
Abstract
OBJECTIVE:
This study aims to evaluate the effect of dentoalveolar distraction extraction (DDE) on site preservation, and to evaluate how the technique keeps the height and width of alveolar bones to a greater extent.
METHODS:
12 beagle dogs, randomly divided into three groups (DDE group, NH group, BOG group), were used. In the dogs of three groups, the root of the left or right third mandibular premolars were respectively extracted by three methods namely, DDE, traditional extraction with natural healing, and traditional extraction with Bio-Oss bone dust implanted and guided bone regeneration (GBR). Cone-beam computed tomography (CBCT) scans and X-rays were taken immediately and three months after the tooth extraction. The height and width of the alveolar ridges were compared among different groups.
RESULTS:
Three months after tooth extraction, at the 1 mm level below the alveolar ridge crest, the amount and degree of buccal alveolar ridge width resorption in DDE group were significantly lower than that of NH and BOG group (P < 0.05). At the 2 mm and 3 mm level below the alveolar ridge crest, the amount and degree of buccal alveolar ridge width resorption in DDE group and BOG had no significant difference, and both were significant lower than that of NH group (P < 0.05). The height resorption of alveolar ridge in DDE group was significantly lower than NH and BOG groups (P < 0.05), while NH and BOG group had no statistically significant.
CONCLUSIONS:
To a greater extent, the alveolar ridge preservation through DDE could preserve the height and width of alveolar ridge crest.
Introduction
Morphologic and dimensional changes of the alveolar ridge after tooth extraction is an inevitable consequence, especially the loss of height and width [1–3]. In oral implantology, lacking of bone mass can lead to difficulties in implant placement [4]. Therefore, the maximum preserving bone mass of the alveolar ridge in tooth extraction area becomes critical to oral aesthetics and functional repair. Currently, alveolar ridge preservation techniques, include bone or bone substitute material filling, biofilm technology, immediate planting, minimally invasive extraction, etc. [1, 6], has emerged with different advantages and disadvantages, in which bone substitute material filling is most frequently used. The techniques were used to increase the bone mass by intervening the healing process of bone quality in tooth extraction, so that to preserve the shape and quality of alveolar ridge. According to the literature review, a number of scholars found alveolar ridge preservation techniques could reduce alveolar bone resorption to some extent compared with natural healing (NH). However, it could not completely prevent this process and there were few differences among alveolar ridge preservation methods on effects [7–9].
In this study, in order to discover a better way to alveolar ridge preservation, we carried out the dentoalveolar distraction extraction (DDE) based on periodontal ligament distraction osteogenesis, which was originally proposed by Liou [10]. Periodontal ligament was considered as a natural suture, teeth and alveolar bone proper were considered as bone stump, therefore alveolar distraction could accelerate osteogenesis [11]. Periodontal ligament distraction osteogenesis could promote the formation of new alveolar bones under the root of teeth to achieve the alveolar ridge preservation [12]. This study mainly evaluate the effects of DDE on alveolar ridge preservation, when compared with traditional extraction with natural healing, and traditional extraction with Bio-Oss bone dust implanted and guided bone regeneration (GBR). X-rays and cone-beam computed tomography (CBCT) scans were utilized to calculate the height and width of alveolar bone preservation.
Materials and methods
Animals
12 beagle dogs, about 12–15 months old and weighing between 7 and 10 kg, purchased from Beijing Jinmuyang Laboratorial Animal Co, Ltd, were used for this experiment. Each dog was housed in a separate cage in a shared room, which were cleaned daily. The room was set at a temperature of 20–25°C, a relative humidity of 40–70% and a light cycle of 8:00–20:00, the dogs were fed twice a day with a total amount of 280–400 g food. The research protocol of this study was approved by the local institutional committee of Beijing Friendship Hospital, Capital Medical University, and undertaken in accordance with the guidelines of institutional animal care.
The experimental dogs were randomly divided into three groups. In experimental group (DDE Group), the root of the left or right third mandibular premolars were extracted by DDE. While, in another group, the root of the left or right third mandibular premolars were extracted by traditional extraction with natural healing (NH Group). For the other four dogs, as control group two (BOG Group), the root of the left or right third mandibular premolars were extracted by traditional extraction followed by Bio-Oss bone dust implant and GBR.
Surgical protocol of the experimental group
The dogs of DDE group were inserted implants (1.4×6 mm, Zhong bang) between the roots of third mandibular premolars for two weeks. A 0.5 mm retentive groove was formed along the dental cervix of mandibular third premolars. A 0.25-mm ligature wire (Changsha Tiantian Dental Equipment Co. Ltd, China) was plunged into the retentive groove. Then, ligature, dental crown and expansion screw (Dentaurum, Newton, Pa) were connected to retention through self-curing resin (Fig. 1a). The other end of expansion screw was connected to implant anchorage via ligature, stable for two days. Within 4 weeks, the expansion screw was unscrewed 1/2 circle (0.5 mm) to increase strength every two days for each time. After stressing for 4 weeks, the teeth of DDE group were pulled out when they were mostly separated from alveolar bone (Fig. 1b). Lastly, the formation of alveolar bone in traction root could be observed by X-rays.

Dentoalveolar distraction extraction. (a) One end of the expansion screw was connected to the implant nail while the other end connected to the crown of the teeth with self-curing resin. (b) Within 4 weeks, the tooth was distracted 7 mm. Due to the limited distance between the jaws, the tooth could not be distracted further, and the tooth was pulled out.
For control group one (NH group), third mandibular premolars were pulled out with dental elevator and forceps, until natural healing. For control group two (BOG group), the third mandibular premolars were pulled out with dental elevator and forceps. Then, the teeth extraction sockets were filled with Bio-Oss bone dust (Geistlich) and covered with Bio-Gide biofilm (Geistlich), combined with GBR. Lastly, the trapezoidal incision in gums of buccal side and teeth extraction wounds were sutured to closure.
Inspection items and measurements
DDE group, NH group and BOG group were taken X-rays and CBCT immediately and three months after tooth extraction. The effects on alveolar bone site preservation in each group were observed through X-rays. CBCT linear measurements using Simplant software were as follows: (1) bone height at the buccal, middle and lingual thirds of the examined alveolus relative to the bone crest and root apex at baseline (Fig. 2a-b); and (2) bone width at different levels (at 1, 2, 3 and 6 mm) apical to the alveolar bone crest (Fig. 2c-d). Each measurement for three times, the average changes of alveolar bone height and width were calculated.
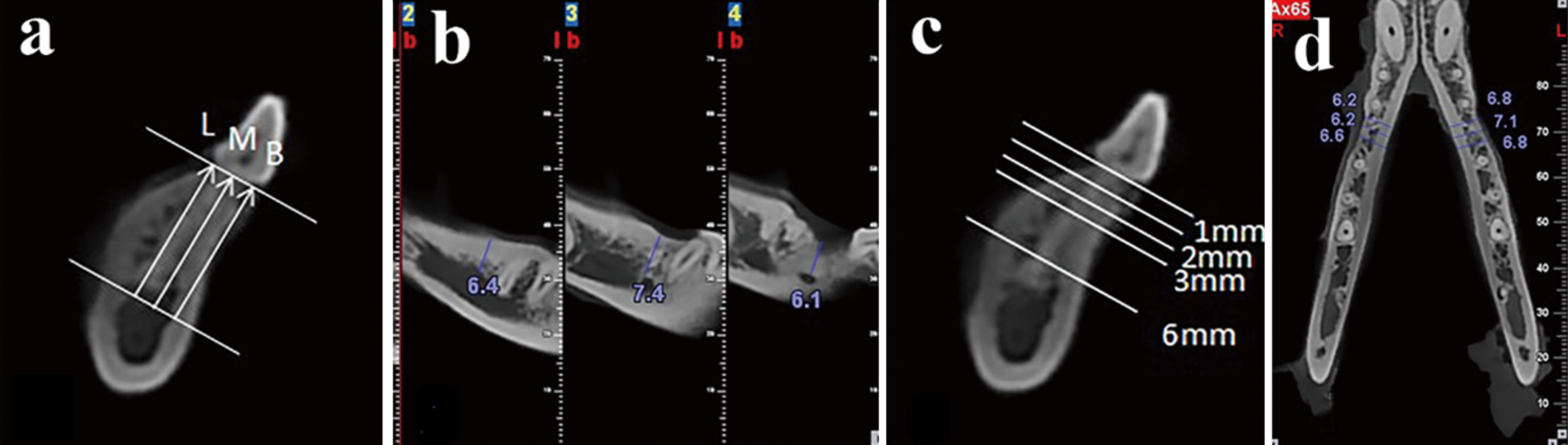
CBCT measurements for alveolar ridge height and width. (a-b) Height measurement: Distance from superior border of mental foramen to alveolar ridge crest, parallel to the long axis of teeth, divided equally as the heights of buccal, middle and lingual. (c-d) Width measurement: Width of alveolar ridge on 1 mm, 2 mm, 3 mm, and 6 mm levels below connection level of adjacent teeth enamel-cemental junction were measured respectively. Three sites on each level were measured, and the mean alveolar ridge width for each level was measured.
In this study, the one-way analysis of variance with a paired comparison method (IBM SPSS Statistics 19.0) was used to compute and compare the differences of the height and width of alveolar ridge in groups. The results were then tabulated and analyzed.
Results
The observation results
All experimental animals were kept in good condition during the experiment, and not found infection and suppuration in all operation sites, and few with mild inflammation of gingival tissues. After the teeth extraction, the X-rays of the DDE group showed there were different degrees of osteogenesis under the traction teeth, the height of the alveolar ridge in one dog was even increased (Fig. 3). Three months after tooth extraction, the appearance of alveolar ridge in the DDE group was relatively plump, and there was no significant difference in term of the appearance of the alveolar ridge in the NH group and the BOG group.

Photos and X-rays for gross observation. In the photos, alveolar ridge in edentulous space of DDE group (a) and BOG (c) group are relatively rounded, while it looked sharp in NH group (b). In the X-rays, the height of alveolar bone in DDE group (d) seemed taller than those in NH group (e) and BOG group (f).
Alveolar ridge height
Three months after extraction, the comparison of alveolar ridge height in buccal, middle and lingual sites among the three groups were shown in Table 1 and Fig. 4a. The buccal alveolar ridge height resorption of DDE group was 0.48±0.13 mm (5.8±1.5%), which was significantly lower than that of the NH group (1.58±0.36 mm, 19.2±3.2%, P < 0.01) and BOG group (1.28±0.41 mm, 16.5±4.8%, P < 0.01), while the BOG group and NH group had no significant difference (P > 0.05). The middle alveolar ridge height resorption of DDE group was 0.40±0.25 mm (4.4±2.5%), which was significantly lower than that of NH group (1.40±0.36 mm, 16.4±3.3%, P < 0.01) and BOG group (1.23±0.26 mm, 15.4±3.4%, P < 0.01), while there was no significant difference between BOG group and NH group (P > 0.05). The lingual alveolar ridge height resorption of DDE group was (0.45±0.17 mm, 5.7±1.7%) significantly lower than that of NH group (1.38±0.33 mm, 18.3±3.3%, P < 0.01) and BOG group (1.33±0.26 mm, 17.4±4.0%, P < 0.01), while there was no significant difference between BOG group and NH group (P > 0.05).
The absorbed height amount (mm) of alveolar ridge in buccal, middle and lingual sites in different groups. The numbers of DDE group on all sites were much smaller than those of NH group and BOG group
The absorbed height amount (mm) of alveolar ridge in buccal, middle and lingual sites in different groups. The numbers of DDE group on all sites were much smaller than those of NH group and BOG group

The height and width resorption in three groups. (a) Comparison of height absorbed amounts on buccal, middle and lingual sides of alveolar ridge. (b) Comparison of degrees of alveolar ridge on 1 mm, 2 mm, 3 mm and 6 mm levels under alveolar ridge crest.
Three months after extraction, the comparison of alveolar ridge width on labial-lingual side among three groups were shown in the Table 2 and Fig. 4b. The width resorption on the 4 levels of measuring sites below the alveolar ridge crest of DDE group was less than that of group BOG and NH. At the 1 mm level below the alveolar ridge crest, the amount and degree of buccal alveolar ridge width resorption in DDE group were 2.28±0.50 mm, 35.5±7.4%, respectively, which were significantly lower than that of group NH and BOG group (NH group, 4.75±0.76 mm, 69.9±12.5%; BOG group, 3.58±0.60 mm, 58.2±10.3%, respectively, all P < 0.05). At the 2 mm level below the alveolar ridge crest, the amount and degree of buccal alveolar ridge width resorption in DDE group were 2.15±0.29 mm and 30.9±3.8%, BOG group were 2.25±0.33 mm and 35.2±6.1%, there were no significant difference between the two groups (P > 0.05), while both were significant lower than that of NH group (3.10±0.25 mm and 45.7±5.6%, all P < 0.05). At the 3 mm level below alveolar ridge crest, there were no significant difference between the DDE group and BOG group in terms of the amount and degree of buccal alveolar ridge width resorption (DDE group: 1.63±0.21 mm and 22.1±2.3%; BOG group: 1.75±0.42 mm and 25.7±6.5%, P > 0.05), while both were significant lower than that of NH group (2.78±0.61 mm and 37.9±7.6%, all P < 0.05). At the 6 mm level below the alveolar ridge crest, there were also no significant difference between the DDE group and BOG group in terms of the amount and degree of buccal alveolar ridge width resorption (DDE group: 0.45±0.21 mm and 5.9±2.6%; BOG group: 0.45±0.13 mm and 6.2±1.9%, P > 0.05), while both were significant lower than that of NH group (0.78±0.21 mm and 10.0±2.5%, all P < 0.05).
Width absorption amount (mm) of alveolar ridge on 1 mm, 2 mm, 3 mm and 6 mm levels under alveolar ridge crest in different groups. On all levels, the numbers of DDE group were smaller than those of the other two groups
Width absorption amount (mm) of alveolar ridge on 1 mm, 2 mm, 3 mm and 6 mm levels under alveolar ridge crest in different groups. On all levels, the numbers of DDE group were smaller than those of the other two groups
Currently, there are many site preservation techniques to increase bone mass by intervening the bone healing process of the extraction socket, so that to preserve the shape and quality of alveolar ridge [13]. All techniques have their own advantages and disadvantages, varying degrees of site preservation, which could not fully meet the clinical needs. Horváth A et al. [7] studied an systematic review and confirmed that site preservation techniques could effectively reduce the bone absorption on the extraction site, but not eliminate this process. Willenbacher M. et al. [8] found, compared with natural healing, the site preservation method could reduce alveolar bone resorption to certain extent, while it could not completely prevent this process. Atieh MA [9] reviewed that there was no enough evidence to suggest that 6 months after tooth extraction, sites preservation method could effectively reduce the width and height of alveolar bone resorption, there was no difference between the save method in term of the effect on sites preservation.
This study discussed the effects of a new alveolar ridge preservation method–DDE based on periodontal ligament distraction osteogenesis. Periodontal ligament distraction osteogenesis was mainly used in orthodontic extraction of the upper first maxillary premolar through rapidly moving canines to close the extraction space [14, 15]. In the horizontal direction, the canines were rapidly drawn into the missing teeth area by periodontal ligament distraction osteogenesis, and the average movement of teeth was 5.7–6.5 mm within 3 weeks. Liou [10] divided the process of osteogenesis into five stages based on the X-ray as following: expansion period of distraction osteogenesis of periodontal ligament, regeneration period of linear bone, shrinkage period of periodontal ligament, hardening and reconstruction period of linear bone and bone maturation period.
In this study, based on the principle of periodontal ligament distraction osteogenesis, we successfully to remove the teeth vertically, and promote the formation of new alveolar bone under the root, thereby achieved site preservation. Within 4 weeks, the average of tooth distraction was 7 mm with mobility degree of II, without obvious root absorption, periodontal inflammation and other adverse reactions. The comparison among the three groups showed that there was no significant difference between the BOG group and the NH group in term of the maintenance of the alveolar ridge height, while the alveolar ridge height absorption of DDE group was significantly lower than that of the two control groups. For preservation of the alveolar crest width, the DDE group was obviously better than the NH group and the BOG group. For preservation of the middle and lingual alveolar ridge width, the effect of DDE group was similar to that of BOG group, which was significantly better thanNH group.
Recalling the healing mechanism of extraction socket, it showed that 5–8 days after extraction, immature bone began to fill the extraction sockets and its sharp bony ridge on edge conducted absorption and reconstruction. After one month, two-thirds of extraction socket was filled by fibrous bone, and then transited to mature bone, which caused the reduction in height and width of alveolar ridge. Some studies showed the decrease of buccolingual alveolar ridge crest width in extraction socket could persist for about one year and reduce to 50% [16]. The bone loss of alveolar crest on buccal side was most remarkable [17, 18]. Min S et al. [19] found 3 months after tooth extraction, the alveolar bone were lost nearly two-thirds at the 1 mm level below alveolar bone crest, while at the ≥3 mm level below alveolar bone crest, bone preservation could up to over three-quarters. Thus, the bone loss of buccal bone plate in extraction socket was the main causing of the height decrease of alveolar ridge, particularly significant in width loss of alveolarridge.
In this study, three months after tooth extraction, at 1 mm level below alveolar bone crest, the alveolar bone loss of NH group reached 69.9%, which was consistent with the previous studies. While the alveolar bone loss in DDE group was about one-third, and the loss in BOG group was one-half. It significantly showed that the alveolar ridge height was higher than that of the other groups. Therefore, we found that DDE could better keep bone height, especially the height of buccal bone plate, so that better keep of the alveolar ridge width. In addition, this study clarified that vertical periodontal ligament distraction osteogenesis could effectively accumulate new bone on the traction root side. New bone gradually filled extraction socket along with the constantly upward traction of the teeth, which was more conducive to maintain the height and width of alveolar ridge in extraction area. In the future, we expect to be able to pull out the teeth at a faster rate, and to dive deeper into the potential of periodontal ligament.
Conclusion
This study demonstrated that DDE could be regarded as a preferable method for alveolar ridge preservation, when compared with NH or Bio-Oss bone dust implant and GBR after traditional tooth extraction.
Conflict of interest
The authors declare no conflict of interest.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (Grant No. 81271164).