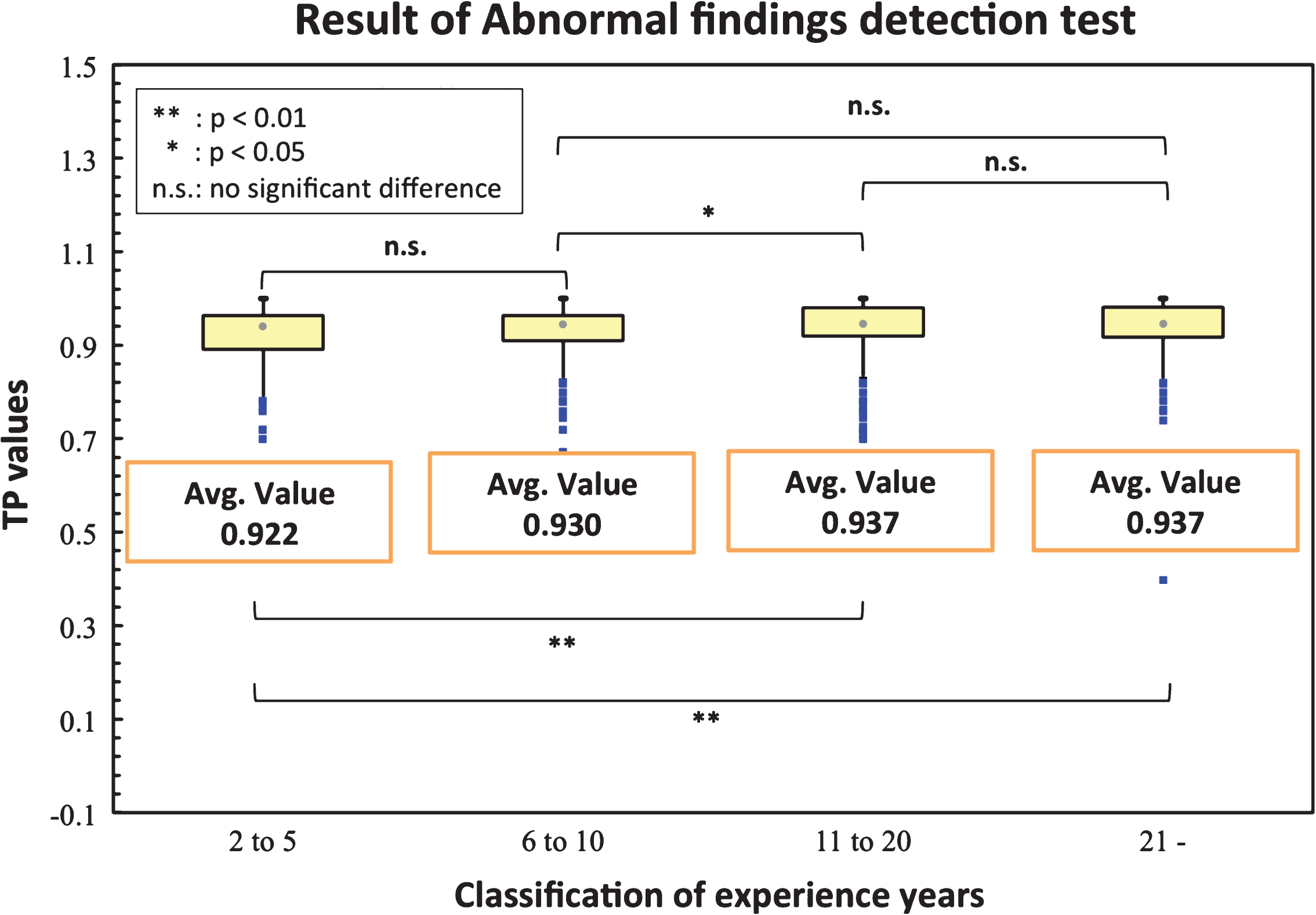
Results of the abnormal findings detection test were classified according to the years of experience and the accuracy of the TP values was evaluated.
As shown in Fig. 7, the average number of FP according to years of experience were 0.465 for 2–5 years, 0.430 for 6–10 years, 0.484 for 11–20 years, and 0.365 for >20 years. The average number of FPs of the group with >20 years of experience was significantly lower than that of the other groups (p < 0.05).
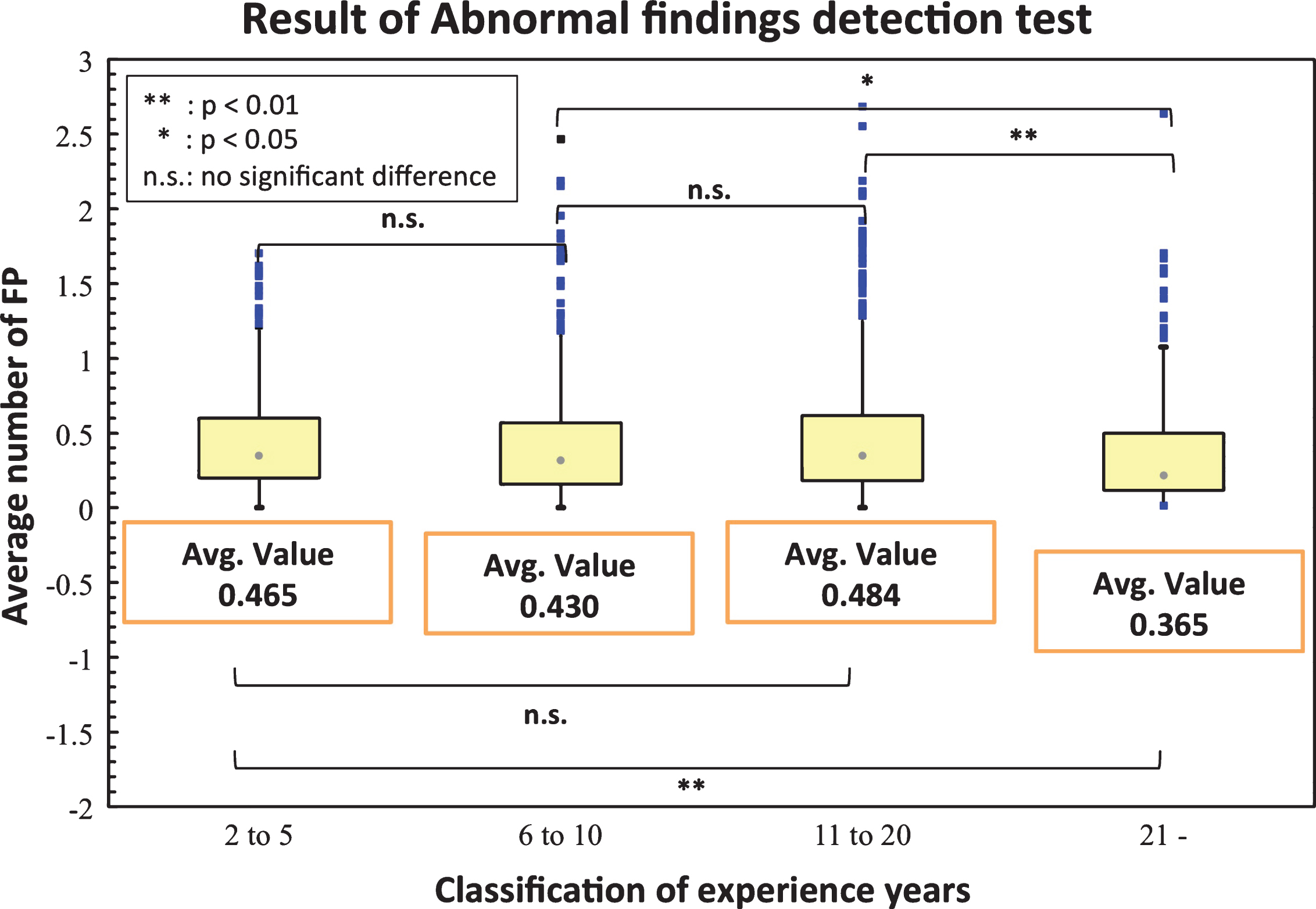
Results of the abnormal finding detection test were classified according to the years of experience, and the accuracy of the average number of FPs was evaluated.
This study examined data collected by the Accreditation Council for Lung Cancer CT Screening over a 10 year period. The certification exam was designed to achieve the philosophy of the Accreditation Council for Lung Cancer CT Screening “to guarantee lung cancer CT screening at a certain accuracy or higher at anytime and anywhere in Japan” [9]. In this study, the scores of the written test, TP values, and average number of FPs of the examinees were compared in regard to the years of experience. There was a weak correlation between the years of experience and the passing rate of the written exam (Fig. 4, left). The website of the Accreditation Council for Lung Cancer CT Screening [10] contains previous test questions, without answers. By using these resources, it is inferred that the examinees have obtained a learning effect that exceeds the acceptance level by 10 points or more, regardless of the number of years of experience. In addition, the aggregated results were classified into four groups based on years of experience (2–5, 6–10, 11–20, and >20 years). The written test scores decreased significantly with an increase in years of experience (Fig. 5), suggesting a decrease in “academic knowledge” with an increase in experience. In other words, after obtaining certification, basic academic knowledge, such as engineering knowledge, image quality, and dose evaluation, was correlated with a lower average score.
In the abnormal finding detection test, the passing rate improved with experience (Fig. 4, right). As shown in Figs. 6 and 7, the TP values and average number of FPs significantly improved with experience. The work of the Radiological Technologist has changed significantly because of shorter imaging times with the use of multiple rows of CT detectors and higher picture quality because of the development of the sequential approximation application reconstruction method. In single-slice CT, once a lesion is recognized on a thick-slice image, thin-slice images are obtained again. Also, the use of Picture Archiving and Communications systems is inadequate, and the necessary range is outputted by “film.” These works have improved the reading ability of Radiological Technologists. In the era of 16-row multi-detector CT scans, a lesion recognized on a thick-slice image was reconstructed from a thin-slice image from the same raw data. However, since the era of 64-row detectors, it has become standard practice to obtain images from thin slices; thus, the role of image confirmation by the Radiological Technologist has markedly decreased along with the ability to detect abnormal findings. The Accreditation Council for Lung Cancer needs to pay close attention to these data trends and issues. The responsibilities of certified Radiological Technologists will continue to change with advancements in medical technology.
To maintain the standards of certified Radiological Technologists, it is necessary to eliminate biases in knowledge by assessing the balance between the foundation and clinical knowledge and to review the educational method. For example, in order to detect abnormal findings, some facilities have adopted computer-aided detection (CAD) technology. In the future, further improvements in accuracy can be expected with the development of diagnostic support software with artificial intelligence or deep learning. In particular, deep learning neural networks trained using previously retrieved low-dose CT image data have been recently developed and applied in lung nodule detection and classification [11, 12]. We believe that training and practice with CAD is indispensable to maintain the standards of certified Radiological Technologists.
Conclusions
The results of this study showed that the average score of the written test tended to be higher with less experience. The TP values and average number of FPs of the abnormal finding detection test improved with the number of years of experience. In order for accredited Radiological Technologists to accurately detect abnormal findings, it is important to revise the educational system according to current standard practices. In the future, the combined use of CAD is expected in clinical applications.