
Abstract
BACKGROUND:
During the MRI examination, pediatric patients sleep under the sedation so that the image artifacts caused by the patient motion could be minimized. However, the sedative injection at the buttocks might cause a difficulty in the diagnosis of the buttock diseases using the MRI manifestations.
OBJECTIVE:
This study aims to explore the imaging characteristics of MR for the pediatric patients with the sedative injected at the buttocks in order to correctly diagnose the diseases.
METHODS:
MR imaging data of 64 pediatric patients injected with the sedative at the buttocks were retrospectively collected, including 8 cases of buttock disease. The imaging manifestations were analyzed and compared.
RESULTS:
Out of 64 patients, 8 were diagnosed as the buttock diseases. MR imaging manifestations of the sedatives injected at the buttocks were the locally patchy and streaky long T1 and long T2 signals and were different from what were shown for the normal tissues and diseases.
CONCLUSION:
The sedative injected at the buttocks has the MRI manifestations different from the normal tissues and diseases. Correctly understanding the MRI manifestations for the pediatric patients with the injection of sedative at the buttocks would reduce the chances of the misdiagnosis on the diseases.
Introduction
Magnetic resonance imaging (MRI) is a noninvasive medical imaging technology, which is widely used in pediatric patients without exposing the body to radiation [1, 2]. The most pediatric patients, especially under 4-years-old, can’t complete the simulation with fear induced by moving themselves into a small aperture and hearing a high decibel noise [3, 4]. Therefore, the pediatric patients are typically scanned in a sleep status under sedation and monitored of the vital signs including respiration and heart rate [5, 6]. For pediatric patients, the safe and most frequently used method of the sedative administration is the buttocks intramuscular injection [7–9]. However, the buttock diseases could be difficult to be differentiated from the sedative injection by the MRI imaging findings when the sedative is injected into the same location of the lesions. This image demonstrating overlap of the injected sedative and lesions in MRI could lead to a medical event such as misdiagnosis.
In order to correctly diagnose different diseases in the buttock, this study was to explore the imaging characteristics of MRI for the pediatric patients with the sedative injected by retrospectively analyzing the MRI features of 58 cases, 6 cases of which were shown with gluteal lumps.
This study was approved by the Ethical Committee of The Fujian Medical University Union Hospital. The parents of all pediatric patients participated in this study had signed on the consent forms before the clinical procedures started.
Material and methods
Patients characteristics
The study included 64 pediatric patients in the age ranging from 3 days to 5 years old and admitted to Fujian Medical University Union Hospital for diagnostic or medical procedures during 2009 – 2013. Clinical characteristics of the 64 pediatric patients were summarized in Table 1. 43 patients were male in this study. Of these patients, 58 showed no abnormal clinical manifestations, or only abdominal distention, abdominal pain, and suspected congenital urinary malformations were observed; 1 patient had the unilateral gluteal lumps; 1 felt the buttock pain. All pediatric patients underwent MRI scans on either the abdomen or the buttocks and were given sedatives on the bottom before the examination.
64 Children, clinical characteristics
64 Children, clinical characteristics
For the MRI examination, Verio 3T super-conductive MRI scanner (Siemens Magnetom, Verio, Germany) with a dedicated buttock receiver coil was used for 48 patients and a Signa 1.5 T ultra-conductive MRI scanner with a dedicated buttock receiver coil (GE Signa Infinity Twinspeed, USA) for 16 patients, respectively. The sequence used in this non-contrast study at the Siemens Magnetom Verio 3.0T was the transient spin echo (TSE). The T1-weighted parameters were 600 ms repetition time (TR), 20 ms echo time (TE), 8 echo train length (ETL), 10 ms echo spacing (ES). The T2-weighted parameters were 4000 ms TR, 104 ms TE, 108 ETL, 10 ms ES, 2 averaging. The similar sequence was used at the GE Signa Infinity Twinspeed 1.5T scanner. The T1-weighted parameters were 440 ms TR, 11 ms TE, 3 ETL, 10 ms ES, 2 number of excitation (NEX). The T2-weighted parameters were 3500 ms TR, 110 ms TE, 19 ETL, 10 ms ES, 2 NEX. All patients were scanned with 3.0 mm thickness and 256×256 matrix field of view.
Sedative and medication method
The sedative used in this study was the Phenobarbital Sodium and administrated into one side of the patient buttocks. The dosage for each application was calculated by 5.0 mg/kg based on the patient weight [10].
Injection location
Gluteus maximus, gluteus medius or gluteus minimus was selected to administrate the sedative in this study for the pediatric patients. A method called as the cross localization was adopted [11, 12]. The buttock was divided into four quadrants with the outer quadrant avoiding the inner angle as the injection area by drawing the horizontal line that started from the vertex of the anal cleft from left to right [13]. Then a vertical bisection line was drawn from the apex of the iliac crest. Furthermore, for the patients under 2 years old, the injection site was slightly moved superiorly. All injections were completed by the experienced nurses using same techniques. The manifestations of MRIs were independently reviewed by two experienced and senior radiologists. Any discrepancy of the finding from the MRI reviews was discussed further among them before the final confirmation.
Results
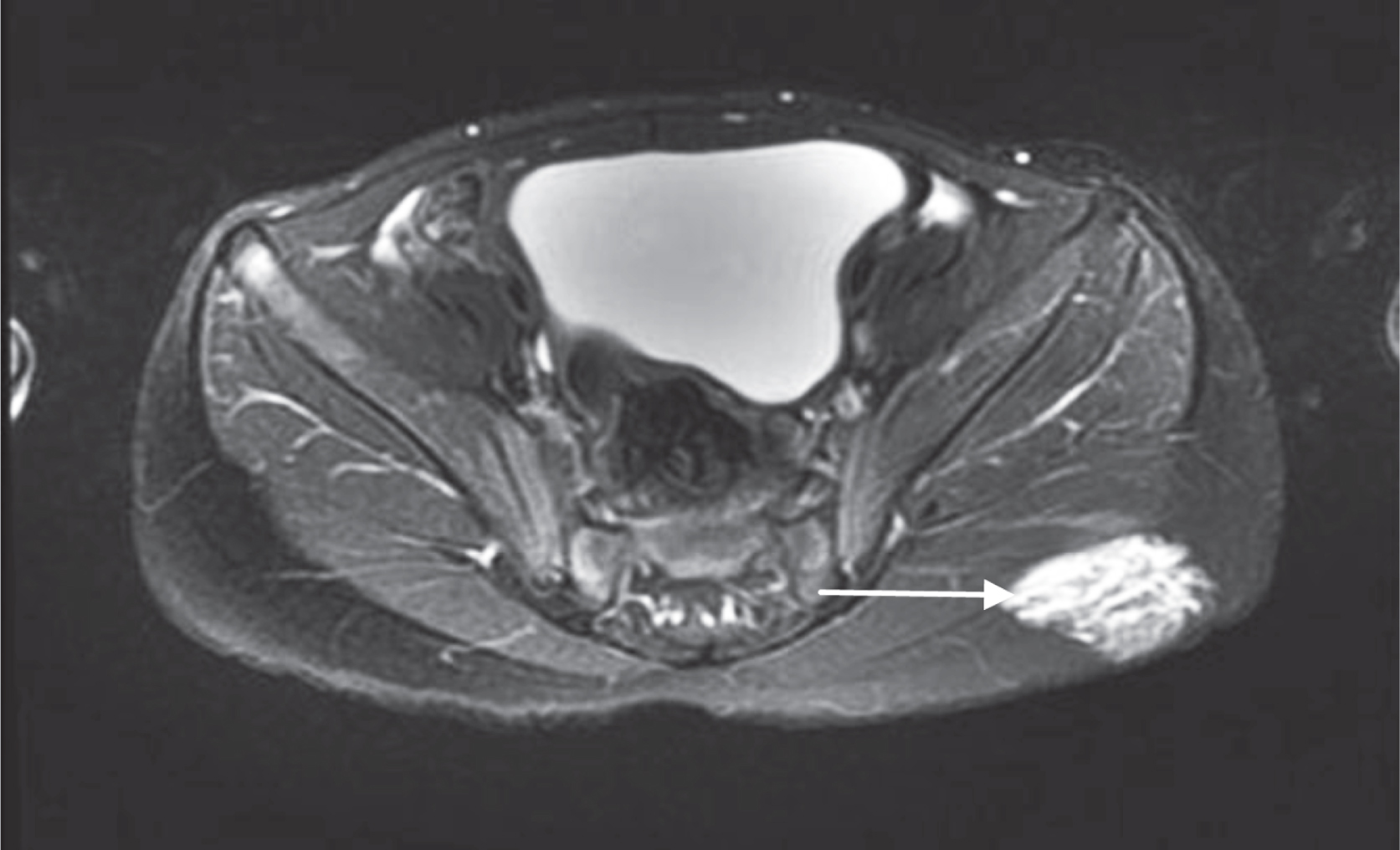
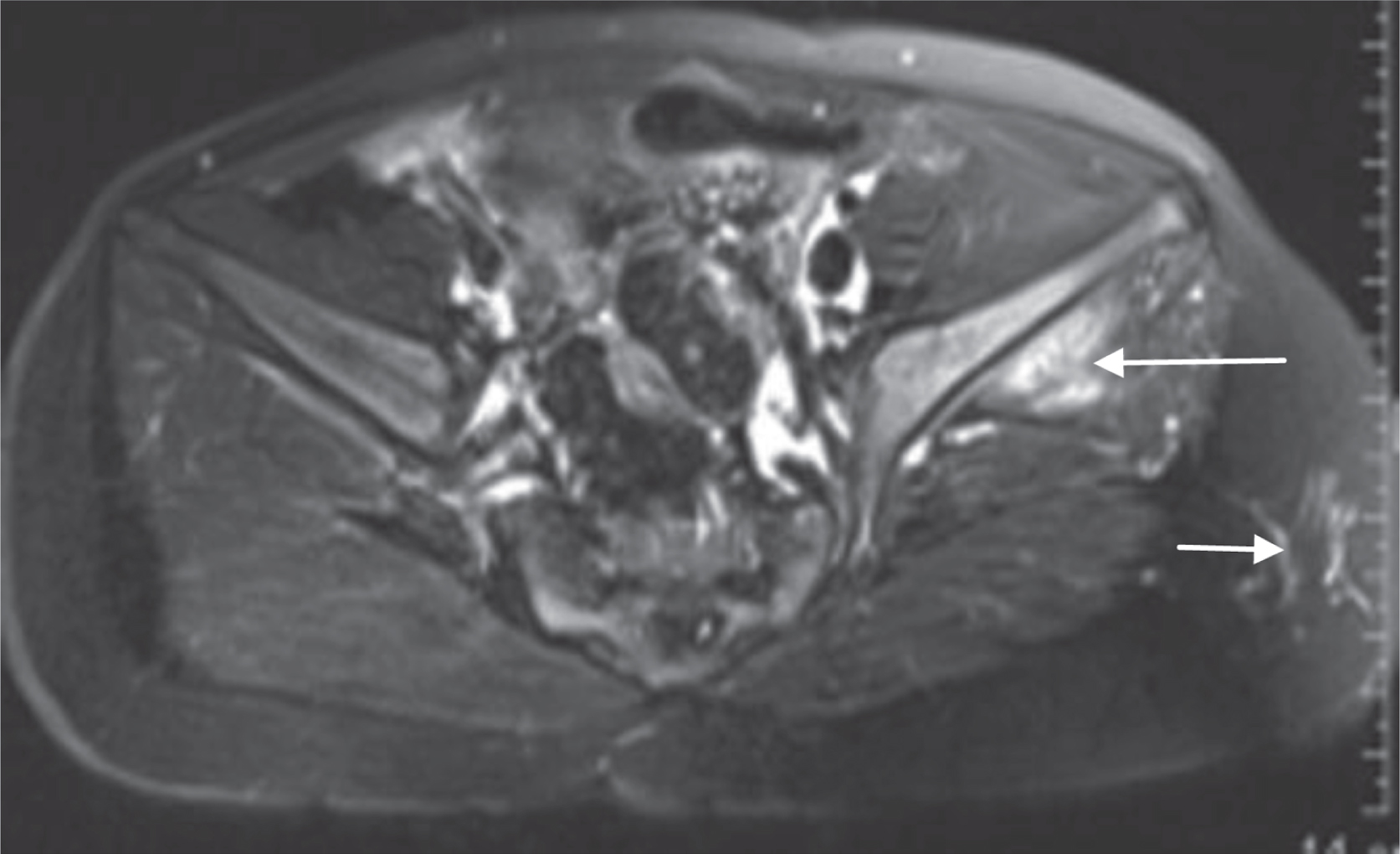
Of the 64 pediatric patients, 52 went to a deep sleep in 15–30 minutes after the injection and were completed MRI scan without a repeat. The other 12 pediatric patients woke up during the examination and had to receive a second injection. The effectiveness rate for the first-sedative injection is 81.3%. During the time of the injection, 31 of 52 patients did not resist while their ears and fingers were touched or slightly pulled. They entered a deep sleep status in 15–20 mins. As shown in Fig. 1, those patients had the T2 weighted MR image (T2WI) demonstrating some image manifestations such as streaky, patchy, homogeneous and hyperintense signal in unilateral gluteal muscular layer. 21 patients of the 52 patients fell into a deep sleep in 25–30 mins, and their T2WI showed streaky, patchy, and cotton-like, hyperintense signal in both the unilateral gluteal muscular layer and the fat layer with a size from 1.9 cm×1.4 cm to 3.0 cm×2.5 cm. For those patients, Fig. 2 demonstrated the boundary of the well-circumscribed signal. Other 12 patients were particularly the light sleepers and would resist or keep moving after the injection even the ears and fingers were touched or slightly moved. They had to be injected again in 30 minutes in order to complete the MRI scans. Their T2WI was showed in Fig. 3 and demonstrated the streaky and patchy mixed the low and high signal in unilateral gluteal fat layer measuring the size from 3.4 cm×2.6 cm to 2.3 cm×1.7 cm.

The T2-weighted axial MR image showed a hyperintense, and homogeneous signal in the gluteal muscular layer (arrow), which represented the sedative 15 minutes after injection.
The T2-weighted axial MR image showed a hyperintense, cotton-like signal in the gluteal muscular and fat layer (arrow), which represented the sedative 30 minutes after injection.

The T2-weighted axial MR image showed a streaky and patchy hyperintense mixed with hypointense, which heterogeneous signal in the subcutaneous fat layer (arrow), which represented the sedative.
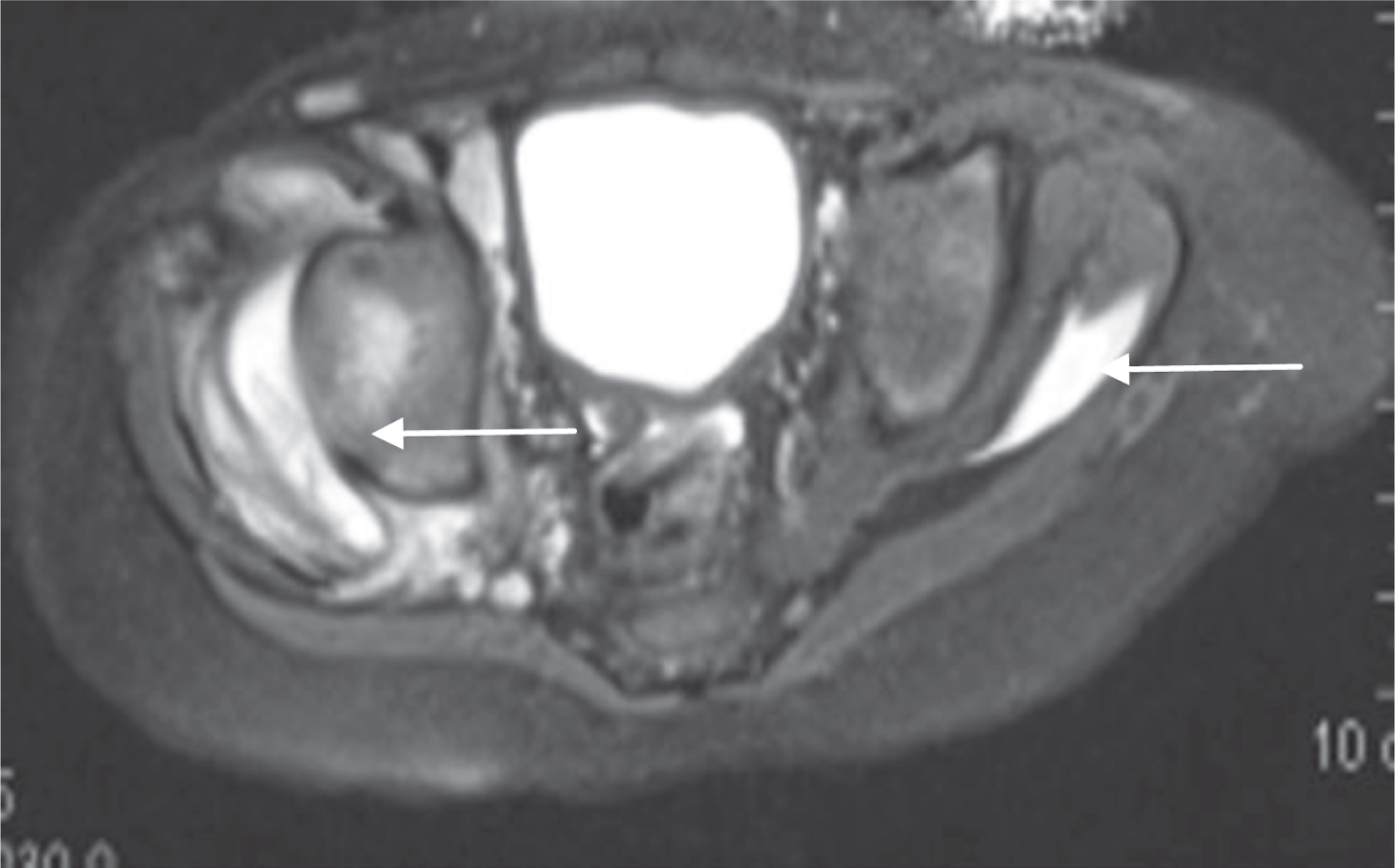
Four cases were diagnosed as the vascular anomalies including two hemangioma cases and two lymphangioma cases. In the two hemangioma cases, the punctiformed or lamellar high signal in gluteus minimus were displayed on T2WI (Fig. 4). The MR signal focusing on the left iliac bone increased but was not destruction. In the two lymphangioma cases, the multiple thin-walled cysts of various sizes and shape were easily to see in the muscular layer and the fat layer on T2WI images. The cystic fluid showed homogeneous, and hyperintense signal while the cystic wall and fibrous septa presented hypointense signal (Fig. 5). Two cases were diagnosed as plexiform neurofibromas, in which a nodular, patchy, and massive mixed signals were observed on T2WI images. The extent of the MR signal was not able to define well in the images, and the boundary was unclear. The sedative injection to the location of the disease resulted in a heterogeneous and hyperintense MRI signal from which the plexiform neurofibromas was very difficult to be determined from T2WI images due to the sedative injected (Fig. 6).
T2–weighted axial MR image showed the hemangioma was located between iliac bone and the gluteus minimus (long arrow) and the sedative was located in muscular layer (short arrow).
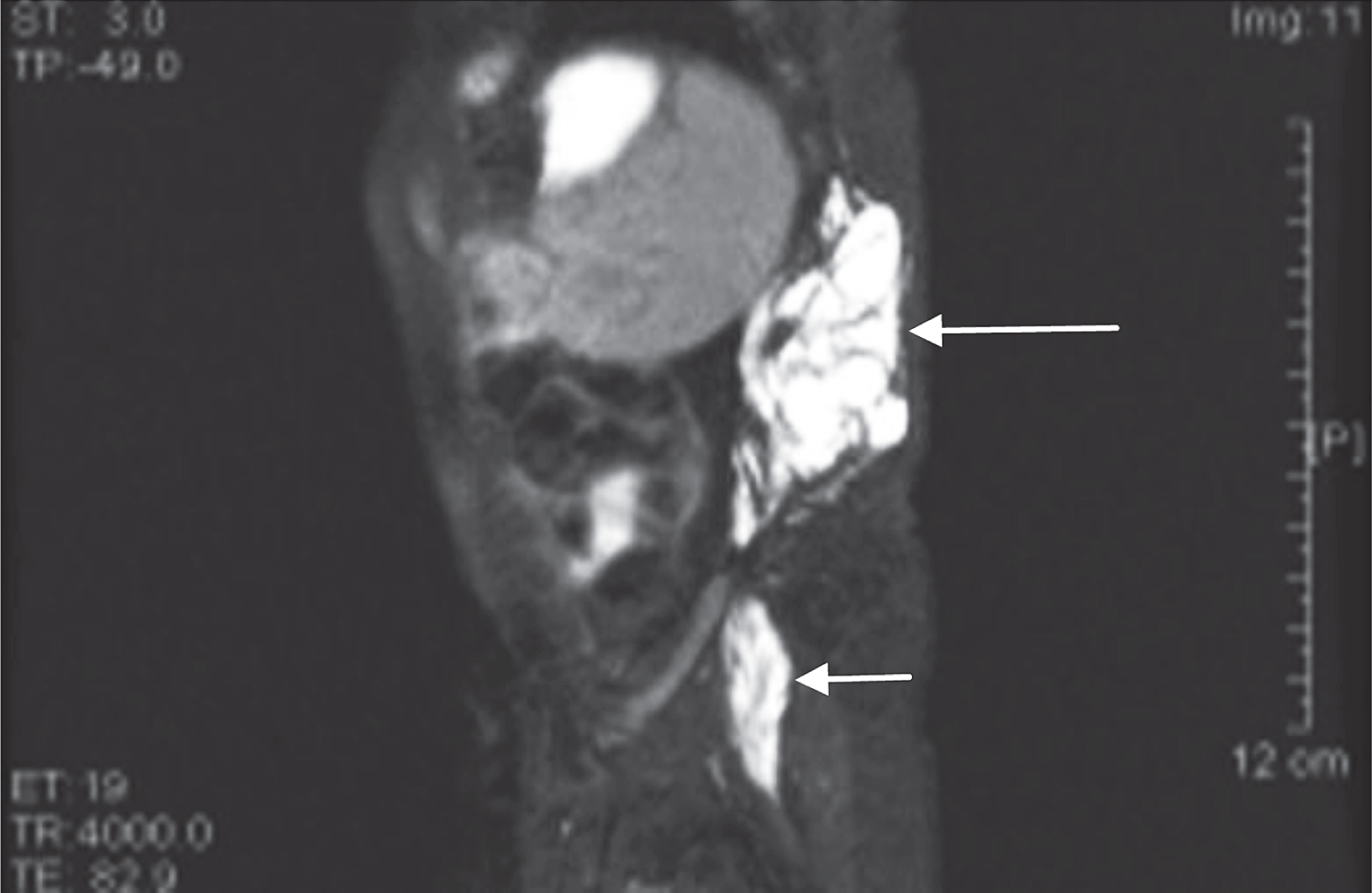
T2–weighted sagittal MRI scans showed the lymphangioma (long arrow) was located in muscular layer and fat layer of the buttock and the sedative was located in the muscular layer (short arrow).

T2–weighted coronal (a) and (b) T2-weighted axial MRI scans showed the plexiform neurofibromas was located in the muscular layer and fat layer of the buttock (long arrow). The sedative signal mixed with signal of plexiform neurofibromas (short arrow).
For two inflammation cases, the T2WI showed the cloud-like, heterogeneous, wide-scope and hyperintense signal at the surrounding soft tissue of the right hip joint (Fig. 7). The locally homogeneous hyperintense signal at the left gluteus medius was the MRI manifestations of the sedatives.
T2–weighted axial MRI scans showed the extensive inflammation in the surrounding soft tissue of right hip joint (long arrow) and the left well-circumscribed sedative (short arrow).
The sedatives can be administrated to the patient bodies by four routes including the oral administration, muscle injection, intravenous administration, and general anesthesia. The oral drug is usually the chloral hydrate, which is pungent, bitter and smelly. In clinic, a certain amount of syrup usually is added to the chloral hydrate to improve the taste. However, adding too much or too little can dissatisfy the pediatric patients because the taste buds of the patients older than 7 months have become more sensitive. In the case of oral administration failure, forcedly feeding can cause vomiting and even suffocation. Taking oral medicine again after vomiting may cause serious adverse reactions to the patients because more sedative is needed to make the patients a deep sleep after vomiting, but the dose is not easy to control. Intravenous administration and general anesthesia are less frequently used to the pediatric patients because of the side effects and less safe. Therefore, the injection at the buttock is a method most commonly used for the pediatric patients.
It was found in this study that 52 pediatric patients with the injection of sedatives in either the muscle layer of the hip or between the muscle and the fat had a good sedative effect and completed the MRI examination successfully. The other 12 patients having the injection of sedative in the buttock fat layer cried during the examination, indicating a week or poor sedative effect on the patients. The tranquilizing effect of pediatric patients was obviously related to the sedative injection depth in tissue.
In the case for the MRI simulation of the patient’s abdomen or buttocks, the hip injection of sedative was necessary to make the patients go to a deep sleep. Therefore, when scanning the abdomen or buttocks, it was also possible to scan the hip so as the sedative on the buttock tissues would be detected by MR imaging. With a standard sedating operation, a lamellar, stripe-like as well as plate-like mixture of long T1 and long T2 signal shadow should be seen in the subcutaneous fat layer, the layer between fat and muscle, and the muscular layer. Because the boundary of this shadow was clear, the sedative distribution inside the tissues was shown as lamellar, a thin layer shape. In the three dimensions view, the MR signal of the sedative injected was shaped like a cotton ball, resulting from the continuous body absorption. The shape and size of the sedative injected in the subcutaneous tissue was constantly changing. After the injection, the lamellar sedative distribution was visible in the soft tissue, and the signal was more homogeneous and hyperintense. Then, with the absorption of the drug, the signal became heterogeneous, and the internal funicular shadow became visible. The longer the time passed after the injection, the smaller and thinner the layer was, and the less the shadow demonstrated, as shown in Figs. 1 and 2. The MRI manifestations of the sedative injected changed with time.
The diseases of vascular anomalies located in the buttocks and discussed in this study included the hemangiomas and lymphangiomas. The MR imaging manifestations of the hemangiomas was an irregularly lamellar or massive signal with a clear boundary [14]. On the T1WI, the hemangioma was demonstrated by a uniform or slightly lower signal, while T2WI showed a significant high signal. The MRI signal was homogeneous and depend on the tissue composition. The MRI characteristics of sedative injection had a more clearly boundary and were more homogeneous. The lymphangioma was a congenital benign hematoma with clear boundary and irregular morphology, which was presented with heterogeneous long T1 and long T2 signal on TIWI and T2WI, but showed a lower signal in the inner fibrous septa [15]. The fibrous septa and the morphology of the lymphangioma were the main differences when compared with the MRI manifestations with the sedation injection.
The plexiform neurofibromas presented in this study can be characterized by a wide range of patchy, nodular and crumb mixed signal on T1WI and T2WI, which had the ill-defined margins and solid mass [16]. In comparison with the tumors, the sedatives appeared well-defined shapes and homogeneously in MR images.
Regarding another type of signal source, the inflammation could occur in joints, soft tissues, muscles, ligaments, and fascia. The MR imaging characteristics of the inflammation could be classified as ill-defined and patchy with long T1 and long T2 signals [17]. Differently, the signals of sedatives were relatively limited and homogeneous inside of the body and changed with time.
In summary, the sedative injection at the buttocks and the buttock diseases could be easily differentiated by the imaging manifestations when they are separated. Similar to applying MRI to diagnose many other types of diseases or lesions [18], if the sedative is injected into the pediatric disease locations, the MR imaging manifestations of the lesions could often be unclear and confusing, which results in a misdiagnosis or miss-diagnosis. Especially for the cases which do not have a clinical symptom, to control a correct injection depth is very critical for the diagnosis of the diseases. In our study, there was a case in which the nurses didn’t recognize the patients had the buttock lesions due to no clinical symptom and the sedative was injected into the disease side of the patient buttocks. To avoid injecting the sedative into the lesion area, the nurse should carefully review the patient medical history or question the parents or patient parents before injecting. Also, when the physicians diagnose each case of the pediatric patients, they should know all patient medical history and the previous medical examinations. The physicians also should pay attention to the MRI characteristics of the individual disease and the sedative inside the tissues including the signal, boundary, size, morphology, and the sedative injection location to avoid any mistake in the determination of the lesions.
Conclusion
The sedative effect is closely associated with the injection depth in the tissue for the pediatric patients. The appropriate depth is in the muscle layer. The subcutaneous adipose tissue should be avoided to be injected with a sedative. The MR imaging features of the sedatives injected at the buttocks for the pediatric patients are the locally patchy and streaky long T1 and long T2 signals at the muscular layer and fat layer. The boundary of the MR signal is clear, and its distribution inside the tissues is well-defined. The characteristic that the MRI manifestations of the sedative injected change over time and its imaging manifestations are helpful to differentiate from the disease. The existence of the lesions in the buttocks should not be excluded if the MR signals are ill-defined and heterogeneous.
Footnotes
Acknowledgments
The study was supported by The Science and Technology Department of Fujian Province (NO.2016Y0044) and Fujian Provincial Health and Family Planning Commission (NO. 2016-CX-19).