
Abstract
PURPOSE:
To further investigate the clinical significance of transient ischemic dilation (TID) on myocardial perfusion imaging (MPI) by analyzing the effect of anisodamine hydrobromide (a drug that can effectively ameliorate microcirculation) on the patients with isolated TID and the findings of previous literatures.
METHODS:
Total 107 patients with isolated TID (TID value≥1.11) were randomly divided into group A (n = 36; intravenous administration of anisodamine hydrobromide), group N (n = 36; intravenous administration of isosorbide dinitrate), and group C (n = 35; intravenous administration of normal saline). MPI and treadmill exercise test (TET) were performed again after 14-day course of intervention. Pre- and post-intervention frequencies of symptom were recorded.
RESULTS:
In group A, after intervention of anisodamine hydrobromide, the summed stress score (SSS) and TID value on MPI significantly decreased than those before intervention (P < 0.001), the durations of exercise (DEs) and metabolic equivalents (METs) in TET notably ascended (P < 0.001), as well as the symptom remarkably improved. In group N and group C, there were no significant differences in SSS, TID value, DEs, METs, and frequencies of symptom between pre- and post-intervention (P > 0.05). No significant improvement of symptoms in group N before and after treatment.
CONCLUSIONS:
TID with perfusion defect may usually predict a possibility of severe and extensive coronary artery disease (CAD). An isolated TID should be considered as a likelihood of coronary microvascular dysfunction (CMD). TET and coronary CT angiography (cCTA) are extremely helpful for the antidiastole on CAD and CMD. The administration of anisodamine hydrobromide might be an optional treatment for the patients with isolated TID.
Keywords
Introduction
Over the past 20 years, single photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) has evolved into a powerful multifaceted tool for the evaluation of coronary artery disease (CAD). Transient ischemic dilation (TID) of the left ventricle on MPI defined as an apparent presence of left ventricular enlargement on post-stress compared to rest images, which was initially described by Stolzenberg in 1980 on planar stress-redistribution thallium scans [1]. The transient ischemic dilation (TID) ratio derived from static stress/rest MPS and gated stress/rest MPS on the end-diastolic and the end-systolic phases. The threshold of TID ratio defining high risk of severe CAD varied from 1.12 to 1.38. Greater than 1.12 were reported to this TID cutoff value (1.12) was 80%sensitive and 92%specific for critical 3-vessel CAD [1]. The exact pathophysiologic mechanism is not entirely clear. A generally accepted explanation for this phenomenon is global subendocardial ischemia at stress [2–4]. In the presence of extensive coronary artery disease (CAD), epicardial perfusion pressure is reduced at stress, whereas left ventricular enddiastolic pressure is elevated, resulting in subendocardial hypoperfusion and ischemia. At this condition, the uptake of radiotracer in the subendocardial region is markedly reduced, resulting in a thinner appearance of the LV wall and larger inner ventricular cavity compared to baseline condition [5]. Another possible mechanism which has been suggested is the presence of myocardial stunning as a cause of left ventricular enlargement after stress-induced ischemia [6, 7]. However, the significance of TID is still controversial.
Currently, most previous literatures have validated TID as a marker of severe and extensive CAD and as a predictor of cardiovascular events [8–11]. In the clinical setting, TID is used as an adjunctive marker to perfusion findings, supporting the diagnosis of obstructive CAD. However, the current meta-analysis evaluated the TID ratio as an isolated parameter, without consideration of perfusion findings. Using a CZT camera, Jameria el al.14 demonstrated that TID ratio could be used as adjunctive marker to perfusion deficit, and is most effective among patients with ejection fraction ≥50%[10]. Moreover, the combination of either severe perfusion deficit (≥10%) or mild perfusion deficit (3%–10%)+elevated TID ratio (≥1.19) was associated with higher sensitivity for extensive CAD compared to perfusion deficit ≥10%alone. Thus, increased TID ratio associated with mild perfusion deficit might suggest more extensive CAD than observed by perfusion findings. Data on the diagnostic value of abnormal TID ratio in an otherwise normal MPI is controversial. Nevertheless, some other studies found that the phenomenon of TID also occurred in the patients with otherwise normal MPI images and even in those without significant stenosis (lumen diameter narrowing <50%) at coronary CT angiography (cCTA), and then supposed that TID in such patients did not increase the likelihood of CAD, its extent or severity, and the risk for future major adverse cardiac events [12, 13]. Therefore, some researchers stated that it would not be appropriate to perform invasive coronary angiography (CAG) on the basis of such isolated TID [14].
In an effort to further investigate the underlying mechanism and clinical significance of TID, especially in the patients without myocardial perfusion defects and significant coronary stenoses, in this study, we tried to apply anisodamine hydrobromide, a drug which can effectively ameliorate microcirculation including coronary microvasculature [15–17], to the patients with isolated TID and then analyzed the therapeutic response combined with the findings of previous literatures.
Patients and methods
Patients and study design
From April 2013 to March 2017, a total of 2485 consecutive patients who complained of recurrent chest tightness were preliminary enrolled. Among these patients, those with previously known cardiovascular history such as coronary artery disease, congestive heart failure, various arrhythmia, pacemaker implantation, uncontrolled hypertension (systolic blood pressure (SBP) ≥160 mmHg and/or diastolic blood pressure (DBP) ≥100 mmHg), rheumatic heart disease, valvular heart disease, congenital heart disease, pulmonary embolism, cor pulmonale, myocarditis, cardiomyopathy, and pericardial disease were excluded. Meanwhile, the patients with cerebrovascular disorders, glaucoma, myasthenia gravis, prostatic hyperplasia, bronchial asthma, pulmonary and pleural diseases, chronic renal insufficiency, severe liver dysfunction, malignant tumour, obstructive gastrointestinal disorders, febrile disorders, acute infection, and a history of allergic reaction to contrast medium for CT scanning were also excluded, yielding 593 patients. Then, these patients should undergo cCTA, SPECT MPI and treadmill exercise test (TET) within 1 week of one another. Those with coronary stenosis (lumen diameter narrowing ≥25%) at cCTA, myocardial perfusion defect (summed stress score (SSS) ≥4) on MPI and positive results in TET, as well as those without TID were further excluded, ultimately resulting in 107 patients who had isolated TID (Fig. 1).
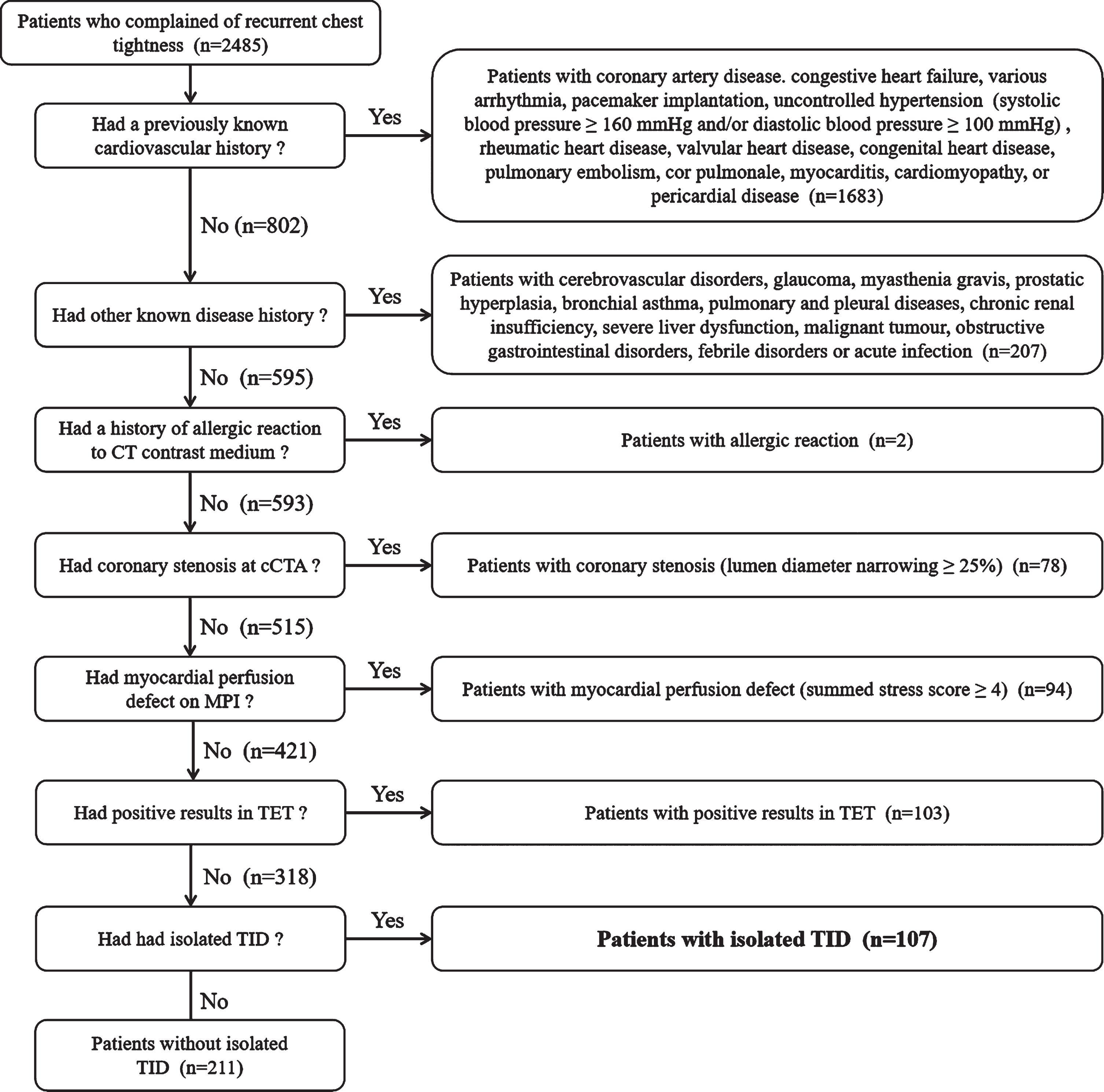
The exclusion steps flow diagram of patients with isolated TID.
Next, all patients with isolated TID were divided into anisodamine hydrobromide group (group A, n = 36), nitrate group (group N, n = 36), and control group (group C, n = 35) with a single-blind randomized controlled method. In group A, a treatment of intravenous infusion of anisodamine hydrobromide (1.0 ml: 10 mg; Chengdu NO.1 Pharmaceutical Co., Ltd, Chengdu, China), diluted with sterile normal saline to 50 mL, was administered at a dose of 0.5 mg/kg. In group N, isosorbide dinitrate (ISDN) injection (10 ml: 10 mg; UCB Pharma Co., Ltd, Zhuhai, China), also diluted with normal saline to 50 mL, was administered at the same dose as that of anisodamine hydrobromide in group A. And in group C, only 50 mL of sterile normal saline was administered as a placebo. All the medicine interventions were carried out at an equal rate of 5 mL/h by micro-infusion pumps for a total of 14 days. Throughout the whole course of treatment, all patients in 3 groups were not aware of any details about the specific drugs they used. When the 14-day medicine intervention was over, each of the 107 patients would undergo a reexamination of SPECT MPI as well as TET. Meanwhile, the pre- and post-intervention frequencies of chest tightness in such patients were recorded, respectively. The study protocol was approved by the ethics committee of Shanghai Chest Hospital, China. All patients signed written informed consent before the study.
All CT examinations were performed by using a 64-slice spiral CT scanner (Brilliance CT 64, Philips Healthcare, Cleveland, USA) with a retrospectively electrocardiogram (ECG)-gated protocol. Before scanning, all patients enrolled were well trained for the breath hold and given sublingual nitroglycerin routinely. Meanwhile, β-blockers were administered in patients with heart rate (HR) >70 beats per minute (bpm). A contrast-enhanced scan was performed with intravenous injection of a bolus of 50–80 mL iopromide (Ultravist 370 mgI/mL, Bayer Schering Pharma, Berlin, Germany) at an injection rate of 5 mL/s followed by a 50 mL saline chaser bolus. The scan range was from the mid pulmonary artery to below the heart with a cranio-caudal direction. Scanning was automatically triggered by the bolus tracking technique included in the scanner. The region of interest (ROI) was placed within the ascending aorta and the triggering threshold was 100 HU. The scanning parameters were as follows: a slice collimation of 64×0.625 mm, a tube voltage of 120 to 140 kV depending on body mass index (BMI), a tube current of 800 to 1000 mAs, a pitch of 0.2, and a gantry rotation time of 0.42 s.
Images of the best diastolic phase and the best systolic phase were automatically reconstructed by using the retrospective ECG gate and the optimal cardiac phase that displayed the minimal motion artifacts. The effective section thickness was 0.67 mm and the reconstruction increment was 0.6 mm.
All the images were independently interpreted by two cardiovascular radiologists who had at least 5 years of experience with cCTA imaging and who were blinded to the patients’ history. Any discordant case was resolved by consensus. Transverse sections and automatically generated curved multiplanar reformations were available for assessing the degree of coronary stenosis. In accordance with the Society of Cardiovascular Computed Tomography (SCCT) guidelines [18], an 18-segment coronary artery model was used, and the coronary stenoses were graded as negative (<25%) and positive (≥25%). And in this study, the patients with positive stenosis would be excluded.
Myocardial perfusion imaging
MPI acquisition and processing were performed with a single-day dobutamine stress and rest technetium –99 m-sestamibi ( 99 mTc-MIBI) ECG-gated SPECT MPI protocol. Any vasodilator and β-blocker should be discontinued for 48 h before examination. Dobutamine (2 ml: 20 mg; Shanghai First Biochemical Pharmaceutical Co. Ltd., Shanghai, China) was infused via intravenous bolus in 3 min dose increments at 5, 10, 15, 20, 25, 30, 35, and 40μg/kg/min with continuous monitoring of symptoms, BP, HR, and 12-lead ECG. Up to 1.0mg of atropine was administered intravenously if the target HR (85%of maximum age- and gender-predicted HR, MPHR) was not achieved at the peak dose of dobutamine. The test endpoints were defined as achievement of target HR or HR ≥130 bpm, serious arrhythmia, horizontal or downsloping ST-segment depression of ≥0.1 mV at an interval of 80 ms after the J-point compared with the baseline measurement, new-onset ST-segment elevation of ≥0.05 mV, severe angina, SBP decrease ≥20 mmHg compared with the baseline measurement, or BP >230/115 mmHg [19, 20].
A dose of 370 MBq of 99 mTc-MIBI (radiochemical purity >95%, Shanghai Xinke Pharmaceutical Co., Ltd, Shanghai, China) was injected intravenously 1–2 min before the termination of dobutamine test for stress imaging, and 4 h later, 1110 MBq of 99 mTc-MIBI was injected for rest imaging. All images were acquired 1–1.5 hours after each injection of 99 mTc-MIBI using a Discovery NM/CT 670 (GE Healthcare, Waukesha, USA). ECG-gated SPECT acquisition was performed in step-and-shoot mode with a 20%acceptance window at 140keV, a 64×64 matrix, and 16-frame fixed temporal resolution forward-backward gating per R-R interval. Thirty projections (60 seconds per projection) were obtained in a 180° semicircular arc extending from the 45° right anterior oblique to the 45° left posterior oblique position. Data were processed on a Xeleris workstation (GE Healthcare, Waukesha, USA). Images were reconstructed by using an iterative ordered-subsets expectation maximization (OSEM) algorithm and were analyzed by using Emory Cardiac Toolbox (ECToolbox) software package (Emory University, Atlanta, USA). A quantitative TID ratio was automatically derived from the gated SPECT images by using Quantitative Gated SPECT (QGS) software (Cedars-Sinai Medical Center, Los Angeles, USA).
All SPECT images were interpreted by a consensus of two experienced nuclear physicians without prior knowledge of the patients’ clinical data. The left ventricle was divided into 17 standard segments according to the statement of American Heart Association [21]. All segments were scored for regional perfusion by using a 5-point scale (0 = normal, 1 = equivocal or mild, 2 = moderate, 3 = severe reduction of radiotracer uptake, 4 = absence of radiotracer uptake). SSS was obtained by adding all the scores of the 17 segments in the image at stress. Images were considered normal perfusion if the SSS was <4. So far there was still a lack of a definitive threshold of TID ratio which varied with different stresses and imaging protocols [15]. In this study, a cutoff value of ≥1.11 which was the minimum cutoff derived from previous literatures was considered to represent TID.
Treadmill exercise test
TET was performed with T2100 Stress Treadmill (GE Healthcare, Waukesha, USA) using the standard Bruce protocol [22, 23]. Continuous ECG monitoring was applied throughout the test. 12-lead ECG and BP were recorded at rest and then every 3 minutes during exercise and recovery. Whenever any abnormality occurred, both ECG and BP should be recorded immediately.
The endpoints of TET included achievement of 85%of age-adjusted MPHR for ≥2 min, a horizontal or downsloping ST-segment depression of ≥0.1 mV in at least 2 adjacent leads, severe arrhythmia (frequent multiform ventricular premature contractions, ventricular bigeminy, ventricular tachycardia, second or third degree atrioventricular block, new bundle branch block, intraventricular conduction delay induced by exercise and other hemodynamically compromised arrhythmia), BP >230/115 mmHg, SBP decrease ≥20 mmHg or DBP decrease ≥10 mmHg compared with the baseline measurement, moderate to severe angina, signs of poor perfusion (cyanosis or pallor), physical exhaustion or any other disabling symptom (ataxia, dizziness or dyspnoea), and the patient’s request to stop. The test was also discontinued if no abnormal signs and symptoms were presented but the patient’s HR exceeded 95%of the age-adjusted limit. The patients should be observed for at least 6 minutes in supine or sitting position for recovery after the exercise was terminated. The recovery phase was terminated if no ST-segment changes were present or exercise-evoked ST-segment changes disappeared during this time, and/or the HR slowed to <100 bpm.
A positive TET was defined as follows [24, 25]: (a) a horizontal or downsloping ST-segment depression of ≥0.1 mV, or upsloping depression of ≥0.2 mV, compared with the baseline measurement, at an interval of 80ms after the J-point for ≥2 minutes in at least 2 adjacent leads, (b) a ST-segment elevation of ≥0.2 mV (20 ms after the J-point) for ≥1 minute in at least 2 continuous leads, (c) an SBP decrease of ≥10 mmHg compared with the baseline measurement, (d) a typical symptom of angina pectoris. The exercise tolerance of each patient with negative TET which was expressed as durations of exercise (DEs) and metabolic equivalents (METs) would be recorded.
Symptoms evaluation
Frequencies of the attack of chest tightness 4 weeks before enrollment and then 4 weeks after medicine intervention in the 107 patients were recorded and then were divided into 4 grades: class I, <1 time/week; class II, 1–3 times/week; class III, ≥4 times/week, but <1 time/day; class IV, ≥1 time/day. The evaluation criteria of chest tightness were self-report of the patient and pathological changes were found by emergency ECG, and the symptoms of chest tightness caused by physiological or psychological factors were excluded.
Statistical analysis
All statistical analyses were performed using SAS 9.13 software (SAS institute Inc., Cary, North Carolina, USA). Continuous variables were presented as mean±standard deviation (SD), and categorical variables were presented as numbers and percentages. A P value <0.05 was considered statistically significant.
A General linear model (GLM) test was used to analyze the differences of age and body mass index in baseline characteristics, SSS and TID Values in MPI, and DEs and METs in TET among the 3 groups. Between pre- and post-intervention in each group, a Student’s t test was used to determine the differences of such variables in MPI and TET.
The baseline characteristics including gender, numbers of the patients with current smoking, hypertension, hyperlipidemia, or diabetes mellitus, and the ones who needed long-term uses of medications among the 3 groups were analyzed by Pearson χ2 test. A CMH-χ2 (Cochran-Mantel-Haenszel) test was done to compare the frequencies of chest tightness before and after intervention.
Results
Patient characteristics
According to our research, the phenomenon of TID can occur not only in the patients with obstructive CAD, but also in those with CMD (Table 1). Among the overall 2485 patients enrolled, there were 107 patients who had isolated TID, which was defined in this study as the presence of TID with otherwise normal MPI images and no significant coronary stenoses at cCTA as well as negative results in TET. The baseline characteristics of the patients with isolated TID are summarized in Table 2. No statistically significant differences in gender, age, BMI, risk factors (smoking, hypertension, hyperlipidemia, diabetes mellitus) were found among the 3 groups (P > 0.05). Some of the patients needed long-term uses of medications such as angiotensin-converting enzyme inhibitors (ACEI), angiotensin receptor blockers (ARB), calcium channel blockers (CCB) for the treatment of hypertension, and statins for dyslipidemia. There were also no significant differences in the basic medication use among the 3 groups (P > 0.05).
Numbers of patients with CAD, CMD and elevated TID in 2485 Patients
Numbers of patients with CAD, CMD and elevated TID in 2485 Patients
Baseline characteristics of patients with isolated TID
Data are expressed as mean±SD or as number (%). BMI, body mass index; ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; CCB, calcium channel blockers.
The baseline SSS in MPI before medicine intervention in group A, group N, and group C were 2.1±0.9, 2.0±0.9, and 1.9±1.1, respectively. There were no significant differences among the 3 groups (P = 0.730). Then in group A, the post-intervention SSS was 0.8±0.7, which was significantly lower than pre-intervention (P < 0.001). However, in group N and group C, the post-intervention SSS were 1.6±0.8 and 1.7±1.0, and no significant differences were found between pre- and post-intervention (P = 0.124 and 0.657, respectively) (Fig. 2).
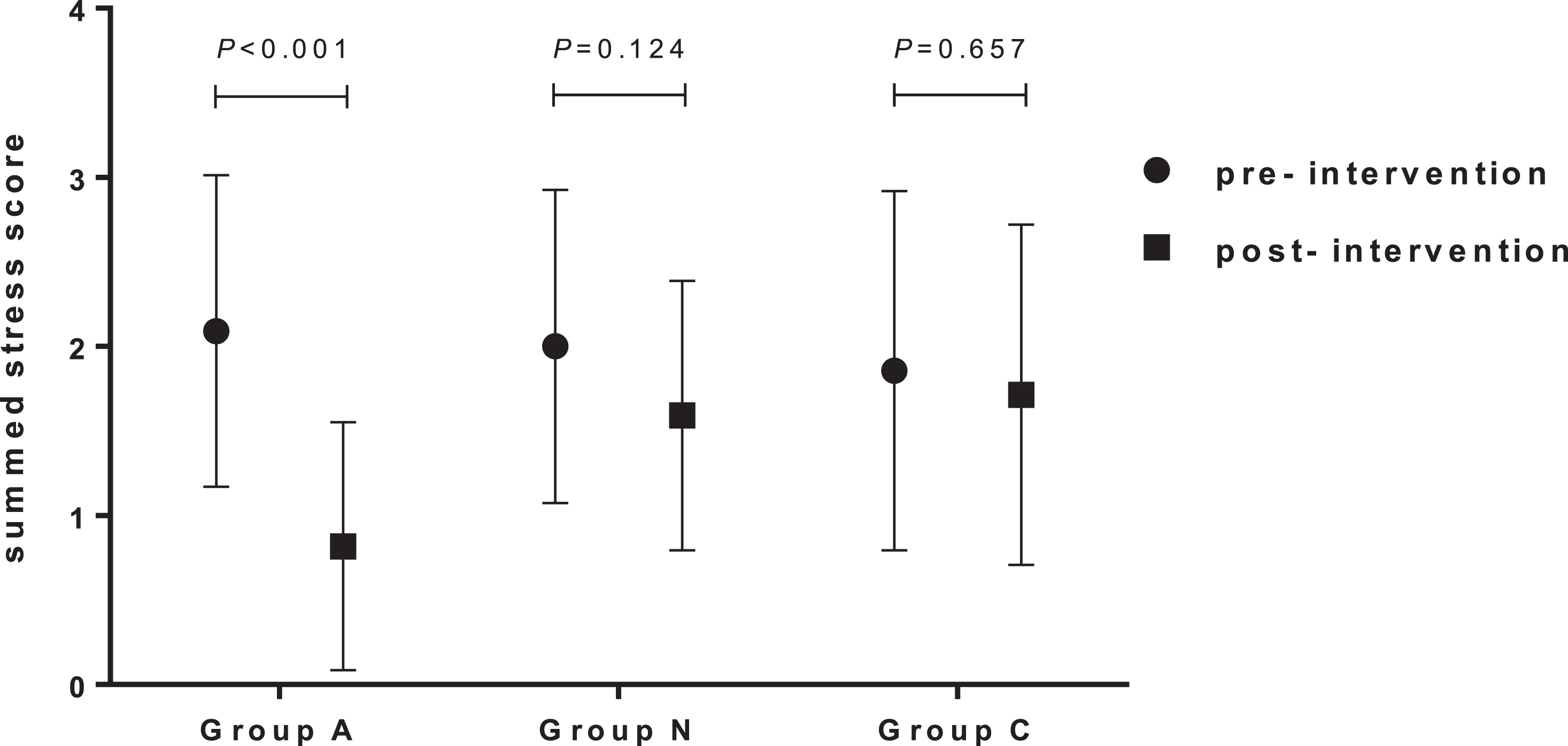
Comparisons of SSS in MPI between pre- and post-intervention among 3 groups.
Meanwhile, the baseline TID value before intervention in group A, group N, and group C were 1.27±0.09, 1.26±0.09 and 1.24±0.10, respectively. There were no significant differences among the 3 groups (P = 0.632). In group A, the post-intervention TID value (1.07±0.07) significantly decreased than pre-intervention (P < 0.001). In group N, although the post-intervention TID value (1.25±0.08) showed slight decreases than baseline, there was no significant difference (P = 0.566). Then in group C, the TID value (1.24±0.10) almost unchanged after intervention (P = 0.989) (Fig. 3, 4).
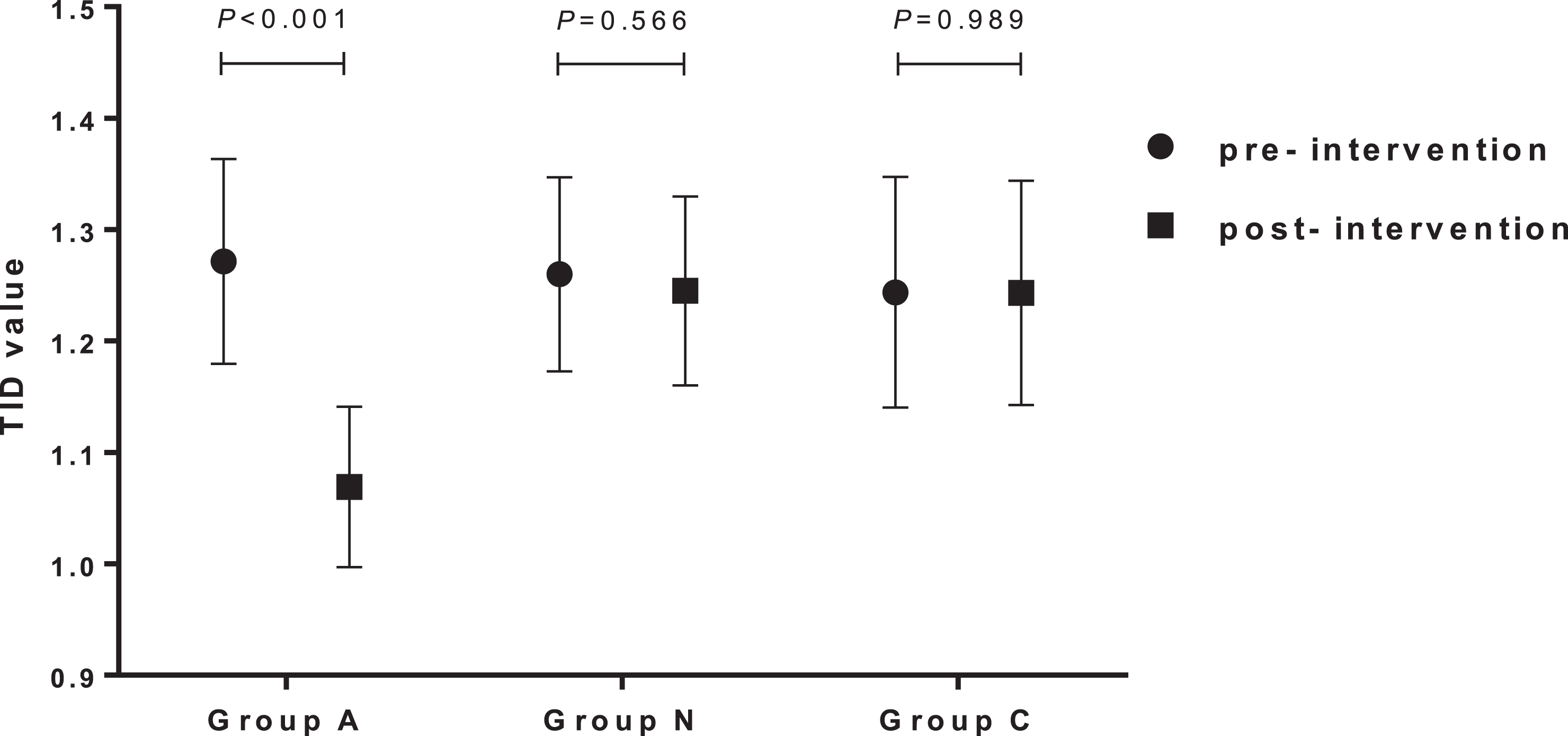
Comparisons of TID values in MPI between pre- and post-intervention among 3 groups.
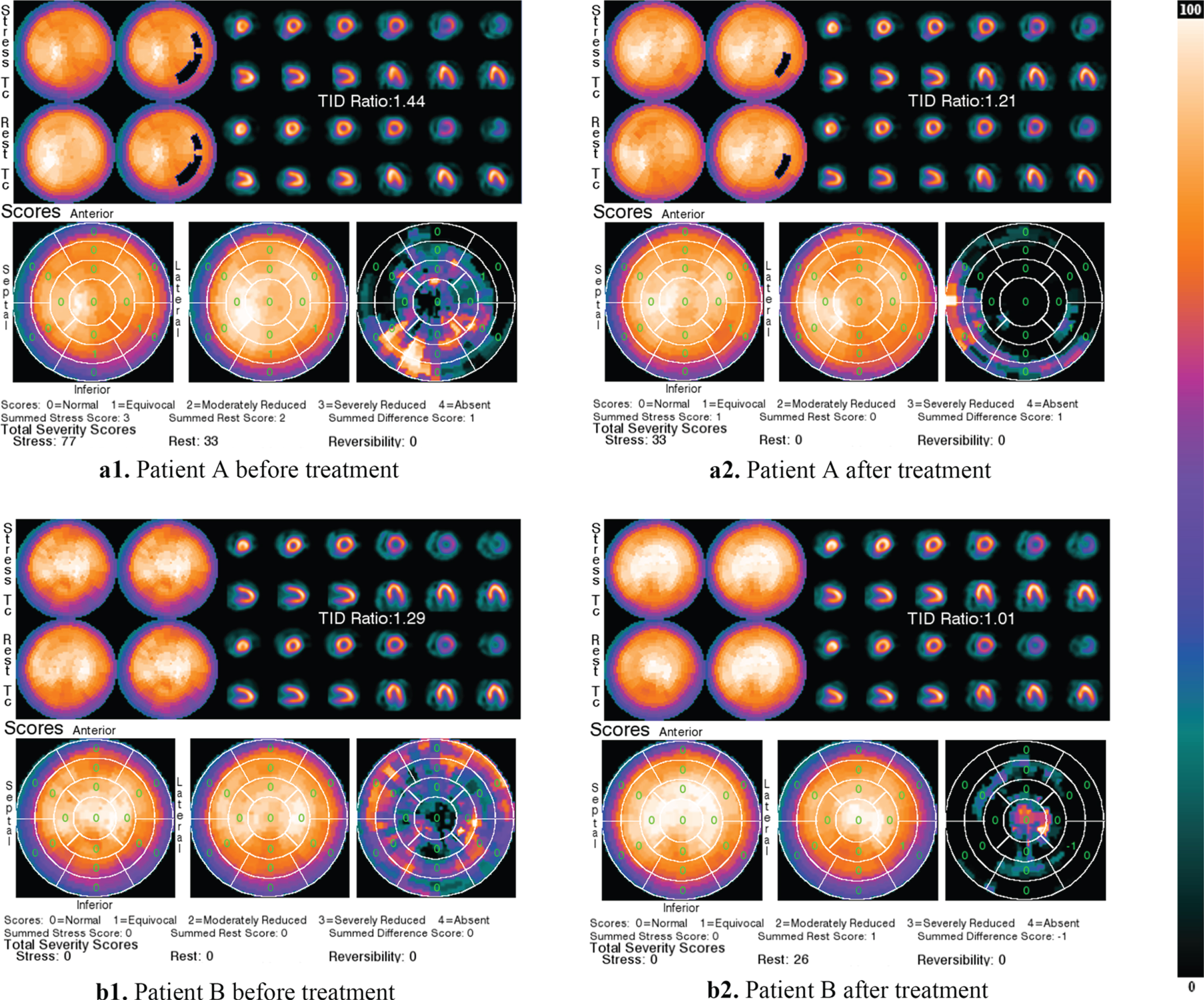
MPI images of two patients with isolated TID but no evidence of CAD who complained of recurrent chest tightness in group A. The SSS and TID value of patient A were 1 and 1.21 after treatment of anisodamine hydrobromide compared with 3 and 1.44 before treatment. Patient B had the same SSS of 0 before and after treatment, with TID value of 1.01 after treatment compared with 1.29 before treatment.
All the 107 patients were determined to be negative in TET. The pre-intervention DEs were 6.5±1.0, 6.8±0.9 and 6.6±0.9 minutes in group A, group N and group C, respectively, with no significant differences among the 3 groups (P = 0.436). After medicine intervention, the patients in group A presented significantly longer DEs (7.9±0.8 minutes) than pre-intervention (P < 0.001), while those in group N and group C presented no significant differences in DEs (7.0±0.8 and 6.5±1.0 minutes, respectively) compared with pre-intervention (P = 0.398 and 0.537, respectively) (Fig. 5).
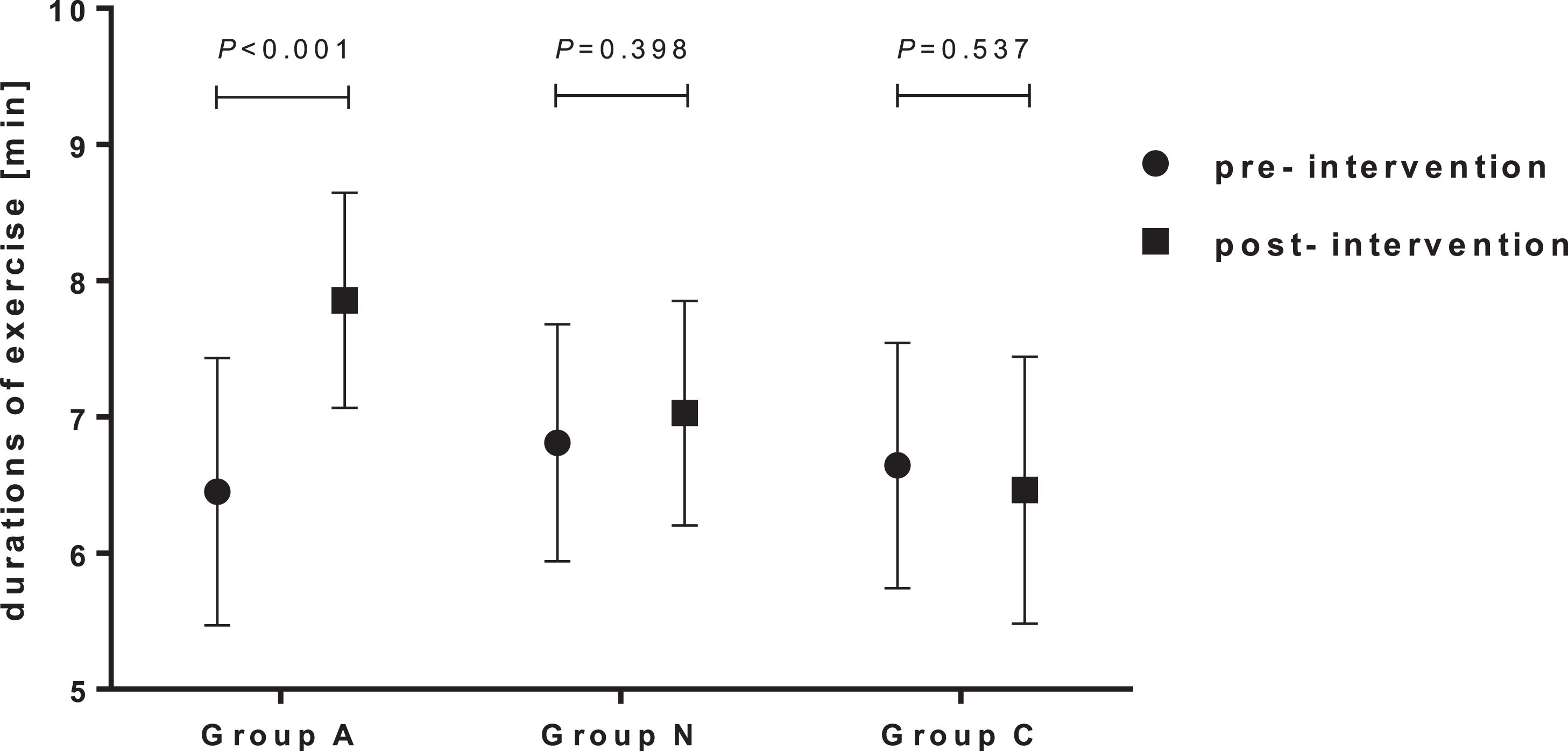
Comparisons of DEs in TET between pre- and post-intervention among 3 groups.
Likewise, the pre-intervention METs did not differ among the 3 groups (7.2±0.8, 7.5±0.7 and 7.4±0.7, P = 0.414). The post-intervention METs in group A (8.2±0.5) notably ascended than pre-intervention (P < 0.001). However, neither the post-intervention METs in group N (7.7±0.6) nor that in group C (7.2±0.8) significantly differed from pre-intervention (P = 0.386 and 0.486, respectively) (Fig. 6).
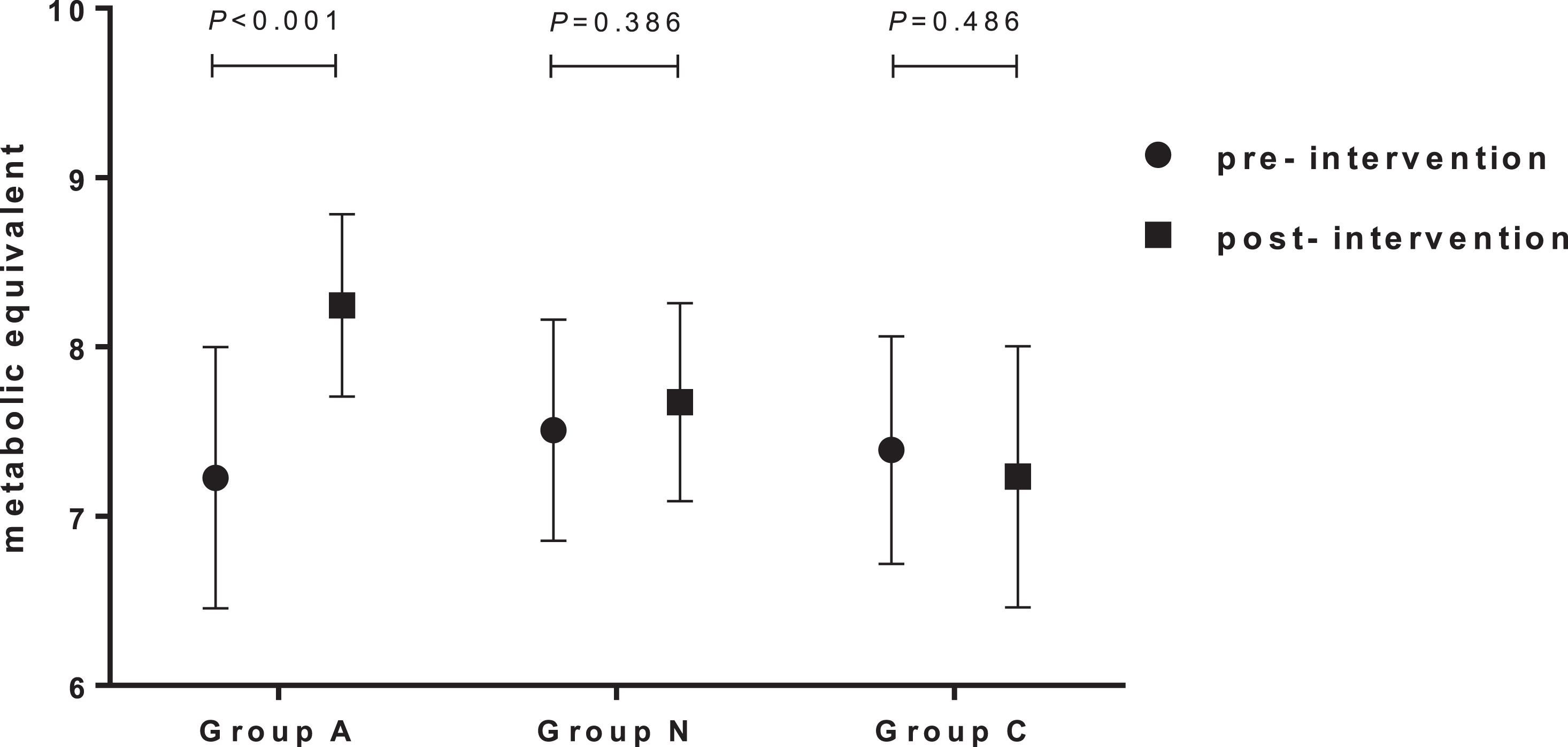
Comparisons of METs in TET between pre- and post-intervention among 3 groups.
According to the classification criteria for the frequency of chest tightness mentioned above, before enrollment, in group A, 1 (2.8%) patient was in class I, 8 (22.2%) were in class II, and 15 (41.7%) in class II, 12 (33.3%) in class IV, compared with 2 (5.5%) in class I, 9 (25.0%) in class II, 15 (41.7%) in class III, 10 (27.8%) in class IV in group N, as well as none in class I, 5 (14.3%) in class II, 17 (48.6%) in class III, 13 (37.1%) in class IV in group C (P = 0.262). While after intervention, there were 6 (16.7%) patients in class I, 22 (61.1%) in class II, 3 (8.3%) in class III, and 5 (13.9%) in class IV in group A, in which there was significant difference between pre- and post-intervention (P < 0.001). However, there were 3 (8.3%) patients in class I, 12 (33.4%) in class II, 13 (36.1%) in class III, 8 (22.2%) in class IV in group N, and 1 (2.9%) in class I, 6 (17.1%) in class II, 14 (40.0%) in class III, 14 (40.0%) in class IV in group C after intervention. No significant differences in the frequencies of chest tightness were found in group N and group C (P = 0.356 and 0.751, respectively) between pre- and post-intervention, although the symptoms of a small number of patients in group N slightly improved.
Briefly, after corresponding intervention, the symptoms improved remarkably in group A, but slightly in group N as well as hardly in group C (Fig. 7).
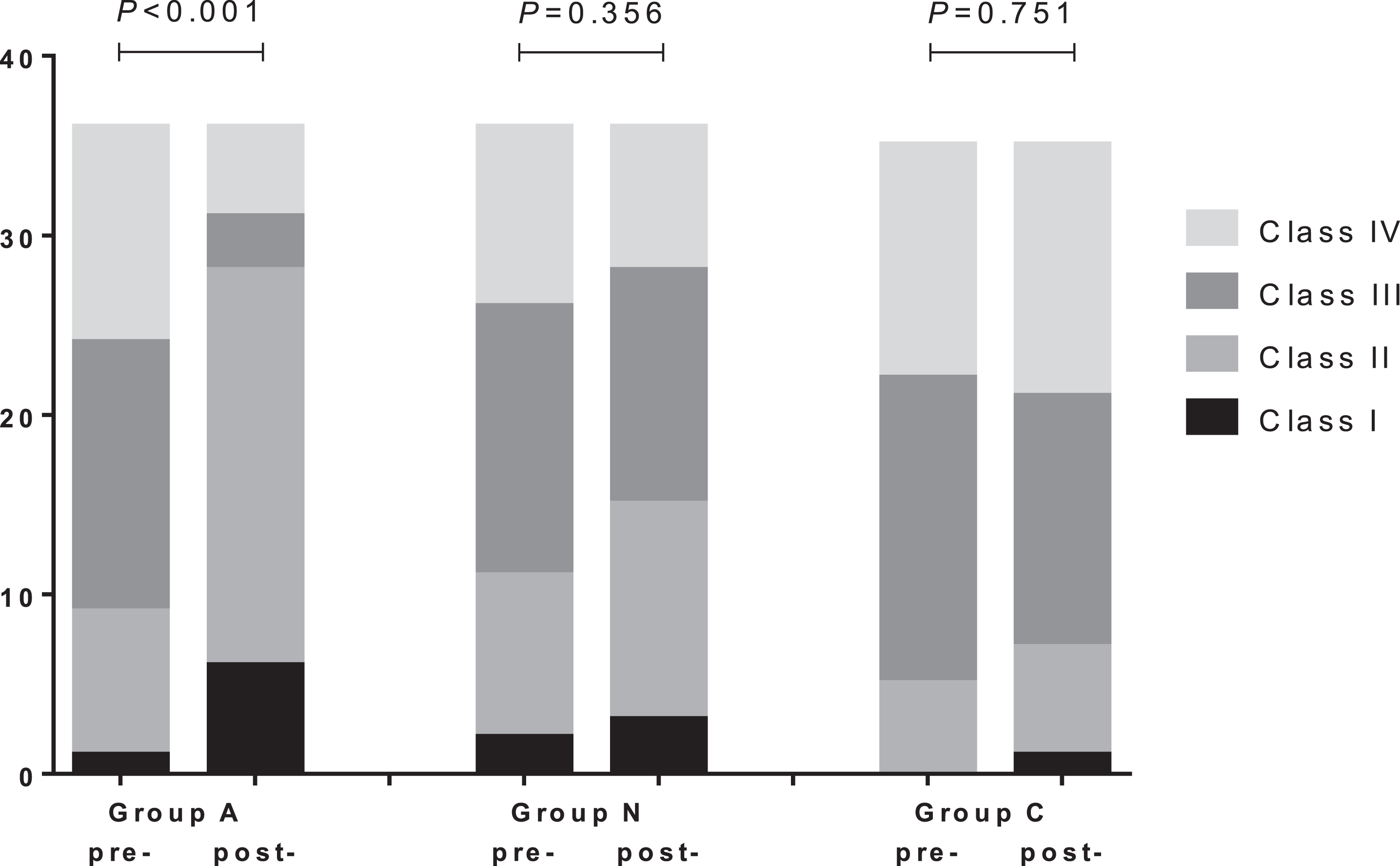
Comparisons of the frequency of chest tightness between pre- and post-intervention among 3 groups.
Currently, there are substantial numbers of patients who are suffering from recurrent attacks of chest tightness but almost no positive results with clinical significance have been found in many related inspections such as TET, even cCTA or CAG. Such patients were often diagnosed as cardiac neurosis (CN) and were usually informed that no treatment was necessary. What’s worse, some of these patients had been treated for a long time with the regimen specially for CAD. Nevertheless, the symptom of chest tightness did not ameliorate. Consequently, such patients not only have suffered from chest discomfort, but also should endure the mental stress and the damage of inappropriate treatment.
In the present study, we observed that the phenomenon of TID with otherwise normal SPECT MPI was not infrequent in the patients with recurrent attacks of chest tightness. By the performance of cCTA, we could identify the existence and then the degree of stenosis in epicardial coronary arteries. The TET then could not only reveal the presence of myocardial ischemia under certain exercise loads but also evaluate the patients’ exercise tolerance and cardial reserve. Furthermore, the performance of SPECT MPI could validate the abnormalities of myocardial perfusion and assess the extent of myocardial ischemia. Therefore, with the comprehensive application of above non-invasive inspections, we could effectively exclude the obstructive epicardial CAD.
Anisodamine hydrobromide is a belladonna alkaloid which was isolated from the Chinese medicinal herb Scopolia tangutica Maxim for the first time in 1965 [26]. Though as a non-subtype-selective muscarinic cholinergic antagonist, since 1980s, anisodamine hydrobromide has been proved to have many properties of a noncholinergic antagonist, such as relieving microvascular spasm, inhibiting calcium overload, antioxidation and scavenging superoxide, inhibiting platelet aggregation and thromboxane synthesis, depressing microthrombosis, suppressing inflammation, and improving vascular endothelium function [15, 27]. Thus, it has been widely used in the treatment of microcirculatory disorders such as disseminated intravascular coagulation (DIC) and septic shock [28, 29], and it can also provide significant cardioprotection against myocardial ischemia/reperfusion injury [16]. In recent years, it has been tried by intracoronary administration while undergoing percutaneous coronary intervention (PCI) to improve coronary no-reflow which is mainly caused by disordered coronary microcirculation [17].
Excitedly, in this study, after the treatment of anisodamine hydrobromide, the SSS and TID value in MPI of the patients with recurrent attacks of chest tightness but no evidence of obstructive epicardial CAD showed a significant decrease, though the baseline SSS was less than 4 which was considered normal perfusion. Meanwhile, there was a remarkable improvement in symptom and exercise tolerance of such patients after treatment. Accordingly, we extrapolate that anisodamine hydrobromide may be effective in the treatment for TID by improving coronary microcirculation.
As we know, ISDN is a non-endothelium dependent exogenous nitric oxide (NO) dono [30], and has been widely used in the treatment for ischemic heart disease based on the vasodilative effect on the epicardial coronary arteries [31]. Nevertheless, on account of the lack of sulfhydryl pools, which are necessary for the biotransformation of nitrates [32], the coronary microvasculature has been proved to present a poor vasodilation response to ISDN [33]. Coincidentally, in this study, administration of ISDN was hardly effective for the patients with isolated TID.
So far, several mechanisms have been described to explain the finding of TID, in which the commonly accepted one is extensive subendocardial ischemia. Overall, we are fully in favor of this prevailing viewpoint based on a great number of previous studies. However, we hold that the specific significance of TID should be identified under different conditions. As is known to us, the factors that cause myocardial ischemia include not only the stenosis or obstruction of coronary artery, but also the abnormality of coronary microvasculature, which is now usually referred to as coronary microvascular dysfunction (CMD) [34]. Accordingly, theoretically, the phenomenon of TID can occur not only in the presence of obstructive CAD, but in the presence of CMD.
As discussed above, the presence of TID in the patients with myocardial perfusion defects on MPI should be considered as a high risk for severe and extensive CAD [8–11]. Meanwhile, the presence of TID with otherwise normal MPI may also indicate a significant likelihood of balanced ischemia from multivessel CAD [14, 35]. On the other hand, several studies found that the phenomenon of TID with otherwise normal MPI could also occur in the absence of CAD [12–14]. Furthermore, there are a few reports of TID found in the patients with hypertension, hypertrophic cardiomyopathy and diabetes mellitus [13, 37], which are closely associate with relative or absolute abnormalities in coronary microvasculature. In our study, all the 107 patients with isolated TID were considered no evidence of obstructive epicardial CAD by the performance of cCTA and TET. However, the symptom of chest tightness in such patients frequently occurred and then significantly ameliorated with the decrease of TID value by the treatment of anisodamine hydrobromide rather than ISDN. Thus, it is reasonable to believe that the presence of TID may be closely related to CMD especially in the patients who have been excluded from CAD.
There are several limitations to this study. First, this study was limited by the small sample size of patients (n = 107) with TID but otherwise normal MPI who suffered from recurrent chest tightness. Additional large-scale multicenter studies are necessary to confirm our findings. Then, because no technique currently allows the direct visualization of coronary microvasculature in vivo in humans, the relation between TID and CMD in this study was concluded from the therapeutic effect of anisodamine hydrobromide, the exclusion of CAD, as well as the relevant findings of previous researches. Such indirect methods as transthoracic Doppler echocardiography, myocardial contrast echocardiography, cardiac magnetic resonance imaging or intracoronary Doppler flow velocity wires [34] might be performed in further studies. In addition, we are not sure whether there is an optimal threshold of TID ratio to identify CAD or CMD in the examination of myocardial perfusion scintigraphy. But all the same, an more important aim of this study is to throw some light on this subject. More basic and clinical researches are expected for a better understanding of the significance of TID.
Conclusions
The phenomenon of TID can occur not only in the patients with obstructive CAD, but also in those with CMD. The presence of TID with perfusion abnormalities on MPI may usually predict a high possibility of severe and extensive CAD. However, the presence of TID with otherwise normal MPI should be considered as a significant likelihood of CMD. Such non-invasive examinations as cCTA and TET are extremely helpful for the antidiastole on CAD and CMD. For those with isolated TID who have no adequate evidence of CAD, it is not appropriate to be ignored without any treatment, nor to be incorrectly treated with the method specially for CAD. The administration of anisodamine hydrobromide might be an optional treatment for the patients with TID, especially for those excluded from CAD.