
Abstract
PURPOSE:
Voluntary deep inspiration breath hold (v-DIBH) reduces cardiac dose during left-sided breast irradiation. The purpose of this study is to evaluate the reproducibility and variability of breath-hold level (BHL) using breath-hold curves and lateral kV setup images together.
MATERIAL/METHOD:
A retrospective analysis of 30 left breast cancer patients treated using the v-DIBH technique in our department is performed. The BHL difference is measured from breath hold curves and lateral (LAT) kilo-Voltage (kV) setup images. The planning CT image and the selected treatment fraction data are collected. If the changes in BHL relate to the displacement of various bones in the kV setup, images are assessed. Furthermore, the maximum heart distance inside the treatment field is compared from LAT MV portal images.
RESULTS:
The median and mean values of the BHL are nearly identical in different fractions (good reproducibility). However, the mean BHL values between planning and all measured fractions are statistically different; 16.3 vs. 20.8 mm for the planning and measured fractions (p < 0.001), which indicates that the variability of BHL is significantly different.
CONCLUSION:
While reproducibility testing shows good agreement for inter-fractional breath-hold level, the variability between planning and fractions is relatively poor.
Keywords
Introduction
Breast cancer radiotherapy (RT) is one of the main treatment modalities for increasing survival and local control rates [1, 2]. Despite these advantages of adjuvant radiotherapy, applied as part of combined modality treatment in breast cancer, it also increases the rate of morbidity, particularly for left-sided breast cancer (LSBC) patients. The risk of cardiac disease is the most common toxicity resulting from breast irradiation [3–7]. Therefore, it is crucial to reduce the heart dose for LSBC treatment.
The heart dose is effectively reduced by the voluntary deep inspiration breath hold (v-DIBH) technique and as opposed to standard free breathing (FB) treatments. In the v-DIBH technique, the patient breathes in deeply, expanding the ribs and taking over the heart from the chest wall. As a result, v-DIBH became one of the methods used in left breast radiation therapy to reduce the cardiac dose.
Several studies have demonstrated the dosimetric advantages of v-DIBH treatments in reducing heart dose [8–12]. However, v-DIBH increases variability during treatment delivery, therefore it is essential to correctly reproduce the breath hold while undergoing treatment. The reproducibility of the v-DIBH is of great importance for applying RT safely. Although the dosimetric benefits of v-DIBH have been the subject of several studies, there are limited data available regarding the setup reproducibility of this method.
Several methods such as an active breathing control (ABC) system, three-dimensional (3D) optical tracking system, and real-time position management (RPM) system have been presented to monitor or control the reproducibility of respiratory motion during RT [13–20]. Furthermore, lateral (LAT) kilo-Voltage (kV) setup images and Mega-Voltage (MV) portal imaging have been used to determine positional variability on the breath hold level (BHL) [13, 14].
In our department, during both simulation and treatment, RPM is utilized to monitor v-DIBH and the patients are coached to hold their breath. In the RPM system, a marker block is positioned below the patient’s xiphoid process and two infrared reflectors in the room capture vertical displacement of the marker block throughout the respiratory. The movement of this device is the basis of reproducing the BHLs. Due to patient-derived factors (improved or decreased inspiration), breath hold levels (BHL) may vary between the planning computer tomography (CT) scan and the treatment. Therefore, the reference BHL needs to be re-verified in the treatment situation.
The present study aims to evaluate the set-up reproducibility and variability of v-DIBH utilizing breath-hold curves and lateral (LAT) kilo-Voltage (kV) setup images together in our clinical practice. The BHL differences were assessed between planning and treatment via breath-hold curves and by measuring the distance between the anterior surface of corpus vertebrae and sternum from lateral (LAT) kilo-Voltage (kV) setup images. In addition, we investigated whether the bony anatomy position variability was related to BHL by matching the setup images. Furthermore, maximum heart distance inside the treatment field was compared between planning and treatment from lateral (LAT) Mega-Voltage (MV) portal images.
Materials and methods
Patient data
Thirty patients left-sided breast cancer patients treated by RPM-based v-DIBH RT at our department were recruited for the present retrospective study. The selected patients received v-DIBH RT to their left breast only after breast-conserving surgery. Each patient’s breath-hold curves, kV setup images, and MV portal images were reviewed retrospectively.
Pre-treatment imaging
Before the planning computed tomography (CT) acquisition, patients were then asked to perform a comfortable v-DIBH. After a few training repetitions, the v-DIBH instruction was given to patients to make sure they can hold their breath for at least 15–20 seconds.
The planning CT was performed in a supine position with both arms raised above the head using the breast board. The Varian RPM system (Varian Medical Systems, Palo Alto, CA, USA) was utilized during the v-DIBH scan to start imaging and to monitor the length and displacement of breath-hold for each patient. A marker block with reflective markers was placed on the patient’s xiphoid process, perpendicularly facing the infrared tracking camera, to detect anterior-posterior respiratory movement. RPM system was configured with a verbal coaching method and amplitude mode. Since the absolute amplitude of breathing motion was monitored, it would change depending on the position of the marker block. Therefore, this position was marked on the patient for a v-DIBH CT scan and used for daily treatment.
The first step in the CT simulation procedure was to observe the patient’s respiratory pattern and breathing motion amplitude. With a 10 mm window range (5 mm on either side of the peak position), the target amplitude for deep inspiration was set at 1.0 cm above the peak of normal breathing amplitude (Fig.1.a). This setup was used for both planning CT scans and daily treatment. After setting up the amplitude threshold, the patient was instructed verbally to take a deep breath and hold it until the yellow bar becomes green. A horizontal blue bar represents the amplitude gating window (Fig.1.b). The reference BHL was defined from the total displacement of the marker block with the axial axis. Then, the patient was instructed to exhale and relax after 20 seconds. The v-DIBH image was acquired within a single breathing hold using a Philips Big Bore Brilliance CT scanner (Philips Medical Systems, Eindhoven, the Netherlands).

a) v-DIBH amplitude set-up is shown, the black line represents the patient’s free breathing respiratory pattern b) Breath-hold level (BHL) and the gating window are shown. BHL (black line) shows the displacement of the marker block with the axial axis. The CT simulation and treatment delivery were performed during a stable breath-hold period defined by upper and lower limits (blue and orange vertical lines, respectively). The gating window range was chosen as 10 mm (5 mm on either side of the reference BHL position). The numbers on the y-axis represent the location of the gating window concerning baseline level (maximal exhale in free breathing). The numbers on the x-axis represent the period time of breath-hold.
The breath-hold curve and gating window recorded during the simulation was used as the reference for breath-hold reproducibility throughout the treatment. Subsequently, the reference BHL was sent to the linear accelerator.
The Eclipse v11.4 treatment-planning system was used for contouring, planning, and dosimetric evaluation. Target volume (breast only) and organ at risk (heart, LAD, lungs, contralateral breast) were delineated according to the RTOG guidelines for each patient. Clinical target volume (CTV) of breast included the apparent glandular breast tissue and lumpectomy CTV, cranial boundary was clinical reference (using radio-opaque marker or radiologic images) or second rib insertion, clinical reference used as caudal boundary. Pectoral muscles, ribs and chest wall were excluded from posterior boundary. Contralateral breast contouring was the same as CTV breast contouring. Pericardium was included contouring of heart. Intravenous radio-opaque fluid was not administered during simulation computed tomography (CT), therefore contrast-enhanced CT was not used for LAD contouring. Patients were treated with a conventional fractionated (2 Gy in 25 fractions). All plans consisted of 3D conformal RT (3DCRT) plans using two opposing tangential beams for the whole breast, with the addition of 2 subfields to increase dose homogeneity.
Setup verification
For patient setup, treatment immobilization was the same as the planning CT immobilization. Initial patient positioning was performed by use of lasers and skin marks during normal breathing. After monitoring normal breathing, the patient was coached to achieve the set-up of v-DIBH from CT simulation by setting the amplitude target window range. 2D kilovoltage (kV) set-up images were obtained daily in breath-hold with an onboard imaging system (OBI) for the anterior-posterior (AP) and lateral (LAT) images. Also, the weekly image guidance with tangential megavoltage (MV) Electronic Portal Imaging Device (EPID) images were acquired before v-DIBH treatment. kV AP/LAT image sets and the MV tangential port film images were acquired and compared to the planning Digitally Reconstructed Radiographs (DRRs). Each tangential field was irradiated with Varian Trilogy using RPM.
v-DIBH reproducibility and data analysis
Patients were required to perform multiple breath-holds during v-DIBH treatment. The inter-fraction v-DIBH reproducibility was evaluated during the treatment. We have measured the breath-holds from the simulation and a total of 5 fractions during treatment. We have selected the fractions from each week of treatment. Each patient was treated with 2 tangential fields including 2 subfields each. Each field and subfields have separate breath holds. Therefore, a total of 930 breath-holds were figured out. The breathing amplitudes of all breath-holds of a patient were measured and compared to the planning BHL. In this study, the term ‘’reproducibility” was defined as a difference in BHL of each patient between fractions of the treatment. The ‘’variability ‘’ was determined as a difference in BHL between planning and fractions for the treatment of each patient.
Position errors between the vertebra and sternum on the lateral (LAT) kV images can be used to measure changes in the actual BHL. For image guidance, the lateral setup image was used. To determine the BHL, bony markers in the sternum and vertebrae were chosen. And the BHL variation was defined as the difference between these structures’ ideal matching in both the AP- and SI directions. The reproducibility of BHL was investigated from the distance between the sternum and the middle corpus of the vertebrae as presented in Fig. 2 (a), taking into account the movement of bony structures both in AP- and SI directions. A total of 180 LAT kV setup images were analyzed.
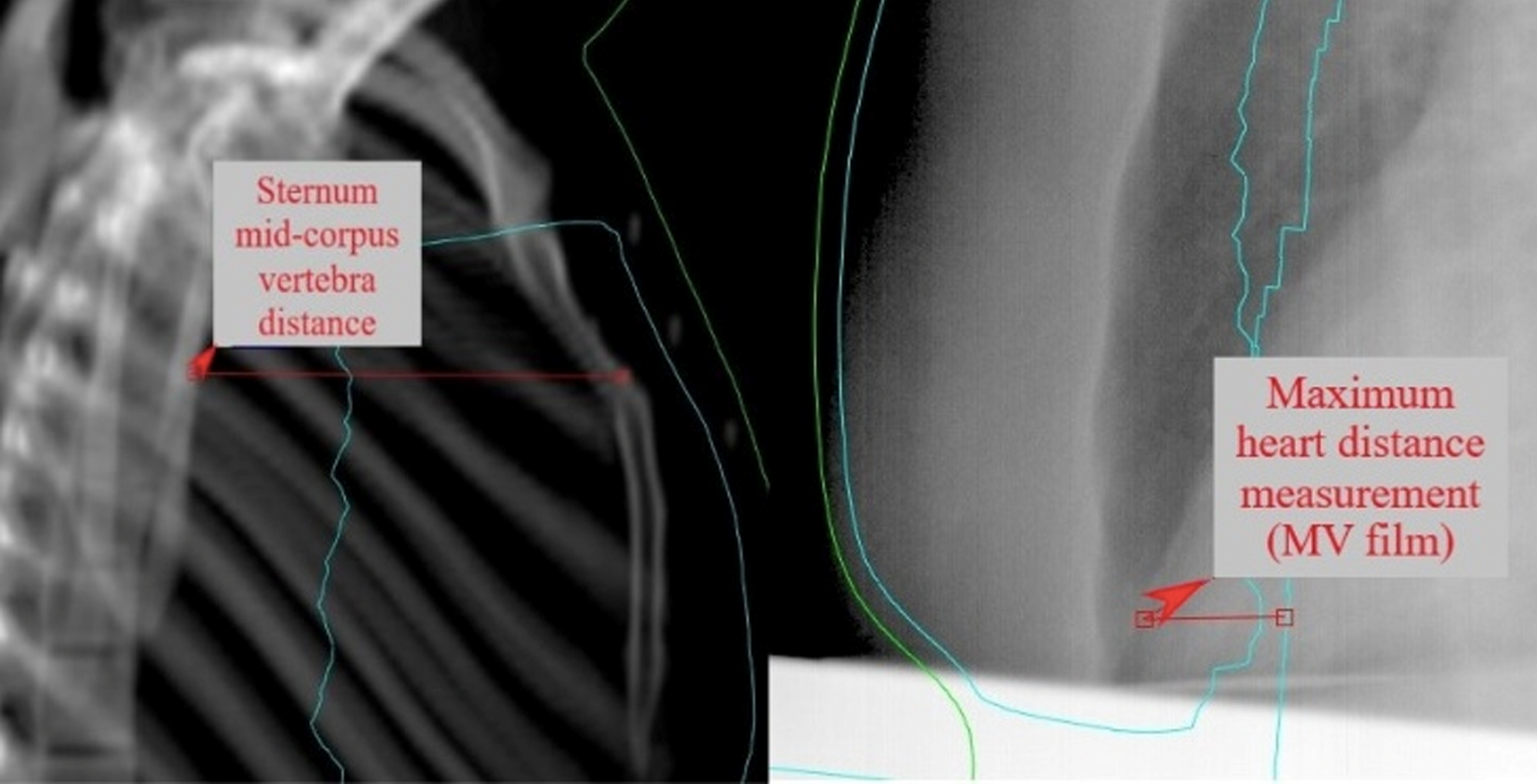
(a) Measurement of sternum-middle corpus vertebrae distance to determine the BHL from LAT kV image (b) Measurement of maximum heart distance inside treatment field from the LAT MV image.
Furthermore, bony landmarks (clavicula, costa, and humerus) displacement was measured from the matched AP and LAT kV images. Humerus displacement was measured in the AP and LAT direction while measuring costa and clavicula position errors in the S-I direction. A total of 600 measurements were performed.
In addition to bony landmarks, the variation in distance of the heart surface inside the tangential treatment field was retrospectively analyzed from the tangential image of the planning CT and set up MV images of the same patient in the treatment position. We measured the maximum heart distances in the treatment field from the lateral MV portal images. A total of 180 MV portal images were analyzed. And the maximum heart distance inside the treatment field was determined as presented in Fig. 2 (b) by measuring distances from the heart to the tangential field edge with v-DIBH MV images. Subsequently, to evaluate the relationship between body mass index and BHL, the weight and height of patients were recorded.
SPSS software version 20 used statistical analyses. Statistical tests were applied to evaluate whether the inter-fraction reproducibility and variability are significantly different. Friedman’s test and Wilcoxon’s test were performed for inter-fraction analysis of v-DIBH reproducibility and variability. Spearman’s rank correlation coefficient was applied to evaluate the relationship between BHL and bony landmarks displacement, and maximum heart distance, respectively. Also, an independent group t-test was used to assess the effect of BMI on BHL. A p-value<0.05 was considered to be statistically significant.
Results
The data for 30 patients with 150 treatment fractions and simulation data were analyzed in this study. The widest acceptable gating window width of 10 mm was applied for all patients as a clinical protocol. The median BHL height was 20.2 mm (range 9.6–32.4 mm). Table 1 describes the median and mean values of BHL for planning and all measured fractions.
The median and mean values of the BHL
The median and mean values of the BHL
The changes in mean BHL for the planning and measured treatment fractions are presented in Fig. 3.
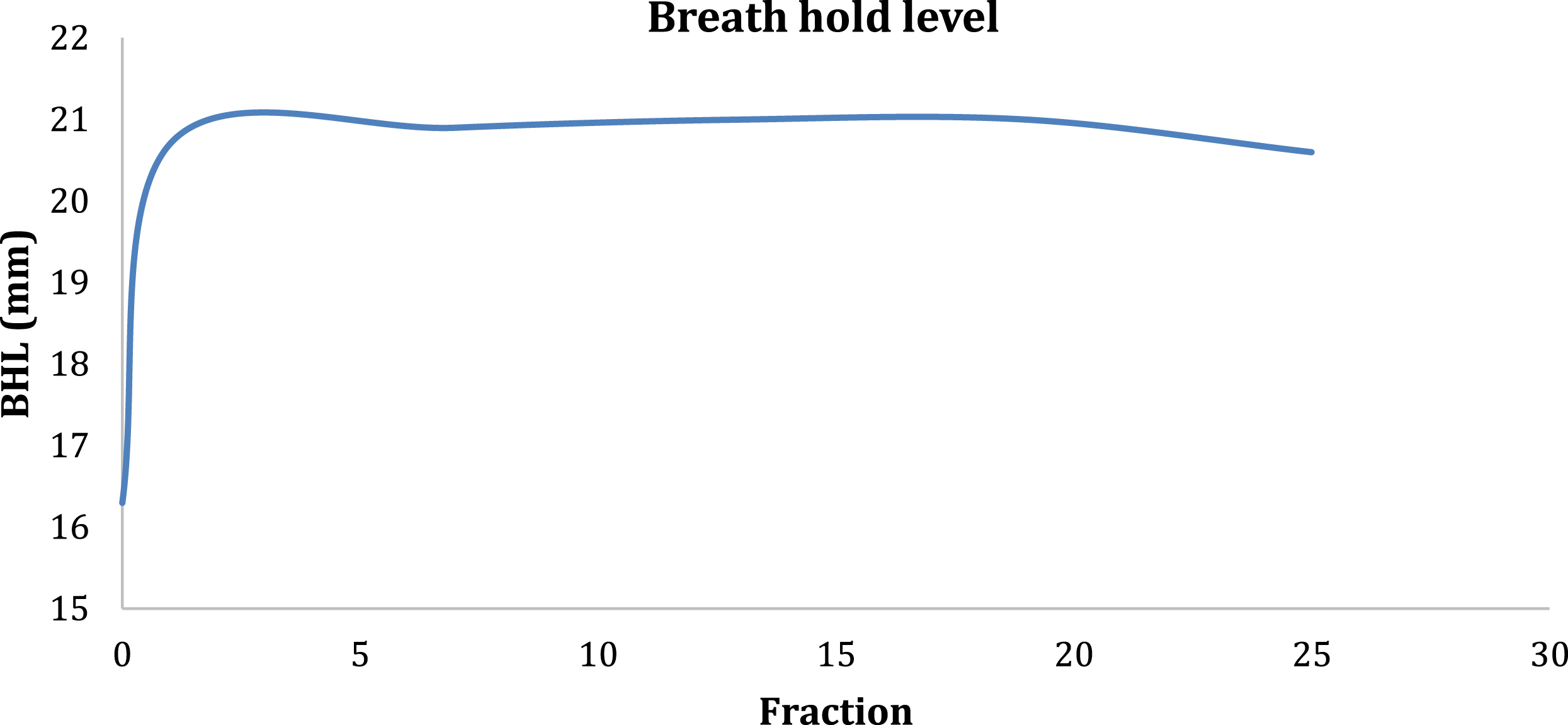
The changes in BHL during treatment.
Figure 3 shows that the height of BHL increased after simulation and is almost consistent during treatment. The median and mean values of the BHL were nearly identical for all measured treatment fractions. The inter-fraction reproducibility difference of BHL was not statistically significant. However, the mean BHL values between planning and all measured fractions were found to be statistically different; 16.3 vs. 20.8 mm for the planning and measured fractions (p < 0.001). This result means that the variability of BHL was significantly different. Also, to evaluate the BHL variability, the distance between the planning and measured treatment fractions, from the sternum and middle part of corpus vertebrae, were measured from the coregistered lateral kV images. The mean distance differs significantly between planning and treatment (p < 0.001).
Table 2 gives the quantitative results for the bony landmarks registration between treatment and planning with v-DIBH. Median shifts for each bony landmark were not found to be statistically significant. This result confirms the daily treatment positioning of the patient.
Numerical bony landmarks displacement
Humerus LAT and S-I displacement, clavicula, and costa S-I displacement are indicated in a histogram in Fig. 4.
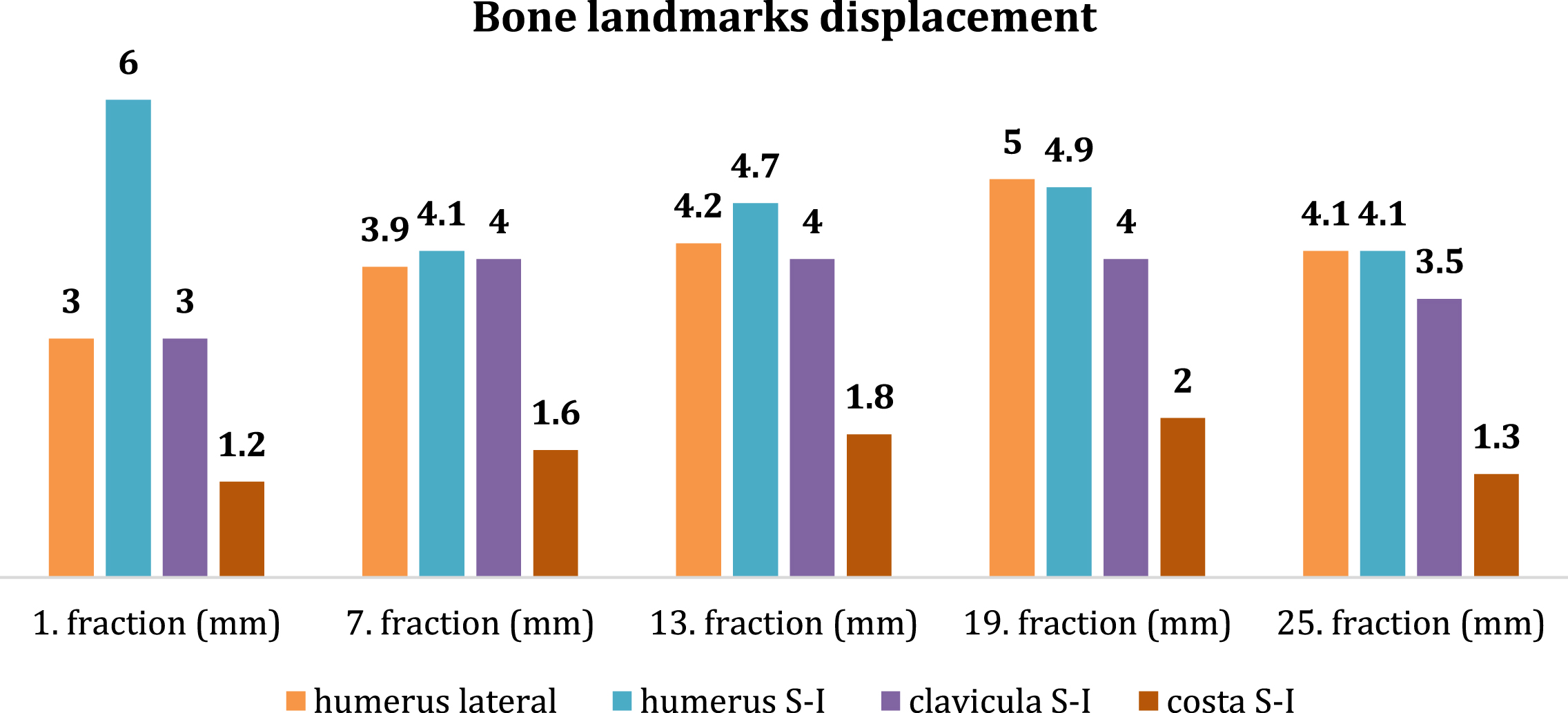
Histogram of the bony landmark displacements for measured fractions.
To investigate whether there is a correlation between the median bony landmarks displacements and the median BHL, Spearman’s rank correlation coefficient was applied and the analysis was not statistically significant (p > 0.05), meaning that the position changes of bony landmarks (humerus, clavicula, costa) did not affect the v-DIBH reproducibility during treatment.
In addition, the difference in distance of the heart displacement inside the tangential treatment field was statistically significant between the planning and treatment (p = 0.004). Spearman’s rank correlation was applied between the maximum heart distance and the BHL, no statistically significant differences were found (p > 0.05).
Furthermore, body mass index (BMI) was categorized as≤25,>25, and its relationship with sternum-middle corpus vertebrae distance was investigated by independent groups t-test. While the BMI of the patients raises, the sternum-vertebra distance tends to increase (p = 0.057). However, BMI has no effect on the BHL and treatment duration (p > 0.05).
In the present study, we assessed the setup reproducibility and variability of v-DIBH treatment for left-sided breast cancer patients using breath-hold curves and lateral kV set-up images in our clinic. As far as we know, this is the first study to evaluate the reproducibility and variability using breath-hold curves and lateral kV set-up images together based on a relatively large v-DIBH data. Our findings showed that the v-DIBH set-up for left-sided breast cancer treatment at our clinic is reproducible with a mean change of less than 1.0 mm for measured treatment fractions. However, the BHL between planning and different treatment fractions were compared and showed statistically significant differences (p < 0.05). The treatment fractions of mean BHL are also greater than the planned mean BHL. This result indicates a relatively poor variability of the v-DIBH treatment.
As seen in Fig. 3, the breath-hold capability of patients has increased significantly and is consistent during the treatment. The lack of an appropriate and enough patient education phase in the CT simulation may cause a large variation between planning and treatment. In a previously published study, Chopra et al. [21] showed some benefits of respiratory training, resulting in increased breath-hold time and tidal volume. The present results suggest that more breath hold training could be useful for patients with poor breath-hold capability before the simulation.
In the current setting of v-DIBH treatment in our department, the absence of visual support for the patient while performing the breath-hold (visual coaching for video goggles) may contribute to the lack of good variability. Instead of visual coaching, audio coaching is a standard procedure in our clinical implementation of v-DIBH treatment. For respiratory gated treatments, it has been demonstrated that audio coaching enhances the patient’s breathing frequency and pattern but not its amplitude [22]. In our study, we found a statistically significant amplitude difference between planning and fraction (16.3 mm vs. 21.0 mm). Furthermore, Cervino et al. [19] studied without and with visual coaching for v-DIBH and suggested that visual coaching improves the v-DIBH reproducibility and variability.
In addition, the present retrospective analysis of the LAT set up kV images by measuring the distance between sternum and vertebrae showed that the reference BHL changed between the planning CT and the start of treatment. The BHL shifts appear to be CT simulation-related because the reproducibility of the BHL was within 1 mm during treatment. The time interval between the planning imaging and the start of the treatment may be the reason for this. The mean BHL similarity in different fractions results in a good reproducibility of v-DIBH treatment. This result indicated that the patient’s breath-hold capability has been improved during treatment. Comparable to this, Laaksomaa et al. [17] found substantial displacement errors in the SI direction for BHL considering the distance between the vertebrae and sternum. In a study by McIntosh et al. [16], the BHL was similarly measured from LAT kV set-up images. The reproducibility of the BHL relative to bony structures was found good, which is like the present results.
The gating window width of 10 mm was used for all patients in this study. This value permits variation of±5 mm around the reference level specified in the CT imaging. The gating window width was not changed individually both in the planning CT and in the treatment. Also, this fixed setting of the gating window width may contribute to the mean BHL difference between planning and treatment. Furthermore, a relatively wide window of 10 mm has been used by McIntosh et al. [16] when the marker block has been placed on the patient’s abdominal surface. Also, Laaksomaa et al. [17] used the maximal window width (10 mm) and the authors found good reproducibility, which is comparable to the present results. In contrast, several authors [8, 13–15] have analyzed inter-fraction reproducibility with the RPM system restricting the narrow gating window widths.
The values presented in Table 2 indicated that small humerus, clavicula, and costa displacement are presented and the reference BHL has not changed related to the positional variations of bony landmarks. The current results imply that the setup images were precisely aligned based on the bony landmarks and resulted in minimal displacement in tangential images. Although we have taken measurements from a total of 5 fractions, we applied daily image guidance throughout the treatment. As demonstrated in Table 2, small inter-fractional setup variation was observed, hence we recommend that daily image guidance should be applied.
In previous studies, Skyttä et al. [13] found acceptable heart position variability concerning the BHL corrections. McIntosh et al. [16] employed kV images and EPID images to analyze the reproducibility of the heart position and they found reduced delivered dose to the heart due to excellent breath-hold reproducibility. In our study, the heart position variability in the distance of the heart surface inside the treatment field was statistically significant. However, as discussed above, the mean BHL in different fractions is larger than the planned mean BHL. The larger BHL may mean that slightly lower doses are delivered to the heart than planned. With the presented study, the heart position variability seems to be in favor of reducing heart dose.
There are some limitations to this study. First, we have not included all left-sided breast cancer patients treated with v-DIBH in our department. We included breast-only treatment and excluded supraclavicular irradiation. Second, the constant breath-hold set up with a 10 mm gating window width (±5 mm from the peak) was used for all patients. However, the amplitude of deep inspiration may differ between patients. We have not examined the impact of the different and narrow gating window widths.
Conclusion
We investigated the reproducibility and variability of v-DIBH treatment for left breast cancer patients using breath-hold curves and lateral kV setup images together with the RPM system. The mean BHL difference was less than 1.0 mm between fractions. Overall, the BHLs were reproducible and consistent, although there was some variation between planning and treatment.
Ethical approval
This retrospective study was approved by the Medical Specialty Training Board of Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital.