
Abstract
OBJECTIVE:
To investigate the correlation between carotid artery stenosis (CAS) measured by magnetic resonance imaging (MRI) and the coronary stenosis (CS) determined by computed tomography angiography (CTA).
METHODS:
In this prospective study, 42 subjects diagnosed with coronary artery disease (CAD) underwent MRI and CTA examinations. The severity degree and number of CAS, the score, detection rate and type of carotid plaque, and also the severity degree and number of CS were assessed. Spearman’s rank correlation test was used to evaluate the correlation between CAS and CS.
RESULTS:
CS was detected in 42 (100%) subjects, while CAS was detected in 36 (85.7%) subjects. Distribution of CAS severity grades in multiple-vessel group was significantly different from other groups, which with more moderate and severe stenosis (p < 0.05). A positive and significant correlation between the CAS severity and CS severity (r = 0.612, p < 0.05), and the number of involved coronary vessels (r = 0.572, p < 0.05) were observed, respectively. Both detection rate (r = 0.587, p < 0.05) and score (r = 0.735, p < 0.05) of carotid plaque showed a good correlation with the number of involved coronary vessels. After carotid MRI, 71 carotid plaques were detected in 42 subjects, with an incidence rate of 9.9% in subjects with mild CS, 18.3% in moderate CS and 71.8% in severe CS.
CONCLUSION:
Correlation between CAS measured by MRI and CS determined by CTA was identified in present study. These results indicated that the non-invasive CAS evaluation employing the MRI may be clinically useful for the assessment of CS.
Introduction
Coronary artery disease (CAD) is the most common type of cardiovascular diseases and recognized as the primary risk factor for heart failure development [1, 2]. In recent years, the prevalence of CAD are increasing year by year due to the aging of population and the change of dietary [3, 4]. Thus, it is important to timely diagnose and predict the presence of CAD. Although selective coronary angiography (SCA) remains the golden standard for the anatomical evaluation of coronary artery disease, SCA is invasive, high-risk and, therefore, may not be practical for routine use in the management and risk assessment of patients with CAD [5, 6]. Recently, some non-invasive methods, such as multi-slice computed tomography (CT) and dual source CT, are emerging as the alternative imaging modality for the patients with CAD [7, 8]. However, the radiation exposure and contrast agent become a major challenge in the wide application of CT [9]. Currently, identifying and daily managing a high-risk CAD population with coronary stenosis (CS) is clinically difficult. Obviously, an alternative non-invasive diagnostic test that can detect and predict the symptoms of CAD seems necessary.
Carotid artery stenosis (CAS) is a marker of atherosclerosis that is a systemic disorder that involves multiple arterial beds [10, 11]. Previously, it is reported that the intima-media thickness (IMT) of carotid arteries is associated with coronary risk factors. Recent studies supported the concept that lesions in coronary arteries is closely related to that in carotid arteries [12, 13]. CAD were independently related to the presence of severe CAS [14]. Thus, it is possible that CS may be assessed by evaluating the presence and characteristics of CAS. Magnetic resonance imaging (MRI) is a new, non-invasive imaging tool, which provides accurate anatomical images and has been advocated as an accurate method for carotid atherosclerosis [15, 16]. Additionally, carotid MRI can track the disease progression and regression, and quantitatively evaluate a spectrum of parameters associated with plaque morphology and composition [17]. Determination of the MRI application in CAS may be useful to the CAD prediction. Thus, the objective of present study was to investigate the correlation between CAS measured by MRI and the CS, expecting that find an alternative non-invasive diagnostic test for the diagnose and prediction of CAD. We measured the CS by computed tomography angiography (CTA) and the CAS by MRI. We also investigated the association between the CS and CAS.
Methods
Patients and study design
This prospective study recruited subjects with CAD, who underwent coronary CTA examination in the Second Affiliated Hospital, Kunming Medical University from July 2016 to July 2018. Subsequently, carotid MRI was performed in these patients who underwent coronary CTA examination within two weeks. A total of 42 subjects were recruited in this study. There were 24 male and 18 female subjects aged from 45 to 86 years (mean, 64.36±1.86 years). The baseline characteristics of the included subjects were shown in Table 2. The study was approved by the Institutional Review Board of Second Affiliated Hospital, Kunming Medical University according to Helsinki declaration.
The inclusion criteria of the study subjects were: 1) subjects with sinus rhythm and breath holding for more than 10 seconds; 2) subjects without coronary stent implantation or recent coronary artery surgery history. The exclusion criteria were: 1) subjects with iodine allergy and claustrophobia, and subjects who cannot control breathing; 2) subjects with severe cardiopulmonary and hepatorenal dysfunction, obvious arrhythmia, atrial fibrillation and premature beat; 3) subjects with severe artifacts from metallic implants after cardiac pacemaker or artificial heart valve replacement; 4) subjects with neck tumours or a history of neck and coronary surgery.
Coronary CTA examination
All coronary CTA examinations were performed using Philips Brilliance 256-slice spiral CT scanner (Philips Medical Systems, Netherlands). A standardized protocol was performed as described elsewhere [18]. After subjects rested 10 minutes, the scans were initiated under full inspiration 6 seconds. 60–90 mL of nonionic contrast agent iopromide (Ultravist; Bayer Schering Pharma AG, Berlin, Germany) was intravenously injected at a flow rate of 5.0–6.0 mL/s into the antecubital vein using dual-tube high pressure syringe (Nemoto Kyorindo, Japan), followed by 30 mL saline at the same flow rate. The entire volume of the cardiac anatomy was scanned in a single breath hold of 4–6 seconds. Scan parameters were a rotation time of 0.27 s, peak tube potential of 120 KV, tube current of 600–800 mA, field of view 140–190 mm, scan length 88–133 mm, 0.65×128 mm detector configuration, slice thickness of 0.8 mm, reconstruction interval of –0.4 mm, pitch of 0.16–0.18 and matrix size of 512×512. All images were analysed using the Extended Brilliance Workspace (Philips Medical Systems, Netherlands).
The coronary arteries were evaluated on a segmental basis using a modified 13-segment coronary arterial model according to the American Heart Association standards [19]. The stenosis of main left coronary artery, right coronary artery, left anterior descending branch and left circumflex branch was evaluate. Branch stenoses were not considered in this analysis. Each stenosis was assessed visually and three grades of stenosis severity were used for this evaluation: (a) mild stenosis (≤50%); (b) moderate stenosis (50% –75%); and (c) severe stenosis (>75%). According to the number of vessels involved in CS, subjects were grouped into three groups: one-vessel involvement, two-vessel involvement, and multiple-vessel involvement, which were used to evaluate the correlation of CA lesion numbers and CAS.
Carotid MRI examination
All image acquisitions were performed with a high-resolution Philips Achieva 3.0T MRI scanner using 16-channel head-and-neck coil (Philips Medical Systems, Netherlands). A standardized protocol with multiple weighting techniques for carotid MRI was performed as described previously [20]. Subjects were scanned axially in the supine position with the neck positioned at the isocenter of the magnet. The position of the neck and head was fixed to reproduce a stable flexion angle. In all subjects, bilateral carotid arteries were examined. The phase-contrast technique and bright-blood angiography were used to acquire the exact location of the forking artery. Then, time-of-flight (TOF) bright-blood angiography was performed to acquire the T1-weighted images (T1WI), T2-weighted images (T2WI) and proton density images (PDWI). The scan area was 2 cm above and below the carotid bifurcation. Each MRI examination took approximately 40 minutes depending on the cardiac frequency. The scan parameters of carotid MRI were listed in Table 1.
Scan parameters of carotid MRI
Scan parameters of carotid MRI
MRI, Magnetic resonance imaging; T1WI, T1-weighted images; T2WI, T2-weighted images; PDWI, proton density images.
Baseline characteristics of the included subjects
The stenosis severity of CAS was evaluated according to North American Symptomatic Carotid Endarterectomy Trial (NASCET) method [21]. Percentage of stenosis was calculated as follows: Percentage of stenosis = 1–N/D×100%, wherein N is the narrowest diameter of the stenosis in cross-section, and D is the diameter of the normal vessel at a point distal. Five grades of CAS severity were used for this evaluation: grade 0 (no stenosis, 0%), grade 1 (mild, <30%), grade 2 (moderate, 30% –69%), grade 3 (severe, 70% –99%), grade 4 (occluded, 100%). A semi-quantitative analysis was used to calculate the plaque score according to the method described by Cai et al [22]: 0 score (no plaque); 1 score (1 plaque with thickness ≤2 mm); 2 scores (2 plaques with thickness ≤2 mm or 1 plaque with thickness >2 mm); 3 scores (a least one of the 2 plaques with thickness >2 mm); 4 scores (more than 2 plaques with thickness >2 mm).
The assessment of CAS or CS, the classification of carotid plaque and plaque score, and all image reading were performed independently by two experienced radiologists according to the diagnostic evaluation criteria. If the results are inconsistent, they will be evaluated by a senior experienced radiologist.
All statistical analyses were performed by IBM SPSS Statistics Version 17.0 (IBM Corp., USA). Qualitative data were described by number or percentage and the comparison among groups was analysed by chi-square test. Quantitative data were expressed as means±standard deviation (SD) and the comparison among groups was analysed by students’ t-test or the analysis of variance (ANOVA). Spearman’s rank correlation test was used to evaluate the correlation between CAS measured by MRI and the CS determined by CTA. All statistical tests were two-sided, significance set at p < 0.05 along with 95% confidence intervals (CI).
Results
Correlation between CS severity and CAS severity
The severity of stenosis detected by CTA or MRI was listed in Table 3. Figures 1–3 showed the representative cases with different severity of stenosis. CS was detected in all 42 (100%) subjects, including 10 (23.8%) cases with mild stenosis (Fig. 1A and 3A), 18 (42.9%) moderate stenosis (Fig. 1B, 2A and 2B), and 14 (33.3%) severe stenosis. CAS was detected in 36 (85.7%) subjects and 6 (14.3%) subjects had no CAS (Fig. 3B–3D). Among these 36 subjects, 15 (35.7%) had mild stenosis (Fig. 1C–1E, and Fig. 2C–2E), 18 (42.9%) moderate stenosis, 3 (7.1%) severe stenosis and no one had complete occlusion. By using Spearman’s test, a positive and significant correlation between the CAS severity and CS severity was observed (r = 0.612, p < 0.05).
Correlation between CAS severity and CS severity
Correlation between CAS severity and CS severity
CAS, carotid artery stenosis; CS, coronary stenosis.
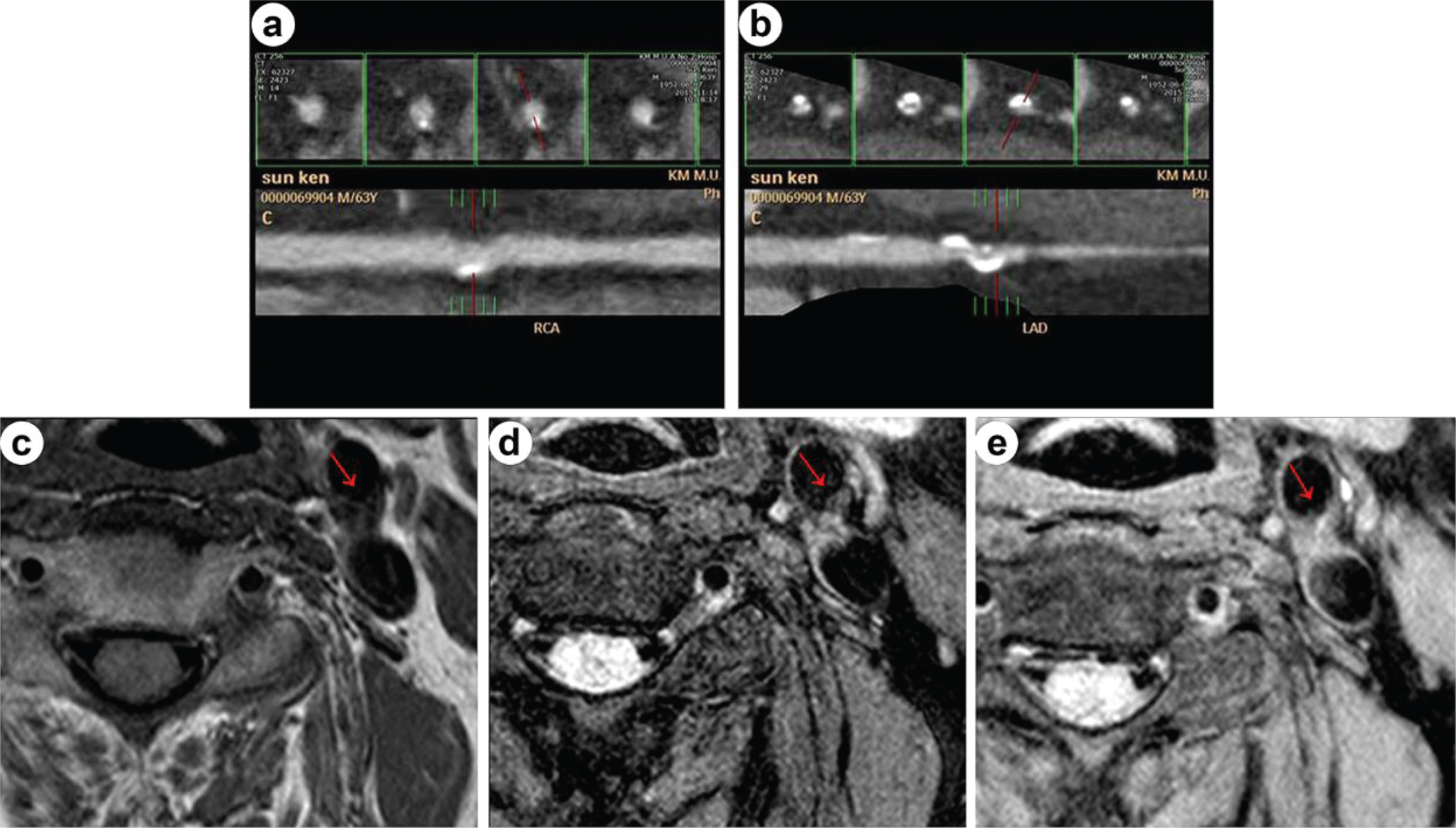
A 63-year-old male subject. Coronary CTA examination showed the small plaque and mild stenosis of right coronary artery (a), and the plaque and moderate stenosis of left anterior descending artery (b). Carotid MRI examination showed the small plaque and mild stenosis at the posterior wall of left common carotid artery (red arrow). Lesions showed iso- or slightly hypo-intense signal on T1WI (c), iso- or slightly hyper-intense signal on T2WI (d), and slightly hyper-intense signal on PWDI (e).
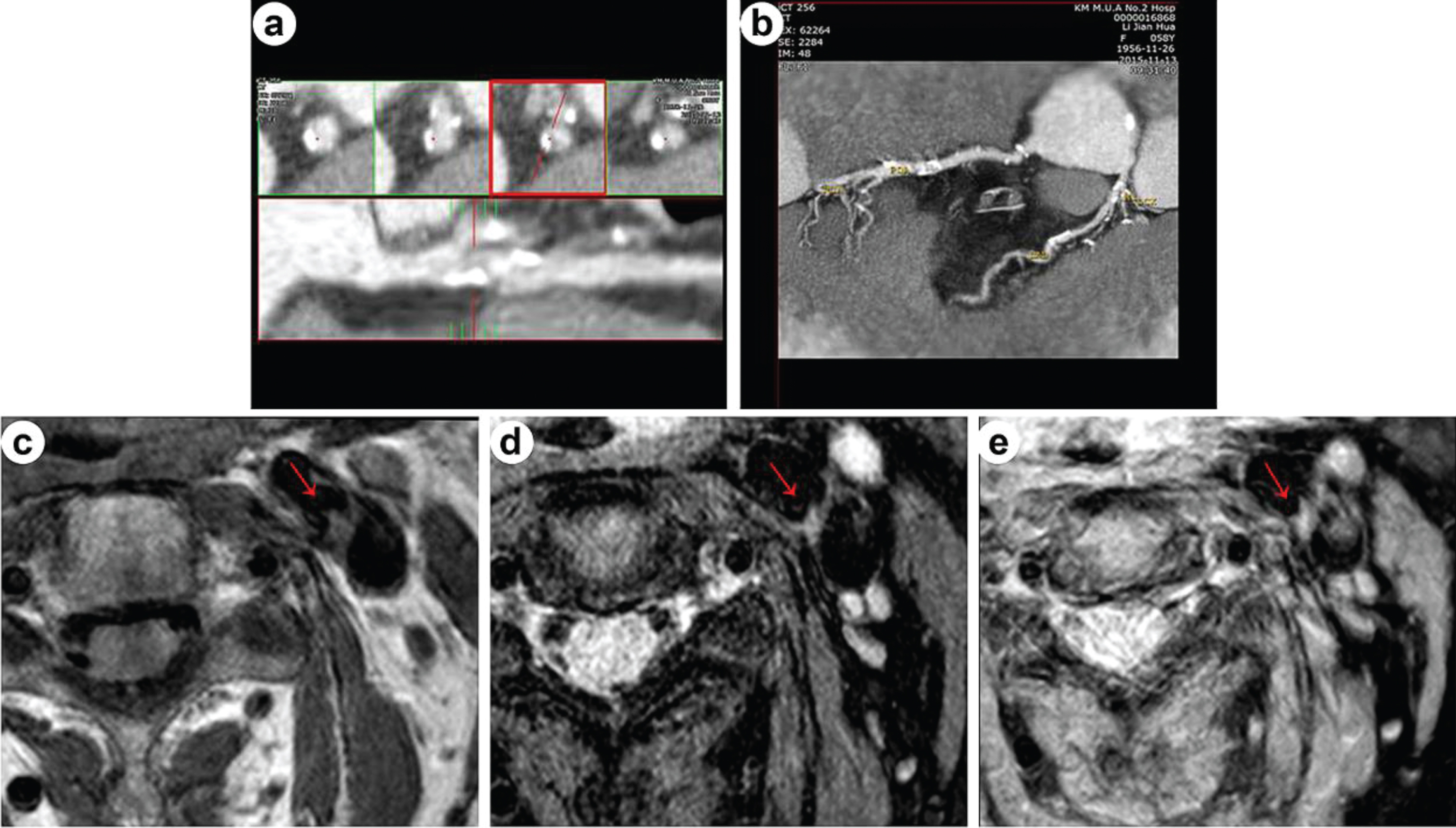
A 59-year-old female subject. Coronary CTA examination showed the soft plaque and moderate stenosis of left anterior descending artery (a-b). Carotid MRI examination showed the small plaque and mild stenosis at the posterior wall of left common carotid artery (red arrow). Lesions showed iso- or slightly hypo-intense signal on T1WI (c), slightly hyper-intense signal on T2WI (d), and slightly hyper-intense signal on PWDI (e).
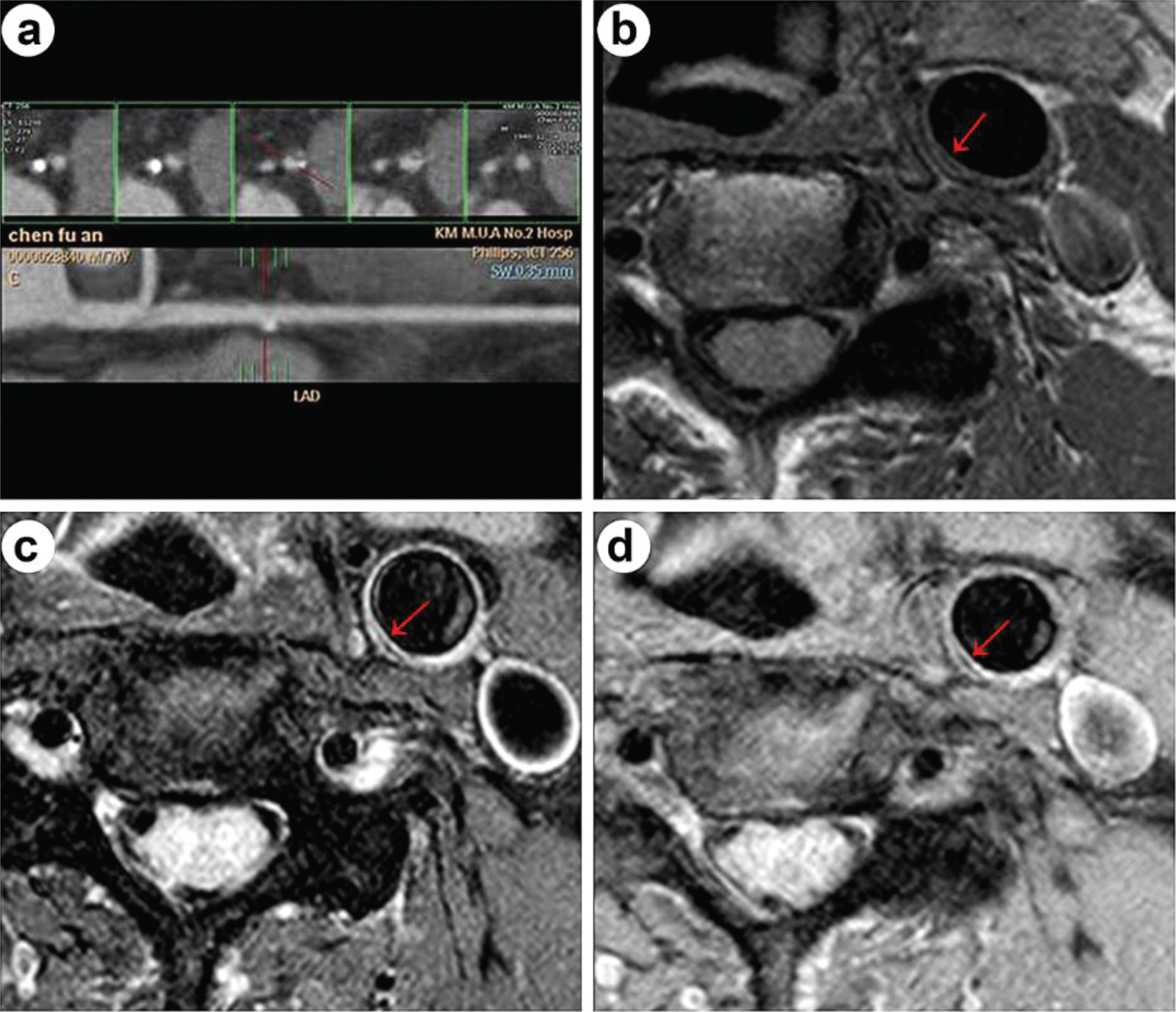
A 74-year-old female subject. Coronary CTA examination showed the soft plaque and mild stenosis of left anterior descending artery (a). Carotid MRI examination showed the small calcified plaque at medial wall of left common carotid artery (red arrow) and no significant stenosis. Lesions showed hypo-intense signal on T1WI (b), T2WI (c), and PWDI (d).
Among 42 subjects, 8 (19.05%) subjects had one-vessel involvement, 10 (23.81%) two-vessel involvement, and 24 (57.14%) multiple-vessel involvement. A positive and significant correlation between the number of involved coronary vessels and CAS severity was observed (r = 0.572, p < 0.05, Table 4). The distribution of CAS severity grades in multiple-vessel group was significantly different from other groups, which with more moderate and severe stenosis (p < 0.05).
Correlation between the number of involved coronary vessels and carotid artery stenosis severity
Correlation between the number of involved coronary vessels and carotid artery stenosis severity
Carotid plaque was detected 29 (69.0%) subjects by carotid MRI examination. Among them, 2 subjects had one-vessel involvement, 6 two-vessel involvement, and 21 multiple-vessel involvement. Thus the detection rates of carotid plaque were 25.0%, 60.0% and 87.8%, respectively (Table 5). The detection rate of carotid plaque in subjects with one-vessel involvement was significant lower than other groups (p < 0.05, Table 5). Besides, the score of carotid plaque in subjects with one-vessel involvement was significant lower than other groups (p < 0.05, Table 5). A positive and significant correlations between the number of involved coronary vessels and both the detection rate (r = 0.587, p < 0.05, Table 5) and score of carotid plaque were observed (r = 0.735, p < 0.05, Table 5).
Correlation between the number of involved coronary vessels and carotid plaque
Correlation between the number of involved coronary vessels and carotid plaque
After carotid MRI examination, among 71 detected carotid plaques in 42 subjects, 7 (9.9%), 13 (18.3%) and 51 (71.8%) were detected in mild, moderate and severe CS cases, respectively (Table 6). The majority of carotid plaque was type I-II (71.4%) in mild CS, type I-II (38.7%) and III (38.7%) in moderate CS, and type IV-V (37.3%) and VI (29.4%) in severe CS. A total of 37 vulnerable plaques (type IV-V) and 34 stable plaques were respectively detected.
Type of carotid plaque according to coronary stenosis severity
Type of carotid plaque according to coronary stenosis severity
It is important to evaluate the degree of CS when assessing disease activity and severity in atherosclerosis [13]. However, multiple methods such as angioscopy and intravascular ultrasound are not practical on a routine management and risk assessment of CAD patients because these techniques are invasive [23–25]. Notably, the carotid vascular wall is more accessible than the coronary artery tree, with a less expensive, more accurate and safer technology [26]. Thus, it might be more interesting to known if the CAS detected by carotid MRI examination may predict the severity of CS. To our knowledge, this is the first study investigating the association between CAS detected by MRI and CA detected by CTA from multiple perspectives, including the severity of stenosis, the involved coronary vessels and carotid plaque. The study demonstrated that the CAS and carotid plaque were strongly associated with the CS, indicating that the non-invasive CAS evaluation employing the MRI may be clinically useful for the assessment of CS.
Both the coronary artery and the carotid artery could be affected by atherosclerosis [14]. Thus, CAS and CAD are usually detected simultaneously in patients in clinical practice [27, 28]. In present study, we defined the severity of CAS and CS respectively, and divided them into different grades. One highlight of this study was the finding of positive correlation between the CAS severity and CS severity. We observed that the degree of CS is increasing with the aggravation of the degree of CAS. In addition, a positive and significant correlation between the number of involved coronary vessels and CAS severity was observed. As the degree of CAS increased, the number of CS involved vessels increased. Similarly, Zhang et al reported that the presence of CAS was weakly correlated with the extent of CAD [14]. Although a correlation between the severity of CAD and CAS has been demonstrated by these clinical studies, they only focused on the number of vessels involved and did not analyse the correlation from multiple perspectives [14, 28]. We firstly investigated the association between CAS detected by MRI and CA from multiple perspectives, including the severity of stenosis, the involved coronary vessels and carotid plaque.
Several reports suggested that carotid IMT is a strong predictor of the extent of CAD [29, 30]. But some researchers hold the opinion that IMT is only a tool for early atherosclerosis prediction, and only weakly correlated with the extent and severity of CAD [31]. Thus, the role of IMT as a marker of atherosclerosis has been questioned. New evidence suggested that the presence and number of plaques was a stronger predictor of cardiovascular risk compared with IMT [32, 33]. Therefore, in present study, the correlation between the severity of CS and carotid plaque was also analysed. Obviously, the study demonstrated that the carotid plaque were strongly associated with the CS. A positive and significant correlations between the number of involved coronary vessels and both the detection rate and score of carotid plaque were observed. In another word, if peripheral atherosclerosis has plaque and with higher plaque score, it indicated that the corresponding CS involves more vessels, that is, the CS degree is more serious. Previously, Zhao et al have also reported the significant correlation between coronary plaque phenotype and carotid plaque composition [12], which is consistent with our result. Additionally, Osamu et al also proposed that carotid plaques could predicted coronary plaque complexity and the development of future coronary complications in patients with stable CAD, which further supported our findings [13]. Overall, these results indicated that carotid plaque detected by MRI was strongly associated with the presence of CS and may be predict the development of CAD.
Additionally, the present study investigated the types of carotid plaque and analysed the potential association between carotid plaque and CS severity for the first time. We found that non-vulnerable plaque (type I-II and III) mainly occurred in the mild and moderate CS, while vulnerable plaque (type IV–VI) mainly in the severe CS. The results demonstrated that in the cases with vulnerable plaque, the degree of CAS has a tendency to increase correspondingly. The previous study indicated that the stenosis progression could reflect the progression CAD [34]. Thus, we can diagnose vulnerable plaque and non-vulnerable plaque through the determination and analysis of carotid plaque components and plaque classification, and then predict the severity of CAD.
There were several limitations in our study. First, the study was limited by the relatively small sample size. Second, the signals of carotid plaque compositions are mixed, which makes it difficult to distinguish between plaques with similar MRI signals, such as intraplaque haemorrhage and lipid necrosis core, fibrous cap and lipid fiber mixed plaque. In this case, plaque typing may be biased. Third, the predictive value as well as risk factors remain to be further studied.
Conclusions
The study demonstrated that the CAS severity were strongly associated with the CS severity. Besides, the number of involved coronary vessels showed a good correlation with the CAS severity, the detection rate and the score of carotid plaque. The results indicated that the evaluation of CAS using a non-invasive MRI examination may be clinically and practically informative for the assessment of CS.
Competing interests
The authors declare that they have no conflict of interest.
Funding
This study was supported by Project of Applied Basic Research Program of Yunnan (Grant number: 2017FE468-178), and Reserve Talents Project for Young and Middle-Aged Academic and Technical Leaders of Yunnan Province (Grant number: 2015HB068), and Medicine Academic Leaders Training Program of Health and Family Planning Commission of Yunnan Province (Grant number: D-201646).
Footnotes
Acknowledgments
Thank Professor Li-Ping He from Kunming Medical University for the help in statistical analysis.