
Abstract
BACKGROUND:
Manual or machine-based analysis of chest radiographs needs the images acquired with technical adequacy. Currently, the equidistance between the medial end of clavicles and the center of spinous processes serves as the only criterion to assess whether a frontal PA chest radiograph is taken with any rotation. However, this measurement is normally difficult to implement because there exists overlapping of anatomies within the region. Moreover, there is no way available to predict exact rotating angles even the distances were correctly measured from PA chest radiographs.
OBJECTIVE:
To quantitatively assess positioning adequacy of PA chest examination, this study proposes and investigates a new method to estimate rotation angles from asymmetric projection of thoracic cage on radiographs.
METHOD:
By looking into the process of radiographic projection, generalized expressions have been established to correlate rotating angles of thorax with projection difference of left and right sides of thoracic cage. A trunk phantom with different positioning angles is employed to acquire radiographs as standard reference to verify the theoretical expressions.
RESULTS:
The angles estimated from asymmetric projections of thoracic cage yield good agreement with those actual rotated angles, and an approximate linear relationship exists between rotation angle and asymmetric projection of thoracic cage. Under the experimental projection settings, every degree of rotation corresponds to the width difference of two sides of thoracic cage around 13–14 pixels.
CONCLUSION:
The proposed new method may be used to quantify rotating angles of chest and assess image quality for thoracic radiographic examination.
Keywords
Introduction
Digital chest X-ray radiography has become one of the most cost-effective and frequently performed medical imaging examinations for diagnosing and screening thoracic abnormalities due to its wide exposure latitude and minimal radiation dose [1, 2]. In the United States nearly half of the radiographs are taken from chest X-ray (CXR) and it is estimated there will be about 5.5% annual growth rate every year on radiography [3]. This tremendous amount of chest radiographic examinations brings great challenges for radiologists to do the following interpretation. To alleviate this burden, computer-aided diagnostic technologies have been introduced to assist clinicians to conduct image analysis such as segmenting suspicious lesions, identifying diagnostic signs and so on. Benefited from the boosting of computation power, recent advancement in deep learning approaches further enhance the ability of image processing algorithms to automatically analyze thoracic radiographs, and the developed diagnosis systems have been reported with performance comparable to medical professionals [4, 5].
To achieve an automatic interpretation of chest radiographs with clinically acceptable reliability, the input images should fulfill necessary requirement of technical adequacy like those required by radiologists for their interpretation. Adequate penetration and right positioning are two main factors to determine image quality offered by a radiographic examination [6]. For digital CXRs, not much effort will be required for penetration adequacy because the available wide exposure range and auto-exposure control settings allow the visualization of vertebral bodies as well as pulmonary vessels through the mediastinum and lungs. However, it’s generally difficult to have radiographs taken under ideal positioning due to subject’s unintentional movement or maneuver during a process of examination. For a frontal erect posteroanterior (PA) position, any degree of rotation around sagittal plane may distort the position of internal anatomic structures, which may cause substantial amounts of medical diagnostic information obscured and result in misinterpretation of the radiographs [7]. Consequently, PA chest radiographs taken under correct positioning is essential to ensure the effectiveness of the following diagnostic interpretation and interventional therapy [8, 9].
It’s well known that the equidistance between the medial end of clavicles and a line drawn through the center of spinous processes at the level of the clavicles serves as the criterion to confirm whether a erect PA chest radiograph is taken with chest being rotated [10, 11]. Though this guideline has been described in most textbooks of radiographic technique for assessing the positioning technical adequacy of PA chest radiographs, so far there is no evidence to show how to quantify the actual angle of patient rotation when the distance from clavicle to spinous process is perceived in CXRs. Hardy et al. [12] carried out a series of experiments using a radiopaque bar representing spinous process line and two other horizontal radiopaque bars representing the clavicles to simulate various configuration of radiographic image acquisition. It is concluded that the assessment of rotation of CXR should also count in the factors of body morphology like anteroposterior thoracic diameter besides the variation of clavicular distance to spinous processes. In another prospective study, Ogoke et al. [13] confirmed that the variation of body habitus, body mass index and gender were all related to the increment of rotation on chest radiographs. Although the above work suggested all the relevant factors should be taken into consideration when the estimation of chest rotation was concerned, they haven’t explicitly expressed how the sagittal rotation was affected by those factors mentioned above.
In order to estimate rotation angles, it is nature to think about approaches to accurately detecting the clavicles as well as the adjacent vertebras according to the textbook recommendations on radiographic technologies. But the radiographic densities around clavicle region often present complex variation due to several anatomic structures overlapped along projection direction [14]. This decreases image contrast and causes problems for accurate detection of clavicle heads and spinous processes. Therefore, the diaphysis of the bone rather than the medial epiphysis of clavicle was selected as an alternative to detect for achieving reliable automatic evaluation of chest radiographs [15]. In view of the rotation estimation of chest radiographs sensitive to the detection of actual boundary of clavicle head, Santosh et al. [16] designed an algorithm to compute the principal rib-orientation from the area of left and right lung regions. Based on the observation that rotating thoracic lung has consistent effect on the positions of clavicles and ribs, they used the principal rib-orientation to estimate the rotation of clavicles. This approach avoids the process of detecting clavicle heads and improves the stability of rotation estimation. These strategies facilitated automatic detection of thorax rotation, but they were only able to distinguish the cases of severely rotated CXRs and form a decision between rotated and non-rotated ones. Meanwhile the pathologic signs such as pleural effusions as well as posterior ribs often made the background complicated for preprocessing and deteriorated the effectiveness of detection algorithms.
Considering the difficulties in reliable detection of ribs and clavicles due to the disturbance of regional overlapped anatomies, and there is no quantitative approach available for evaluating rotating angles of CXRs, this paper will look into the process of radiographic projection and build generalized expressions to correlate thoracic rotation angles with asymmetric projection between left and right sides of thorax. As the outlines of rib cage can be reliably identified for calculating the geometric asymmetry of chest radiographs, the proposed approach would be useful to quantitatively evaluate chest radiographic positioning and standardize chest radiographic acquisition for the following automatic diagnostic analysis.
Materials and methods
Geometry of projection radiography
A standard frontal PA chest radiograph is a 2D projection of X-ray beam passing through 3D thoracic structures from posterior to anterior direction and acquired by a detector with the patient standing in an upright position. Figure 1(a)-(c) demonstrate a correctly acquired CXR with the spine overlapping with the sternal midline in the midsagittal plane which equally divides rib cage into the symmetric left and right halves. That means the shape of rib cage presented in the chest radiograph is symmetrically distributed and the distance L0 from the center of the (T7) vertebral body to the lateral border of left thoracic cage is equal to its counterpart R0 in the right side. This symmetric projection characterization might be one of simplest but most efficient signs being used to identify the abnormalities of chest radiographs or assess image quality of radiographic examination. As the thorax is a 3D anatomic structure with dimension of width LR and depth PA in a cross-section view, the symmetric relationship between left and right sides of rib cage may not exist anymore when chest is rotated during the procedure of image acquisition. Technically the rotation angles would be predictable when necessary information is available such as the difference of projection of left and right sides of thorax, source-to-image distance (SID), object-to-image distance (OID), source-to-object distance (SOD) and so on.

Illustrative explanation of projection radiography.
To illustrate the approach of rotation estimation, the sectional slice at the 7th thoracic vertebra was taken as an example to demonstrate the asymmetric projection caused by the chest rotation. In Fig. 1(a), W represents the distance from the center of the vertebral body to the lateral border of the right (left) thoracic cage and is termed as virtual rotation radius (VRR); θ represents original angle between the VRR and PA projection direction, which is related to the shape index of thorax and termed as SIT angle; δ represents rotated angle of thorax around the center of vertebra. When the thorax is rotated by an angle of δ, the projection of the VRR will be elongated from L0 to L1 in the left side, while the projection in the right side will be foreshortened from R0 to R1. According to the theory of trigonometry and similarity, the new projection can be expressed as following:
From the equation (1) and (2), the difference and total projection of the left and right rib cage, and the ratio between them can be calculated as:
Expressions (1)–(5) generally correlate the projection lengths of two sides of rib cage with the function of rotation angle δ. In order to have a direct relationship to estimate rotation angle from projection lengths of both sides of rib cage, the equation (5) can be further approximated according to the fact that the standard SID distance (normally set to standard 180 cm for achieving satisfactory magnification for erect PA chest radiograph) is much greater than the VRR. That is
According to the small angle approximation, the rotation angle, its sine and tangent functions will be fairly close when the rotation angle is small (less than 15 degrees say). Thus, the equation (7) can be further simplified as:
In equations (8) and (9) the asymmetric projection of the rib cage represented by the width difference relative to total width of left and right rib cage is directly related to the rotated angle δ. Or, the rotating angle can be calculated by rearranging the equation (9) providing the information of geometric asymmetric projection available, i.e.
To verify the above theoretic relationship between rotation angle and radiographic asymmetric projection of thoracic cage, a transparent trunk part of a life-size, full body anthropomorphic phantom is taken as a subject to simulate chest radiographic examination. This rigid phantom is selected because it can be manipulated relative easily to produce desired rotation angles and no ethic approval is needed to apply for carrying out the experiments. A reliable medical X-ray examination machine, Siemens Multix Select DR system, was adopted to generate digital radiographs of the phantom through an auto-exposure control mode with a fixed 100 kVp high radiation energy. In order to rotate the phantom of trunk to a specific angle, the phantom is sitting erectly in a box and fixed with no relative movement to box by using radiolucent foams. The metal frame underneath the box supports the weight of the phantom and box. The phantom and the box together with the metal frame can be manually rotated around one center point as shown in Fig. 2 (a) and (b).
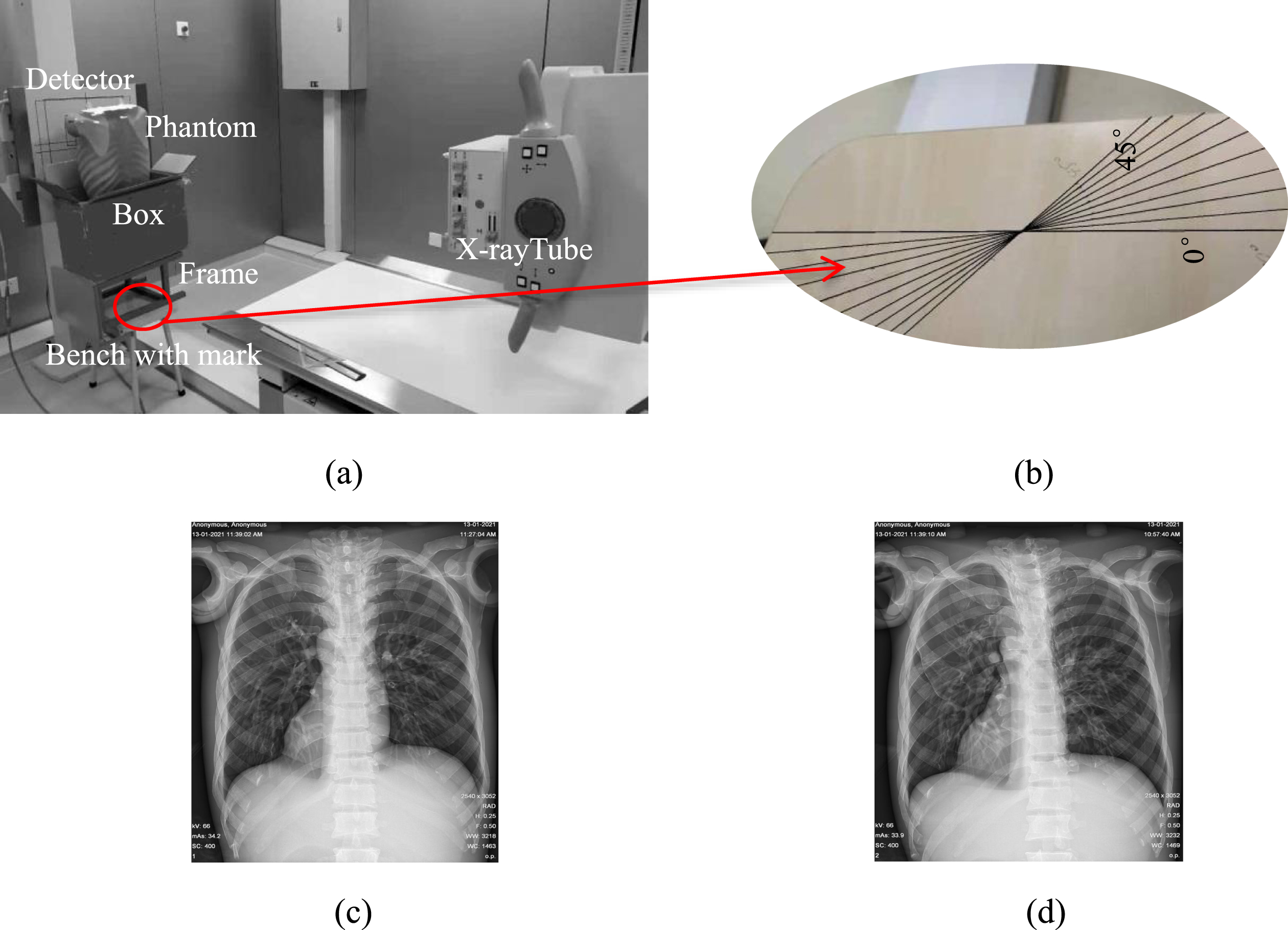
Setup designed for experiments (a) to enable the chest rotated in different angles marked on the bench top (b), and radiographs taken under rotating angles of 0° (c) and 10° (d).
During the experiments the metal frame is rotated from 0 to 30 degrees with an equal interval of 5 degrees along the lines marked on the top of the bench which keeps standing still on the ground. Figure 2 (c) and (d) show two examples of radiographic images of the trunk phantom taken under the rotating angle of 0° and 10°. After the radiographs are acquired, the distance between the center of the thoracic vertebral body and the outline of the lateral border of the left (right) thoracic cage, i.e. the L1 and R1 are measured and recorded for the verification of the equations (1) to (10).
Based on the projection geometry of the experimental settings and the physical dimension of trunk phantom, the SID, SOD, VRR and θ angle are taken as 180 cm, 165 cm, 13.7 cm and 70° respectively. They are then substituted into equation (1) – (10) to calculate the asymmetric projection of the left and right sides of rib cage. Table 1 lists the calculated results in pixels with a size of 139μm, same as that of detector used in real X-ray examination machine. As a comparison, Table 1 also lists the averaged results measured from the actual radiographs of trunk phantom by two experienced radiologists. It can be found that the theoretical calculation results are able to correlate with those measured from actual radiographs fairly well. Figure 3 plots two fitted lines of projection difference (L1-R1) of two sides of rib cage changing with the rotation angles for calculation and measurement results.
Dimensions of rib cage calculated from equations and actually measured
Dimensions of rib cage calculated from equations and actually measured
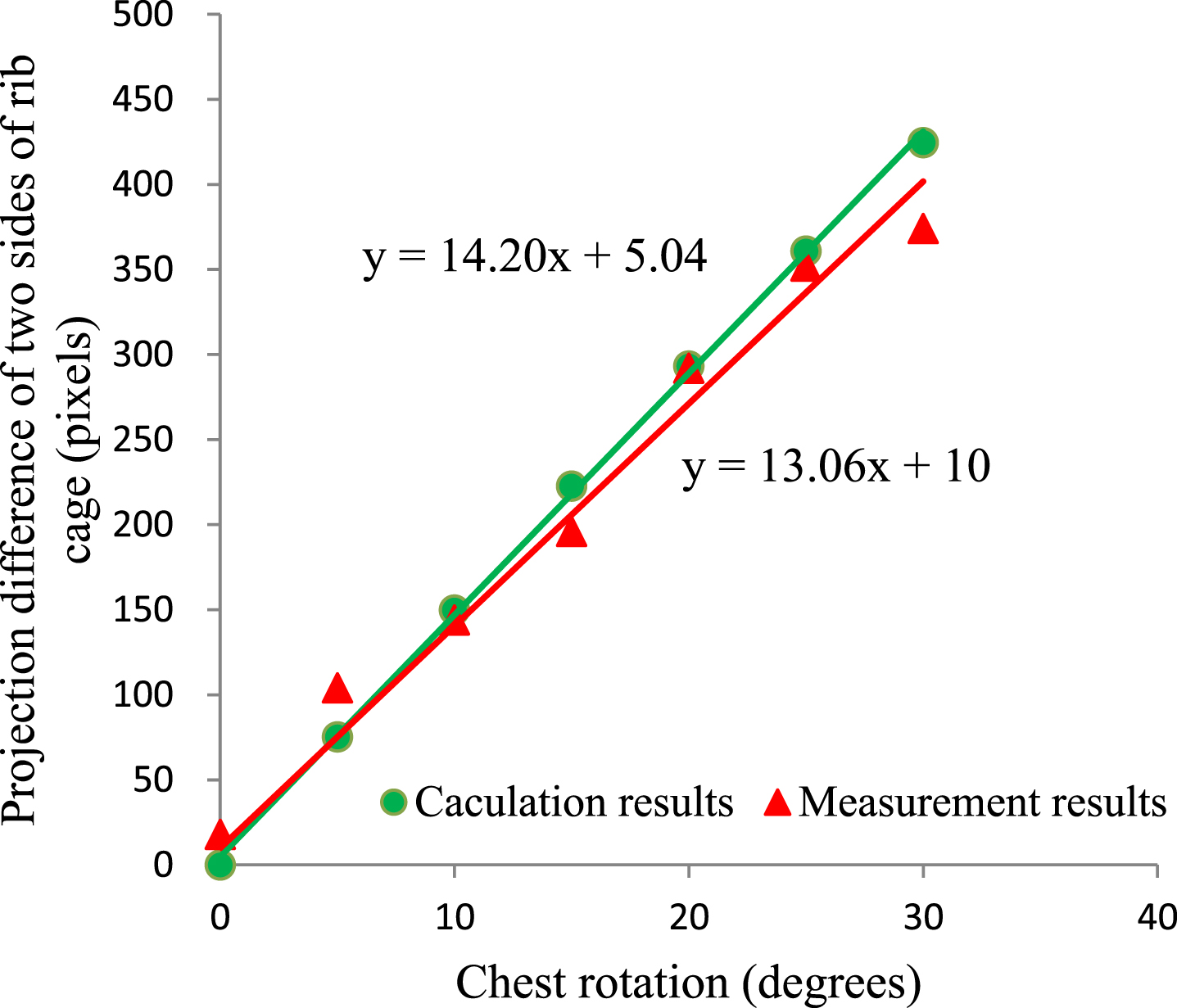
Relationship between rotating angle and asymmetry of rib cage calculated from equation 5 and measured from actual radiographs of trunk phantom.
This study tries to generalize a simple relationship between thorax rotation and geometric asymmetric projection of two sides of thoracic cage on radiographs. Although the initial expression in the equation (5) looks not such straightforward, both theoretical calculation and actual experiments have identified that this relationship can be approximated linear. According to the linear equations optimally fitted from the data of experimental measurement and theoretical calculation, it can be found that one additional degree of rotation angle will bring the asymmetric projection between left and right side of rib cage around 13-14 pixels. By substituting all relevant experimental data into the equation (9) or (10), similar correlation coefficients can be obtained between rotation angle and geometric asymmetry between two sides of rib cage. This verifies that the approximated equations can be used to predict rotating angles from asymmetric projection of rib cage too.
In order to eliminate the inter-observer variation in identifying rotating center around vertebral body as well as lateral borders of both sides of thoracic cage, two experienced radiologists are invited to use a free available and widely used DICOM viewer software ImageJ to mark the rotating center from chest CT images and measure the dimension of thoracic cage from chest radiographs. The Line Selection and Wand tools in the ImageJ can help the radiologists find the interested edge of ribcage and trace its shape with a pixel level of accuracy [17]. According to the fitted linear relationship between the rotation angle of chest and the asymmetric projection of rib cage, the pixel level of measurement uncertainty only brings the deviation of the estimated angle less than 0.1 degrees. Although the lateral borders of thorax and the center of vertebral bodies are not difficult to locate in a manual manner because of good contrast of these bony structures, and the estimation results are not sensitive to the measurement uncertainty, an automatic approach is still expected to be developed to identify these anatomic marks in order to improve repeatability and reliability of this new estimation approach. One of the most possible options might be deep learning approaches which have shown remarkably powerful for the tasks of chest radiograph analysis such as lung segmentation and bone suppression.
During estimating rotation angles, the VRR and SIT angle are taken from the CT scanning results of trunk phantom. Obviously, these data may not be applied to all individuals as the dimension and shape of thoracic cage are kept evolving in different gender and ages, particularly in the young population [18]. However, the size and morphology of rib cage becomes quite constant for adults over 30 with average LR and PA dimension of rib cage 25 cm and 16.5 cm respectively [19]. If the range of VRR was taken from 12 cm to 16 cm, the prediction of asymmetric projection of rib cage relative to one degree of rotation angle will become 12 and 17 pixels.
It can be found from equations (9) and (10) that the prediction of rotation angle from asymmetric projection of rib cage is influenced by two factors, i.e. the SIT angle and the VRR length which are measured around 70 degrees and 13.7 cm for the case of trunk phantom. By comparing these two factors the SIT makes contribution around 4 time of that from the ratio of VRR and SOD. Thus, the variation of shape of thoracic cage will have more influence on final prediction of asymmetric projection of rib cage. As the ratio of thoracic width to height within the middle levels of thorax demonstrates little changes with increasing age [18], the asymmetry of mid thoracic cage can be a better option for reliably predicting rotation angles of thorax.
Conclusions
To quantitatively estimate rotation angle of chest from CXRs for assessing positioning criterion, this paper generalized expressions to explicitly calculate chest rotation from asymmetric projection of rib cage. The calculation and measurement results verified that the rotation angles linearly change with the asymmetry of thoracic cage. Meanwhile, the shape and dimension of rib cage were found as two main factors affecting the predictability of rotation angle. This quantitative analysis approach can be used to reliably assess image quality of thoracic radiographic examination.
Footnotes
Acknowledgment
This study was supported by the National Natural Science Foundation of China (Grant No. 81830052), Construction project of Shanghai Key Laboratory of Molecular Imaging (18DZ2260400), the Innovative and Collaborative Project Funding of Shanghai University of Medicine and Health Sciences (SPCI-17-18-001) and 2020 Joint Project of Health Committee in Shanghai PuDong New Area (PW2020D-14).