
Abstract
Thyroid cancer is the most common type of endocrine-related cancer and the most common cancer in young women. Currently, single photon emission computed tomography (SPECT) and computed tomography (CT) are used with radioiodine scintigraphy to evaluate patients with thyroid cancer. The gamma camera for SPECT contains a mechanical collimator that greatly compromises dose efficiency and limits diagnostic sensitivity. Fortunately, the Compton camera is emerging as an ideal approach for mapping the distribution of radiopharmaceuticals inside the thyroid. In this preliminary study, based on the state-of-the-art readout chip Timepix3, we investigate the feasibility of using Compton camera for radiotracer SPECT imaging in thyroid cancer. A thyroid phantom is designed to mimic human neck, the mechanism of Compton camera-based event detection is simulated to generate realistic list-mode data, and a weighted back-projection method is developed to reconstruct the original distribution of the emission source. Study results show that the Compton camera can improve the detection efficiency for two or higher orders of magnitude comparing with the conventional gamma cameras. The thyroid gland regions can be reconstructed from the Compton camera measurements in terms of radiotracer distribution. This makes the Compton-camera-based SPECT imaging a promising modality for future clinical applications with significant benefits for dose reduction, scattering artifact reduction, temporal resolution enhancement, scan throughput increment, and others.
Introduction
The thyroid cancer is the most common type of endocrine-related cancer, the most common cancer in women 15 to 30 years old [1], and the second most common cancer after breast cancer in women under 50 [2]. It is estimated that there will be 52,890 new cases in 2020, representing 2.9% of all the new cancer cases in the United States [1]. Differentiated thyroid cancer (DTC), including papillary and follicular cancer, comprises the vast majority (>90%) of all thyroid cancers. Although patients with DTC have a good prognosis, lifelong follow-up is required, since potentially curable local recurrences and distant metastases may occur even decades later [3]. Radioiodine planar imaging with radioactive iodine-123 (I-123) or radioiodine-131 (I-131) plays a major role, and remains the gold standard in follow-up exams after initial surgery. It is highly desirable and challenging to characterize malignant radioiodine uptakes in cancer nodes with high image quality at a minimized dosage.
Currently, radioiodine scintigraphy with the single photon emission computed tomography (SPECT) integrated computed tomography (CT) is widely used to evaluate patients with thyroid cancer [4, 5]. The gamma camera for SPECT consists of a metallic collimator and a gamma ray sensitive detector. However, this structure has many disadvantages: large and heavy, restricted field of view, low detection efficiency, etc. It results in a greatly compromised dose efficiency and a severely limited diagnostic sensitivity. Fortunately, the Compton camera is emerging as an ideal approach to map the distribution of radiopharmaceuticals inside the thyroid. Because the Compton camera does not require any collimator, it can offer a superior detection sensitivity over a broad field of view. Especially in the context of SPECT imaging, this imaging mode improves the image quality and helps reduce the radiation exposure of the patient.
Compton camera is a group of imaging devices that are built based on the so called Compton scattering effect [6]. The scattering effect is the scattering of an x-ray or gamma photon by an electron into a material. The result is a decrease in the energy of the incident photon, and transfer of a part of the photon energy to the recoiling electron. Since the concept of Compton imaging was first reported in 1974 [7], different types of Compton cameras have been constructed for different applications in fields of astrophysics, nuclear medicine, molecular imaging, security inspection, and so on [8–10]. Although many efforts have been reported to develop Compton cameras for nuclear imaging, to the best of our knowledge, there is still no one that is commercially available, and the Compton camera has not been applied for clinical applications in the nuclear medicine field. The state-of-the-art Compton camera that has a great potential for thyroid imaging is based on an event based readout chip Timepix3 [11]. The Timepix 3 chip is a general-purpose integrated circuit suitable for readout of both semiconductor detectors and gas-filled detectors [12]. It can send every hit pixel immediately to a readout and record the time-of-arrival (ToA) and energy of an incident gamma simultaneously in the pixel. The chip offers high energy resolution (1 keV at 60 keV, 7 keV at 356 keV), as well as time resolution (1.6 ns) [12]. The current pixel size is 55μmx55μm. The Timepix3 readout chip can be combined with different sensor materials. It is a perfect device for creation of a compact Compton camera. In 2018, Turecek et al. presented a very compact detector system AdvaPIX for imaging with gamma-rays using the Compton camera principle [13]. The system consists of two layers of hybrid pixel detectors Timepix3 with the sensors being optimized for gamma-ray tracking. The front detector layer (scattering) is made of silicon of 1 mm thickness, while the last layer (absorbing) is equipped with thick CdTe or CZT sensors up to 2 mm in thickness. In early 2020, this team reported a miniaturized single layer Compton camera MiniPIX consisting of a single Timepix3 detector with a thick 2 mm CdTe sensor. Thanks to Timepix3 high resolution ToA measurement, it is possible to measure the drift time of charge transport within the sensor and thus determine the vertical position (depth) of both interactions. By knowing both energy and position of the events in the sensor, the image of the gamma source can be reconstructed. Those latest advances motivate us to employ the AdvaPIX/MiniPIX to design Compton-camera-based SPECT imaging system to meet the clinical challenges, with the thyroid cancer detection and diagnosis as an example.
In this paper, we will numerically investigate the feasibility of thyroid cancer imaging using Timepix3 based Compton camera and report our preliminary results. In the next section, we present the imaging theory and method. In section III, we report our experimental design and results. In the last section, we discuss related issues and draw conclusions.
Theory and method
In this section, we will present our methodology. It includes the design of thyroid phantom to mimic human neck, the mechanism of Compton camera based event detection, the numerical simulation to generate realistic list-mode data, and the weighted backprojection method to reconstruction the original distribution of the emission.
Thyroid phantom
The thyroid is a butterfly-shaped gland that sits in front of the windpipe (called the trachea) and just below the larynx or Adam’s apple in the neck (see left image in Fig. 1). The thyroid has two lobes, connected by a bridge in the middle [14]. The gland makes thyroid hormone that travels in the blood to all parts of human body. The thyroid hormone controls human body’s metabolism in many ways, including how fast is the calories burned and how fast is the heart beat. Because the iodine is a building block of the thyroid hormones, thyroid tissue has the capacity to concentrate this element. Therefore, radioiodine is widely employed for thyroid functional imaging. According to the statistical information in [15], the averaged width, thickness and length of thyroid right lobe are respectively 1.57 cm, 2.09 cm and 6.18 cm, and the counterparts of thyroid left lobe are respectively 1.52 cm, 1.89 cm and 5.85 cm. To simulate a digital thyroid phantom, we assume a medium-size neck and model it as a cylinder with a 13.0 cm diameter and 13.0 cm height. We also assume that the center of the cylinder sits at the origin of the global coordinate. Two ellipsoid are employed to mimic the lobes (see right image in Fig. 1). The parameters of the lobes are listed in Table 1, where the “center” means the center of each ellipsoid in the global coordinate system, and the “half-axis lengths” are those of the ellipsoid along different directions. Those objects are used to define the thyroid gland regions that can have radioiodine uptakes. SPECT images reveal the radioiodine uptake distributions. Because cancer is rarely found in hot nodules, hot and cold nodules can be judged as benign and malignant respectively by radiologists. That is, we can use different uptake distributions to characterize heterogeneous thyroid nodules, and different uptake distributions in these regions can mimic various pathological states of the thyroid. The radioiodine-131 is assumed inside the thyroid, and gamma rays with 364keV are emitted.
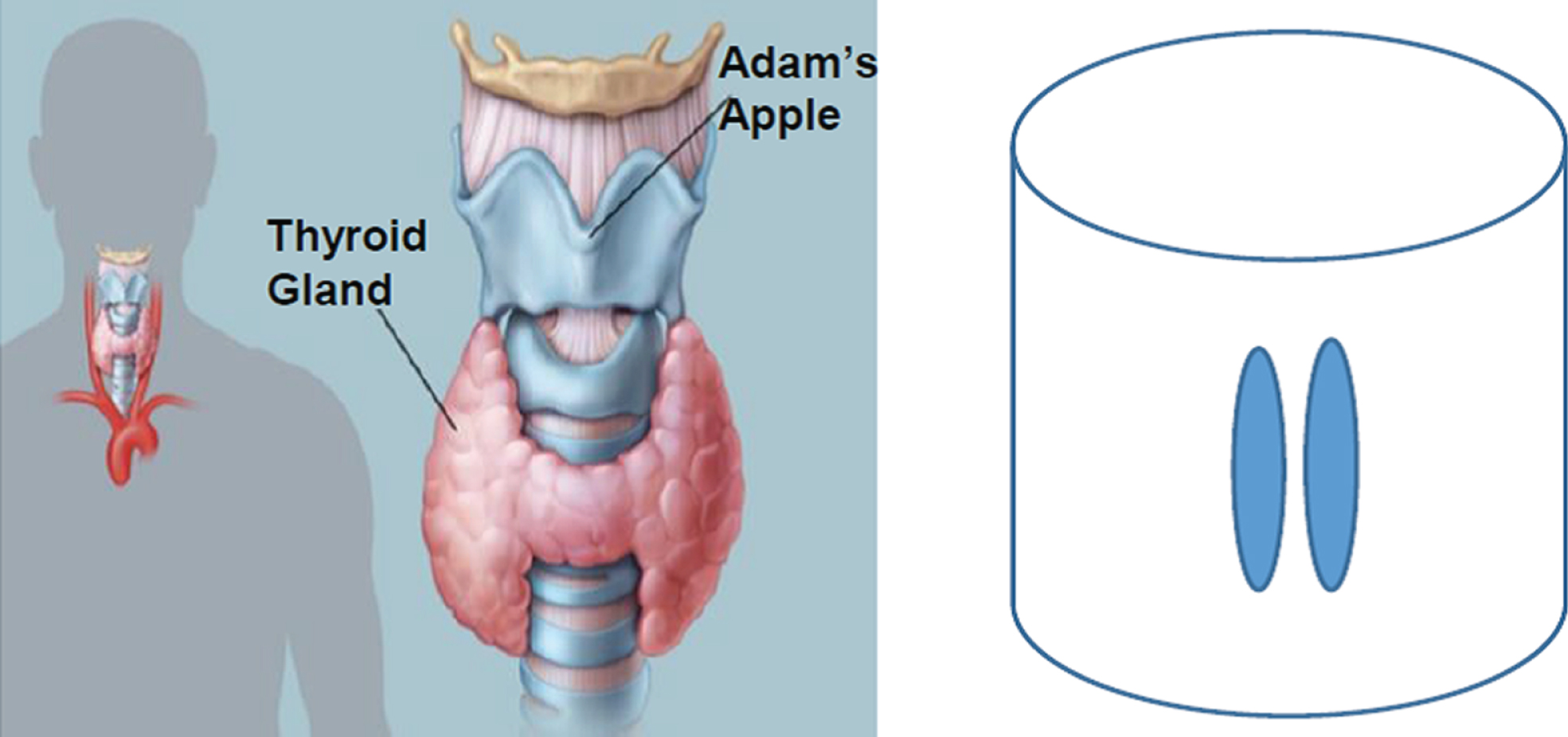
Rendering of the thyroid in the human (left) [14] and the designed digital phantom (right).
Parameters of the thyroid phantom size
Since the purpose of this study is to investigate the feasibility of thyroid imaging, we assume that both lobes are health, and the radioiodine-131 is uniformly distributed inside thyroid tissues. Otherwise, the lesion region will has less radioiodine-131 distribution. This assumption does not affect the evaluation for the follow-up image reconstruction algorithms. In the field of SPECT imaging, the probability for an emitted photon to arrive at a detector depends on the integral of the linear attenuation coefficient along the gamma ray path between the emission and detection sites, which reflects an average of many individual attenuation coefficients of pixels/voxels. Therefore, for most SPECT imaging tasks the attenuation map can be often approximated as a uniform distribution. In this study, we also assume they are homogenous, and a uniform attenuation coefficient of water is assigned to all the phantom pixels. Like the conventional SPECT imaging, the effect of this kind of simplification is endurable for the final results.
Compton scattering is the scattering of an x-ray or gamma photon by an electron into a material [6]. As Illustrated in Fig. 2, assuming the energy of the incident photon is E0 and the electron is in the rest status, the direction of the photon will be changed after it hits the electron. The recoiled electron will have an energy E1, the scattered photon will have an energy E2, and the photon direction will have a change of scattering angle θ. The angle depends on the original energy E0 and the transferred energy E1 of the photon, and it can be described by the Compton equation
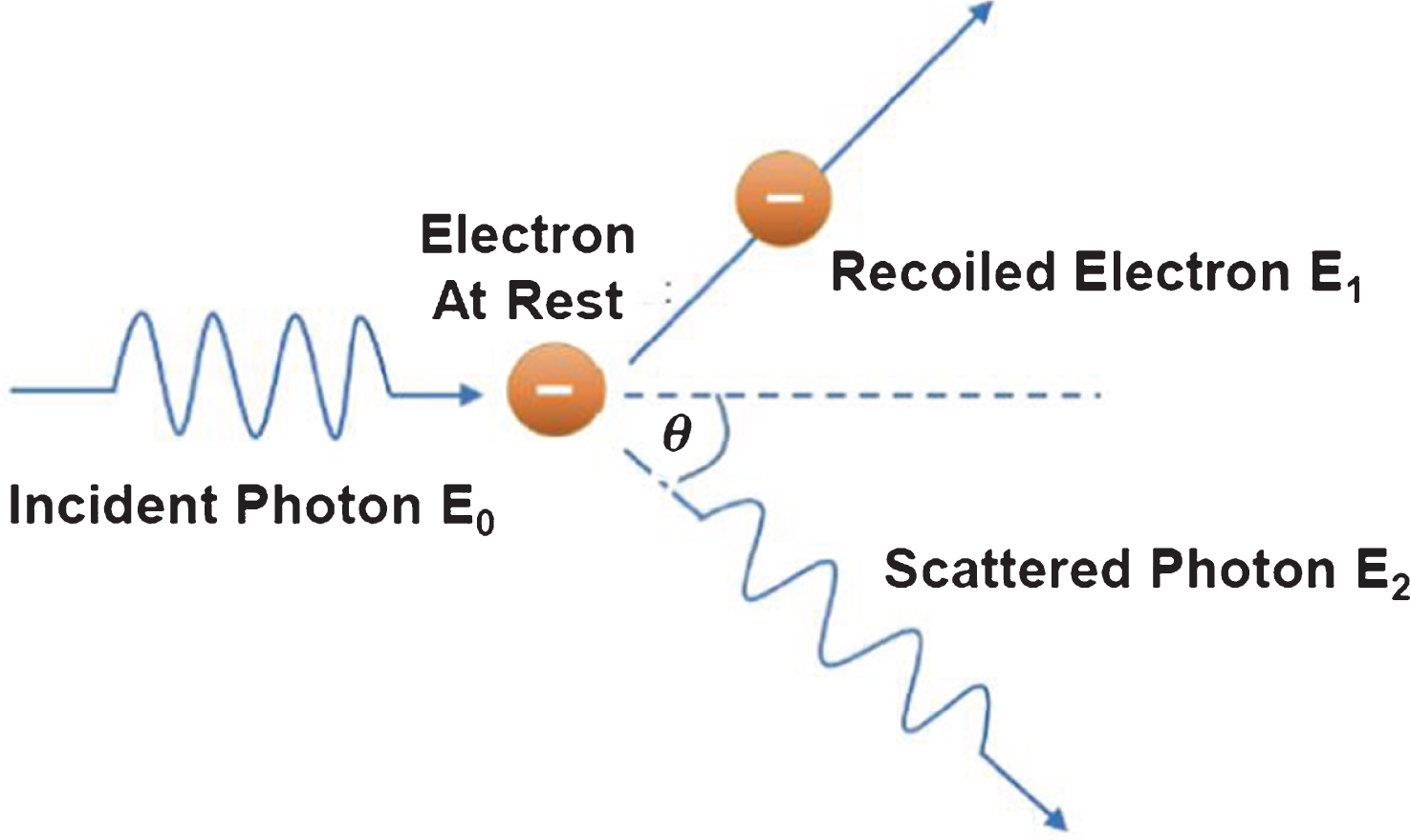
Illustration of Compton scattering.
where m ɛ = 9.109 × 10-31kg is the electron mass, c = 2.998 × 108m/s is the light speed, m ɛ c2 = 8.187 × 10-14J ≅ 511keV and 1keV = 1.602 × 10-16J. Because of the energy conservation, we have E0 = E1 + E2. Equation (1) can also be written in terms of E1 and E2, or E0 and E2.
A typical Compton camera usually consists of two layers. The front layer can record the recoiled electron energy E1 and incident position, and the bottom layer can record the scattered photon energy E2 and the corresponding position. The two positions in layers can uniquely determine the scattering direction. In the three-dimensional space, for a fixed direction of the scattered photon with energy E2 and the scattering angle θ, the potential direction of incident photon with energy E0 can form a cone whose apex angle is 2θ. To image the thyroid phantom designed in the previous subsection 2.1, we assume a cylindrical detector with a diameter of 26.0cm and height of 13.0cm, and both the detector and phantom share the same origin (see Fig. 3).
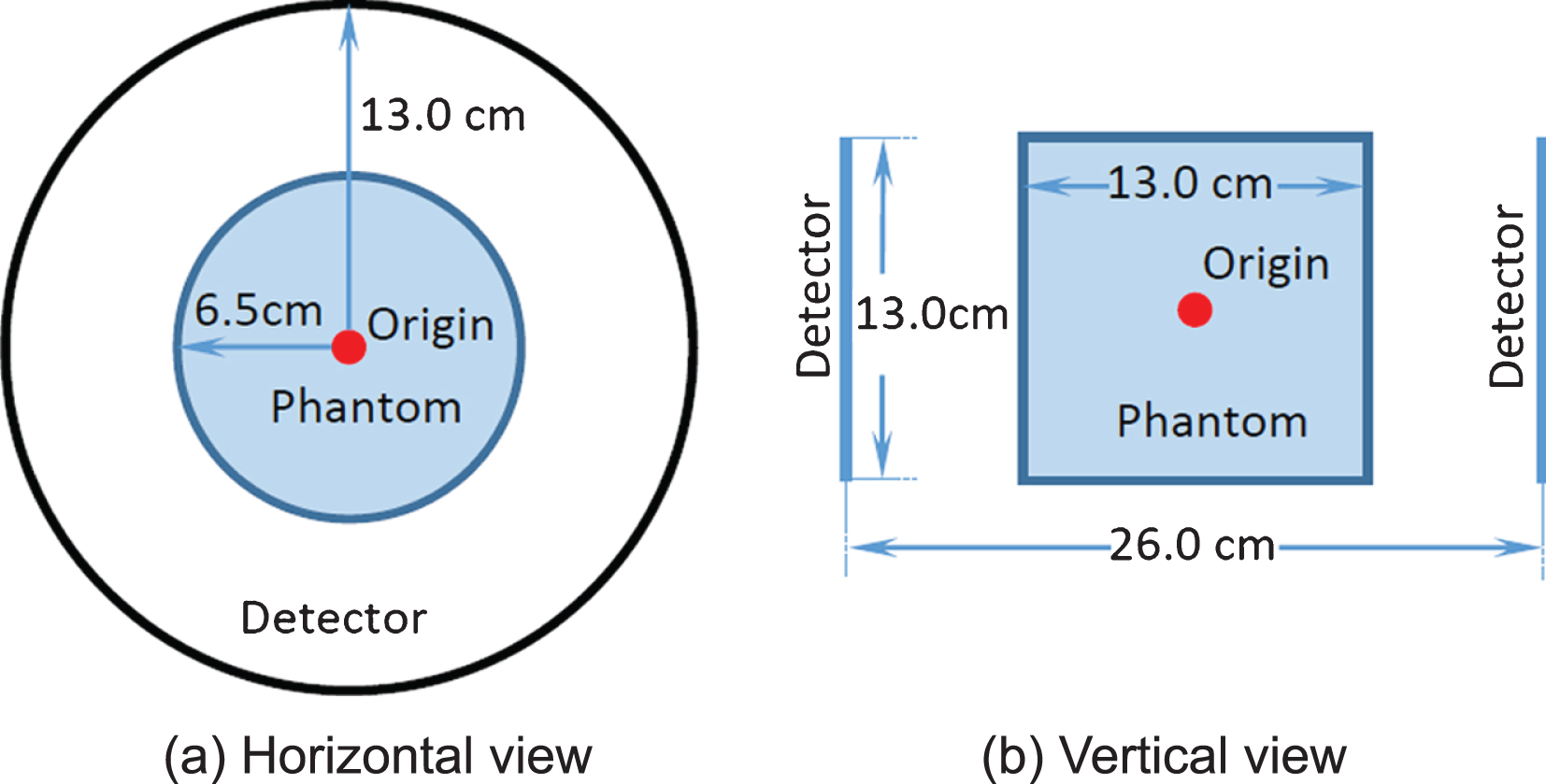
Horizontal and vertical sketch views of the detector and phantom.
The thyroid gland does not distinguish between radioactive and nonradioactive iodine. In clinical applications, a very small dose of radioactive iodine (I-123 or I-131) is administered orally, and images are taken at specified intervals after the initial dose is administered. The radionuclide emits gamma photons, which allows external measurement. Once a gamma photon is emitted from the inside of human body, it will interact with the human tissue (e.g. scattering and absorption) and the procedure can be simulated using the well-established Monte-Carlo method [16]. Because the Compton camera can identify the incoming photon energy, here we use the Beer’s law to mimic the absorption and scattering effects inside the human body. This is because we can use the post-processing steps to discard the photons that arrive at the detector with an energy smaller than the original emission energy. In other words, if a photon was scattered by the soft tissues or other organs inside the human body, its energy will be decreased along with the change of its direction, and this energy decrease can be identified by the Compton detector and discarded by post-processing steps. This is similar to the parallel-hole collimator based photon detection mechanism for the conventional CT and SPECT. Figure 4 illustrate the main geometrical parameters to generate the list-mode data, and the procedure is summarized as the following five steps:
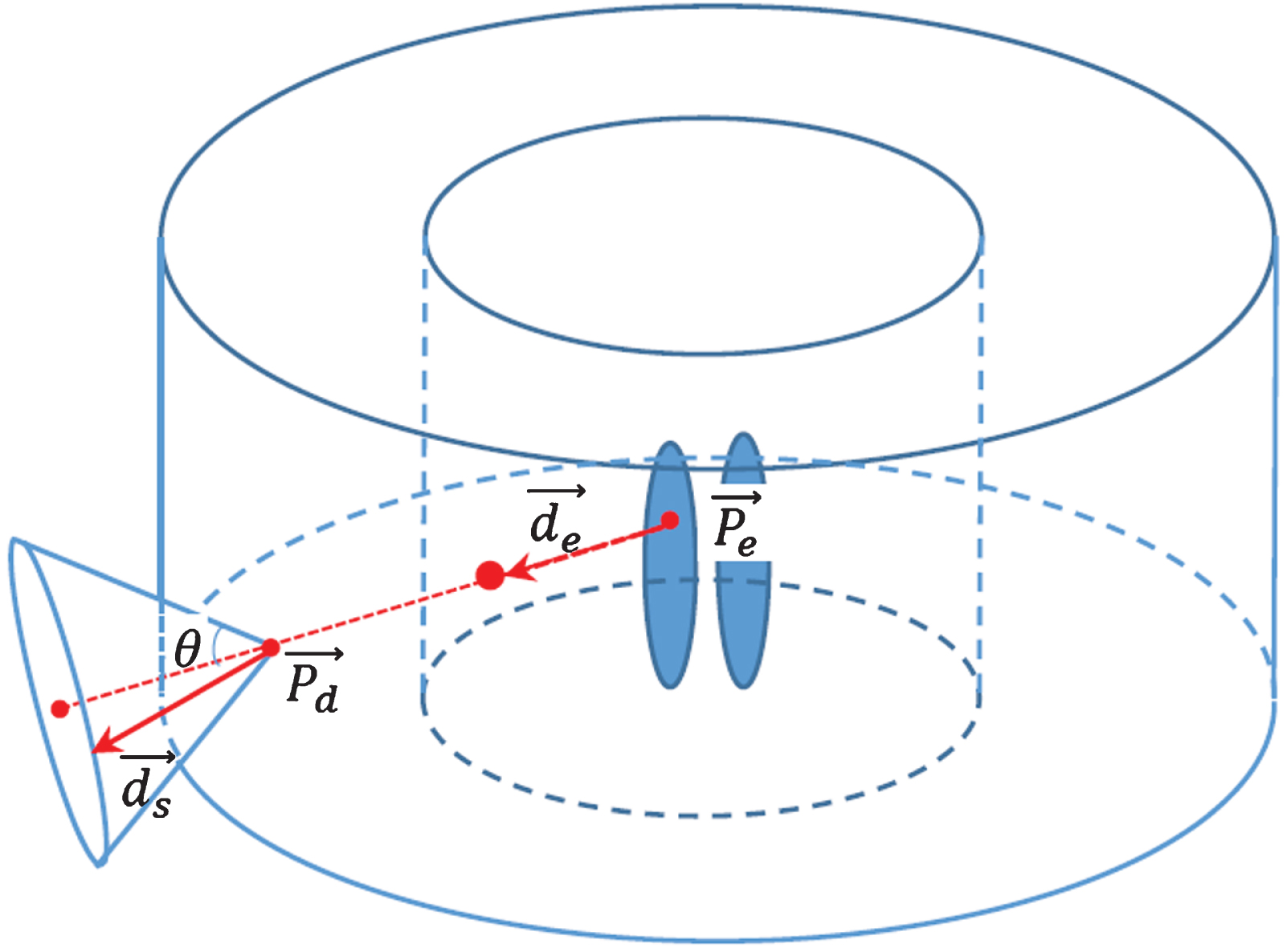
Illustration of list-mode data generation.
To simulate the interaction of a photon with energy E0, an emission position The line integral If the photon can arrive at the Compton camera, the position In the three-dimensional space, for a fixed position If both the recoiled electron with energy E1 and the scattered photon with energy E2 can be detected simultaneously, a qualified event is obtained for image reconstruction. This event can be expressed by a trilet
Once we have sufficient number of detected events in terms of the trilet
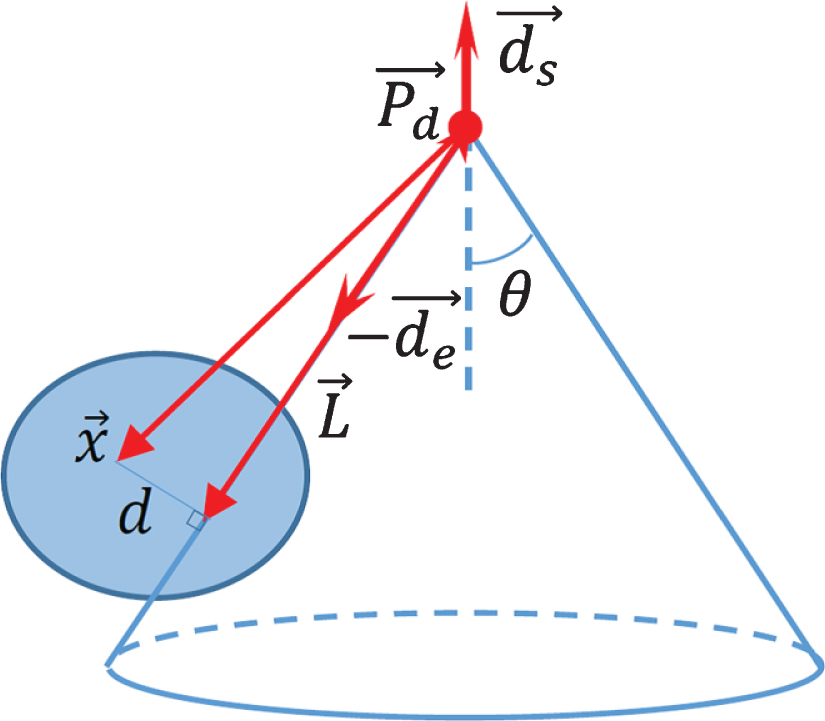
Weighted backprojection in 3D to invert Compton scattering data.
Different from the state-of-the-art backprojection algorithm [20], for a given point vector
In this study, we employ a continuous model for the phantom and a discrete model for the Compton Camera based detector. That is, the coordinates of each emission position
Numerical verification for data generation
To verify the correctness of the list-mode data generation, we assume a total photon number of 2×106 photons, and the photons are uniformly distributed in and emitted from the thyroid gland regions. The experiment is repeated for 10 times, the averaged photon numbers are used to analyze accuracy, and the statistical results are summarized as in Table 2.
Accuracy analysis of the data generation
Accuracy analysis of the data generation
Among all the photons emitted from the thyroid gland regions, 883,050 (44.15%) emission directions can be covered by the Compton camera. That is, if the attenuation coefficient equals to zero inside the phantom everywhere, 44.15% photons can arrive at the Compton camera. To compute the expected photon number for comparison, we assume that all the photons are emitted from the origin for simplification, and the corresponding theoretical value of the probability can be calculated as
To analyze the detection efficiency, a conventional Anger gamma camera for SPECT is also simulated. For fair comparison, we use the same parameter configuration as the Compton camera validation experiment in the above subsection. The only difference is the additional collimator. In our simulation, we assume that the collimators are ideal, that is, the thickness of the collimators are zeros. The collimators are arranged in parallel-fan-beam geometry. In the horizontal plane the collimators forms fan-beam geometry, and in the vertical plane the collimators forms parallel-beam geometry. Again, 2×106 photons are uniformly distributed and emitted from the thyroid gland regions, and the experiment is repeated 10 times. From Fig. 3, one can see that the maximum available depth for the collimator is 6.5 cm in our setting. We acknowledge that the best collimator depth (∼6.0 cm) has been optimized for iodine imaging for SPECT [21, 22], but with a relative greater distance from the source to the detector in this study. To demonstrate the relationship between the collimator depth and detection efficiency as a general conclusion for more general applications, the experiments are repeated for different depths of the collimator, the average of detected photons for different depths are summarized as in Table 3. From Table 3, we can see that the deeper the collimator is for the gamma camera, the less the photons are detected by the gamma camera, and the higher the efficiency ratio is for the Compton camera with respect to the gamma camera. Here, the efficiency ratio is defined as the ratio between the photon numbers detected by the Compton camera and the gamma camera. For a moderate collimator depth (e.g. 3.0 cm), the Compton camera can improve the detection efficiency for two orders of magnitude comparing with the gamma camera. For the optimal collimator depth 6.0cm for iodine imaging, there are only 273 photons being received in total in the Anger system, which is impossible to reconstruct a volumetric image in the current dose level. However, the Compton camera can provide sufficient information to reconstruct the radiotracer distributions (see the results in next subsection). The high detection efficiency has huge benefits for dose reduction, scattering artifact reduction, temporal resolution enhancement, scan throughput increment, and so on. Because of the much-improved detection efficiency, for a given time internal we can receive the same amounts of photons for much less radioiodine uptakes, which implies dose reduction. For the same amount of radioiodine uptakes, we can receive the same amount of photons in a much shorter time interval, which implies a much higher temporal resolution for dynamic imaging. Because the Compton camera does not need the collimator, there is no photon scatter issue of the conventional SPECT camera. Currently, it takes 20 – 30 minutes to do a conventional SPECT scan. If we keep the radioiodine uptakes unchanged (that is, the radiation dose unchanged), it is our expectation that the SPECT scan will be reduced to < 1 minute and hence improve the scan throughput. Meanwhile, the high detection efficiency implies high performance point of care imaging for patients in hospitals and clinics, including but not limited to thyroid cancer. In our simulations, it should be pointed out that the physical size of the Compton camera pixel is 1.0×1.13 mm2. It is way greater than the current state-of-the-art pixel size of MiniPIX Compton camera (55×55μm2). If a smaller Compton camera pixel size is used for numerical simulation, the corresponding efficiency ratio in Table 3 will be increased to higher orders of magnitude.
Detection efficiency analysis results
Detection efficiency analysis results
To reconstruct the original distribution of the gamma emission sources for Compton camera based SPECT imaging, the backprojection algorithm was developed. Previously, the backprojection method was reported for Compton camera based 2D imaging [20, 23]. Here, our focus is 3D imaging, and the backprojection algorithm in the subsection 2.4 is implemented in C++. For the thyroid phantom, the reconstructed volumetric image size is 150×150×150, and each voxel size covers a cubic region of 0.87×0.87×0.87 mm3. For different total photon numbers, the reconstructed volumetric images are shown in Fig. 6, and the thyroid gland regions are magnified in Fig. 7. Those 3D rendering images are generated using MatLab (Version R2020a, MathWorks, Natick, MA) Volume View App via maximum intensity projection. One can see that the greater the total photon number is, the smaller the reconstructed noise level is. This is consistent with the general knowledge that a greater photon number implies higher radiation dose and better reconstructed image quality.
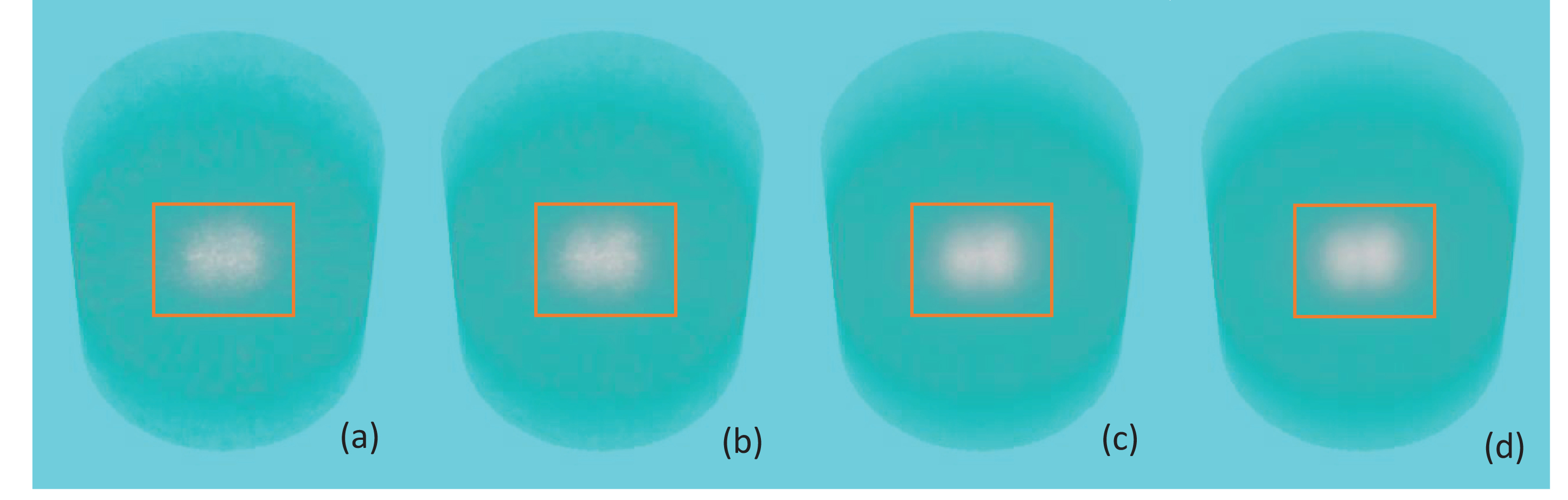
Maximum intensity projection rendering of 3D backprojected volumetric images from the simulations with different total photon numbers (a) 8×104, (b) 2×105, (c) 8×105, and (d) 2×106, respectively. Squares indicate the regions to be magnified in Fig. 7.
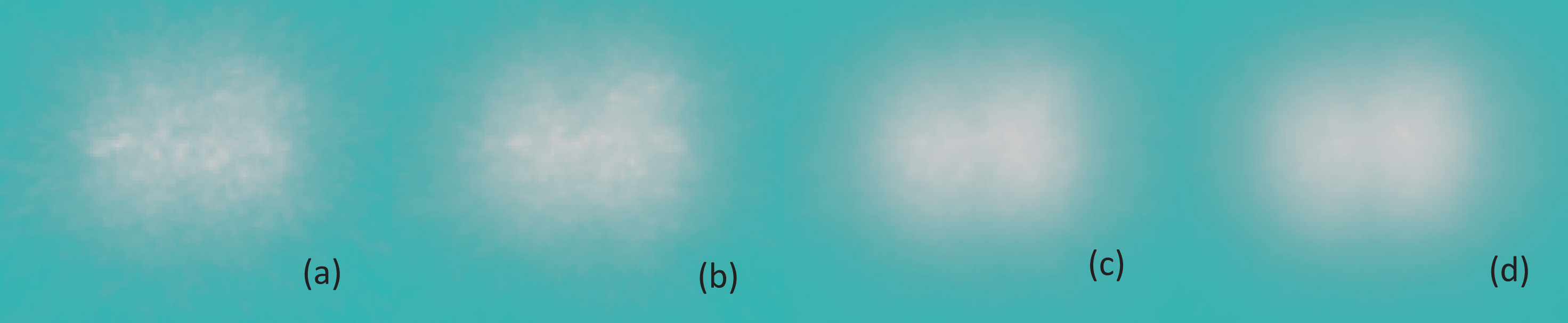
Magnified thyroid gland regions in Fig. 6. (a)∼(d) are corresponding to the counterparts in Fig.(6).
Although the backprojected image quality can be improved by increasing the number of emission photons, those images still suffer from blurring effects and noise that are the inherent shortcomings of the backprojection algorithm. In the CT field, it is well known that filtering plays an important role to deblur the backprojected images. When the projections in terms of Radon transform are backprojected into the image space, a ramp filtering can be used to deblur the backprojected images to recover the original ones. Inspired by this knowledge, we introduce a ramp filter on the backprojected images for the Compton camera. Particularly, denote the 3D Fourier transform of the backprojected image as
where
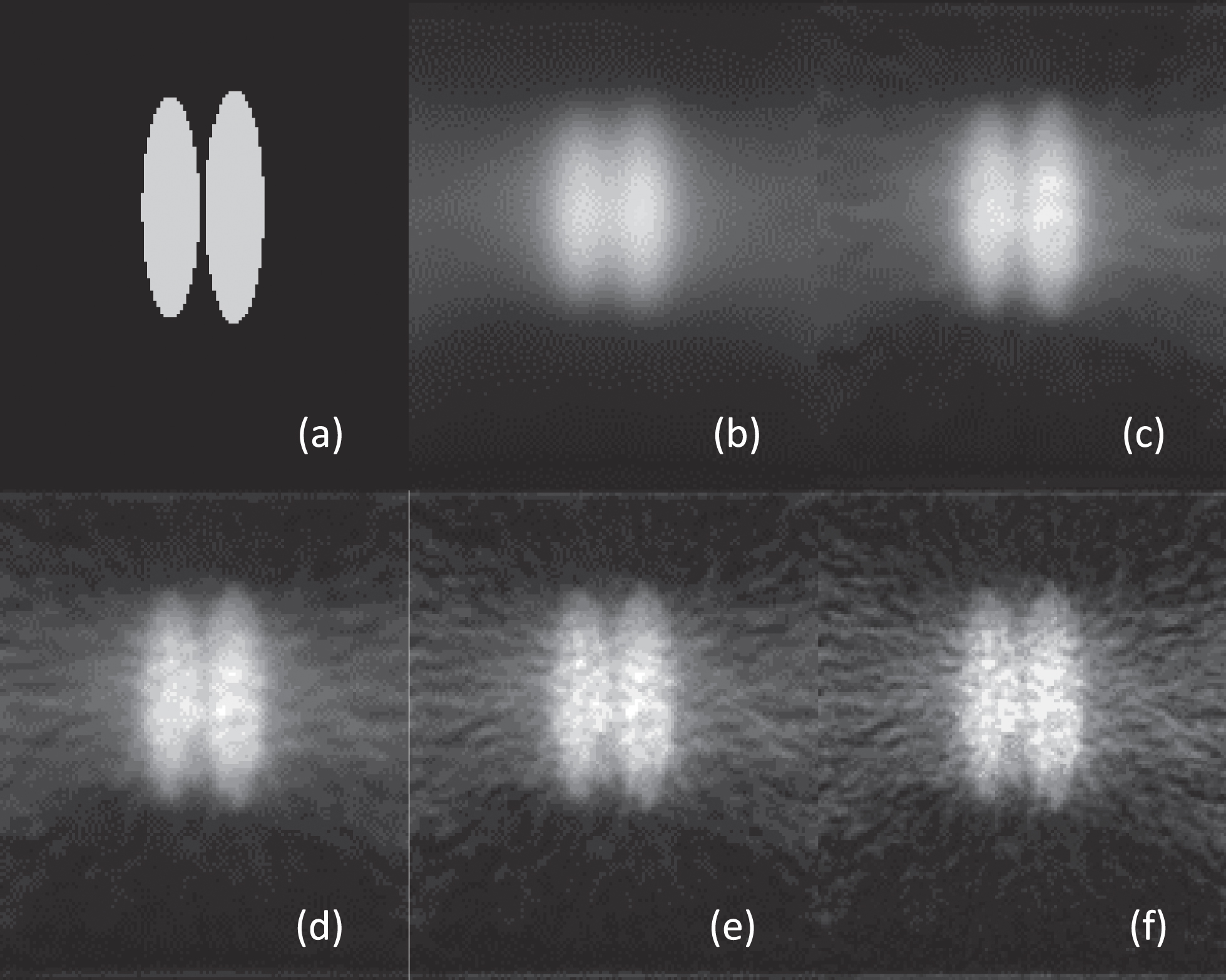
Sagittal view of the deblurred results of Fig. 6 (d) using different window length for ramp filtering. (a) is the ground truth; and (b)-(f) are the results of ρ = 0.2, 0.4, 0.6, 0.8 and 1.0, respectively.
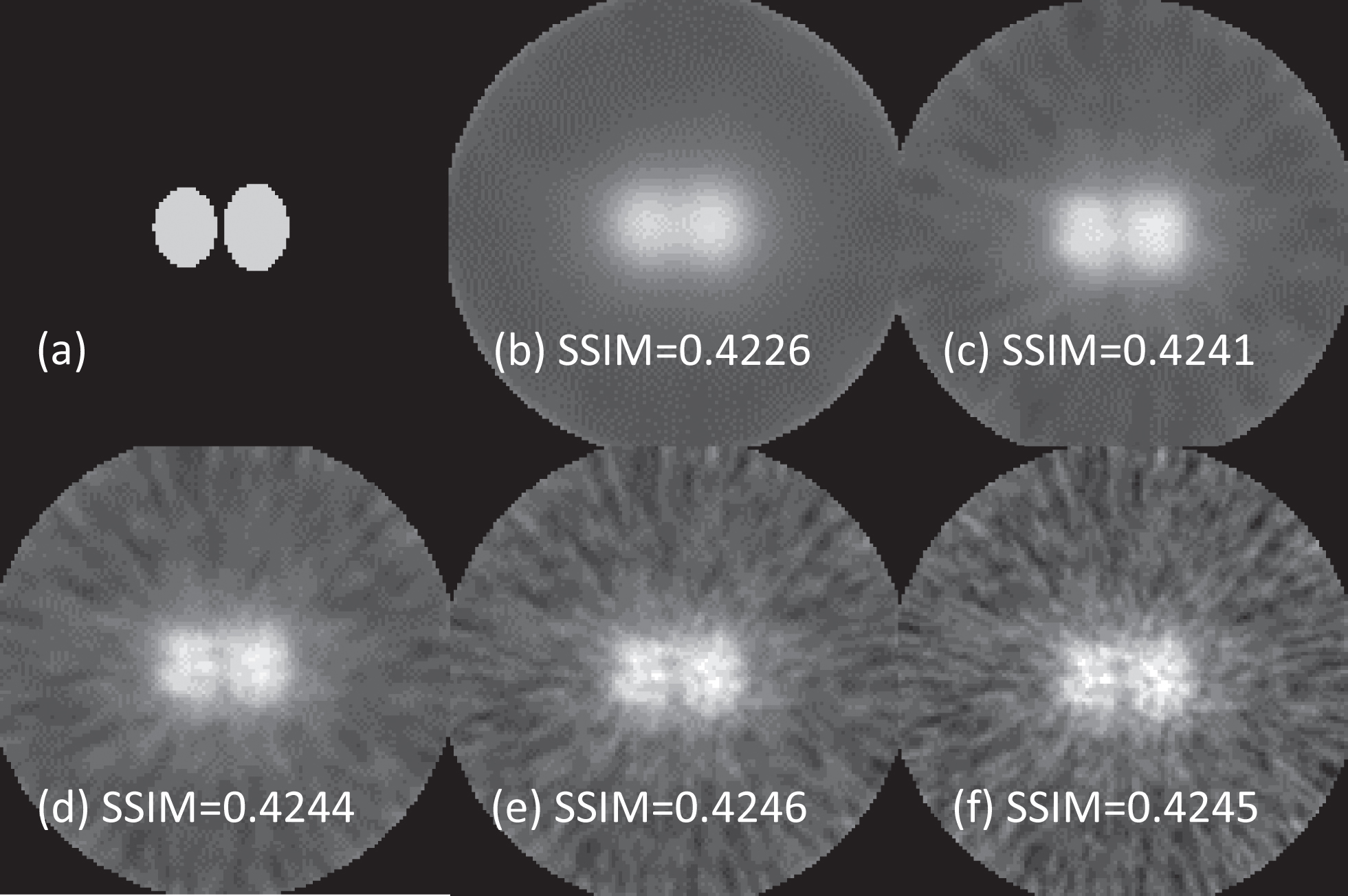
Same as Fig. 8 but for transaxial view.
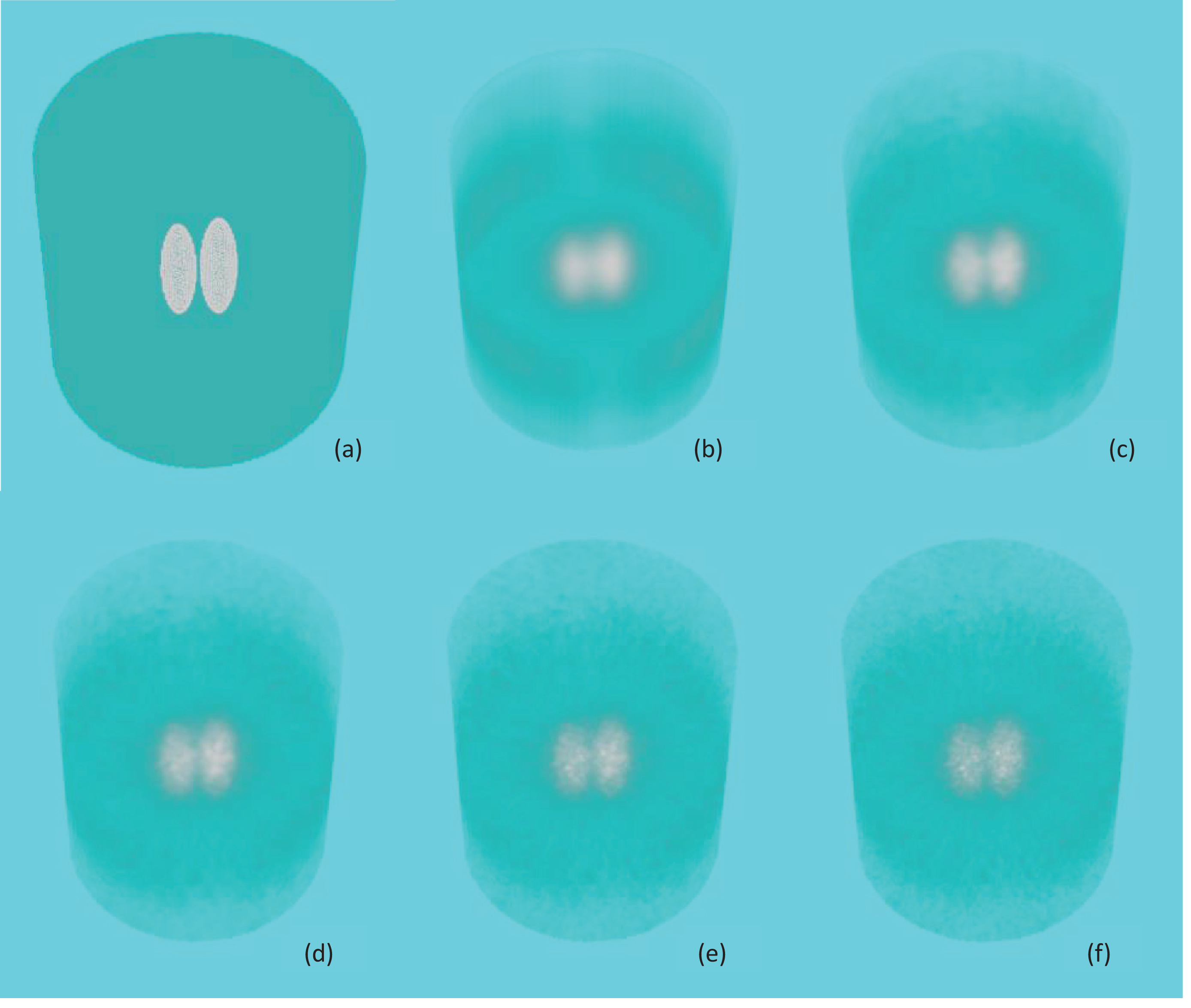
Same as Fig. 8 but the 3D rendings of the whole volumetric images using the maximum intensity projection.
As a general rule, for the tomographic imaging system development, the first step is to numerically investigate the feasibility of the system design. It is not cost-effective to directly build such a system and a real phantom. Hence, in this paper, we numerically investigate the feasibility of thyroid cancer imaging using Timepix3 based Compton camera and report our preliminary results. At the moment, we cannot build a real system and perform physical experiment due to lack of funding but the simulation results are solid, based on established imaging physics and reconstruction theory. These results provide us evidence and confidence to pursue along this direction. We would like to underline that the numerical simulation approach is well accepted in the tomographic imaging field, and the numerical results are typically inspiring, instead of being misleading.
While the Compton camera can be used for many cancer types, we focus on thyroid cancer for two reasons. First, the current Timepix3-based Compton camera detector is the state-of-the-art but relatively small. It is naturally suitable for imaging a small organ, and the human neck has a perfect size as well. Second, Thyroid cancer is the most common cancer in women 15 to 30 years old, and the second most common cancer after breast cancer in women under 50. The Thyroid tissue is the only organ in the human body to have iodine effectively accumulated. Therefore, as an initial application of the Timepix3-based Compton camera, Thyroid cancer is the best match.
Although the high efficiency of Compton camera for SPECT has been compared with the benchmark Anger system [22], to the best of our knowledge, for the first time 3D volumetric image is reconstructed to target clinical applications with thyroid cancer as an example. The state-of-the-art Timpix3 based Compton camera is simulated and a novel yet fast 3D backprojeciton strategy is developed. Those points are our key contributions.
In our current phantom setting, the thyroid gland regions are modeled as ellipsoids and the neck is assumed homogenous with a uniform photon attenuation coefficient. In the near future, this phantom can be re-designed to reflect 3D neck image volume for higher accuracy. The National Library of Medicine (NLM) Visible Human Project (VHP) created public and detailed 3D representations of the human male and female anatomies [25]. The neck CT volumes can be extracted from both the male and female CT scans, the thyroids can be segmented and labeled, and the Hounsfield unit can be converted to linear attenuation coefficients. Because the effective photon energy for CT images is different from that of SPECT images, the linear attenuation coefficients in the CT images can be mapped to the equivalent values for gamma rays in reference to the databases from the National Institute of Standards and Technology [26]. Meanwhile, the cancer defects can be simulated by changing the radiotracer distributions.
In the current list-mode data generation, the Beer’s law is used to mimic the interactions inside the human body. Previously, we developed a tetrahedron-based inhomogeneous Monte Carlo optical simulator (TIM-OS) [16]. In the TIM-OS algorithm, the photon propagation is guided by a tetrahedral mesh of an object. In the future, we plan to employ this TIM-OS simulator [27] to generate gamma ray Compton scattering signals. The realistic digital phantom can be modeled as a tetrahedron-based inhomogeneous finite-element mesh. The linear attenuation coefficients will be mapped to the tetrahedrons in the phantom. An important new component is to include the Compton camera. After a gamma ray arrives at the Compton camera, a simulation procedure will be triggered to capture Compton scattering. We will incorporate the implementation of the components in subsection 2.3 into this procedure. Besides, in the absorption layer of the Compton camera, we will also consider the second or higher order scattering.
Currently, a 3D novel backprojection and ramp filter are used to reconstruct the original radiotracer distributions. It has been proved that the iterative reconstruction formula for maximum-likelihood expectation-maximization (ML-EM) hold in the list-mode case [28, 29], in which each detected event can be considered to be a unique detector unit. In the near future, we can follow the framework in [19] to implement the ML-EM algorithm for better image quality with more computational cost. The results from backprojection method can be used to initialize the ML-EM image for fast convergence. Besides, we can also introduce the sparsity of the radiotracer distributions to constraint the solutions (e.g. total variation minimization, advanced dictionary based sparse representation [30]).
Deep learning based tomographic imaging is an important application of artificial intelligence and a new frontier of machine learning. In 2016, we published the first perspective on this direction [31]. Until recently, most reconstruction approaches could be classified as analytic reconstruction and iterative reconstruction. Iterative reconstruction has been most widely used in SPECT. Recently, a third type of reconstruction was conceived: data-driven, learning-based or deep tomographic reconstruction. This new approach has become the mainstream in the imaging field. Rather than totally relying on an accurate mathematical or physics model, it is empowered by big data with which a deep network can be trained for superior tomographic reconstruction. In the near future, another direction is to employ deep learning based techniques for Compton scattering based SPECT reconstruction of radiotracer distribution in the thyroid.
In summary, comparing with the conventional gamma camera for SPECT imaging, the Compton camera does not have the heavy collimator which implies a higher photon detection efficiency. In this preliminary study, we investigate the feasibility of Compton camera for radiotracer SPECT imaging in thyroid cancer. Our numerical simulation results shows that Compton camera can improve the photon detection efficiency for at least two orders of magnitude with respect to the gamma camera, and the thyroid gland regions can be reconstructed from the Compton camera measurements in terms of radiotracer distribution. This makes the Compton-camera-based SPECT imaging a promising direction for clinical applications with huge benefits for dose reduction, scattering artifact reduction, temporal resolution enhancement, scan throughput increment, and so on.
Footnotes
Acknowledgments
The authors are grateful to Dr. Wenxiang Cong in Rensselaer Polytechnic Institute for constructive discussions.