
Abstract
OBJECTIVE:
To present an optimized examination model by analyzing the risk of disease and image quality according to the combination of the ion chamber of automatic exposure control (AEC) with digital radiography (DR).
METHODS:
The X-ray quality was analyzed by first calculating the percentage average error (PAE) of DR. After that, when using AEC, the combination of the ion chambers was the same as the left and centre and right, right and centre, left and centre, centre, right, and left, for a total of six. Accordingly, the entrance surface dose (ESD), risk of disease, and image quality were evaluated. ESD was obtained by attaching a semiconductor dosimeter to the L4 level of the lumbar spine, and then irradiating X-rays to dosimeter centre through average and standard deviation of radiation dose. The calculated ESD was input into the PCXMC 2.0 programme to evaluate disease risk caused by radiation. Meanwhile, image quality according to chamber combination was quantified as the signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) through Image J.
RESULTS:
X-ray quality of DR used in the experiment was within the normal range of±10. ESD of six ion chamber combinations was 1.363mGy, 0.964mGy, 0.946mGy, 0.866mGy, 0.748mGy, 0.726mGy for lumbar anteroposterior (AP), and the lumbar lateral values were 1.126mGy, 0.209mGy, 0.830mGy, 0.662mGy, 0.111mGy, and 0.250mGy, respectively. Meanwhile, disease risk analyzed through PCXMC 2.0 was bone marrow, colon, liver, lung, stomach, urinary and other tissue cancer, and disease risk showed a tendency to increase in proportion to ESD. SNR and CNR recorded the lowest values when three chambers were combined and did not show proportionality with dose, while showed the highest values when two chambers were combined.
CONCLUSION:
In this study, combination of three ion chambers showed the highest disease risk and lowest image quality. Using one ion chamber showed the lowest disease risk, but lower image quality than two ion chambers. Therefore, if considering all above factors, combination of two ion chambers can optimally maintain the disease risk and image quality. Thus, it is considered an optimal X-ray examination parameter.
Keywords
Introduction
Due to the introduction of thin-film transistors and the digitization of radiography, most medical environments now use digital radiography (DR) to diagnose and treat diseases [1–3]. Compared to film-screen and computed radiography (CR) systems, DR has been shown to be highly efficacious in many medical imaging application areas. DR can combine various examination parameters, has a high image processing speed, improved dynamic range, and a wide range of post-processing methods; therefore, it quickly replaced the existing methods [4–6].
The most prominent of these advantages is the possibility of a combination of examination parameters. A basic method of forming an X-ray image is a form in which a detector records X-rays formed by a combination of tube voltage and tube current. The recently introduced DR shows an engineering approach to forming an X-ray image by introducing automatic exposure control (AEC) to the conventional X-ray formation method. AEC refers to a device that automatically controls amounts of X-rays that penetrate the human body through an ion chamber [7]. When the AEC is activated, the X-ray irradiation unit generates the optimal radiation dose required for image formation, and the X-ray detector detects X-rays more sensitively by setting sensitivity. In other words, the use of an AEC has the advantage that the radiation dose and image quality can be optimally adjusted [7–11].
Despite these advantages, the International Commission on Radiological Protection (ICRP) and the American Association of Physicists in Medicine (AAPM) warn against the use of DR indiscriminately [12–14]. Radiation generates an exposure dose as it passes through the human body. This exposure dose is converted into an absorbed dose within organs, determining the radiation risk to the human body [13]. In addition, organs in the human body have different sensitivities to absorbed doses, which can lead to diseases such as cancer [13]. Therefore, an X-ray examination is justified only if there is an examination benefit considering the radiation harm that can occur.
In addition to the justification for the examination, image quality is another consideration. Because most DR control the image quality by combining examination parameters in the AEC environment, it is necessary to set the ion chamber and parameters appropriate for the situation. Therefore, the ultimate goal of using DR should be to ensure image quality above a certain level while considering the risk of disease. Accordingly, various studies have attempted to optimize the exposure dose and image quality [15–18].
Nevertheless, the existing studies are limited as they focused on optimizing the exposure dose and image quality using conventional X-ray formation mechanisms. The international recommendation mentions the importance of managing the exposure dose and image quality in an environment where the AEC of the DR is used. However, there is a lack of research on the risk of disease and image quality related to the parameters of the DR. Therefore, in this study, when examinations are conducted by combining the ion chamber of the AEC, the risk of disease is predicted through Monte Carlo simulation, and the image quality is analyzed accordingly. We present an optimized digital examination model that can be applied in clinical practice.
Materials and methods
Digital radiography and experiment equipment
The experiment was conducted 30 times from May 01 to 30, 2022. For DR, a Philips Digital DIAGNOST VR at our institution with a maximum set tube voltage of 150 kVp and a tube current of 800 mA was used (Fig. 1). In addition, the phantom used in the experiment was a Rando Man Phantom (Alderson Research Laboratories, USA) composed of a tissue equivalent material, and the experimental sites selected were lumbar anteroposterior (AP) and lateral, which are frequently examined in clinical practice (Fig. 2).

The digital radiography unit used in the experiment. The upper part is the X-ray irradiation unit that generates X-rays, and the lower is the X-ray detection unit.

The Rando Phantom used in the experiment is composed of a material equivalent to a human body, so it is mainly used to evaluate the amount of radiation generated during X-ray examinations.
The examination conditions used in the experiment were an 81 kVp tube voltage for lumbar AP and an 85 kVp tube voltage for lumbar lateral. The other examination conditions were set to the same tube current of 400 mA, collimation of 43×43 cm2, gird ratio of 10:1, and a total filtration equivalent of 5.1 mmAl. The combination of the ion chambers was the same as the left and centre and right, right and centre, left and centre, centre, right, and left, for a total of six. The detector used was a Trixell product of the indirect conversion detection type, with a pixel size of 143μm, and bit processing of 14 bits (Table 1).
Fixed X-ray examination conditions
The radiation dose and X-ray quality were measured using a MagicMax universal semiconductor dosimeter (IBA Dosimetry, Germany). The radiation dose was determined by measuring the entrance surface dose (ESD) (Fig. 3). The X-ray spectrum was analyzed using the SRS-78 programme to calculate the average energy of X-rays according to the examination conditions of the DR, and the risk of X-rays was simulated by implementing the Monte Carlo Simulation using the PCXMC 2.0 programme (Fig. 4).

MagicMax Universal, a multi-purpose semiconductor dosimeter used to measure X-ray quality and radiation dose.
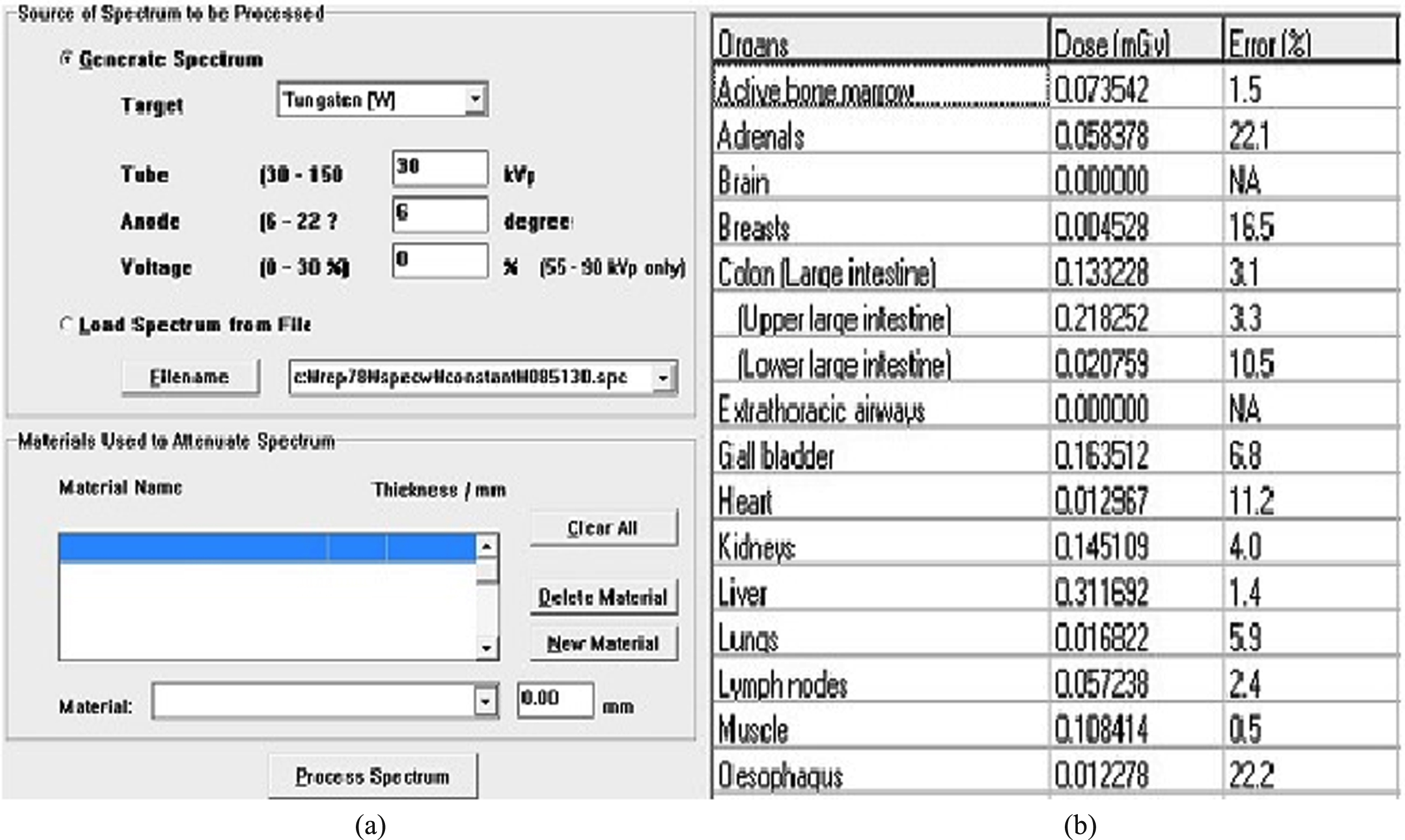
Simulation of disease risk using PCXMC 2.0 requires the input of the average energy of X-rays. (a) provides the function of analyzing the average X-ray energy through spectrum analysis with the SRS-78 programme. (b) is the PCXMC 2.0 programme, which is used to simulate the risk of disease.
The X-ray quality of the equipment was evaluated by irradiating to determine whether the DR used in the experiment was operating normally. A after the tube current was fixed at 400 mA, the tube voltage was sequentially increased to 81, 90, 102, 109, and 125 kVp, and the resulting percentage average error (PAE) and half-value-layer (HVL) were evaluated. For the PAE, if the set tube voltage is X
P
and the average value of the measured tube voltage is
The ESD of lumbar AP and lateral was calculated as the average and standard deviation of the radiation dose taken 30 times. The phantom was positioned on the wall detector in the AP and lateral directions. In addition, according to the phantom manufacturer manual, a MagicMax dosimeter was attached to the front and side surfaces of number 25 of the Rando Phantom to measure the ESD of the lumbar (Fig. 5).

Arrangement of the dosimeter, phantom, and detector to measure the entrance surface dose of lumbar anteroposterior and lateral. The dosimeter was attached to number 25 of the Rando Phantom, and the average and standard deviation of the radiation taken 30 times were calculated.
PCXMC 2.0 was used to predict the disease risk of lumbar AP and lateral examination. The disease risk simulation through PCXMC 2.0 was performed in the stages of examination data input, computer simulation, dose calculation, and risk assessment. In examination data input step, variables in relation to the equipment and radiation must be input. The variables to be entered in terms of the equipment are the maximum and average energies of the X-rays, angle of the anode of the DR, material of the anode, and total filtration. The maximum and average energies at lumbar AP are 81 keV, and 47.3 keV, and those at the lumbar lateral are 85 keV, and 48.7 keV, where the anode angle is 13°, the anode material is tungsten, and the total filtration is 5.1 mmAl (Table 2).
Equipment side variables to be entered in PCXMC 2.0
Equipment side variables to be entered in PCXMC 2.0
The variables to be entered in terms of radiation are the examination conditions, collimation size and SID. The tube voltage of the lumbar AP was 81 kVp and lumbar lateral was 85 kVp, collimation size was 43×43 cm2 and SID was 100 cm (Table 3).
Radiation side variables to be entered in PCXMC 2.0
After inputting both equipment and radiation variables in the examination data input stage, computer simulation was performed. In the computer simulation stage, Monte Carlo simulation for radiation dose prediction was performed based on the input examination data. Then, in the dose calculation stage, the ESD measured through MagicMax was input into PCXMC 2.0 to analyze the absorbed dose in the organs. Finally, in the risk assessment stage, the disease risk was simulated based on the results of absorbed dose and effective dose for each organ. The disease risk was shown as the probability of developing bone marrow cancer, liver cancer, lung cancer, stomach cancer, bladder cancer, and other tissue-related cancers by X-rays exposed to organs.
Image quality was analyzed using Image J 1.53 s (National Institutes of Health, USA) to determine the signal to noise ratio (SNR) and contrast to noise ratio (CNR) of lumbar AP and lateral. It is expressed as average and standard deviation. Medical image analysis using Image J basically requires the use of international standards and no compression data. Therefore, so that Image J can recognize the X-ray image, the X-ray image was stored as a file of no compression of the digital imaging and communications in medicine (DICOM) standard through picture archiving and communication systems (PACS). After reading the X-ray images with Image J, the SNR and CNR were analyzed using the region of interest (ROI) manager plugin of Image J (Fig. 6).

After reading the X-ray image using Image J, the image quality was analyzed using the analysis plugin. Currently, the X-ray image use a lumbar spine image in digital image communication in medicine format.
Lumbar AP and lateral ROI were set on lumbar spine level 4 as 0.5×0.5 cm2. The background standard deviation was set to the left centre for lumbar ap and the right centre for lumbar lateral. At this time, the pixel number of the ROI was 35×35 (Fig. 7). The equations for quantifying the SNR and CNR are the same as those in Equations (2) and (3).
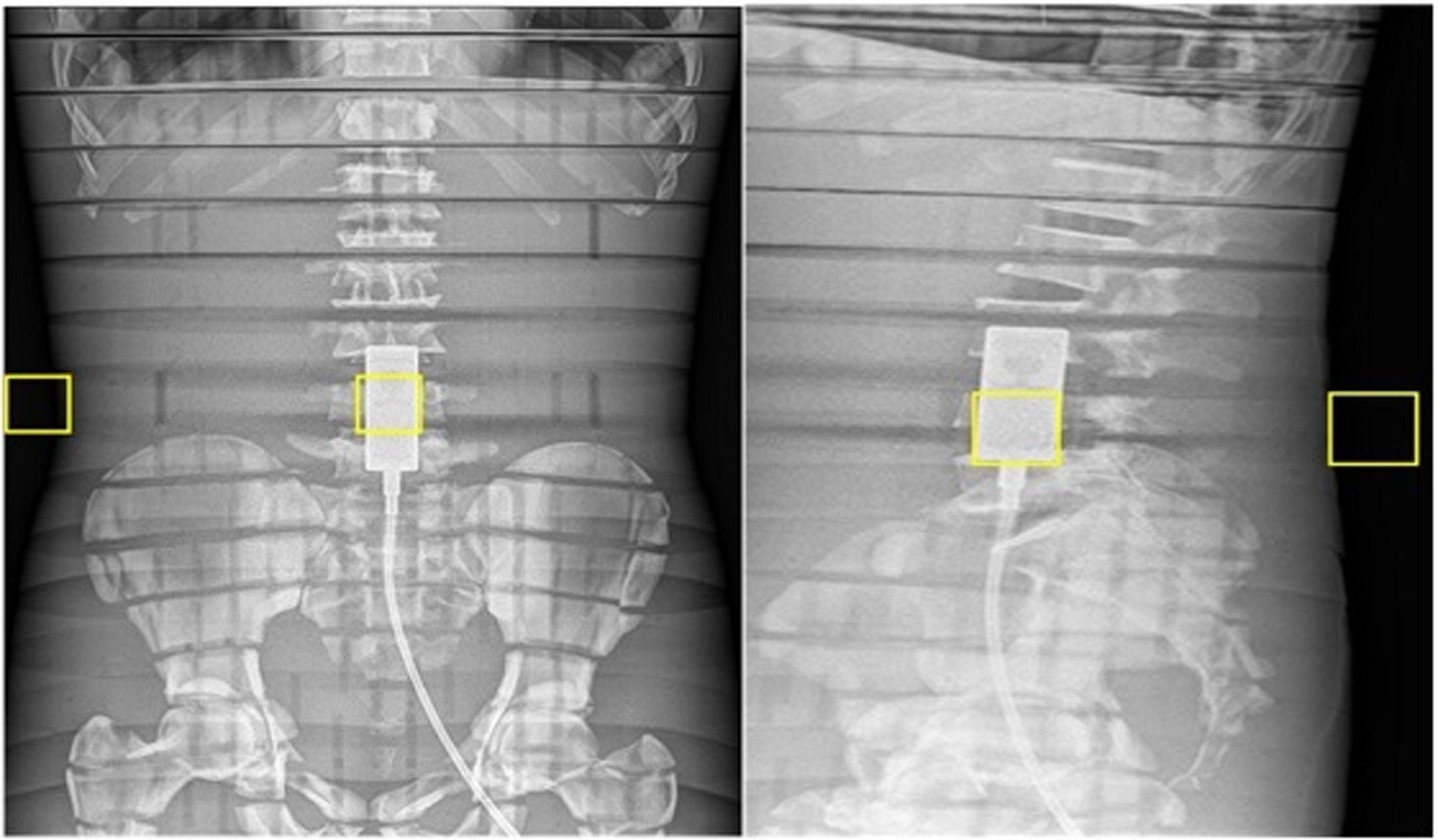
To analyze the image quality of lumbar anteroposterior and lateral, the region of interest and the background were selected through ROI manager of Image J. The middle yellow box is the region of interest, level 4 of the lumbar spine. The yellow box on the left of the lumbar anteroposterior and the yellow box on the right of the lumbar lateral are the background regions.
*Mean value of the region of interest (ROI): average signal volume in the ROI
*SD of BG: background standard deviation
*BG SIavg: average background signal strength
*ROI SIavg: average signal intensity in the ROI
After that, statistical analysis on image quality was performed. One way analysis was performed using the SPSS 23.0 (IBM Corporation, USA) statistical programme to analyze the image quality differences between the six ion chamber combinations. In order to secure the minimum reliability in statistical analysis, data of SNR and CNR obtained by exposing X-rays 30 times were used. At this time, statistical analysis determined that there was a significant difference when the p-value was less than 0.05 in the 95% confidence interval.
X-ray quality of digital radiography
PAEs for each tube voltage were –0.7%, –1.0%, –2.2%, –2.8%, –3.2%, and HVLs were 4.2, 4.5, 5.0, 5.5, and 6.2 mmAl (Table 4).
Percentage average error and half-value-layer in digital radiography
Percentage average error and half-value-layer in digital radiography
In the lumbar AP, the ESD was highest in the order of left and centre and right, right and centre, left and centre, centre, right, and left. In the lumbar lateral, the ESD was highest in the order of left and centre and right, left and centre, centre, left, right and centre, and right (Table 5).
Entrance surface dose of ion chambers
Entrance surface dose of ion chambers
Disease risk was simulated using PCXMC 2.0. The absorbed dose to organs that are expected to be exposed to radiation, such as the red bone marrow, colon, liver, lung, stomach, bladder, and other tissues, was calculated. The absorbed dose to organs is proportional to the ESD. Lumbar AP was highest in the order of left and centre and right, right and centre, left and centre, centre, right, and left, lumbar lateral was highest in the order of left and centre and right, left and centre, centre, left, right and centre, right. The absorbed dose by the organs in lumbar AP was highest in the order of the bladder, stomach, colon, liver, other tissues, bone marrow, and lung. The absorbed dose by the organs in lumbar lateral was highest in the order of the liver, colon, bladder, bone marrow, other tissues, stomach, and lung (Table 6).
Organ absorbed dose simulation using PCXMC 2.0
Organ absorbed dose simulation using PCXMC 2.0
As a result of analyzing the risk of using the chamber based on this, in proportion to the results of ESD and the absorbed dose to the organs, lumbar AP was highest in the order of left and centre and right, right and centre, left and centre, centre, right, and left. The lumbar lateral was highest in the order of left and centre and right, left and centre, centre, left, right and centre, and right. As for the risk of disease by organ, lumbar AP showed the highest risk in the colon, other tissues, bladder, stomach, liver, bone marrow, and lung. And lumbar lateral showed the highest risk in the colon, other tissues, liver, bone marrow, bladder, lung, and stomach (Table 7).
Cancer risk simulation using PCXMC 2.0
In lumbar AP, the image quality was the highest in the order of right and centre, left and centre, centre, right, left, left and centre and right. In lumbar lateral, the image quality was highest in the order of left and centre, centre, left, right and centre, left and centre and right, right. In this study, image quality according to the combination of the ion chamber showed a statistically significant difference. (Table 8).
Evaluation results of image quality
Evaluation results of image quality
***p < 0.001.
The ICRP shows a multifaceted approach as part of the regulation of the indiscriminate use of X-rays [19–21]. As one of them, by publishing ICRP publication 135 in 2017, the importance of the diagnostic reference level (DRL) was announced for the management of radiation dose in the medical field [20]. One of the peculiarities is that compared to computed tomography (CT) and interventional radiography (IVR), the ICRP mentioned the importance of setting a DRL for general radiography (GR), which is examined with a relatively low radiation dose. Therefore, the use of X-rays in the medical field is recognized as an important international issue [22–26].
From the perspective of radiation protection, the harm that can be caused by the indiscriminate use of radiation appears as deterministic and stochastic effects. The deterministic effect is the concept that there is a threshold dose that causes radiation harm when receiving a radiation dose, and the stochastic effect is the concept that the probability of occurrence of cancer or genetic effects increases in proportion to the radiation dose above a certain level [13]. Therefore, radiation protection aims to prevent deterministic effects and minimize stochastic effects. Because, GR examination is performed at a dose below the threshold dose that develops a deterministic effect, the purpose of GR examination should be to minimize the stochastic effect that can cause diseases such as cancer.
At the same time, considering the stochastic effect, GR examination should also consider the image quality. The AAPM mentions the importance of optimizing image quality through a combination of appropriate parameters when using an AEC [14]. Compared to conventional methods, DR is inspected by combining various parameters. Therefore, inappropriate parameter selection is a major cause of image quality degradation. Previous studies only evaluate the radiation dose generated in the AEC environment [7, 23], or the overall effective dose according to the combination of ion chambers and the approach to assessing the image quality in an experience-based method have been shown [7, 26]. In other words, there are insufficient studies to objectively evaluate the disease risk according to the absorbed dose for each organ and the related image quality. Therefore, in this study, the disease risk and image quality according to the combination of ion chambers were evaluated, and an examination model that guarantees the minimum risk of radiation and high image quality in the clinical environment was presented.
First, it was necessary to select an experimental range in which changes in the exposure dose and image quality could be observed by parameter setting. Usually, the exposure dose varies depending on the tissue of the human body, because the material, thickness, and density of the tissue are different. The exposure dose increases in the order of bone, muscle, and fat, and when an AEC is used, the exposure dose increases in proportion to the thickness and density [22]. Compared to other tissues, the lumbar spine is composed of bones and muscles that generate a large exposure dose, and its thickness and density are high, resulting in a large exposure dose. In addition, lumbar region includes radiation-sensitive organs such as the colon, stomach, and bladder within the image formation range, and in some cases, they accompany their own movements. Therefore, a careful parameter setting is required to prevent image quality degradation [23]. The exposure dose and image quality can change significantly depending on the parameter setting in lumbar examinations. Therefore, lumbar region, which is easy to observe exposure dose and image quality by parameter setting, was selected as the experimental site.
The examination conditions of the DR used in the experiment were set in consideration of whether or not they were optimized. Various existing studies emphasize the importance of setting examination conditions to optimize radiation dose [4–7], official institutions also mention the importance of setting examination conditions for optimizing radiation dose [13, 22]. Therefore, in this study, the examination conditions were set according to the guideline provided by the official national institution that conducted this study [22]. Reflecting this, the tube voltage of lumbar AP was set to 81 kVp, and lumbar lateral to 85 kVp. In addition, physical factors such as tube current, collimation size, grid ratio, and total filtration equivalent were all fixed the same. Changes in the physical factors cause unpredictable changes in disease risk and image quality [5, 18], this is because many variables can be generated in this study to present the optimized parameters.
The PAE and HVL of the voltage were measured to determine whether the DR generated normal X-rays. In the case of tube voltage, when the PAE is within±10% of the set tube voltage, and the HVL shows more than 2.3 mmAl at 80 kVp, the equipment encounters no issues [24]. The DR used in this experiment showed that the PAE was within the normal range for all the tube voltages. In addition, the HVL showed results above the normal range and, at the same time showed a linear increase as the tube voltage increased, confirming that the equipment had no problem in terms of X-ray quality.
The ESD was measured using a semiconductor dosimeter and recalculated by multiplying the back-scattering coefficient suggested in the International Commission on Radiation Units and Measurements (ICRU) report 74 to consider the actual contribution of the ESD to the human body [25]. The ESD of the lumbar AP was high when the three chambers and two or more ion chambers were used. The AEC generates a radiation dose in proportion to the composition, thickness, and density of the material. The lumbar AP has a large cross-sectional area that responds to the ion chamber and includes many bones and muscles with high radiation absorption. This result demonstrates the proportionality between the ion chamber and ESD [22]. On the other hand, lumbar lateral showed high ESD like lumbar AP when the three chambers were combined, but below that, the proportionality of the radiation dose according to the ion chamber combination cannot be found. This is because the lumbar lateral has a smaller cross-sectional area to respond to the ion chamber than the lumbar AP. Particularly, when the right ion chamber is used, there is almost no cross-sectional area reacting to the chamber. Therefore, the decrease in ESD is more pronounced. When the right ion chamber is used, the cross-sectional area to which the AEC responds is smaller, and the density is low compared to other chambers, and a proper radiation dose cannot be formed.
Disease risk was evaluated through Monte Carlo simulation using PCXMC 2.0. The risk of disease caused by the radiation dose is evaluated based on the absorbed dose and effective dose. PCXMC 2.0 makes it possible to predict the risk of future disease by presenting the absorbed and effective doses for each organ caused by ESD as objective values [26–28]. Taken together, PCXMC 2.0 can provide an indicator that is very suitable for this study to evaluate the risk of disease posed by radiation dose. In addition, because various studies have reported their excellent performance and accuracy using PCXMC 2.0 [25–27], this study analyzed the risk of future diseases that can occur during lumbar X-ray examination using PCXMC 2.0.
Among the determinant organs reported by the ICRP, the lumbar AP and lateral determinant organs were the bone marrow, colon, lung, stomach, bladder, liver and other tissues, and the risk of future disease was shown to be cancer [13]. First, the absorbed dose for each organ and the cancer incidence probability of the lumbar AP and lateral according to the ion chamber combination were proportional to the ESD. This results from the typical reflection that the exposure dose is proportional to the amount of radiation and energy absorption owing to the interaction between radiation and matter [13, 14]. However, in terms of organs, the absorbed dose and cancer incidence differed between lumbar AP and lateral sides. In the case of lumbar AP, the absorbed dose by organ was highest in the order of the bladder, stomach, colon, liver, other tissues, bone marrow, and lung. In the lumbar lateral region, the absorbed dose by organ was highest in the order of the liver, colon, bladder, bone marrow, other tissues, stomach, and lung. This is because the difference in the cross-sectional area due to the ion chamber was reflected, so the absorbed dose for each organ of the lumbar AP and lateral was different. In the case of lumbar AP, the risk of cancer by organ was highest in the of colon, other tissues, bladder, stomach, liver, bone marrow, and lung. In the case of lumbar lateral, the risk of cancer by organ was highest in the order of colon, other tissues, liver, bone marrow, bladder, lung, and stomach.
Image quality was evaluated through SNR and CNR according to the combination of the ion chamber. In AEC environment, the more ion chambers are combined, the greater the radiation dose, and it shows high image quality in proportion to the radiation dose. The results of the one-way analysis and the post hoc analysis also showed that the combination of the ion chamber and the image quality were proportional. In particular, when the centre ion chamber was used or combined, more ESD occurred due to the presence of dense and thick lumbar spine, and a dosimeter attached, so higher image quality was recorded than when other chambers were used [19, 29]. However, the lumbar lateral examination recorded a clear image quality deterioration when the right ion chamber was used compared to the use of the centre chamber. This is a result of the fact that the cross-sectional area and density of the phantom that responds to the right chamber of the lumbar lateral are very small, so that proper ESD and signal volume cannot be formed. Except for these cases, the image quality showed a linear increase in proportion to the radiation dose. This trend continued until two ion chambers were combined. This is a result that typically reflects the tendency of the radiation dose and image quality to increase as more ion chambers are combined in the AEC environment [7, 23]. However, the combination of the three ion chambers showed the lowest image quality despite the highest ESD. This is because of the figure of merit (FOM) of the system; when the system exceeds the expressible maximum, the reproducibility is saturated, and the noise greatly increases [30]. The reason for the degradation of the image quality when the three ion chambers are combined is that the noise related to the image quality increases due to the FOM saturation of the system.
Conclusion
This study aimed to present a clinically applicable test model by objectively evaluating the risk of disease and image quality during lumbar X-ray examinations according to the combination of ion chambers. The limitations of this study are as follows; the point is that we could not evaluate the disease risk and the image quality of the parametric model using a portable X-ray machine or DR from another company. This means that the parameters of the system proposed in this study cannot be universal. In addition, since it is an experiment using a phantom, it is also considering that the usefulness of the parameters could not be analyzed with the image quality technique related to the actual expert reading such as radiologist. Therefore, it is another task to study the combination of X-ray parameters with other radiation generators and other image quality methods, and it is worth pursuing in the future. Nevertheless, compared with previous studies, this study presented a differentiated method of objectively analyzing the absorbed dose for each organ, the risk of disease, and the resulting image quality by combining the ion chamber, based on this, it is of great significance in that it has proven that when two ion chambers are combined, the disease risk can be minimized and high image quality can be guaranteed. When using AEC, if the radiation dose generated by the bone, muscle, density, and thickness constituting the human body is expected to adversely affect the disease and image quality, we propose the examination model that combines two ion chambers to optimize the disease risk and image quality.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no conflict of interest, financial or otherwise.
Footnotes
Acknowledgments
The authors would like to thank all participants enrolled in this paper.