
Abstract
BACKGROUND:
Energetics alteration plays a crucial role in the myocardial injury process in chronic hypoxia diseases (CHD). 31P magnetic resonance spectroscopy (MRS) can investigate alterations in cardiac energetics in vivo.
OBJECTIVE:
To characterize the potential value of 31P MRS in evaluating cardiac energetics alteration of chronic hypoxic rats (CHRs).
METHODS:
Twenty-four CHRs were induced by SU5416 combined with hypoxia and divided into four groups according to the modeling time of one, two, three and five weeks, respectively. Control group also contains six rats. 31P MRS was performed weekly and the ratio of concentrations of phosphocreatine (PCr) to adenosine triphosphate (ATP) (PCr/ATP) was obtained. In addition, the cardiac structure index and systolic function parameters, including the right ventricular ejection fraction (RVEF), right ventricular end-diastolic volume index (RVEDVi), right ventricular end-systolic volume index (RVESVi), and the left ventricular function parameters, were measured.
RESULTS:
Decreased resting cardiac PCr/ATP ratio in CHRs was observed at the first week, compared to the control group (2.90±0.35 vs. 3.31±0.45, p = 0.045), while the RVEF, RVEDVi, and RVESVi decreased at the second week (p < 0.05). The PCr/ATP ratio displayed a significant correlation with RVEF (r = 0.605, p = 0.001), RVEDVi, and RVESVi (r = –0.661, r = –0.703; p < 0.001).
CONCLUSIONS:
31P MRS can easily detect the cardiac energetics alteration in a CHR model before the onset of ventricular dysfunction. The decreased PCr/ATP ratio likely reveales myocardial injury and cardiac dysfunction.
Introduction
Chronic hypoxia is a common pathophysiological process of chronic hypoxia diseases (CHD) such as chronic obstructive pulmonary disease, interstitial lung disease, and chronic high-altitude disease [1]. Chronic hypoxia elicits a variety of functional responses in cardiomyocytes, including cell proliferation, cell hypertrophy and cell death [2]. It can lead to myocardial injury by an irregularity in energetics alteration in cardiomyocytes under unfavorable conditions, finally resulting in heart failure [2, 3]. Furthermore, chronic hypoxia can also cause pulmonary endothelial cell death and pulmonary vascular contractures. These processes lead to increase pulmonary vascular resistance and pulmonary hypertension (PH), subsequent hypertrophy and failure of the right ventricle (RV), and even death [4]. However, hypoxia-induced PH progresses slowly, with patients often exhibiting subclinical symptoms in the early stage. Thus, early detection of myocardial injury and clinical intervention are necessary. Some available data suggest that alterations in cardiac energy balance might be an early feature in the course of cardiac disease before myocardial injury occurs [4, 5].
Currently, several non-invasive approaches are available to evaluate myocardial injuries. Serum cardiac biomarkers tend to be sensitive; however, they are not specific enough and are limited by the time of myocardial injury. Doppler ultrasound technique cannot indicate myocardial injury directly. Although radionuclide myocardial perfusion imaging can reveal myocardial activity, its application is limited by its radioactivity and poor tissue resolution.
Cardiac magnetic resonance (CMR) imaging is the gold standard technique for assessing ventricular structure and function [5]. In mammalians, cardiac energy balance mainly refers to the dynamic homeostasis of phosphocreatine (PCr) and adenosine triphosphate (ATP) within mitochondria. Phosphorus-31 (31P) has high natural abundance (100%) and high content in cells. The 31P chemical shift range of biological organisms is wide (about 30 ppm), which is convenient for nuclear magnetic resonance (NMR) detection. It also allows the evaluation of myocardium energetics by 31P magnetic resonance spectroscopy (31P MRS). 31P MRS might be a potential tool to reflect the hypoxic energetic alteration by obtaining the ratio of concentrations of PCr to ATP (PCr/ATP) in vivo [6, 7]. Previous studies have mainly focused on diabetic cardiomyopathy or hypertrophic cardiomyopathy using 31P MRS, and only a few have investigated hypoxic myocardial abnormalities [8, 9]. Limited evidence is available on the course of disruption in myocardial energy balance. The progression of chronic hypoxia-related cardiac energetics alteration can be observed by 31P MRS in this follow-up study. The onset of energetics alteration might be a potential indicator for early assessment of chronic hypoxia. This study aimed to characterize the potential value of 31P MRS in evaluating cardiac energetics alteration in chronicahypoxic rats (CHR).
Methods
Animals
This study was performed according to the National Institutes of Health Guidelines for the Use of Laboratory Animals and was approved by the Ethical Review Committee of Experimental Animal Welfare of Nanjing Medical University (IACUC-1712011). Thirty male Sprague–Dawley rats weighing 230±10 g were obtained. Six rats served as the control group. The remaining 24 rats were given a single subcutaneous injection of SU5416 (20 mg/kg, MCE, HY-10374). Then they were placed in normobaric hypoxia chambers (CYES–II; Shanghai Anting Scientific Instrument Factory) with 10±1%oxygen as CHR. Every 6 rats were taken out for magnetic resonance scanning and hemodynamic measurements at the 1st, 2nd, 3rd and 5th week, and they were then sacrificed for pathological analysis. The CHRs were divided into four groups according to the modeling time (1w/2w/3w/5w, n = 6, respectively).
31P magnetic resonance spectroscopy
All the MR procedures were performed weekly in the 1st, 2nd, 3rd, and 5th weeks of modeling separately on a 7.0 Tesla horizontal magnet (Bruker BioSpec 7T). The animals were anesthetized using gaseous isoflurane in oxygen (3%box induction) and maintained at 0.5–2.5%during the entire MR procedures.
In this study, we adopted a method called ‘outer volume suppression’ as a reference and optimized it [10]. A 20 mm diameter dual-tuned (31P/1H) surface coil was used for transmission and reception. A standard non-localized pulse-acquisition sequence with six spatially selective saturation bands surrounding the volume of interest was used to avoid signal contamination from the structures around the heart. The acquisition parameters were: 50μsec block pulse, 23° flip angle, 1.5 s repetition time, 10 kHz bandwidth (BW), and 128 average.
Cardiac energy status was evaluated using PCr/ATP ratio calculated by dividing PCr by γ-ATP resonances using the spectral analysis software (TopSpin versions 4.0) (as shown in Fig. 1).
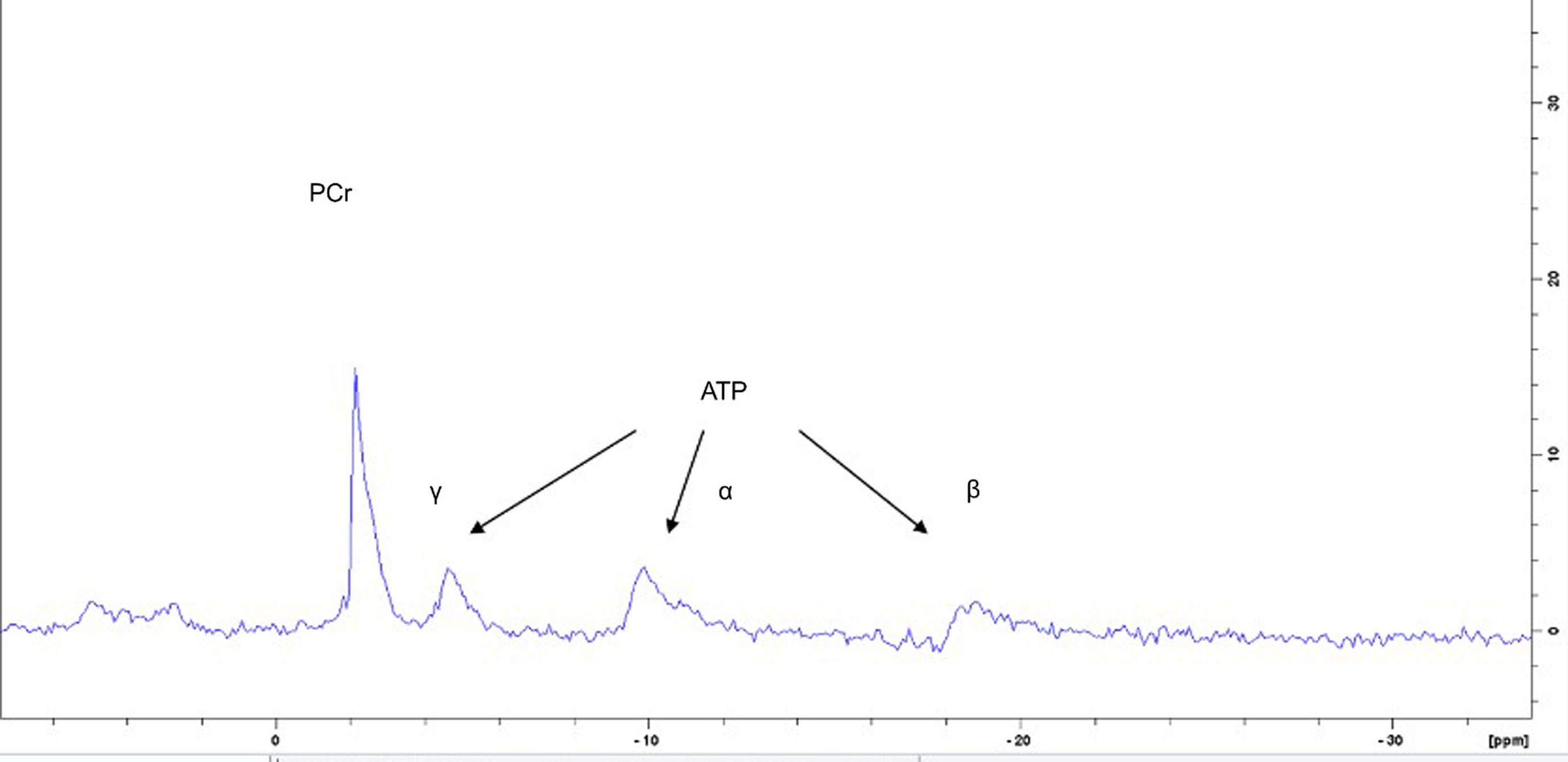
Cardiac energy status was evaluated using PCr/ATP ratio calculated by dividing PCr by γ-ATP resonance.
The system was equipped with a 72 mm inner diameter volume coil. The heart was placed at the center of the coil to acquire prospective ECG and respiratory-gated cine images to achieve four-chamber and short-axis views of the heart, with the following parameters: TE = 2.5 ms, TR = 8 ms, flip angle = 15°, field of view = 4.7*5.0 cm, 192×192 matrix, in-plane resolution = 244μm, slice thickness = 1.5 mm, and 14–23 frames/heartbeat. In addition, a set of five short-axis images was used to cover the heart.
Left and right ventricular volumetric parameters were obtained using the image analysis software (Circle CVI 42, Circle Cardiovascular Imaging Inc.) by outlining the end myocardium of both ventricles during end-systolic and end-diastolic phases (as shown in Fig. 2). The ventricle volumes were indexed to the body surface area (BSA) and calculated by the formula of BSA (m2) = 0.91*weight(g)2/3/1000. The right ventricular ejection fraction (RVEF), right ventricular end-diastolic volume index (RVEDVi), right ventricular end-systolic volume index (RVESVi), left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume index (LVEDVi), and left ventricular end-systolic volume index (LVESVi) were acquired.
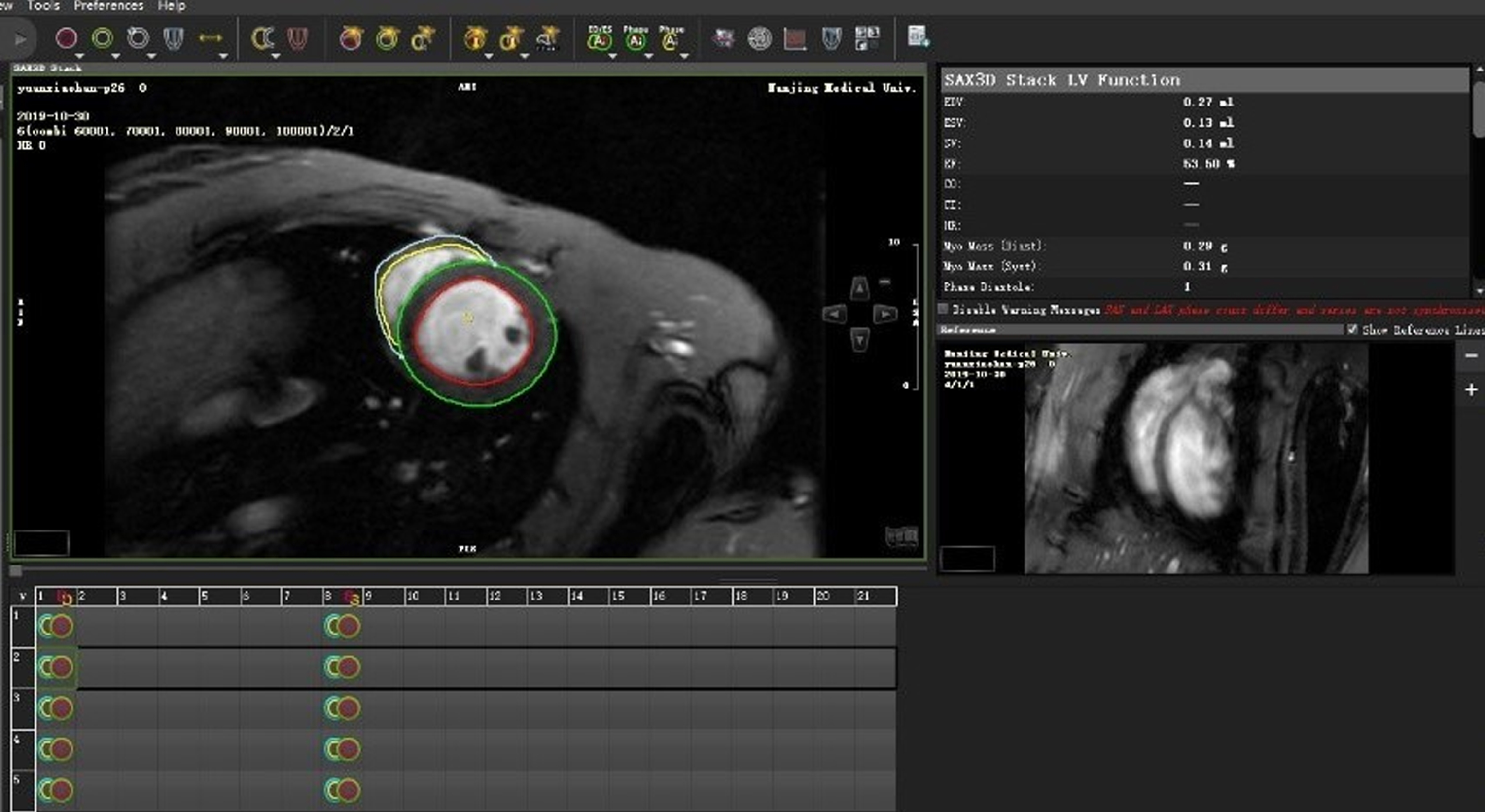
Left and right ventricular volumetric parameters were obtained using the image analysis software (Circle CVI 42, Circle Cardiovascular Imaging Inc.) by outlining the end myocardium of both ventricles during end-systolic and end-diastolic phases.
Every rat received a right heart catheter after MR procedures (as shown in Fig. 3). The rats were weighed and anesthetized with 1.0 g/kg urethane (Sigma–Aldrich), administered intraperitoneally. A polyethylene catheter (PE10, 427400; BD Biosciences) and heparin saline (125 U/mL; Changzhou Yinsheng Pharmaceutical Co., Ltd.) were inserted into the right jugular vein and advanced into the right ventricle. The catheter was connected to an MPA Acquisition and Analysis System (MP100; BIOPAC Systems, Inc.) by a pressure transducer (TSD104A; BIOPAC Systems Inc.). The right ventricular systolic pressure (RVSP) was recorded using a multiparameter monitor PM–8000 (Zhuhai Joyful Medical Equipment Co.) [11].
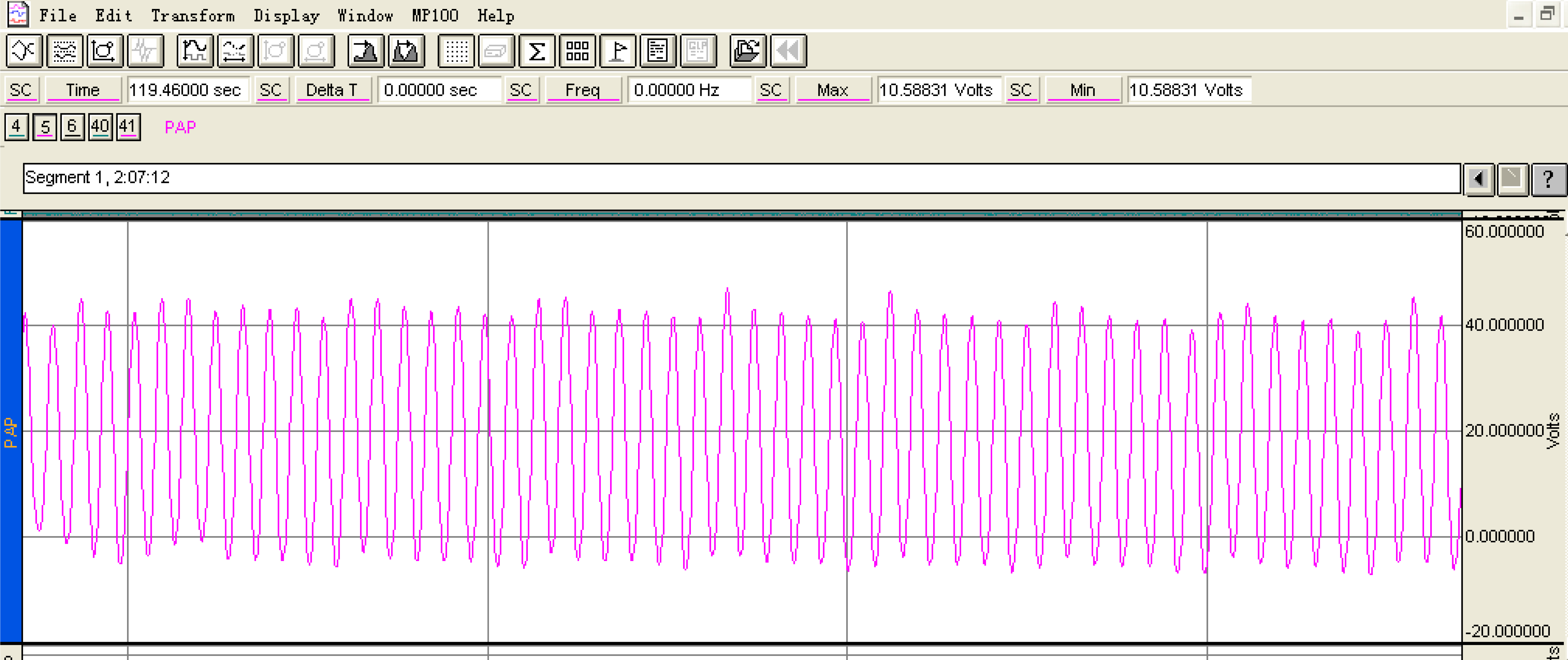
The right ventricular systolic pressure (RVSP) was recorded using a multiparameter monitor PM 8000 (Zhuhai Joyful Medical Equipment Co.). We will measure the RVSP of each rat three times, and finally take the average value.
After measuring hemodynamic parameters and blood sample collection, the rats were sacrificed by cervical dislocation, and the thorax was opened. The heart was removed, and the RV and left ventricle (LV) were separated. The mass ratio of RV to LV (RV/LV) was evaluated.
Cardiomyocyte hypertrophy was observed based on hematoxylin and eosin (H&E) staining. The myocardial fibrosis was assessed using Masson’s trichrome staining. Three 1 mm3 pieces were taken from the RV, LV, and S, separately, for transmission electron microscope (TEM) observations. Myocardial mitochondria were observed under the JEOL-1010 TEM.
Statistical analysis
Experimental data were expressed as mean±SD (
Results
Morphometric and hemodynamic in CHRs
RVSP and RV/LV increased continuously during hypoxia in CHRs; they underwent significant changes in the first week of modeling. During this experiment, one healthy rat died due to the right heart catheter, and one CHR died after a surgical procedure in the second week of hypoxia (as reported in Table 1).
Morphometric and Hemodynamic Characteristics (
)
Morphometric and Hemodynamic Characteristics (
Values are expressed as mean±SD. Note: BSA, body surface area; RVSP, right ventricular systolic pressure; RV/LV: the mass of right ventricle (RV) divided by the sum of the mass of left ventricle (LV). *P < 0.05 vs. control group.
RVEF significantly decreased, and RVEDVi and RVESVi increased from the second week. LVEF showed a brief decline in the first week, and then recovered in the second and third weeks. Both LVEF and LVEDVi got a significant reduction in the 5th week for a long hypoxia exposure (as shown in Table 2 and Fig. 4).
Cardiac magnetic resonance Characteristics (
Values are expressed as mean±SD. Note: RVEF, right ventricular ejection fraction; RVEDV, right ventricular end-diastolic volume; RVEDVi, right ventricular end-diastolic volume index; RVESV, right ventricular end-systolic volume; RVESVi, right ventricular end-systolic volume index; RVCO, right ventricular cardiac output; RVCI, right ventricular cardiac index; LVEF, left ventricular ejection fraction; LVEDV, left ventricular end-diastolic volume; LVEDVi, left ventricular end-diastolic volume index; LVESV, left ventricular end-systolic volume; LVESVi, left ventricular end-systolic volume index; LVCO, left ventricular cardiac output; LVCI, left ventricular cardiac index. *p < 0.05 vs. control group.
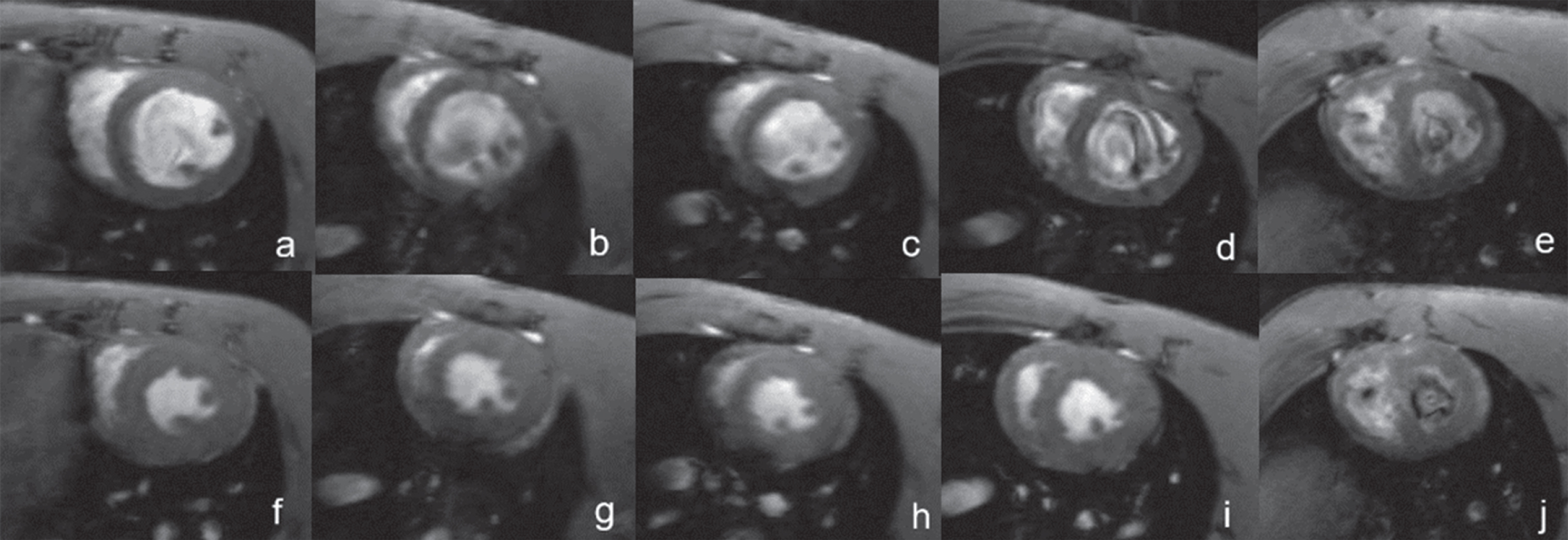
Cardiac magnetic resonance imaging: A-E: Short-axis cardiac images of end-diastole in healthy rats (a) and chronic hypoxia rats (1, 2, 3, and 5 weeks of modeling, b-e); F-J: Short-axis cardiac images of end-systole in healthy rats (f) and chronic hypoxia rats (1, 2, 3, and 5 weeks of modeling, g-i). Right ventricular dilation can be seen during hypoxia. In addition, interventricular septum flattening can be observed at the late stage of the disease, it shifted toward the LV and modified LV into geometry (“D-shape”).
31P MRS provided the capacity to follow up the cardiac PCr/ATP ratio in vivo. The PCr/ATP ratio dropped weekly, and it showed a significant decline in the first week of hypoxia vs. the control group (p < 0.05) (as repotted in Table 3). The histological results confirmed it (as shown Figs. 5 6).
Cardiac PCr/ATP ratio (
)
Cardiac PCr/ATP ratio (
Values are expressed as mean±SD. Note: PCr, phosphor creatine concentration; ATP, adenosine triphosphate. *p < 0.05 vs. control group.
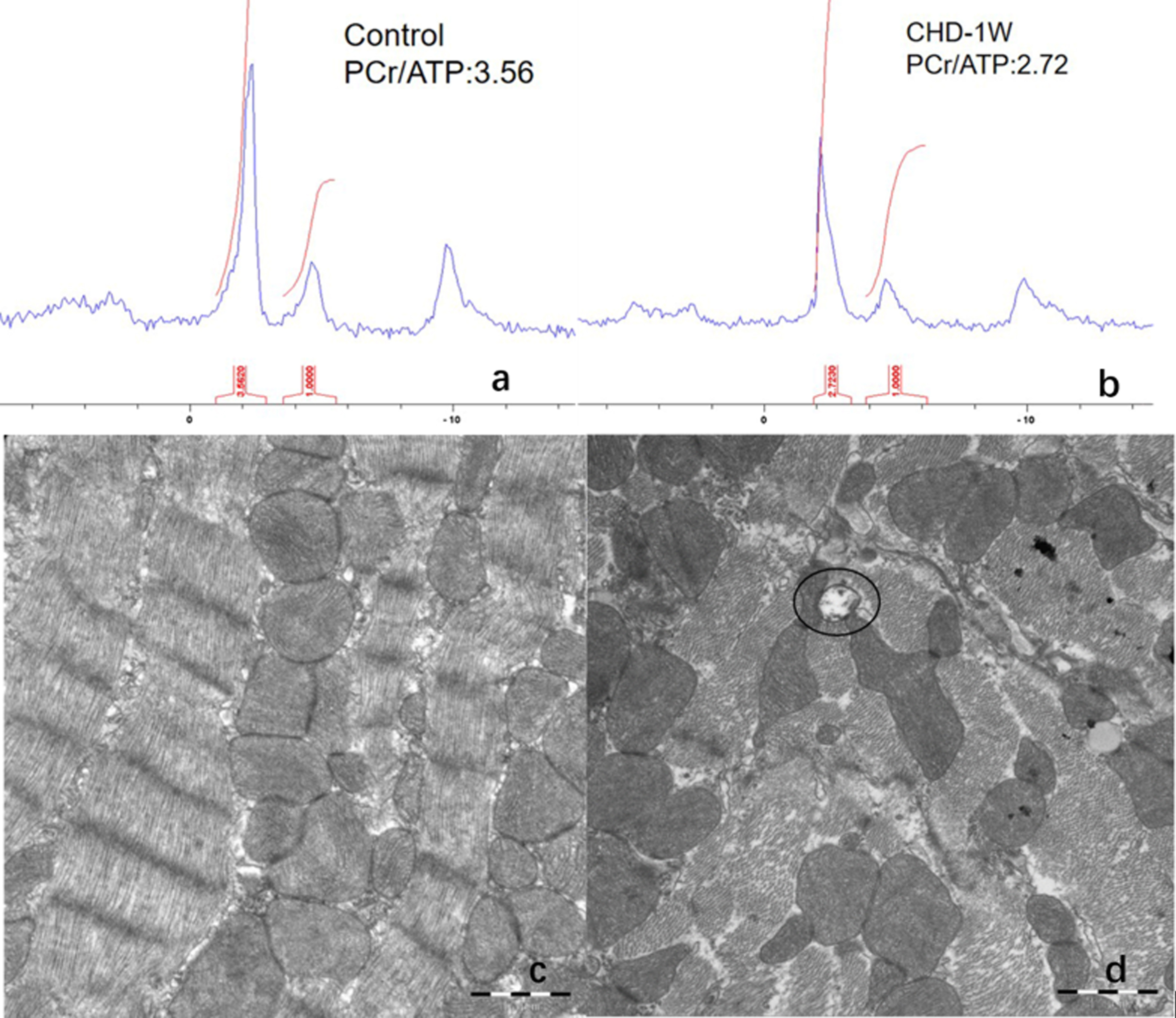
a-b: Myocardial PCr/ATP ratio dropped significantly in the first week of hypoxia. c-d: Increased mitochondrial autophagy in cardiomyocytes can also be observed simultaneously (TEM, ×25000).
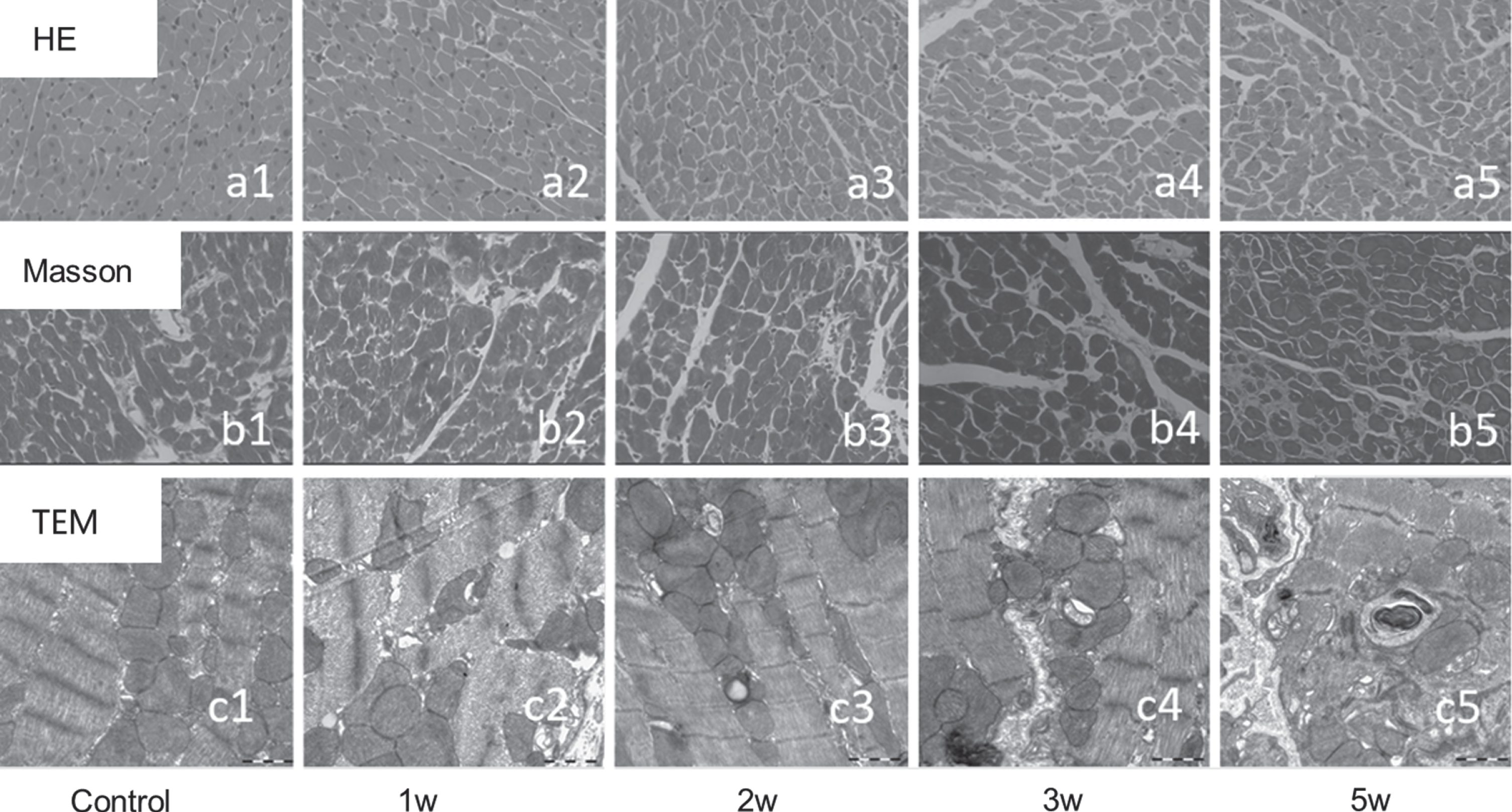
a1-a5: HE staining showed that cardiomyocyte hypertrophy and vacuolation occurred with the prolonged hypoxia time in the five groups. b1-b5: MASSON staining showed that with the occurrence of myocardial cell necrosis and apoptosis, the extracellular matrix fibrosis components increased (blue stained part). c1-c5: Increased mitochondrial autophagy in cardiomyocytes can also be observed simultaneously (TEM, ×25000).
RVEF showed a negative correlation with RVSP (r = –0.798, p < 0.0 01). RVESVi also positively correlated with RVSP. Cardiac PCr/ATP ratio showed a positive correlation with the RVEF (r = 0.605, p < 0.05), and inverse correlation with RVEDVi (r = –0.661, p = 0.001) and RVESVi (r = –0.703, p = 0.001). Cardiac PCr/ATP also showed a negative correlation with RVSP (r = –0.579, p = 0.002) (as shown in Fig. 7).
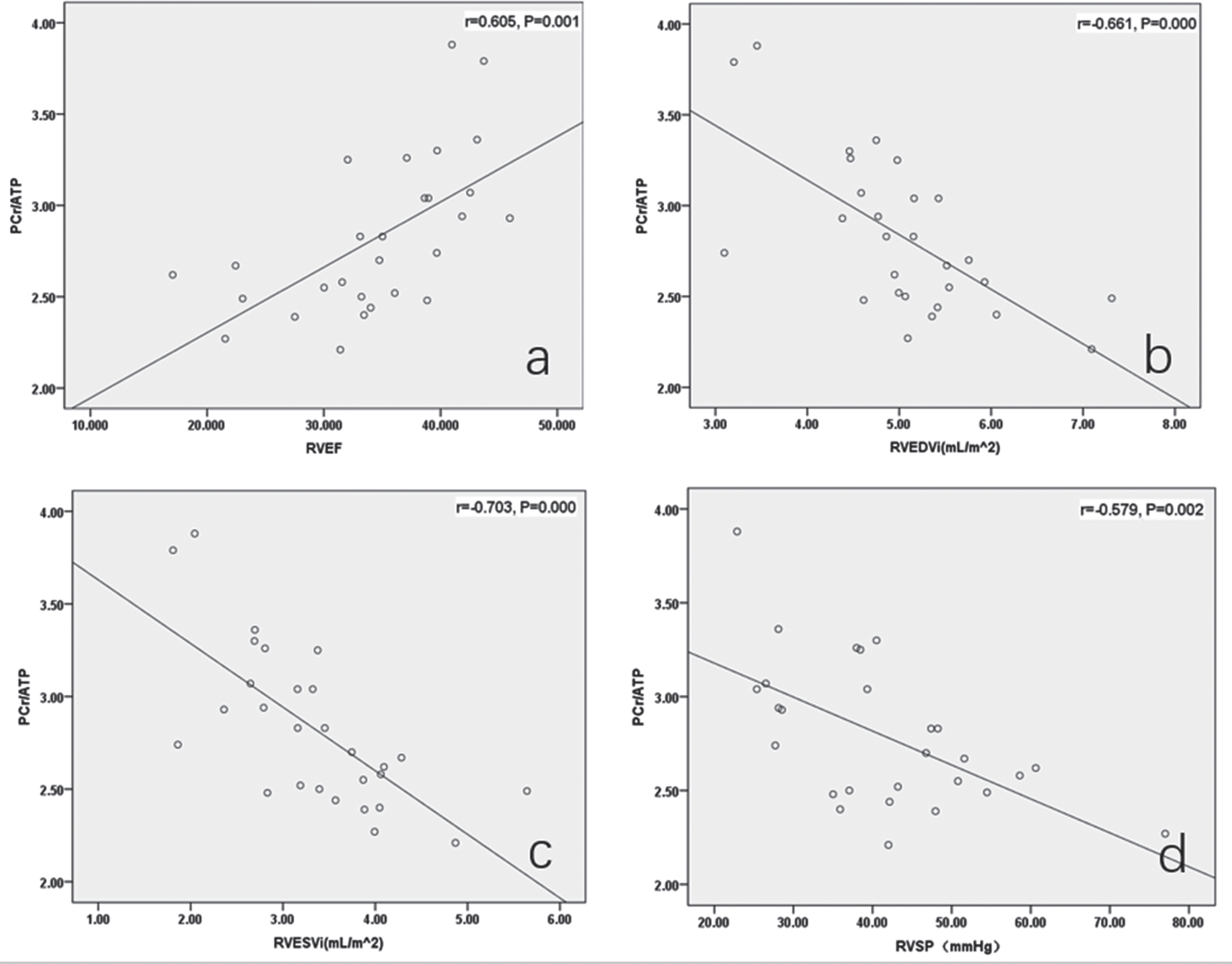
Correlation of PCr/ATP ratio with right ventricular performance and hemodynamics. a-c: Cardiac PCr/ATP ratio exhibited a positive correlation with the RVEF (r = 0.605, p < 0.05), and an inverse correlation with RVEDVi (r = –0.661, p < 0.001) and RVESVi (r = –0.703, p < 0.001). d: Cardiac PCr/ATP ratio also had a negative correlation with RVSP (r = –0.579, p = 0.002).
This follow-up study reported on the course of CHD development in CHR using 31P MRS. A decline in the myocardial PCr/ATP ratio was observed in the first week, while ventricular structure and function indexes exhibited no modification until the second week of molding. These findings indicate that the myocardial energetics alteration occurs before ventricular dysfunction. Furthermore, 31P MRS is a potential tool for detecting the severity of CHD. To the best of the authors’ knowledge, this is the first study in this area.
Hypoxia induces hypoxic myocardial injury and angio-obliterative PH in rats [12, 13]. Persistent RV hypertrophy and decreased RV function could be observed from the second week of modeling while the LV appeared insensitive to decreased oxygen levels, demonstrating that hypoxia-induced pathological changes mainly occur in the RV. Several previous studies have reached the same conclusion [14, 15]. In this study, a decrease in LVEF was observed in the first week of hypoxia, which was recovered in the second week possibly due to the compensation of the decreased oxygen availability or changes in the morphology of the RV and ventricular septum. The overload of RV pressure and volume cause the nterventricular septal swing, modified LV into geometry (‘D-shape’). Dilatation of the RV also increases the constrictive effect of the pericardium, all these can result in a reduction in the distensibility and filling of the LV [16]. This may explain why a preserved LVEF in the later stage of the experiment. The strong correlation between RVEF and RVSP indicated that RV function indicators could reflect the course of PH.
However, due to the adaptation to chronic hypoxia, RV was less prone to develop contractile dysfunctions initially. Therefore, it is necessary to seek a method that can sensitively reflect myocardial damage in its early stages. 31P MRS has previously been applied in hypertrophic cardiomyopathy, diabetic cardiomyopathy, and ischemic cardiomyopathy to detect myocardial energetics alteration [8, 9]; here, we applied it in hypoxic cardiomyopathy.
31P MRS provides myocardial metabolism information by detecting high-phosphate energy metabolism (PCr/ATP ratio) in cardiomyocytes. In this study, the myocardial PCr/ATP ratio decreased significantly in the first week before the modification of the ventricular structure and function parameters. As expected, increased mitochondrial autophagy was observed in cardiomyocytes in the first week of hypoxia. Cardiac metabolism principally relies on oxidative metabolism. Therefore, an adequate supply of oxygen and metabolic substrates is a significant prerequisite. Chronic hypoxia can lead to irregular cardiac energetics, which can be implicated in the pathophysiology of the heart [17, 18]. In response to chronic hypoxia, myocardial mitochondrial function was impaired, and the creatine kinase system was also affected. The transfer of high-energy phosphate groups of intracellular ATP to PCr was inhibited, resulting in decreased intracellular PCr levels. At the same time, ATP levels generated via mitochondrial lactate oxidation decreased [17]. Finally, hypoxic cardiomyocytes underwent necrosis or apoptosis. Thus, the decline in cardiac PCr/ATP ratio shown by 31P MRS might be an early feature in the course of myocardial injury. Therefore, we speculate that 31P MRS is a reliable tool for detecting myocardial injury in its early stages and a more sensitive method than traditional cardiac structural and functional parameters in CHD.
The PCr/ATP ratio obtained by 31P MRS proved to have a good correlation with RVSP. In future clinical applications, 31P MRS may tend to replace the invasive RHC procedure for detecting CHD severity. PCr/ATP ratio also exhibited a moderate, positive correlation with the RVEF and an inverse correlation with RVEDVi and RVESVi, and the change of PCr/ATP ratio occurred earlier than the traditional cardiac magnetic resonance index, indicating that 31P MRS can be used as a more sensitive non-invasive examination for observing the changes in the heart of CHD patients. Nowadays, clinical treatment of CHD is always focused on inflammation, hypoxia, and PH. Only a few treatments are involved for targeting myocardial injuries [15]. With 31P MRS, an earlier clinical intervention to prevent myocardial injury is important to improve the prognosis of CHD.
There are several limitations in the present study. First, this study achieved a higher cardiac PCr/ATP ratio (2.49–3.31) than some previous studies (1.72–2.70) [10, 21]. The muscle on the chest wall might result in a higher myocardial PCr/ATP ratio [22]. Six spatially selective saturation bands were placed around the volume of interest in this study to avoid signal contamination from the chest wall and other structures around the heart. Second, a standard non-localized pulse-acquisition sequence was selected in this 31P MRS scanning. A localized scan might help acquire a more accurate result. Also, cardiac strain analysis might be more sensitive than volume parameter changes; however, the relevant strain analysis was not involved in this study.
Conclusions
In conclusion, CMR is a reliable tool for observing modifications in cardiac size and function during the progression of CHD. 31P MRS is a potential non-invasive tool for the analysis of myocardial energy homeostasis in CHD in vivo. It can sensitively reveal the cardiac energetics alteration in CHD before the onset of ventricular dysfunction and reflect its severity.
Competing interests
The author(s) declare that there is no conflict of interest.
Disclosure statement
We certify that we all have participated sufficiently in the work. All authors have read and approved the manuscript. Publication is approved by all authors. Authors have nothing to disclose with regard to commercial support.
Acknowledgment and funding
This work was supported by the National Natural Science Foundation of China (Grant No. 81601464 and 81701651) to Yinsu Zhu and Xiaomei Zhu.