
Abstract
PURPOSE:
To evaluate efficacy and safety of flexible ureteroscopy and laser lithotripsy (FURSL) for treatment of the upper urinary tract calculi.
METHODS:
We retrospectively analyzed 784 patients who underwent FURSL between January 2015 and October 2020 in our unit. All patients were preoperatively evaluated with urine analysis, serum biochemistry, urinary ultrasonography, non-contrast computed tomography and intravenous urography. The procedure was considered as successful in patients with complete stone disappearance or fragments < 4 mm on B ultrasound or computed tomography. The operative parameters, postoperative outcomes and complications were recorded and analyzed respectively.
RESULTS:
The average operative time and postoperative hospital stay were 46.9±15.8 min and 1.2±1.1 days, respectively, among 784 patients. In addition, 746 patients were followed up and 38 patients were lost. In these patients, 700 (93.8%) cases met the stone removal criteria and 46 cases (6.2%) did not meet the stone removal criteria who need further treatment. The stone free rate (SFR) is 92.5%after 1–3 months and SFR of middle and upper calyceal calculi was higher than that of lower calyceal calculi significantly. The most common complications were fever (58/784, 7.4%), gross hematuria (540/784, 68.9%) and lpsilateral low back pain (47/784, 6.0%). The incidence rate of serious complication was 1.28%(10/784), including 5 cases of septic shock and 5 cases of subcapsular hematoma, which were cured after active treatment.
CONCLUSION:
FURSL is a reliable treatment for small and medium calculi patients of upper urinary tract. The curative effect of stone removal is clear. The complications are few and the safety is high. However, there are certain limitations to the efficacy in treating larger stone and lower calyceal calculi.
Introduction
Urolithiasis is one of the most common health problems with increasing occurrence rate worldwide [1]. In recent years, the number of patients with upper urinary tract calculi has increased significantly, most of them were renal calculi. Among of these patients, 25%of them need surgical intervention when they were diagnosed [2]. At present, minimally invasive surgery is the main treatment for the upper urinary tract stone, which including extracorporeal shock wave lithotripsy (ESWL), laparoscopic ureterolithotomy, percutaneous nephrolithotomy (PCNL), ureteroscopy lithotripsy (URS) and flexible ureteroscopy and laser lithotripsy (FURSL). According to the guideline, ESWL is the first choice for the stone of non-renal lower calyx less than 2 cm and for the ureteral stone less than 1 cm, and for the renal stone larger than 2 cm, PCNL is the first choice. With advances in endoscopic technology coupled with the development of laser lithotripsy systems and novel endoscopic baskets, flexible ureteroscopy has become an increasingly popular option for the treatment of upper urinary tract stones, especially for renal stones [3–7]. At present, many literatures [8–11] show that flexible ureteroscopy can successfully treat patients with stones > 2 cm with a high stone-free rate and a low complication rate and show that the efficacy of flexible ureteroscopy can allow an alternative to PCNL. With the continuous improvement and perfection of flexible ureteroscope and associated lithotripsy equipment, especially the development of YAG holmium laser system, it has the advantages of small trauma and high stone free rate (SFR). It has brought a qualitative leap for the minimally invasive treatment of upper urinary tract calculi and is favored by majority of the clinicians.
At present, FURSL has been demonstrated as an alternative treatment choice to PCNL or ESWL with minimal complications and a high success rate in treating the upper urinary tract stones [12–15]. The FURSL was applied in clinical practice since 2015 in our units, and until now, we use this technique in treatment for the patients of upper urinary tract calculi. Most of them, the diameter of stones are less than 2 cm, and the renal stones of some cases are more than 2 cm. Based on it, we collected the clinical data of the patients of upper urinary tract calculi who underwent the FURSL procedure, and summarized and analyzed the outcomes of FURSL. Therefore, the purpose of our present study was to evaluate the clinical efficacy and safety of FURSL for upper urinary tract calculi in our units.
Materials and methods
Study population
We retrospectively analyzed the data of 784 patients with upper urinary tract stones who successfully received FURSL in our unit from January 2015 to October 2020. Prior to operation, all patients received the routine assessment which included medical history inspection, routine blood test, coagulation parameters, urine analysis, serum creatinine, electrocardiogram, ultrasonography, intravenous urography, compute tomography scan of abdomen and pelvis. The stone burden was measured based on the maximal diameter of the stone on non-contrast CT in all patients. Appropriate antibiotic prophylaxis was administered pre-operatively and intra-operatively according to the patient’s positive urine culture results, and adequate control of urinary tract infections was confirmed by urine culture before surgical management. Prophylactic antibiotic including quinolones or cephalosporins was administered pre-operatively and intra-operatively to patients with negative urine culture results. All operations were performed by surgeons of the same seniority.
Surgical procedure
All patients were placed in the lithotomy position and all operations were performed under the general anesthesia. Among all patients, 421 cases were indwelled F6 double J stent for 2 weeks before FURSL procedure. At first, the double J tubes were removed if the double J tubes were placed, then under the guideline of safety wire, the F9.8 semi-rigid ureteroscope were used to access to ureter. If ureteric calculi were observed, lithotripsy was performed using a Holmium laser with a 365μm fiber at an energy range of 0.8–1.2 W and a frequency of 20–25 Hz. After confirming the clearance of stone from the ureter, a F12/14 ureter access sheath (UAS) was inserted into the proximal ureter with the guide wire. Then, a F7.5 flexible ureteroscope was passed through the UAS, and the front end of the UAS was placed in the pyeloureteral junction under direct view of the flexible ureteroscope. The perfusion flow was set to 60–100 mL/min. When entering the renal pelvis, the renal pelvis and calyces were observed and the stones were found accurately. Lithotripsy was performed using a holmium: yttrium aluminum garnet (Ho: YAG) laser with a 200μm fiber at an energy range of 1.0–2.5 W and a frequency of 15–25 Hz. According to the actual situation of the operation, three types of lithotripsy were used: fragmentation (high energy, low frequency), dust (low energy, high frequency), and popcorn effect (high energy, high frequency). The stone should be powdered as much as possible (the maximum diameter of the stone is less than 0.4 cm), and the larger stone should be taken out with the help of reticular basket for the analysis of stone composition. In order to avoid the damage of flexible ureteroscope, the stones which located at the lower renal calyceal could be put into the middle or upper renal calyceal and renal pelvis through the reticular basket, and then lithotripsy could be carried out. At the end of the operation, all renal calices were checked to confirm satisfied fragmentation before the F6 double J stent was placed routinely.
Data collection and Follow up
All the patients’ data were obtained from the hospital’s electronic medical record system. The characteristics of the patients which include the age, gender, body mass index (BMI), stone burden, history of previous surgery on the ipsilateral side, urine cultures, whether using antibiotics and comorbidities. The operation time, postoperative hospital stays, one-time success rate of lithotripsy, renal function and hemoglobin changes before and after operation were recorded. In addition, the postoperative complications were also recorded according to the modified Clavien-Dindo classification as recommended. KUB examination was performed in all cases on the first day after operation. All patients were followed up routinely in the outpatient clinic at 1 to 3 months postoperatively. At 1 month postoperatively, non-contrast CT or urinary ultrasound were performed to confirm the stone clearance status, in which stone-free rate (SFR) was defined as radiological residual fragments less than 4 mm, and the double J stent was removed in the outpatient clinic. If the residual stone fragments were more than 4 mm which required the further treatment such as FURL, ESWL and external physical vibration lithecbole (EPVL), the removal of double J stent would be delayed until three months postoperatively due to the clearance of stones.
Data analysis
SPSS 20.0 software was applied for statistical analysis. Continuous data were analyzed using the mean±SD and compared by non-parametric t test. The count data were expressed by the number of cases (percentage), and the comparison between groups was used χ2 test. P < 0.05 was considered statistically significant.
Results
Total 784 patients were analyzed retrospectively. The characteristics of the patients and the stone were showed in Table 1. The FURSL operation was performed successfully in all patients. Peri-operative data were summarized in Table 2. The mean operating time was 46.9±15.8 minutes and post-operative hospital stay was 1.2±1.1 days. Meanwhile, we compared the serum creatinine and hemoglobin before and after the operation, and no significant differences were observed (P > 0.05). No severe bleeding and acute renal failure were observed.
Baseline characteristics of the 784 patients
Baseline characteristics of the 784 patients
Clinical outcomes of the 784 patients with treatment of FURSL
*Compared to pre-operation, no significant difference was obtained. # compared to postoperative one day, significant difference was observed. P < 0.05 was considered statistically significant.
Complications were classified as intra-operative and post-operative and summarized in Table 2. Ureter injure is the main complication during the operation, which is caused by the ureteral access sheath entering the ureter. In this study, ureteral injury and renal pelvis perforation occurred in 12 cases and 1 case respectively. No ureteral rupture or tearing were not observed. After the operation, fever and ipsilateral low back pain were observed in 58 cases and 47 cases respectively, which were cured by the additional antibiotic and drug treatment. During the follow-up period, gross hematuria (540/784,68.88%) is the main common post-operative complication, most of which are improved significantly after conservative treatment. Renal subcapsular hematoma after the FURSL operation were identified in five patients, which was cured after symptomatic treatment such as antibiotic and hemostasis. The incidence of septic shock was very low and only 5 cases occurred, who recovered after active and effective treatment in intensive care unit (ICU). All patients received the KUB examination at 1 day and 1 month postoperatively respectively. Also, non-contrast CT or urinary system ultrasound was performed in all patients at 1 month after the operation. No patients were lost to follow-up. The SFR of one day and one month postoperatively were 66.2%and 92.5%respectively. Compared to 1 day postoperatively, the SFR were significant high at 1 month postoperatively (P < 0.05).
The follow-up data were showed in the Table 3. Three months after operation, 746 cases were followed up and 38 patients were lost due to various reasons. Three months after operation, there was 700 (93.8%) cases and 46 cases (6.2%) in stone clearance group (Fig. 1) and residual stone group (Fig. 2), respectively. In the residual stone group, 25 cases were re-treated with the FURSL, 10 cases and 21 cases were treated with ESWL and observation respectively after removal of double J stent. The diameter of stones in the stone clearance group and the residual stone group were (1.6±0.3) cm and (2.1±0.8) cm, respectively, which show the significant difference(P < 0.05). There were 608 (81.5%) and 21 (2.81%) cases with stones less than 2 cm in diameter, and 92 (12.33%) and 25 (3.35%) cases with stones more than 2 cm in diameter in both groups, respectively. The difference between two groups was statistically significant(P < 0.05). Meanwhile, there were 81 cases (11.57%) and 38 cases (5.43%) of lower calyceal calculi, 619 cases (82.98%) and 8 cases (1.07%) of non lower calyceal calculi in stone clearance group and residual stone group, respectively, which showed the significant statistically difference (P < 0.05).
Follow-up of 746 patients three months postoperatively
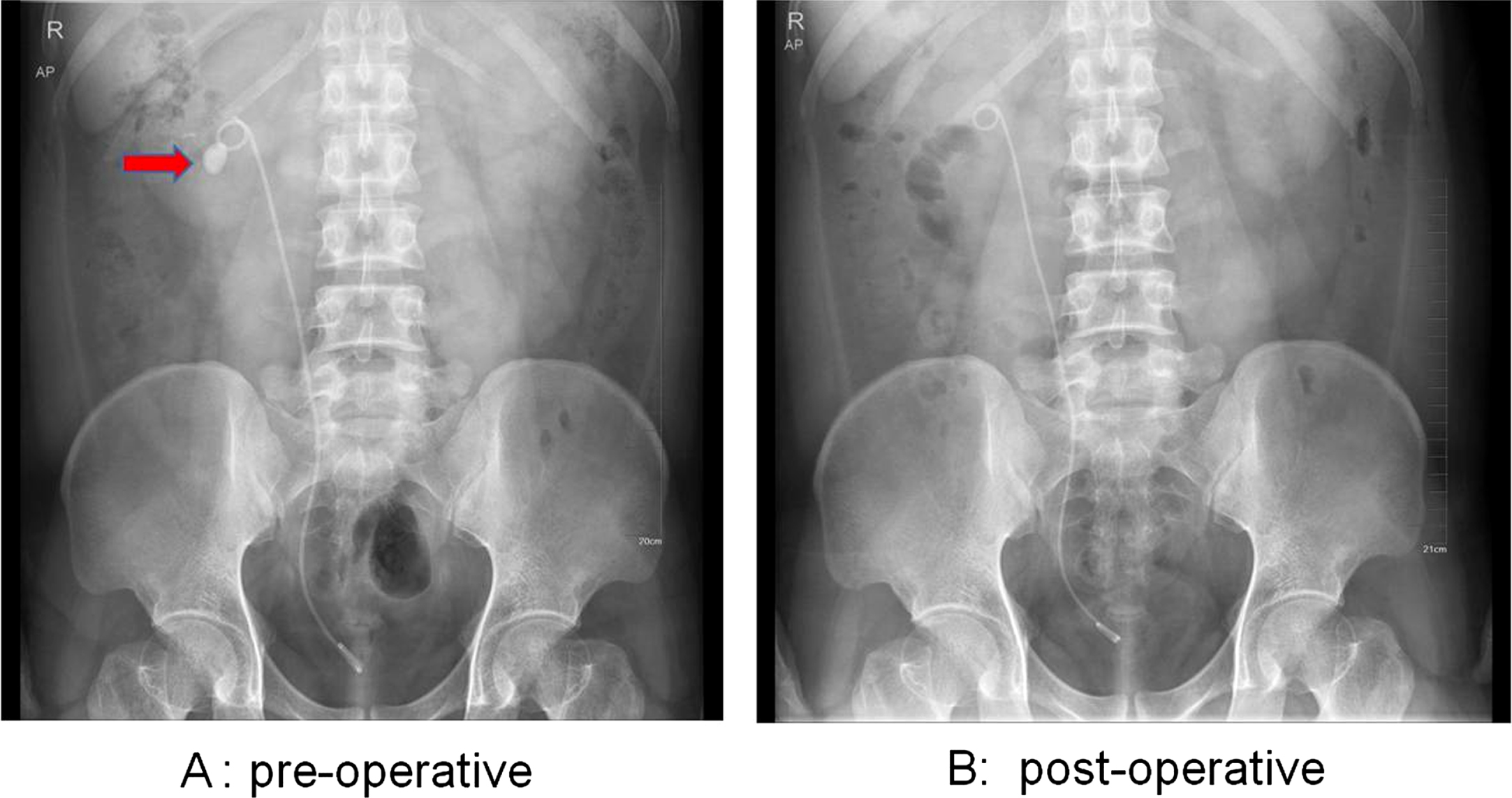
Stone clearance group (A) The stone was located at the right renal pelvis in the KUB plain before operation (red arrow). B: Compared with the pre-operative, the stone were completely removed. No stones were observed in the KUB plain.
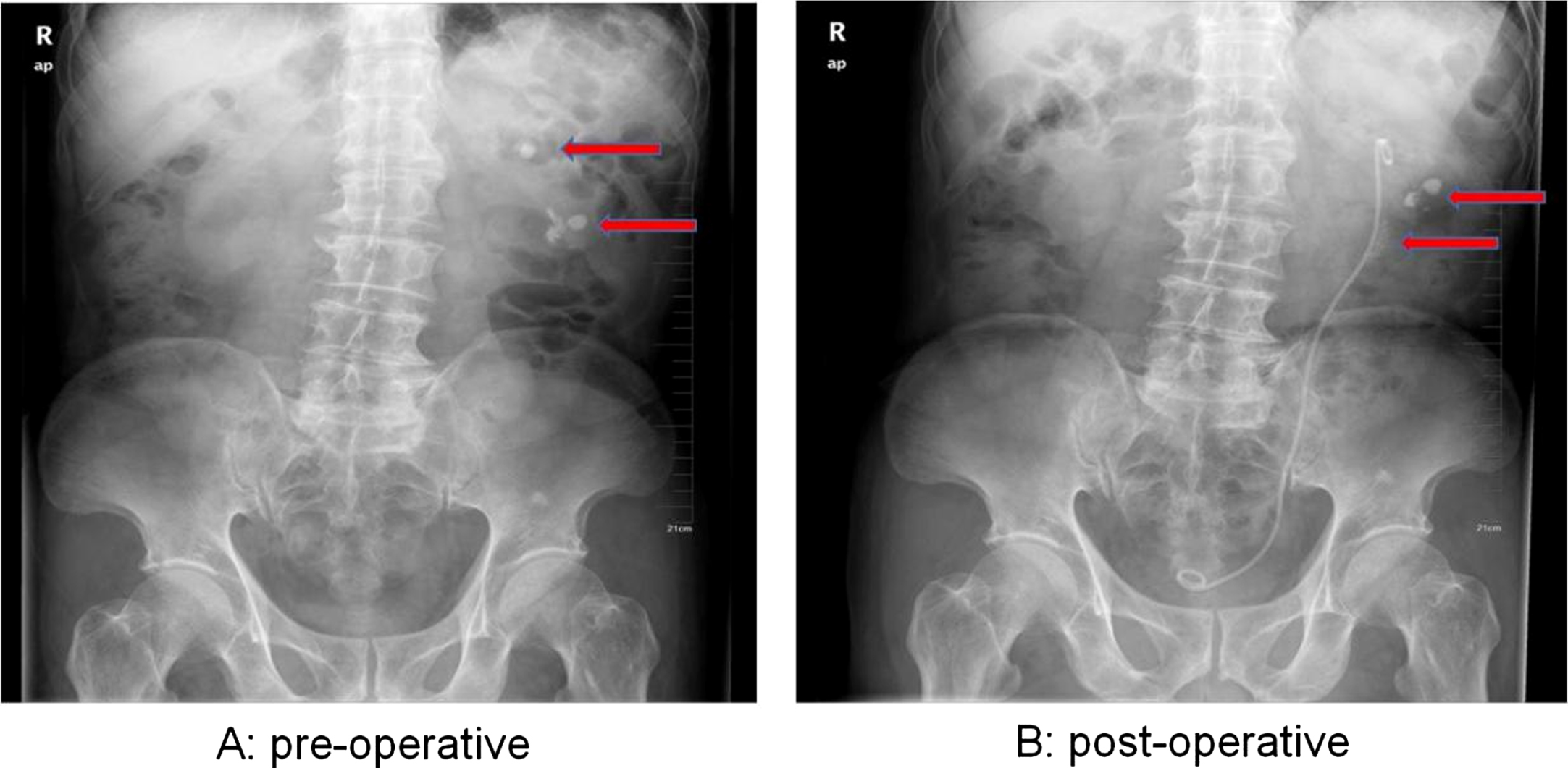
Residual stone group (A): The stones were located at the upper and lower renal calyces in the left kidney before operation (red arrow). (B): Compared with the pre-operative, the upper calyceal stones were completely removed after operation. On the contrary, residual renal calyceal stones were observed in the KUB plain (red arrow).
In recent years, flexible ureteroscopy has become more minimally invasive, effective and safe endoscopic surgery for upper urinary tract calculi and renal stone. FURSL has been performed at many hospitals worldwide due to the acceptable SFR and limited invasiveness, and it was recommended by European Association of Urology as the first choice for the removal of renal stone < 2 cm and alternative method for the removal of stone > 2 cm in patients with contraindications for PCNL [1]. Advances in technologies such as the development of new flexible ureteroscopes and small diameter effective lasers have made FURSL an efficient and safe option to manage urinary stones [16]. At present, flexible ureteroscopy is used widely, but there are still some clinical problems to be solved.
Before the operation, the characteristics of stone (size, number, density, location) and morphological structure of renal collecting system should be considered first. In our study, we evaluated the characteristics of stones and the structure of collecting system preoperatively through non-contract CT examination and intravenous urography of urinary system and excluded the patients who were not suitable for FURSL. We focused on the influence of stone size, burden and location on FURSL. According to the guideline, ESWL and FURSL are the first-line treatment for the stone of non-renal lower calyx less than 2 cm, and for the renal stone larger than 2 cm, PCNL is the first-line treatment. Our present study showed that the overall effect of treatment in < 2 cm stone group is superior to it in > 2 cm stone group. In addition, for the patients with high stone burden, FURSL would prolong the operation time and increase the risk of surgery. In our study, we adjusted the holmium laser parameters during the operation according to the density and burden of stones. For the patients with high stone density and burden, we usually used high-energy and low-frequency to make the stone fragment first, then we used high-frequency and low-energy to make the fragmental stone dust. Many studies [17–19] have showed that for the less than 2 cm renal stones, the post-operative stone-free rate of RIRS was higher and re-treatment rate was lower, and the complications were not increased significantly. For the patients with > 2 cm renal stone, the study [11] also have showed that FURSL can successfully treat patients with a high stone-free rate and a low complication rate, and with an average of 1.6 procedure per patient, which could be an alternative therapy to PCNL. In our study, majority of patients with stones less than 2 cm, which is related to our preoperative selection of patients, for large stones, we need to further study to confirm its effectiveness and safety.
The location of stone is another important aspect that we need to consider. At present, the treatment of renal lower calyx stones is still challenging and the techniques of FURSL, ESWL and PCNL have their own advantages and disadvantages. For renal lower calyx stones, PCNL has a high stone free rate, but the incidence of complications is high, such as bleeding, long post-operative hospital stay. The main advantage of ESWL is non-invasive and convenience, however the main disadvantage of it is low stone free rate and high incidence of retreatment, especially for renal lower calyx stone. Base on higher SFR and fewer complications of FURSL, more and more patients with renal stone take it as the first choice of treatment. As we know, infundibulopelvic angle (IPA) is the most important factor in the FURSL procedure, when the IPA < 30°, the success rate of operation and stone free rate will decrease significantly in renal lower calyx stones [20]. Guven [21] reported that in their 1112 patients, residual stones in 276 cases (24.8%) following the first RIRS session; out of these, 121 patients (39.4%) required a second active intervention. Residual fragments were on average 8.36 mm and located in the lower pole calyces (55%) of the treated kidney. In our study, the effect of FURSL in the treatment of non-renal lower calyx stone was also better than that of renal lower calyx stone significantly. For renal lower calyx stones, we usually moved the stones to the upper and middle calyces by the basket and then the stones were broken by holmium laser. However, in the patients with renal lower calyx stone, when IPA < 30°, the stone was difficult to move and break, which result in the stone free rate is decreased significantly.
Stent placement before FURSL can theoretically expand the ureter to improve access and remove stones. Even if current guidelines [22] suggest that routine stenting before ureteroscopic procedure is not necessary, several studies [23] have showed preoperative stenting improves the stone free rate, reduces intra-operative complications and facilitates the placement of uretaral access sheaths. In our study, stent placement was undergone regularly before operation in most of the patients, which increased the success rate of the FURSL procedure. In recent years, with the increasing experience, there are some patients in our unit, especially female patients who did not place stent before operation. Our present study has showed that the preoperative ureteral stenting had no significant effect on operative outcomes or complications such as SFR, operative times and perioperative complications, which is similar to previous study [24].
In this study, hematuria, fever and low back pain were the most common postoperative complications. Among these patients, septic shock and subcapsular hematoma occurred in five patients respectively, and no serious complications were occurred such as ureteral degloving and rupture. We analyzed that it is related to the long operative time, high stone burden and the patients, own condition. All these patients were cured after active treatment. In a prospective study of multiple centers [25], the overall incidence of postoperative complications was 3.5%(416/11885), most of which were Clavien-Dindo grade I or II. Only 0.2%of the patients needed blood transfusion and five patients died within 30 days after operation, and the readmission rate within 3 months after operation was 8.4%. Most of the patients were mainly due to mild abdominal pain and discomfort of ureteral stent. Cindolo [26] first described six cases of mortality after FURSL. Then, they also analyzed outcomes of 12 patients with major complications after FURSL. Eight patients developed a renal injury, one an arteriovenous fistula, two a ureter avulsion, and one acute sepsis; artery embolization and surgical repair were successful in six patients whereas the other half underwent open nephrectomy [27]. In our study, all patients with the serious complications were cured after active treatment and no patients were died due to the FURSL. Therefore, we believe that FURSL is a safe treatment for the upper urinary tract calculi.
However, the main limitation of FURSL is represented by treatment resulting in residual small fragments that may prompt subsequent stone events. The purpose of the procedure is to remove the stone completely, but the stone free rate cannot reach 100%. Treatment of renal and ureteral stones varies widely. Thus, achieving true stone-free status in all patients is still difficult. Moreover, imaging used to assess residual fragments following procedure impacts the diagnosed stone-free rate percentage considerably. In particular, the use of computed tomography scans has led to a better evaluation of residual fragments as well as so-called clinically insignificant residual fragments, which in a considerable number of cases are, despite their definition, causes of adverse urological events, thus creating a thorny problem for both patients and urologists [28]. Different laser setting can lead to stone dusting and fragmentation. The dusting technique require low energy and high frequency to make the stone to tiny fragment sizes that can pass spontaneously. On the contrary, high energy and low frequency can result in fragments which can be extracted by endoscopic baskets. El-Nahas [29] retrospectively reviewed outcomes of 107 consecutive patients undergoing FURSL using either the dusting (N = 51) or the fragmentation and retrieval techniques (N = 56). Both techniques showed comparable safety, hospital stay and requirement for secondary procedures, but the dusting technique had a significantly shorter operation time while the fragmentation and retrieval technique had a significantly better SFR. In our study, the SFR of FURSL is 92.5%, which is similar the previous studies, we considered that it were related to most stones are located in the upper middle calyx of the kidney and the stone diameter is less than 2 cm. Except that, we use the technique of dusting and fragment, the fragments could be removed by the baskets and the dusting would pass out of the body spontaneously. During the follow-up, the effect of stone removal was satisfactory and most of the patients obtained the good therapeutic effect.
In addition, we also observed that about one fourth of the patients had residual stones less than 4 mm, and according to our criterion, we think it as meaningless stone. The previous study [30] shows that among patients with post-ureteroscopic renal stone fragments < 4 mm, approximately one in five (or 19.6%) will experience a stone event over the following 1.6 years. The remaining patients will either become stone-free via spontaneous passage or retain asymptomatic stable-sized fragments. Thus, meaningless stone does not represent no stone, no matter how small the stone is, there is a certain risk. The current study [31] show that the SFRs at postoperative day 1, 30 in suctioning UAS group are higher than it in the traditional UAS group. We look forward to investigating and identifying whether there may be more ways to remove stones in the future.
Conclusion
At present, FURSL has been widely used in the treatment of upper urinary tract calculi. With high efficiency and low incidence of complications, this technology has become a reliable method for the treatment of small and medium stones in upper urinary tract. However, there are some limitations in the treatment of large stones and lower calyceal stones. Lower calyceal stones are an independent risk factor for the efficacy of FURSL. The shortcomings of this study are single center retrospective study, no control group, lack of long-term follow-up data. It still needs the large sample and multi-center study to further verify the efficacy of FURSL in the treatment of upper urinary tract calculi.
Conflict of interest
No
Inform consent
No
Ethics approved
No
Funding Sources
No
Data availability statement
All data generated or analyzed during this study are included in this article [and/or] its supplementary material files. Further enquiries can be directed to the corresponding author.
Author contribution
Tao Wei: Data Collection, Manuscript writing
Xu Ming: Data Collection
Zang Yachen: Data Collection
Zhu Jin: Data Collection
Xue Boxin: Project development
Sun Chuanyang: Project development
All authors read and approved the final version of the manuscript