
Abstract
BACKGROUND:
Due to the limited temporal resolution and cardiac motion, coronary computed tomography angiography (CCTA) exam is one of the most challenging CT protocols which may require operating radiologist to apply additional phase adjustment or motion correction for image reconstruction.
OBJECTIVE:
To evaluate image quality between automatic and manual CCTA reconstruction in a 0.25 second rotation time, 16 cm coverage, single-beat, CT scanner with automated phase selection and AI-assisted motion correction.
METHODS:
CCTA exams of 535 consecutive patients were included. All exams were first reconstructed with an automatically selected phase. If there was an unacceptable motion artifact, a manual reconstruction process was performed by radiologists. Additionally, automatic image series which consist of auto-phase selection and a follow-up motion correction were reconstructed. For these two manual and automatic image series, a four-point Likert scale rating system was used to evaluate image quality of the coronary artery segment by two experienced radiologists, according to the 18-segment model.
RESULTS:
Fifty-one patients (9.5%) did not have satisfactory image quality after auto-phase selection. In these patients, the heart rate during scanning was higher (78.3±18.4 bpm) than in the remaining 484 patients (68.9±13.1 bpm). Overall, 734 out of the 918 vessel segments were identified for quality evaluation among 51 patients. Automatic and manual image series were rated as having average Likert scores of 3.48±0.62 and 3.32±0.67 (P < 0.001), respectively.
CONCLUSIONS:
Using a 0.25 second rotation speed, 16 cm z-coverage, CT scanner installed with an AI-assisted motion correction algorithm, the automatic image reconstruction with scanner equipped auto-phase-selection and motion correction algorithm outperforms manually controlled image reconstruction by radiologists. This suggests that the traditional CCTA exam reconstruction workflow could be altered allowing less radiologist involvement and becoming more efficient.
Keywords
List of abbreviations
Coronary computed tomography angiography
Beats per minute
Single source CT
Right coronary artery
Left circumflex artery
Left anterior descending artery
Left main artery
Invasive coronary angiography
Artificial intelligence
Effective dose
Introduction
Coronary computed tomography angiography (CCTA) has become a routine and noninvasive imaging method for coronary artery disease diagnosis [1–5]. But a CCTA exam is also one of the most challenging CT protocols due to cardiac motion. It was estimated that less than 19 ms scan time (temporal resolution) is required to avoid any cardiac motion artifacts [6, 7]. Currently however, CT temporal resolution is still limited by the CT gantry rotation speed which is hard to improve due to mechanical capability. Thus, to achieve diagnostic image quality with reasonable radiation dose, several techniques were developed. At first, Data acquisition is controlled by ECG (Electrocardiogram) gating at cardiac cycle with least motion which normally locate at systole or diastole phase. To further improve temporal resolution and reduce motion artifacts, motion correction algorithms may be required. This makes CCTA exam one of the most complicated CT protocols.
In general, for 16-cm-coverage wide detector scanner, single-beat cardiac scan consists of two steps –phase selection and motion correction. After data acquisition, radiologist will select a reconstruction phase with lowest motion artifacts. Even with automatic phase option in most commercial CTs, radiologist often needs to visually check the image quality and adjust reconstruction phase because radiologist cannot determine whether the artifact is due to sub-optimal phase or just temporal resolution limit. After this subjective and time-consuming procedure, radiologist will then determine whether further motion correction is needed. In this situation, whether to choose additional phase adjustments or motion correction depends on experience of the operating radiologist [4]. This makes image quality of CCTA vary between different clinics and radiologists. Thus, workflow simplification and standardization are required for CCTA exam.
Recently, a newly-developed 320 row scanner was introduced with 0.25 s rotation time (temporal resolution 125 ms). At the same time, a new generation of AI-based motion correction was developed with improved correction quality and computing efficiency. We hypothesized that due to the combination of all these developments, CCTA reconstruction can be performed more automatically. For high heart rate patients (> = 75 bpm), it was found that image quality was diagnostically sufficient by simply using auto-phase selection and motion correction [8]. But, until now, no direct comparison had been carried out between automatic and manual reconstruction.
Thus, the objective of this study is to investigate the feasibility of one-stop automatic CCTA exam on the general patient base using 320 row CT with 16 cm z-axis coverage and 0.25 s rotation time. For this purpose, we compared the image quality between automatic and manual CCTA reconstruction images.
Materials and methods
Study population
This prospective study was approved by the Ethics Committee of Zhongshan Hospital (Shanghai, China), and written informed consent was obtained from all participants before the commencement of the study. All exams were carried out in accordance with relevant guidelines and regulations.
From May 2020 to December 2020, 535 consecutive patients, regardless of heart rate during the CT scan, were included in this study. Exclusion criteria included a past history of allergy to the iodinated contrast agent, pregnancy, and bypass graft surgery. All exams were first reconstructed with an automated phase option. Then, a radiologist (with 10 years of experience in CCTA exam) evaluated the image quality. If there were no apparent motion artifacts and the image quality met diagnostic requirements, this patient was classified as Phase-Good. If the radiologist determined that a further reconstruction procedure was required, this patient was classified as Phase-Poor. An image quality comparison between automatic and manual reconstruction was carried out in the Phase-Poor patients. The recruitment procedure is illustrated in Fig. 1.
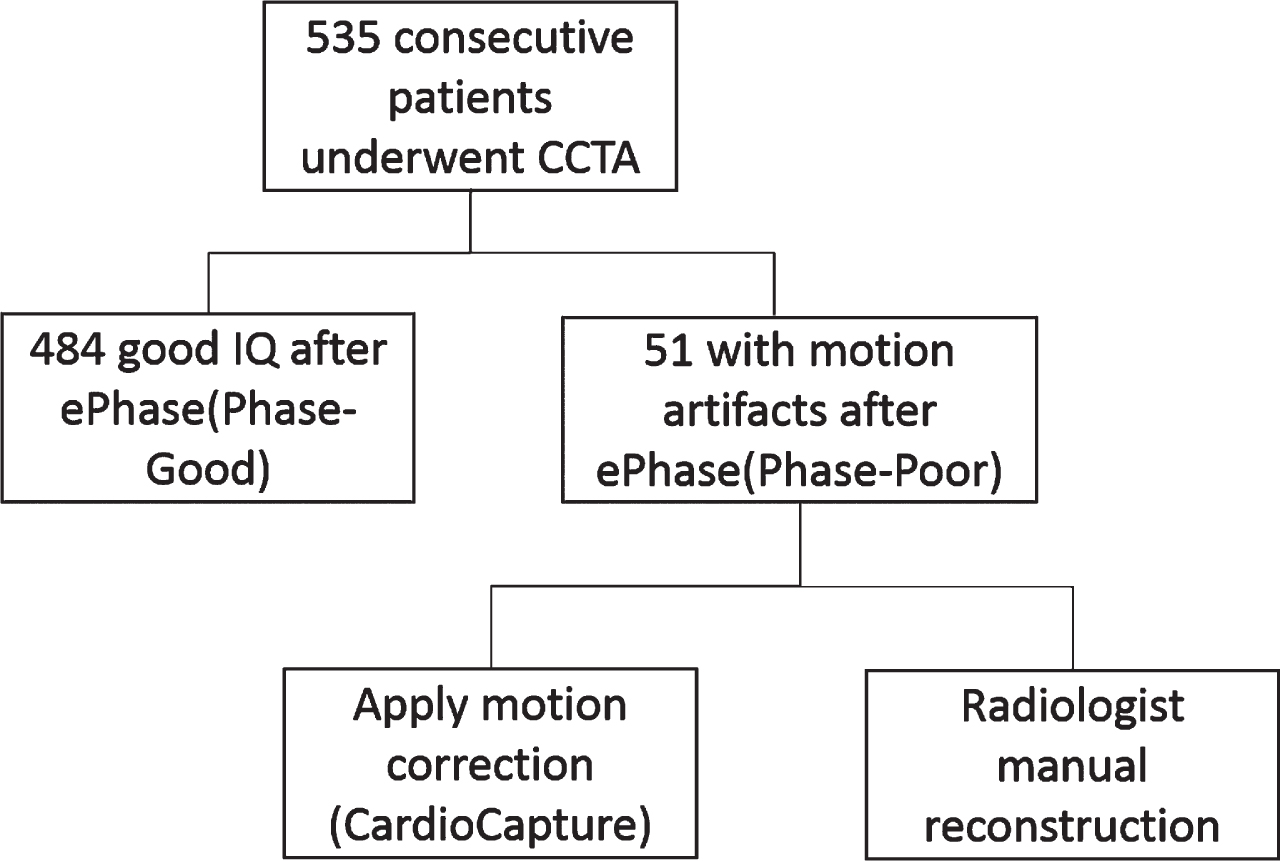
Flowchart for classification of the 535 enrolled patients.
All examinations were performed on the 320-row detector CT scanner (uCT 960+, United Imaging Healthcare) with prospectively electrocardiograph triggering in a single heartbeat. Scanning parameters were as follows: z-coverage was 12 cm, 14 cm, or 16 cm depending on the patient’s heart size; reconstruction matrix size was 512×512 pixels; gantry rotation time was 0.25 second; tube voltage was 100 kV; and tube current was determined by a dose modulation (DOM) technique. A medium body prepatient X-ray filter was used with a scan field view of 420 mm to minimize the radiation dose. The display field-of view (DFOV) for the image reconstruction was 200 mm with an image slice thickness and increment of 0.5 mm. Data acquisition was triggered using a bolus-tracking technique, which started 6.0 sec after the attenuation value in the descending aorta became higher than 110 Hounsfield units. Data acquisition covering 30–55% of the R-R interval was carried out for HR > 75 bpm, 30–80% for 65 < HR<75, 65–80% for HR < 65 and 30–80% for arrhythmia. Non-ionic contrast media (iopamidol, 370 mg iodine/ml, Bayer) was injected at a rate of 4–5 ml/s via the median cubital vein, at a dose of 0.7 ml/kg of body weight and followed by 20 to 30 ml of saline solution. The dose and flow rate of the contrast agent were determined by the body mass index and vein condition. All selected patients were treated with oral metoprolol 1–1.5 hours before the examination and sublingual nitroglycerine just before scanning.
Image reconstruction
All images were reconstructed using the algorithm with commercial hybrid iterative reconstruction (KARL3D, United Imaging Healthcare) at level 3 for reducing image noise. After data acquisition, an optimal phase could be selected using the ePhase function which is based on coronary quality evaluation and measuring the image differences between phases [9]. To further improve temporal resolution, a novel AI-assisted motion correction option, CardioCapture, further reduced the remaining motion artifacts even at optimal phase. Some details of the algorithm was described in reference [8]. For Phase-Poor patients, two follow up reconstruction procedures were carried out. First, a routine manual cardiac reconstruction procedure was performed by one operating radiologist (with 10 years of experience in CCTA exam and diagnosis). In the manual reconstruction, radiologist will first try to find the optimal reconstruction phase. He/she will choose one slice image which has apparent motion artifact at default or auto-selected phase reconstruction and use Cardiac CT scanner provided ‘phase preview’ function which reconstructs several neighboring phases at selected slice position (as in Fig. 3). Then radiologist selects the least motion artifact phase within the preview images and reconstructs the whole volume images for final verification. This procedure may be repeated for several times. After selecting the optimal phase, if there still exist motion artifacts, final motion correction will be applied. Second, an automatic reconstruction including motion correction was directly applied to the auto-phase selected images.
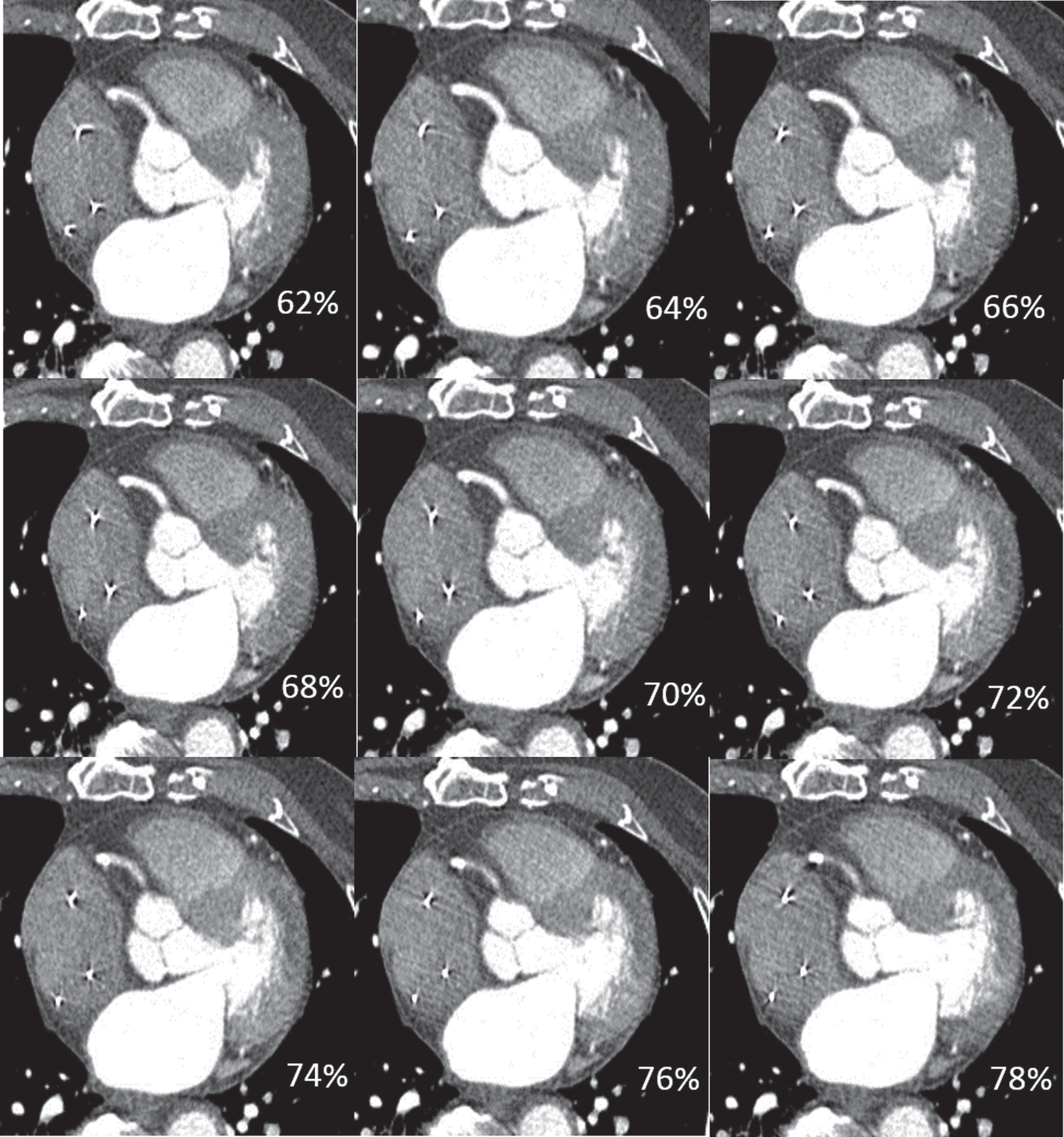
Images of a 93 years old man with pacemaker, 60 bpm at scanning, arrhythmias (41–113 bpm). According to the heart rate characteristics at scanning, the reconstruction preview phase was centered at 70%, and the time frame was extended to each side by 4 phases. Finally, the radiologist chose 72% phase for reconstruction.
The effective radiation dosage of CCTA was calculated in millisievert using a modified CT dose index volume specific for the CT scanner: the estimated effective dosage was calculated as the dose-length product times a conversion factor for the chest k = 0.014 (mSv / [mGy×cm]) in adults [10].
Image evaluation
In addition to the operating radiologist, two independent radiologists (with 8 and 11 years of experience in CCTA diagnosis) who were blinded to the reconstruction algorithms assessed the image quality of the coronary segments. Image series of automatic and manual reconstructions were assessed in a random order after an interval of 2 weeks to reduce reader bias. Coronary artery segments with a diameter of 1.5 mm or more were evaluated according to the 18-segment model, which is defined by the Society of Cardiovascular Computed Tomography [11].
Accordingly, a 4-point grading scale system was used to evaluate the image quality [4, 12]. Score 1 denotes non-diagnostic image quality (severe artifacts with inadequate delineation between the lumen and the surrounding tissue); Score 2 denotes adequate image quality (noticeably blurred vessel, but acceptable for diagnosis); Score 3 denotes good image quality (blurring of vessel margin and minor artifacts, fully evaluable); and Score 4 denotes excellent image quality (with the absence of artifacts). The coronary segment was considered non-diagnostic when the score was 1 and diagnostic from 2 to 4. For the final statistical analysis, a consensus was reached after negotiation between the two radiologists if they originally differed on their scoring.
Statistical analysis
Statistical analyses were performed by SPSS software (version 22.0; SPSS, Chicago, Ill). Data are presented as means±their standard deviation. The Kolmogorov-Smirnov test was used to test whether the data were normally distributed. McNemar’s test was used to analyze the statistical significance of the differences between paired proportions. The χ2 test was used to evaluate proportions of categorical data. The Student t test was used to compare continuous variables. Inter-observer agreement between the two radiologist readers with regard to subjective image quality score was evaluated with the Cohen k test by using the following scale: k values of less than 0.20 were indicative of poor agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, good agreement; and 0.81–1.00, excellent agreement.
Results
Study population
In total, 535 consecutive clinical coronary CT angiography examinations were included in this study. Table 1 describes the clinical characteristics of the 535 patients. They are divided into two groups according to Fig. 1. No significant differences were found between the Phase-Good and Phase-Poor groups in terms of age, sex, BMI, HR variability and dose. The heart rate during scanning is higher in the Phase-Poor group (78.3±18.4 bpm) than in the Phase-Good group (68.9±13.1 bpm). In Fig. 2, we plot the HR distribution for the two groups.
Patient Characteristics
Patient Characteristics
*PG = Phase-Good, PP = Phase-Poor.

HR histogram of Phase-Good and Phase-Poor group. Curves are fitted to a normal distribution
In the 51 phase-poor patients, 732 out of the 918 segments were evaluated with 186 (20%) of the segments (diameters < 1.5 mm) being excluded. For automatic reconstruction, among the 732 segments, 731 segments (99.9%) were rated as having diagnostic image quality (scores 2–4) and the average score was 3.48±0.62 (Table 2). For manual reconstruction, there were 730 (99.8%) diagnostic segments with an average score of 3.32±0.67. The kappa k values between the two radiologists were 0.71 and 0.73 for automatic and manual reconstruction, respectively. Table 3 summarizes the scores in four major vessels (RCA, LM, LAD, LCX) and other remaining vessels. RCA and LM show no significant difference between the two reconstructions for p value 0.078 and 0.442, respectively.
Segment number for each image quality scores for automatic and manual reconstruction (total 732 segments)
Segment number for each image quality scores for automatic and manual reconstruction (total 732 segments)
Score statistics of four major vessels and other vessels for automatic and manual reconstruction
In LAD, LCX and other remaining vessels, automatic reconstruction had better image quality than manual reconstruction (p < 0.001). Specifically, 151 segments have higher or better image quality and 49 segments were worse in automatic reconstruction than manual reconstruction at segment base. At patient base, 37 patients were better and 11 were worse in automatic reconstruction.
In Figs. 3–5, we show a case in which automatic and manual reconstruction gave similar final image quality. Initially, ePhase selected the best phase 55% but the image quality was considered non-diagnostic by the radiologist. Then, according to the heart rate characteristics of the patient, the radiologist tried to use phase preview to select a better phase and previewed a reconstruction phase centered at 70%. 72% was selected, but it still had severe motion artifacts. Finally, CardioCapture was applied to both the automatically and manually selected phases. The final reconstructed image series were rated at the same image quality score and diagnostic value.
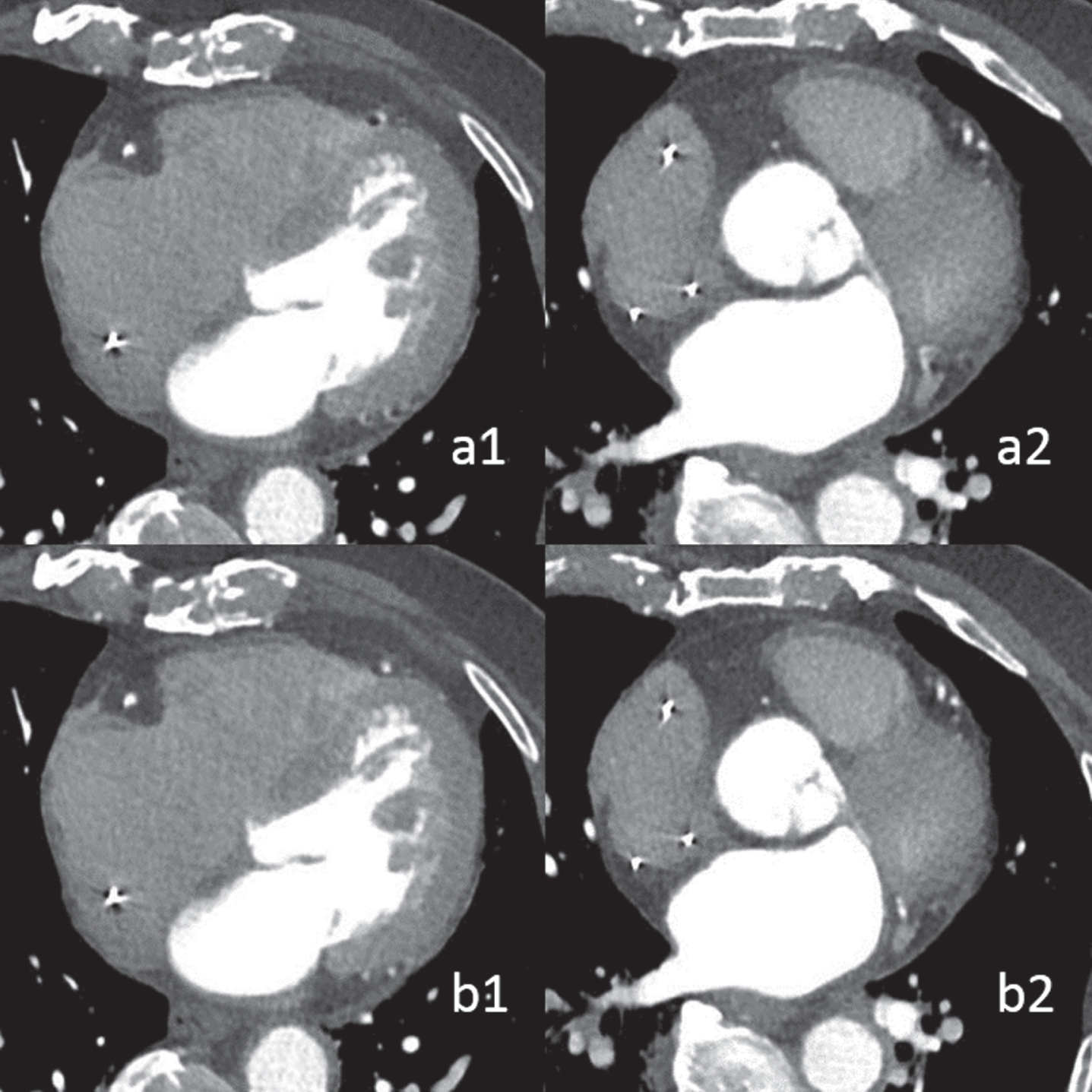
a1: Automatically selected 55% phase. The edge of the mid-LAD and mid-LCX was blurred, which cannot meet diagnostic needs. a2: Radiologist-selected 72% phase reconstruction, mid-LCX was still blurred, and non-diagnostic with score 1. b1: image after motion correction based on 55% phase(a1), motion artifacts in the LAD and LCX disappeared, the edges were clear, sharp with score 4, and the remaining coronary arteries were diagnostic. b2: image after motion correction based on 72% phase(a2), mid-LCX was clear, the edge was sharp without artifacts, the score was 4 points. The remaining coronary arteries were diagnostic.
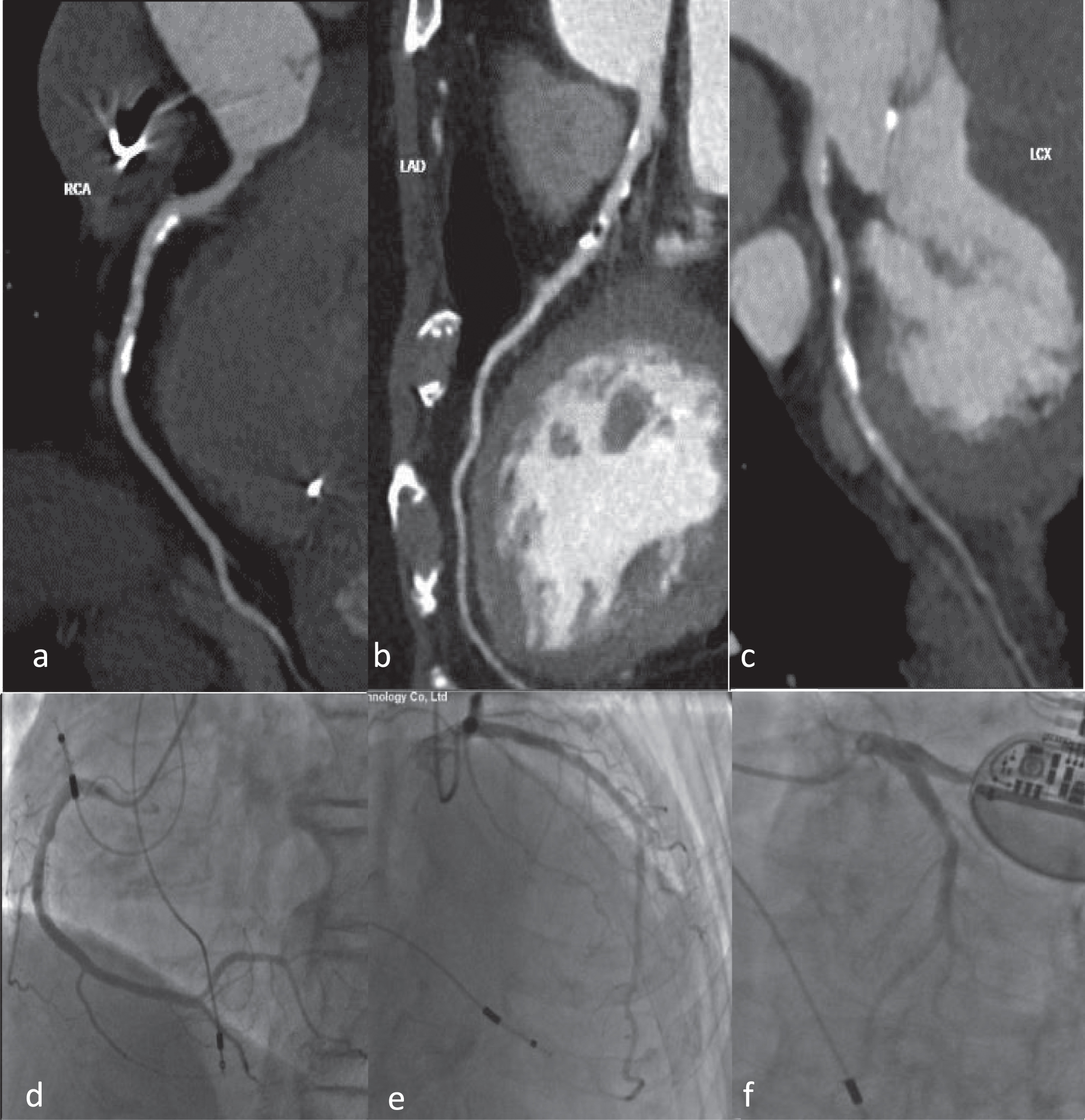
In this example case, 40% stenosis was diagnosed in mid-RCA (a) and 30% confirmed by ICA(d); 70% stenosis was diagnosed in proximal LAD(b) and 60% confirmed by ICA(e); 30% stenosis was diagnosed in mid-LCX(c) and 20% confirmed by ICA(f).
Our study demonstrates that combining automatic phase selection (ePhase) and AI-assisted motion correction (CardioCapture) results in the image quality of the automatic reconstructions averaging slightly better than that of the manual reconstruction. Our study statistics showed that about 90% (484/535) could have diagnostic image quality at optimal phase reconstruction which indicates that 125 ms temporal resolution (0.25 s rotation time) is sufficient for most patients having a CCTA exam. The remaining 10% of the patient population require better temporal resolution. We also found that a number of patients (28 of 51) below 75 bpm were still Phase-Poor and would need further motion correction. This suggests that heart rate is not the only factor determining the cardiac motion intensity.
In current routine CCTA exams, when there are some motion artifacts in the images after default or automatic phase reconstruction, the radiologist will first try to find a better reconstruction phase. The challenging Phase-Poor cases could be divided into two categories: one segment moving faster than scanner temporal resolution and two or more segments moving asynchronously. For the first case, because the radiologist normally chooses to look at only one slice position during phase preview, it is difficult for them to evaluate the overall best phase of the entire cardiac vessel structure. Thus this ‘optimal’ phase is subjective. In contrast, the computer could be more ‘objective’ and determine the image quality using the whole artery vessel base efficiently. For the second case, it will be hard for a radiologist to balance between the two segments. In most situations, the radiologist will pay more attention to main or large vessels. This could explain why automatic reconstruction showed higher score advantage in LAD, LCX and other vessels than manual reconstruction. However, for both above cases, motion correction could improve temporal resolution and remove the artifacts on the whole coronary artery base. To our knowledge, manual radiologist image assessment and phase adjustment during a CCTA exam is still the first choice of radiologists in general clinical practice. Thus, CCTA image quality is highly dependent on experience of technician or radiologist. In this sense, with increasing computing power and more efficient AI algorithms, motion correction should be routinely applied in all CCTA exams to improve the CCTA exam workflow. In Fig. 6, we illustrate the proposed workflow in which motion correction is always applied for the initial image assessment. We believe the proposed workflow could improve the CCTA exam in the three aspects: efficiency of CCTA exam, standardization of CCTA image quality and disease detection of the whole coronary arteries even for small vessels.

The proposed CCTA workflow in which motion correction is directly applied after automatic phase selection.
There were several previous works which focused on automated phase selection for dual-source or single beat CT scanners [13–15]. They were mainly focused on the general population base where most patients already had satisfactory image quality after optimal phase reconstruction. However, our current study focused on more challenging cases. In comparison with several previous studies, using a whole-heart coverage scanner, phase selection before motion correction was often done by an experienced radiologist [4] or details for phase selection were not provided [2, 5]. In one study, the best cardiac phase and motion correction were both applied but this study focused on lean patients and 70 kVp image quality [16, 17].
There were some limitations to this study: First, our patient classification between Phase-Good and Phase-Poor was subjective and based on the experience at a single institution. Furthermore, sample size of the Phase-Poor patients which needed radiologist involvement in our study was not quite as large as we would have liked. These factors could influence the population fraction which need further reconstructions and the image quality score. Second, due to the limited number of challenging patient cases, a diagnostic accuracy study with ICA comparison was not performed but should considered important future research. However, according to some previous studies [1, 5], the image quality score should be well correlated to the diagnostic accuracy. Third, we did not quantitatively or qualitatively compare image quality between automatic and manual selected phases. This could influence image quality after motion correction. According to the principle of motion correction algorithms, correction quality could depend on the selected phase. Further studies are expected regarding this.
In conclusion, with the combination of rotation speed (0.25 sec rotation time), automatic phase selection and AI-based motion correction algorithm, most patients will meet diagnostic image quality requirements with proper phase reconstruction selected by computer. Some challenging patients could be resolved by motion correction based on an automatically selected phase. In this sense, the workflow of these challenging CT exams could be simplified to improve both the patient experience and diagnostic accuracy.
Footnotes
Acknowledgments
This study has received funding by National Natural Science Foundation of China (grant number 91859107); National Natural Science Foundation of China (grant number 82171897); Shanghai Science and Technology Committee (grant number 19411965500); Clinical Research Project of Zhongshan Hospital, Fudan University (grant number 2018ZSLC22).
Conflict of interest
The authors declare that they have no conflict of interest.