
Abstract
OBJECTIVE:
To investigate relationship between the diffusion indexes of corticospinal tract (CST) and the neurological motor outcomes in chronic pontine stroke patients.
METHODS:
Diffusion tensor imaging (DTI) is performed in 27 patients with chronic pontine stroke. Fractional anisotropy (FA) values along the CST area, the track number, and the CST length are measured. Neurological and motor outcomes are evaluated based on Fugl-meyer (FM), National Institutes of Health Stroke Scale (NIHSS), Barthel index (BI), and modified Rankin scale (mRS) scores. The relationships between FA ratios (rFAs) in the CST of stroke subjects and their clinical motor scores are analyzed through Spearman’s correlation analysis. Then, diffusion tensor tractography (DTT) is performed to show the injury degree of CST.
RESULTS:
First, FA values are decreased in the infarct area, cerebral peduncle, posterior limb of the internal capsule, and precentral gyrus compared with those in the contralateral side. The number of CST is decreased in the ipsilateral side of the infarct. Second, rFAs in the cerebral peduncle, posterior limb of the internal capsule, and CST rnum correlate positively with FM scores (r = 0.824, 0.672, 0.651, p < 0.001) and negatively with mRS scores (r = –0.835, –0.604, –0.645, p≤0.001). Third, the injury degree of CST correlates negatively with FM scores (r = –0.627, p < 0.001).
CONCLUSIONS:
The study demonstrates that rFAs in the cerebral peduncle, posterior limb of the internal capsule, and CST rnum associate with motor outcome, suggesting that DTI may be applicable for outcome evaluation.
Introduction
Strokes are a major cause of death, with ischemic strokes accounting for 87% of all strokes [1]. Posterior circulation strokes may lead to high disability and mortality [2]. Pontine strokes make up 3% of first ischemic strokes and 10% –15% of posterior circulation strokes [3]. Epidemiological studies investigating particularly chronic pontine stroke are lacking. While pontine stroke is relatively common, they generally occur as a part of larger posterior circulation stroke. Studies examining chronic pontine stroke exclusively are lacking. The main clinical manifestations of pontine strokes include limb inactivity, central facial and lingual paralysis, sensory disturbances, speech ambiguity, and vertigo [4]. Clinical presentation of pontine stroke can vary, but it is primarily determined by the anatomical boundaries of the infarcted region within the pons and the blood vessels involved. It’s difficult to distinguish pontine stroke from other ischemic strokes just according to clinical presentation. Initial neuroimaging would aid in evaluating intracranial pathologies. Most surviving stroke patients have functional disorders. No single outcome measure can describe or predict all dimensions of recovery and disability after stroke. Clinicians often use neurological and motor functional scales in evaluations of stroke-related outcomes. The standard neurological and motor assessment of stroke patients, the National Institutes of Health Stroke Scale (NIHSS), Fugl-meyer (FM), Barthel index (BI), and modified Rankin scale (mRS) are weighted significantly towards motor and sensory function [5–7]. However, some scales are not objective, with the findings may be influenced by patients or doctors [8].
In this study, we mainly used Magnetic resonance imaging (MRI) to detect pontine stroke patients. MRI is playing an important role not only in identifying stroke lesions, but also in delineating the relationship between lesions and brain anatomical and functional changes. Noninvasive MRI biomarkers may provide insight regarding specific neural events underlying stroke recovery. Besides, these biomarkers may identify patients who may benefit from specific rehabilitative interventions [9].
Diffusion tensor imaging (DTI), a noninvasive MRI technique, measures the random motion of water molecules and provides information on cellular integrity and pathology. Pathological processes that change the microstructural environment (e.g., neuronal size, extracellular space, and tissue integrity) result in altered diffusion. DTI is one of the most widely used MRI methods to investigate white matter integrity in vivo. DTI allows quantitative analysis of fiber pathways and the anatomy of axonal fiber bundles, and it can identify disease-specific alterations of fiber tracts [10]. This type of imaging allows for visualization and quantitative examination of fiber tracts and their integrity in vivo [11, 12]. In this way, the topographic relation of the lesion location and corticospinal fibers can be evaluated [13]. DTI can identify and estimate neural tracts at the subcortical level [14]. In recent decades, DTI has been widely applied in studies on brain tumors, epilepsy, depression, Alzheimer’s disease, and several other brain diseases [15, 16]. However, most previous research on DTI has focused on the blood supply area in the middle cerebral artery [17–19], and knowledge on motor recovery mechanisms in patients with pontine strokes is limited.
The corticospinal tract (CST) is the major neuronal pathway that mediates voluntary movements and is the most important motor pathway for predicting motor outcome in stroke patients [20]. Diffusion tensor tractography (DTT) is a method that produces the reconstruction and estimation of CST structure (or integrity) in the live human brain, which is derived from DTI. However, DTI can’t provide information how white matter fibers connect between adjacent voxels. With the development of computer software, people use the data obtained by DTI to reconstruct the white matter fibers in the brain, which is called DTT. DTT is the further development of DTI technology. DTT can identify the special fiber pathways and their connections in the brain. As a result, injury of the CST after stroke could be estimated three dimensionally using DTT. Several studies have demonstrated that DTT is helpful for predicting motor outcome in stroke patients [21, 22].
In this study, we used DTI and DTT to explore the correlations between diffusion indexes of the pontine infarct and areas distal to the infarct and clinical, neurological, and motor outcomes. We also investigated the relationship between the degree of injury of the CST and motor outcome.
Materials and methods
Subjects
This prospective study was approved by the ethics committee of Zhongda Hospital, Southeast University of China, and all participants provided written informed consent. The study group consisted of 27 chronic pontine stroke patients who were diagnosed between December 2016 and July 2018.
The inclusion criteria were as follows: (1) aged between 45 and 75 years old; (2) a single infarct confined to the pons identified via MR imaging, first onset; (3) post-stroke time of 6–24 mo from the acute stroke phase; (4) right handed; (5) mild dysfunction after the stroke (Fugl–Meyer [FM] ≥80, Barthel index [BI] ≥90); and (6) no history of severe physical or neurological disability. The exclusion criteria were as follows: (1) severe or unstable disease, such as intracranial tumors; (2) other neuropsychiatric disorders, such as depression; (3) severe white matter degeneration; (4) contraindications to MR imaging; (5) lesions outside the pons or extensive infarcts involving the midbrain or medulla; and (6) recurrence of infarctions or secondary hemorrhages.
Neurological and motor scale assessments
Clinical data included hypertension, diabetes, hyperlipemia, and other risk factors. FM, NIHSS, BI, and mRS scores were measured to analyze each patient’s neurological deficit, motor deficit, and independence. Two resident physicians of neurology administered all the scales the same day as an MR examination. The final score was the average of all the scores.
MR imaging protocol
For the MR imaging protocol, a 3.0-T MR imager (Magentom Trio Tim; Siemens, Erlangen, Germany) and standard head coil were used. Each subject lay flat on the scanning bed in the supine position. The subject’s head was fixed with sponge pads to reduce movement, and earplugs were worn to reduce scanning noise. The 3D T1-weighted imaging protocol was as follows: TR 1,900 ms, TE 2.48 ms, 176 slices, 1 mm thickness, 0 mm interval, 90° flip angle, 256×256 acquisition matrix, 250×250 mm field of view; fast spin-echo T2-weighted imaging (TR 6,000 ms, TE 95 ms), fluid attenuation inversion recovery (TR 8,500 ms, TE 94 ms), and diffusion-weighted imaging (TR 10,000 ms, TE 95 ms, 70 slices, 2 mm thickness, 0 mm interval, NEX 2, 128×128 acquisition matrix, 220×220 mm field of view, 30 diffusion directions with a b-value of b = 1,000 s/mm2 and one with a value of 0 s/mm2).
MR data processing
DTI and DTT data postprocessing
The DTI raw data were encoded in DICOM format and input into a personal computer. Open-source software TrackVis and its Diffusion Toolkit software (Wang R, Wedeen VJ, Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Boston, MA) was used for image processing. Several regions of interest (ROIs) were selected, and DTT technology was used to reconstruct bilateral corticospinal tract. We input raw data in Diffusion Toolkit software and set two ROIs. Each ROI (a sphere with a radius of 4.0 mm, symmetrical on both sides) was drawn on color-coded fractional anisotropy (FA) images. ROI1 was the posterior limb of the internal capsule, and ROI2 was the lower pons. Only fibers that passed through ROI1 and ROI2 were displayed and defined as the CST. Two resident physicians of radiology drew each ROI. To evaluate the reproducible or the inter-observer variability, 15 cases were randomly selected and two resident physicians drew the ROIs at the same regions independently. Interclass correlation coefficient (ICC) was used to measure the inter-observer reliability by comparing two physicians’ measurements of the FA values of these regions. Cronbach’s alpha above 0.75 indicated excellent reliability. Finally, we found all the measurements met the acquirement. The thresholds for tracking termination were 0.2 for FA and 35° for the angle. Then it could generate a track file from DTI raw data. We input the track file in TrackVis [23] software to get the DTT images.
The FA values for the infarct and unaffected sides were calculated. The FA values for the cerebral peduncle, posterior limb of the internal capsule, and precentral gyrus, in addition to the number and length of the CST on the bilateral side, were also measured. The FA ratio (rFA) was calculated of the ipsilesional (FAips) to contralesional (FAcon) side as rFA = FAips/FAcon. The CST rnum was calculated as follows: CSTnumips/CSTnumcon, where CST rnum denoted the ratio of CST number of the ipsilesional to contralesional side, CSTnumips denoted the CST number of the ipsilesional side and CSTnumcon denoted the CST number of the contralesional side. CST rlen = CSTlenips/CSTlencon, where CST rlen denoted the ratio of CST length of the ipsilesional to contralesional side, CSTlenips denoted the CST length of the ipsilesional side and CSTlencon denoted the CST length of the contralesional side.
The spatial relationship between each pontine infarct and the CST was evaluated using the DTT images in three-dimensional space. The degree of CST involvement and injury was also evaluated directly through DTT images. Observe whether the CST was inside the pontine infarct, or be compressed, curved, disrupted.
Measurement of infarct volume
Two resident physicians of radiology used ImageJ software (NIH, Bethesda, Maryland) to measure the infarct volume in fluid-attenuated inversion recovery (FLAIR) images (Fig. 1). FLAIR images can inhibit hyperintense cerebrospinal fluid and show the hyperintense or hypointense infarct lesions in this study. FLAIR belongs to inversion recovery (IR) sequence. Abnormal hyperintense or hypointense voxels were labeled manually in native image space. The whole lesion volumes were determined by summation across all relevant slices. We take the average of two physicians’ measurements. In this way, we can reduce the influence of human factors and random error, making our measurements more reliable. To evaluate the inter-reader agreement, 15 cases were randomly selected and two resident physicians measured the infarct volume in FLAIR images independently. Interclass correlation coefficient (ICC) was used to measure the inter-reader reliability by comparing two physicians’ measurements of the infarct volume. Cronbach’s alpha above 0.75 indicated excellent reliability. Finally, we found all the measurements met the acquirement.
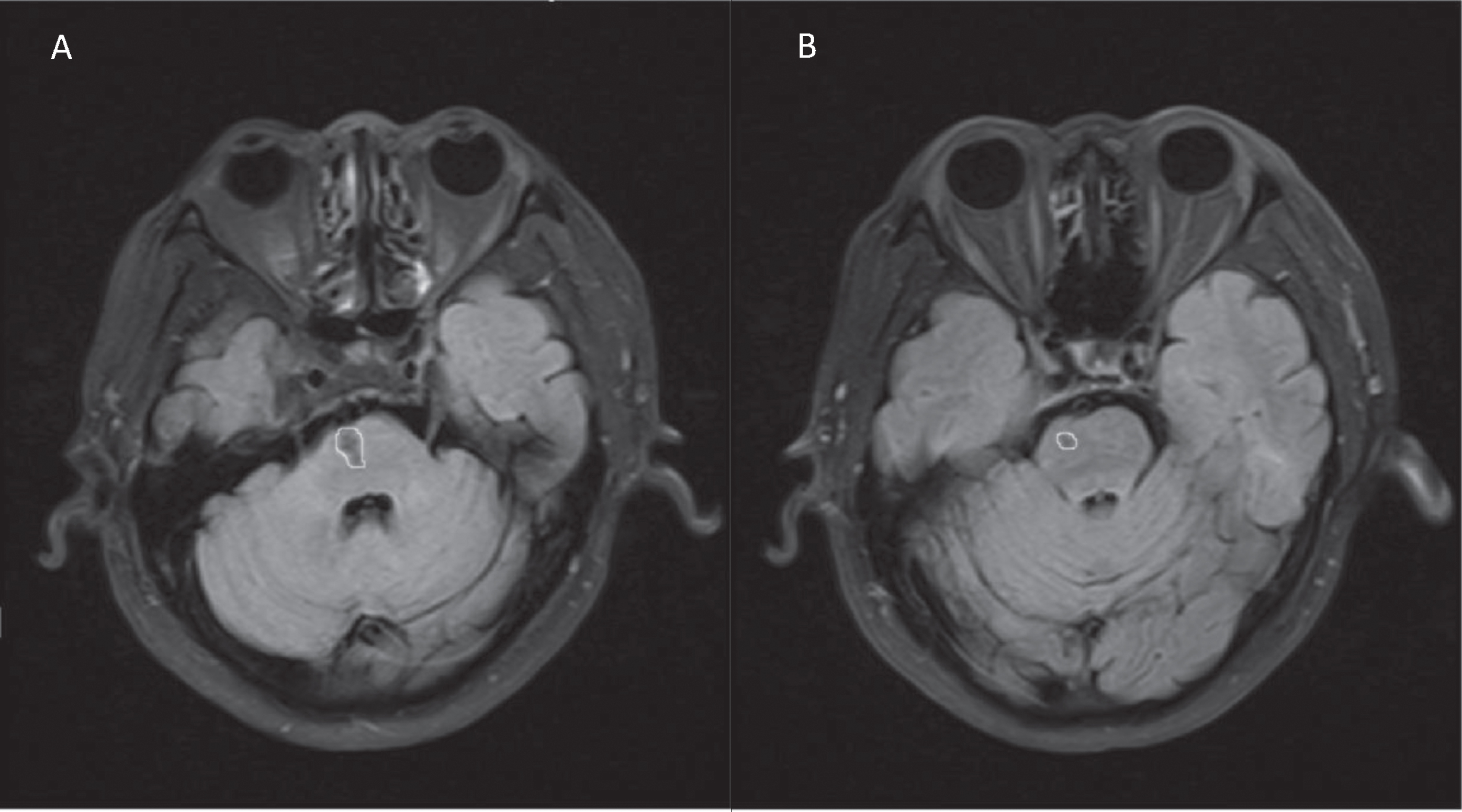
Example of detected and segmented infarct regions on fluid-attenuated inversion recovery images. The infarct lesions were labeled manually with yellow circles. The whole lesion volumes were the summation of A (66.199) and B (16.463). In this case, the whole lesion volumes were 82.662 mm3.
Statistical analysis was performed using SPSS 19.0 for Windows software. All values are presented as mean±standard deviation. FA values for the ipsilateral and contralateral sides of the infarct; FA values for the bilateral side of the cerebral peduncle, posterior limb of the internal capsule, and precentral gyrus; and the number and length of the CST in the bilateral side of the stroke patients were compared using a paired-sample t-test. Spearman’s correlation analysis was applied to rFA, CST rnum, CST rlen, infarct volume data and motor outcome data. Spearman correlation’s analysis was also used to investigate the relationship between the classification of the degree of CST injury and FM scores. A p-value of 0.05 (two tailed) was considered to indicate a significant difference in all statistical procedures.
Results
Clinical data and neurological and motor function assessments
The clinical data about the sex, age, and other risk factors on the stroke patients were listed (Table 1). The stroke patients had mild functional defects (FM: 80–100, median: 96; NIHSS: 0–2, median: 0; BI: 95–100 m, median: 100 mRS: 0–3, median: Next, 12 stroke patients had infarcts on the left side of the pons, and 15 stroke patients had infarcts on the right side of the pons. The average volume of infarcts was 68.18 mm3, ranging from 9.58 to 200.07 mm3.
Demographic and clinical imaging data on the stroke patients
Demographic and clinical imaging data on the stroke patients
When the affected and unaffected sides of the stroke patients were compared, the FA values for the pontine infarcts, cerebral peduncle, posterior limb of the internal capsule, and precentral gyrus, in addition to the number of CST in the affected side, were significantly decreased (p < 0.01). There was no difference in the CST length of the affected and unaffected sides (p > 0.05) (Table 2).
Comparison of diffusion indexes in different areas of the stroke patients
Comparison of diffusion indexes in different areas of the stroke patients
All patients had some degree of motor deficit. The rFA values of the cerebral peduncle, posterior limb of the internal capsule, and CST rnum were correlated positively with FM scores (r = 0.824, p < 0.001; r = 0.672, p < 0.001; and r = 0.651, p < 0.001, respectively) and correlated negatively with mRS scores (r = –0.835, p < 0.001; r = –0.604, p = 0.001; and r = –0.645, p < 0.001, respectively) (Table 3) (Fig. 2). However, the rFA values for the pontine infarct and precentral gyrus exhibited an insignificant correlation with all functional scales. The diffusion indexes of stroke patients showed an insignificant correlation with NIHSS or BI scores (Table 3). Additionally, in this study, no significant correlation existed between the infarct volume and neurological and motor scales in the stroke patients (p > 0.05) (Table 4).
Correlations between diffusion-related ratios and clinical motor outcomes of the stroke patients
Correlations between diffusion-related ratios and clinical motor outcomes of the stroke patients

Correlations between diffusion-related ratios and neurological motor outcomes. In this study, rFAs in the cerebral peduncle, posterior limb of the internal capsule, and CST rnum correlated positively with Fugl-meyer (FM) scores(A, C, E) (r = 0.824, 0.672, 0.651, p < 0.001) and negatively with modified Rankin scale (mRS) scores(B, D, F) (r = –0.835, –0.604, –0.645, p≤0.001).
Correlations between pontine infarct volumes and clinical motor outcomes
We directly determined the spatial relations between the CST and infarct through DTT. The DTT findings were classified into three grades in accordance with the degree of CST involvement. In grade 1 (n = 12), the CST was outside the infarct, without compression. In grade 2 (n = 9), a small portion of the CST was located in the infarct and compressed, curved, or slightly disrupted. In grade 3 (n = 6), the CST was mostly or completely disrupted at the site of the infarct (Fig. 3). The classification of the degree of CST injury correlated negatively with FM scores (r = –0.627, p < 0.001) (Fig. 4).
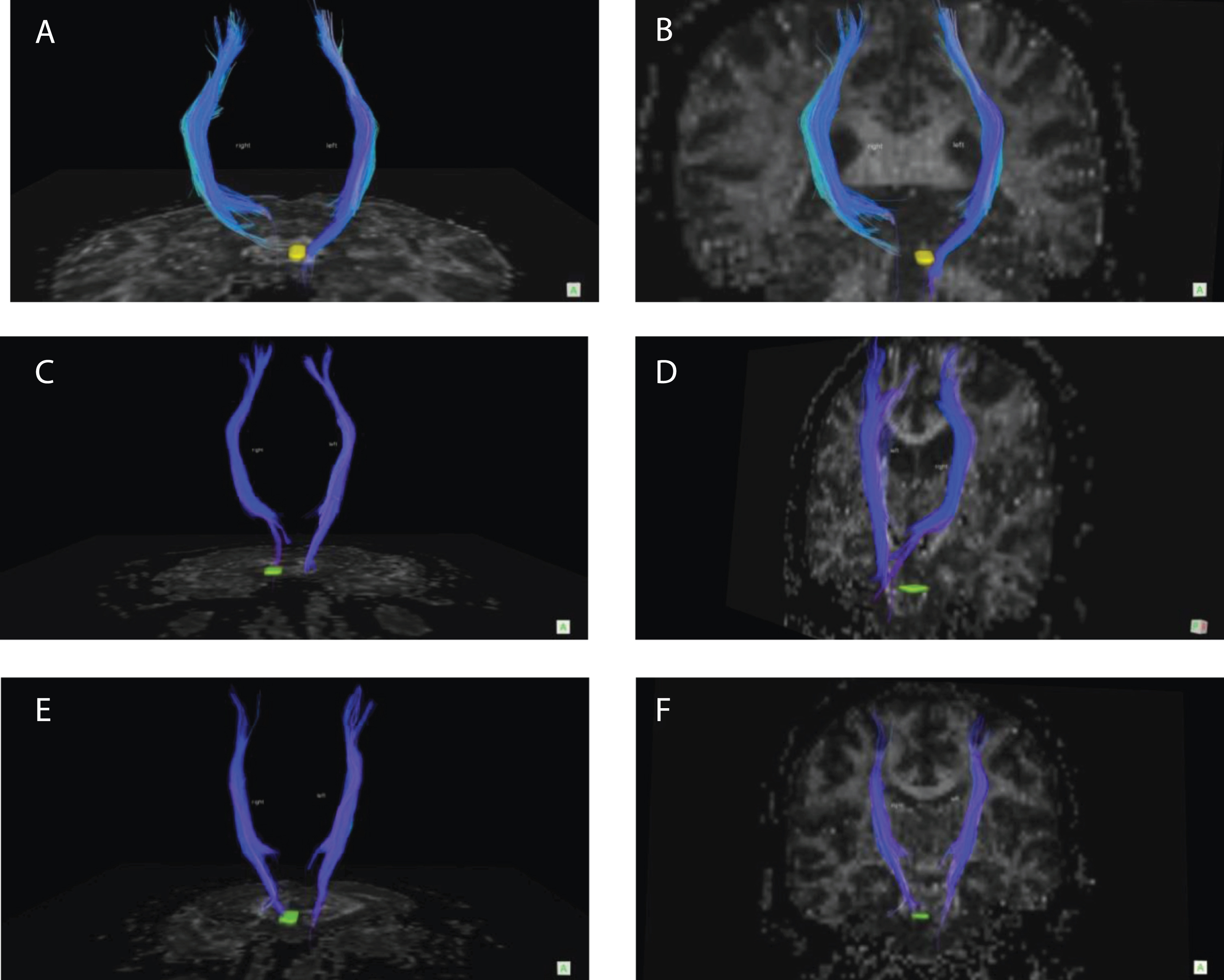
DTT demonstration of three grades of findings classified in accordance with the degree of CST involvement. (A-B) Grade 1, (C-D) grade 2, and (E-F) grade 3.
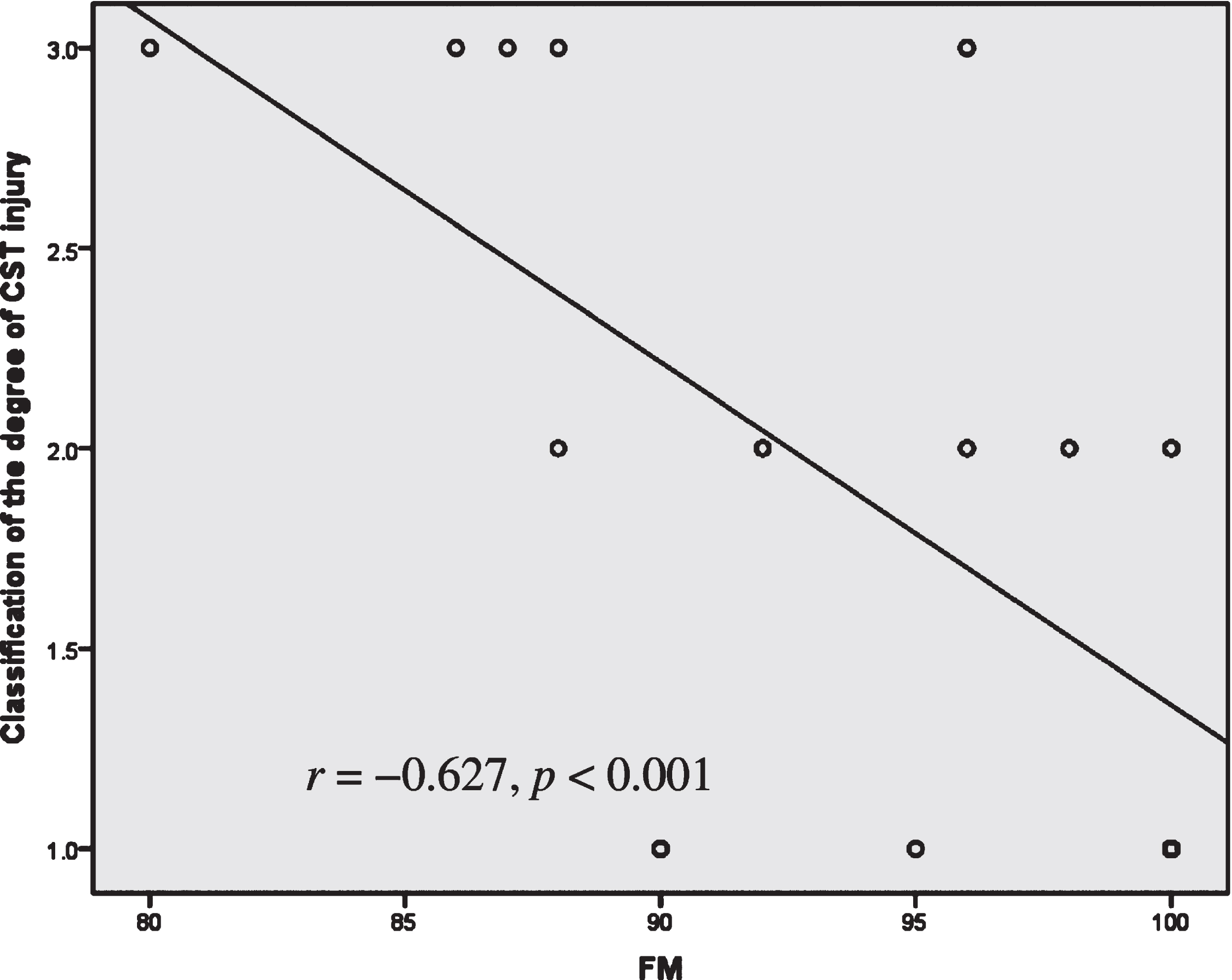
Correlation between the classification of the degree of CST injury and Fugl-meyer (FM) scores. The classification of the degree of CST injury correlated negatively with FM scores (r = –0.627, p < 0.001).
Molecular diffusion can be measured using several indexes derived from DTI data. The FA value is currently the most commonly used measure to quantitatively assess the anisotropic degree of tissues, indicating the proportion of anisotropic components of water molecules. The value ranges from 0 to 1, where 0 denotes that diffusion is unlimited and 1 means maximum anisotropy. The FA value can be used to evaluate the degree of necrosis of fibers after injury of white matter. Lower FA values are associated with nerve fiber dysfunction, pointing to a relatively poor prognosis [24].
After pontine ischemic strokes, the reduction in FA values distal to the infarct are attributed to myelinolysis and impaired structural integrity of the CST due to Wallerian degeneration [25]. Over time, these values gradually return to normal because of glial cell proliferation, myelin degradation, and removal of axonal debris [25]. The neurological repair process involves competition between Wallerian degeneration and self-repair of white matter fibers [26]. Regeneration and repair of injured fibers can slow down or terminate Wallerian degeneration [26]. Therefore, changes in FA values can demonstrate pathophysiological changes in distal infarcts [27, 28]. Previous studies reported that FA values of the ipsilateral side remained lower than those of the contralateral side, even 1 y postinfarction [29]. The finding is in accordance with that found in the present study. Several previous studies indicated that Wallerian degeneration was associated with the size and location of the infarct [30, 31]. According to this idea, an infarct with a small volume may cause only mild nerve fiber damage and be less likely to cause Wallerian degeneration. In our research, we detected no substantial correlation between the infarct volume and motor outcome. In our study, the infarct volume was relatively small and confined to the pons. Thus, the degree of neurological and motor function damage was relatively mild.
In this study, we measured the ratios of diffusion indexes in areas through which the CST passed. These ratios provide an effective and objectively means of evaluating the degree of CST injury. In our study, the rFA values for the cerebral peduncle and posterior limb of the internal capsule and the CST rnum correlated positively with FM scores and negatively with mRS scores. The FM scale evaluates the recovery of motor function in stroke patients, including joint function of upper and lower limbs, balance, and sensation. Previous studies demonstrated that FM scores correlated with some diffusion indexes [24]. The mRS mainly evaluates the degree of disability and dependence. This scale is also an indicator of motor recovery. In the present study, the ratios of diffusion indexes were strongly correlated with both FM and mRS scores, which indicated that diffusion indexes may reflect the recovery of motor function. However, the diffusion indexes of stroke patients showed an insignificant correlation with BI and NIHSS scores. The latter may be explained by the nature of the NIHSS, which provides only an approximate estimation and focuses on the evaluation of nervous system defects. Based on these scales, the prognosis of the patients in the present study was relatively good, with insignificant nervous system damage. The BI focuses on the assessment of daily living capability. Although some patients had mild motor dysfunction, many independent daily activities of living (e.g., eating, dressing, and toileting/continence) were not impaired. The rFA values of pontine infarcts and the precentral gyrus exhibited an insignificant correlation with all functional scales. The former may be explained by the location of the infarct in an area where the CST did not pass through, thereby exerting a minimal influence on motor recovery. The rFA values of the precentral gyrus may be attributed to the following factors: The precentral gyrus locates in the distal end of the pontine infarction, the degree of Wallerian degeneration was slight, and the degree of CST involvement in the precentral gyrus was slight.
DTT three-dimensional imaging can show the spatial relationship between an infarct and the CST and be used to evaluate motor function outcome [32–34]. In our study, there was a substantial correlation between the classification of CST injury and motor function recovery. In the chronic stage of a stroke, the recovery of neurological and motor functions is closely related to the reorganization of brain function. The present study showed that when the CST passed through only the edge of the infarct or was located outside the infarct, patients had improved outcomes, with only slight motor dysfunction. In most patients, minimal edema around the infarct was absorbed in the chronic stage of the stroke, with disappearance of the space-occupying lesion. For some patients whose CST was compressed, curved, or interrupted to some extent, motor function improved in the chronic stage. Possible reasons are a reduction in congestion and edema around the infarct, recovery of nerve fibers that had been compressed, and compensatory effects of unaffected motor fibers around the infarct. When a large part of the CST is interrupted, motor dysfunction may occur. In the present study, some patients with CST interruption exhibited weak muscle strength. The nerve fibers of these patients were severely impaired and thus required a long time for reorganization and regeneration.
In pontine strokes, the spatial relationship between the infarct and fibrous tract is more complex than in the case of supratentorial strokes, and our knowledge of the impact of this relationship on the prognosis of patients is limited. DTI imaging studies of the CST in chronic pontine strokes reflect changes in the way fibers pass through the CST. Thus, the findings provide a reliable reference for clinical rehabilitation treatment and guidance, as well as for the recovery of neurological and motor functions.
The lesions in this study were concentrated in a relatively small area. Thus, the level of CST injury was lower than that observed in cases of extensive brain parenchymal lesions. The concentrated nature of the lesions in the present study also meant it was possible to evaluate CST recovery homogeneously.
Conclusions
In conclusion, rFA values in the cerebral peduncle and posterior limb of the internal capsule and CST rnum values were associated with motor outcome, which suggests that DTI may be applicable to outcome evaluations. DTT can be used to evaluate the degree of involvement of the CST in patients with chronic pontine strokes, which are related to motor outcome.
Footnotes
Appendix
An age- and sex-matched control group of 27 healthy subjects from social society with no history of neurological or psychiatric disorders was recruited to compare DTI-derived measures between the patients and healthy controls. Previous studies reported that motor impairment after a stroke was related to the lesion site and size, as well as to other factors, such as patient’s age or comorbidities [1–3]. All these factors may influence the motor outcome of stroke patients. We used an age- and sex-matched control group (healthy cases) to rule out the effects of some risk factors and comorbidities on motor function recovery, such as hypertension, diabetes, hyperlipidemia, smoke, alcohol. The following table shows that results revealed no difference in the sex, age, or other risk factors in the stroke and control groups (p > 0.05)
Stroke group
Control group
t/χ2
p
(n = 27)
(n = 27)
Demographic and risk factors
Age (y)
60.44±6.73
57.44±6.87
1.621
0.111
Age range (y)
47–72
48–70
—
—
Sex (F/M)
8/19
8/19
0.000
1.000
Hypertension
10 (37.04%)
9 (33.33%)
0.081
0.776
Diabetes
8 (29.63%)
6 (22.22%)
0.386
0.535
Hyperlipidemia
12 (44.44%)
10 (37.04%)
0.307
0.580
Smoke
16 (59.26%)
13 (48.15%)
0.670
0.413
Alcohol
9 (33.33%)
8 (29.63%)
0.086
0.770
[1] S.K. Schiemanck, G. Kwakkel, M.W. Post, et al., Impact of internal capsule lesions on outcome of motor hand function at one year post-stroke, J Rehabil Med
[2] J.M. Hicks, E. Taub, B. Womble, et al., Relation of white matter hyperintensities and motor deficits in chronic stroke, Restor Neurol Neurosci
[3] S.C. Cramer and R.J. Seitz, Imaging functional recovery from stroke, In: Handbook of Clinical Neurology