
Abstract
BACKGROUND:
Multi Fractionated stereotactic radiosurgery (MF-SRS) of Linac has an essential role in the treatment of skull base meningiomas (sbMNG). However, Gamma Knife Icon (GK) allows MF-SRS using mask immobilization with onboard image guidance.
OBJECTIVE:
This dosimetric study aims to investigate whether equivalent plan quality can be achieved with Volumetric Modulated Arc Therapy (VMAT) in patients with large sbMNG (>10 cm3) previously treated with GK.
METHODS:
Twenty patients with the median target volume of 19.7cm3 are re-planned by using VMAT with 20 Gy in 5 fractions. Plan qualities are compared to tumor coverage, paddick conformity index (PCI), gradient index (GI), V4 Gy, V10 Gy, V12 Gy, optic chiasm V20 Gy, brainstem V23 Gy, optic nerve V25 Gy volumes, and maximum doses for all. Additionally, beam-on time and approximate planning time are also analyzed and compared.
RESULTS:
All plans provide adequate clinical requirements. First, the CI is comparable for the GK and VMAT (0.99±0.01 vs. 1.13±0.20; p = 0.18). Second, VMAT has a significantly higher GI than GK (3.81±0.35 vs. 2.63±0.09; p < 0.001). Third, the PCI is significantly higher in GK than VMAT (0.76±0.05 vs. 0.70±0.07; p < 0.001). The lower GI of the GK also results in significantly lower V4 Gy (156.1±43.8 vs. 207.5±40.1 cm3, p < 0.001) and V10 Gy (26.1±9.0 vs. 28.9±7.7 cm3, p < 0.001) compared to VMAT. Last, the VMAT reduces beam-on time (4.8±0.5 vs. 19±1.1 min.; p < 0.001).
CONCLUSION:
Although both systems have succeeded in creating effective plans in clinical practice, the GK reveals more effective lower normal brain tissue doses. However, the shorter treatment time with LINAC, excluding the total procedure time, can be considered advantageous over GK.
Introduction
Meningioma (MNG) is the most common (37.6%) primary intracranial tumor, and approximately 30% are observed in the skull base [1]. Natural history studies have demonstrated that up to 40% of patients with an untreated skull base MNG (sbMNG) will deteriorate neurologically and require treatment within a limited period of observation [2]. Despite the recent advances in microsurgical technique, the morbidity and mortality after surgical resection of large (>10 cm3) sbMNGs is still high due to the intricate anatomy of the skull base. To avoid these, complete surgical resection cannot be achieved in many patients; thus, patients face an increased risk for recurrence. Radiation therapy (RT) is usually recommended to improve local tumor control in patients with residual or recurrent sbMNGs and those with unresectable tumors or unfit for surgery [3].
For decades, conventional RT has played an essential role in the management of sbMNGs with up to 91% local control at 10 years and 85.2% unchanged/improved quality of life [4]. Despite these promising results, there has been an interest in using single-fraction (sfSRS) and hypofractionated stereotactic radiosurgery (hfSRS) as alternatives to fully fractionated RT for selected sbMNGs to shorten the length of treatment and reduce the high radiation dose administered to the surrounding normal brain tissue. For large sbMNGs, hfSRS, also called multifraction SRS (mfSRS), has been employed as an alternative to single-fraction SRS to improve the balance between tumor control and normal tissue toxicity over sfSRS. Besides, hfSRS can reduce the risk of late side effects as it allows normal tissue repair between fractions while delivering a high dose per fraction. In addition, reoxygenation and reassortment between fractions can improve tumor control by increasing cell kill.
SRS can be given using various radiosurgical technologies such as Gamma Knife radiosurgery (GKRS), Linear Accelerator (LINAC)-Based Radiosurgery, and Charged-Particle Proton Radiosurgery. The LINAC-based SRS had been used as a reasonable selection on account of fast delivery with multileaf collimator (MLC) and availability of a general radiation unit with an onboard image (OBI) and cone-beam computed tomography (CBCT) stereotactic imaging for accurate target alignment and intrafraction motion management. The target dose distribution can be tailored by varying collimator sizes, eliminating undesirable arcs, manipulating arc angles, using multiple isocenters, and differentially weighting the isocenters. Similarly, the latest release of the Gamma Knife Icon™ (Elekta, Stockholm, Sweden) rethinks the solution entirely, and it introduces onboard CBCT and infrared motion tracking system known as the intrafraction motion management (IFMM) system to allow patients to be treated without a frame at all, instead of using thermoplastic mask immobilization for multisession treatments [5, 6]. As the design of Gamma Knife with the use of radioactive sources as a source of radiation and a radiation body and collimator system with an essentially fixed geometry specifically designed to receive a patient’s head makes GKRS an extremely reliable intracranial SRS solution, many dosimetry comparison studies have been conducted to compare the plan quality of GKRS with other SRS modalities with results usually in favor of GKRS in terms of better conformity and reduced normal brain dose [7–9]. With the advances mentioned above, it has become possible to make such comparisons in hfSRS.
For large sbMNGs with an average of 19.7 cm3 in patients, this retrospective dosimetric study aimed to investigate whether equivalent radiosurgical plan quality could be obtained for the new generation Gamma Knife Icon™ (Elekta, Stockholm, Sweden), which allows hfSRS treatments, and Volumetric Modulated Arc Therapy (VMAT) of TrueBeam™ LINAC (Varian Medical Systems Palo Alto, CA, USA), which is the standard radiosurgical treatment technique for many clinics.
Materials and methods
Patient selection
Following ethical approval, we retrospectively identified 20 consecutive patients with large sbMNGs primarily treated with Gamma Knife Icon™ (Elekta, Stockholm, Sweden) at our institution between 2017-2019. The median treatment volume was 19.7 cm3 and ranged from 10.8 to 37.4 cm3. The prescribed dose was 20 Gy in 5 fractions for all tumors. The dose and fractionation scheme was formulated by a neurosurgeon, medical physicist, and radiation oncologist in collaboration. Table 1. displayed details of the patient’s characteristics.
Summary of patients’ characteristics
Summary of patients’ characteristics
Gamma knife planning
A pre-treatment warmed thermoplastic mask was molded over the patient’s face, and a reference cone-beam CT (CBCT) scan is obtained. Then pre-treatment 1-mm, thin-slice, volumetric, axial CT, contrast-enhanced T1 images, and T2-weighted MRI images were obtained and exported to Leksell Gamma Plan® (version 11.1.1 Elekta Instrument, Stockholm, Sweden) following image fusion, distortion correction, and tumor and organ at risk (OAR) outlining in Brainlab Elements (BrainLAB, Feldkirchen, Germany). The reference CBCT is registered with the planning MRI using the registration algorithm of the Gamma Plan. Target delineation was performed using T1-weighted MRI, and the gross tumor volume (GTV) was equal to the clinical target volume (CTV) and planning target volume (PTV). Shots with collimator sizes 4, 8, and 16 mm were placed inside the target and manipulated to achieve high target coverage (GTV) simultaneously, high selectivity, and reasonable treatment times using the best-fit isodose method until a clinically acceptable plan was formulated. A second CBCT was co-registered with the reference CBCT. The new adapted 3D distribution and dose-volume histograms are again reviewed, and if satisfactory, the treatment is delivered. Before every fraction, CBCT was acquired to confirm the exact position of the skull. Automated co-registration was done to define the daily variation in translation and rotation. The program automatically adapts the shot positions to the daily position and recalculates the dose distribution. sbMNGs were irradiated daily. The OARs were contoured, and the planning objective was to minimize the dose to normal brain tissue as much as possible [10]. Cobalt-60 sources in the Gamma Knife was < 3 years old over the entire range of treatments. Source activity (2.8 Gy/min) was > 75% of original activity (3.7 Gy/min) for all cases, so treatment times were those of the actual delivery of treatment which was not corrected for a particular source age.
VMAT planning
CT images containing the target and OAR contours with MRI fusion were transferred from GK TPS to Pinnacle TPS (version 9.10, Philips Medical Systems Inc. Cleveland, OH) for creating VMAT plans via the DICOM-RT (Digital Imaging and Communications in Medicine–Radiotherapy) format. VMAT plans were made using Pinnacle’s Smart Arc optimization algorithm using a coplanar technique with two full arcs of clockwise and two full arcs of counterclockwise. 1 mm margins were added to the GTV to define the PTV. All plans were generated by 6 MV based on TrueBeam™ (Varian Medical Systems Palo Alto, CA, USA) at 1400 MU/min dose rate and equipped with 120-leaf high-definition (HD) multileaf collimator MLC (2.5 mm leaf width). Additionally, jaw tracking was enabled to reduce MLC transmission for all plans that were normalized to deliver the prescription dose to 99.5% of the target volume [11]. The final dose calculation was performed with Collapse Cone (CC) Convolution algorithm on Pinnacle TPS, including heterogeneity correction and using a dose grid ranging 1 mm without depending on the size of the target.
Plan comparison
The total volume of normal brain (i.e., brain excluding gross tumor volumes) receiving 4 Gy (V4 Gy), 12 Gy (V12 Gy), and 20 Gy (V20 Gy) were collected as the representation of low, medium, and high brain doses. Maximum doses of OAR (cochlea, bilateral lens, optic chiasm, brainstem, optic nerve), and optic chiasm V20 Gy, brainstem V23 Gy, optic nerves V25 Gy doses, were derived from dose-volume histograms (DVH). Beam-on time (in minutes) and approximate planning time were also obtained for each plan. Beam-on time for VMAT plans was calculated by dividing the treatment monitor units (MU) by 600 MU/minute. Although the highest dose rate in VMAT treatment is 600 MU/minute, an average beam-on time was calculated considering that it performed arcs rotation with a high dose rate in stereotactic radiation therapy. For GKRS, the beam-on time was reported by the treatment planning system (TPS) based on the current dose rate, which was high with a new source (calibrated at 3.5 Gy/minute for our installation) but decreased with time according to the decay of Cobalt 60. We normalized the GKRS beam-on time to a dose rate of 2.8 Gy/minute in this study. A planning time was estimated by each planner who conducted the planning. Comparison of GKRS and LINAC plans in axial, sagittal, and coronal slices were presented in Fig. 1.
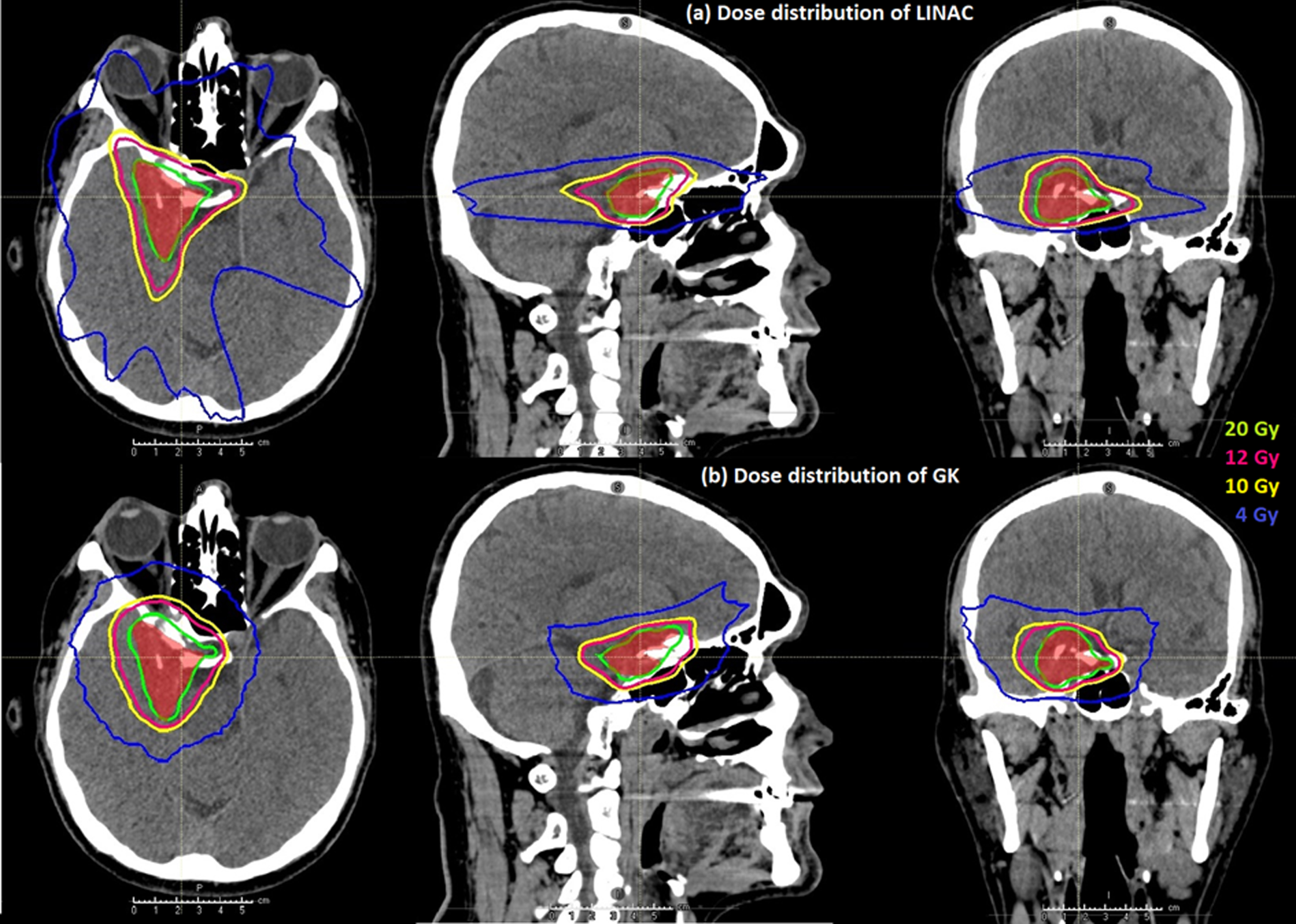
Axial, sagittal, and coronal views of isodose distribution with (a) VMAT and (b) GKRS for a given patient. Target is defined by the red areas on all images showed.
For each tumor, dosimetric parameters of the OAR were measured from DVH analysis, and plan quality was calculated from GKRS and Pinnacle TPS. For target coverage (GTV), mean dose (Dmean), maximum dose as D98 %, minimum dose as D2 %, Conformality Index (CI) as recommended by ICRU 62, Paddick Conformality Index (PCI), and Paddick Gradient Index (PGI) were compared [12, 13]. The formulas were as follows:
The comparison between plans based on the analysis of DVHs was performed for OARs, including the brain, brain stem, optic chiasma, left and right optic nerves, left and right cochlea, and left and right lens. For the brain, DVH points of Dmax Gy and V12Gy%, V10Gy%, and V4Gy%, as the representation of low, medium, and high brain doses were examined. Maximum dose points were compared for all other OARs.
Statistical analyses were conducted with R 3.5.3 and SPSS 23.0. When the sample size is less than 30 for the comparisons the nonparametric test was used. Nevertheless, for its assumption of normality, some distributional plots were used such as the box-whisker plot. Wilcoxon Signed Ranks Test was used for the dependent samples comparisons. A value of p < 0.05 was considered to indicate statistically significant differences.
Patients were compared in terms of doses received by the normal brain tissue for GKRS and VMAT plans. The median brain-V12 Gy was 14.8±5.97 cm3 (range, 6.58-31.49 cm3) for GKRS and 16.6±5.25 cm3 (range, 8.38-29.06 cm3) for VMAT (p = 0.16). However, the comparison of median low brain doses (brain-V4 Gy) revealed a statistically significant difference (p < 0.0001) between GKRS (156.1±43.78 cm3; range, 91.40-259.81 cm3) and VMAT (207.5 cm3 ± 40.09; range, 167.64-304.85 cm3). The dose difference started at GKRS brain-V10 Gy (26.1±8.97 cm3; range 11.04-50.5 cm3) and VMAT brain-V10 Gy (28.9±7.68 cm3; range, 18.65-48.50 cm3) (p < 0.001). Figure 2 presents the Box-Whisker Plot of the brain (V12 Gy, V10 Gy, and V4 Gy) according to GKRS and VMAT. The mean beam-on times differed significantly between GKRS and VMAT. The median beam-on time was 19±1.12 minutes (range, 9.7-38.5 minutes) for GKRS (GKtime) and 4.8±0.53 minutes (range, 4.23-5.15 minutes) for VMAT (VMATtime) (p < 0.001) (Fig. 2).
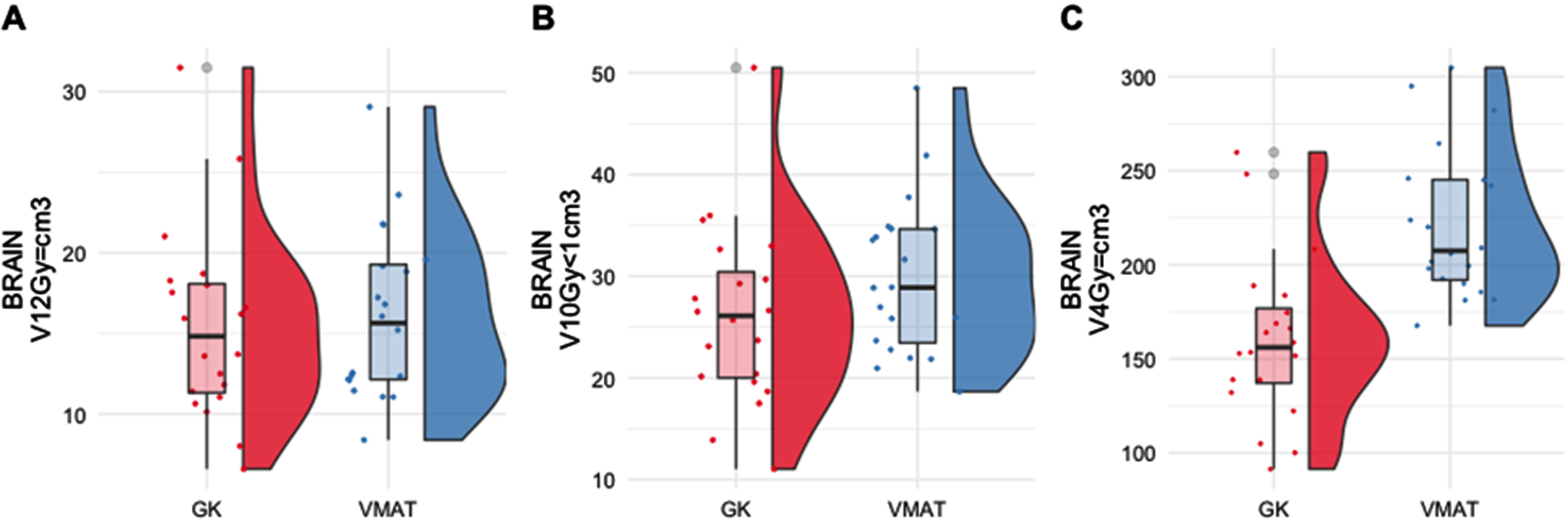
The Box-Whisker Plot of Brain (V12 Gy, V10 Gy, and V4Gy=) according to GKRS and VMAT (n = 20).
Regarding brainstem and optic chiasm, maximum doses were found to be statistically similar in both plans. Comparison of maximum left and right lens doses showed that VMAT had a significantly higher dose than GKRS (p < 0.001). The comparisons between GKRS and VMAT regarding the dosimetry in terms of other critical structures, including the left optic nerve, left cochlea, right optic nerve, and right cochlea, were insignificant (p > 0.05). The detailed data were presented in Table 2.
Descriptive Statistics and Comparisons according to GKRS and VMAT (n = 20)
p*<0.05, p**<0.01. Gk: gamma knife, D max: maximum dose, VMAT: volumetric arc therapy.
Patients were analyzed in terms of indexes used for plan quality according to GKRS and VMAT. The detailed data were presented in Table 3. The conformality index of GKRS and VMAT showed similar values of 0.99±.01 (range 0.96-1.01) and 1.13±.20 (range 1.02-1.67), respectively. VMAT had a significantly higher GI than GKRS (3.81±.35 vs. 2.63±.09, respectively, p < 0.001). However, GKRS had a significantly higher Paddick conformality index compared to VMAT (0.76±.05 vs. 0.70±.07, respectively, p < 0.001). The Bar Plot of Time and Index according to GKRS and VMAT was presented in Fig. 3.
Descriptive Statistics and Comparisons of Index according to GKRS and VMAT (n = 20)
p*<0.05, p**<0.01. GK: Gamma Knife; CI: Conformality Index, PCI: Paddick Conformality Index; GI: Paddick Gradient Index.
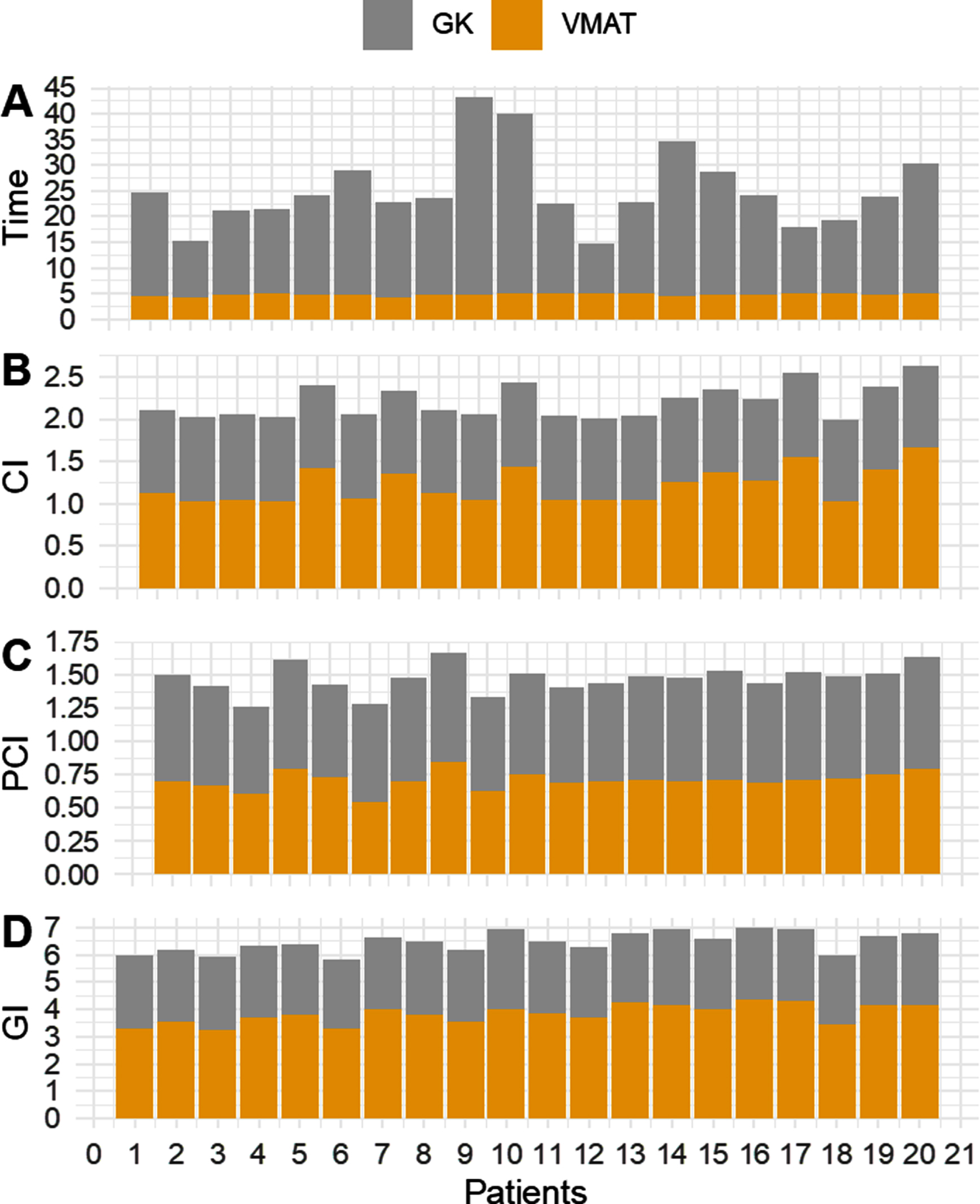
The Bar Plot of treatment time and Index according to GKRS and VMAT. (a) The treatment times were longer in GKRS plans. (b) CI was similar in both treatment plans. (c) and (d) plot showed that PCI and GI indexes for each patient, which revealed, GKRS is higher than VMAT.
Gamma Knife Icon™ (Elekta, Stockholm, Sweden) has been newly introduced with the capability of delivering a masked-based hfSRS option for cranial tumors, including meningioma. As there is a limited number of dosimetric studies comparing GKRS and LINAC-based SRS plans, we aimed to compare the plan quality and OAR sparing of fractionated SRS plans to assess the clinical practice of treatment devices to guide our patients in daily routine. Our results revealed that both modalities could deliver highly conformal doses to lesions larger than 10 cm3 at the skull base with similar CI and PCI. However, GK plans are superior to LINAC in dose fall-off (lower GI) and low brain dose (V4 Gy and V10 Gy), with shorter beam-on time for one fraction being the only advantage of LINAC plans excluding the total procedure time.
In our study, a 1 mm PTV margin was used for VMAT treatments with LINAC. The difference between imaging capacity and how radiation is delivered in LINAC treatments indicates that a different PTV margin can be used. Eaton et al [14] have shown that the most significant effect on normal tissue sparing, such as gradient fall-off and normal brain dose, is directly related to the selected PTV margin. The purpose of choosing the minimum PTV margin in our study is that an extra 1 mm margin on a large volume will contain much more normal tissue than a 1 mm margin in a small lesion. There are several studies about the dose to the normal brain tissue and adverse effects after SRS treatment of the brain [15–19]. In these studies, it was emphasized that radiation dose, fraction number, and volume are the main variables affecting the development of radiation necrosis. In the data published by Lawrence et al. 16 on RT-induced brain injury for sfSRS, a clear correlation has been demonstrated between the target size and the risk of adverse events. They recommended adopting the “volume receiving 12 Gy” as the standard method of reporting the dose to the normal brain in SRS procedures. Furthermore, they emphasized reducing the dose in the brain due to the relationship between toxicity and detailed normal brain dose-volume information. In our study, even if we assume the same treatment volume using the same PTV margin for both modalities, it was better for GKRS treatment for low (V4Gy%), medium (V10Gy%), and high (V12Gy%) in brain doses. Although “brain volume receiving 12 Gy”, which is essential for SRS treatment, was not statistically significantly different for both treatment modalities, it has been shown that the dose will be reduced in GKRS. There is a statistically significant difference in low and medium dose values in GKRS compared to VMAT treatment.
Thomas et al. [7] have shown that multi-arc VMAT presents similar conformity, equivalent dose fall-off, equivalent moderate, low isodose spill, and equivalent mean dose for multiple target single SRS compared to GKRS. A limitation of our study was the lack of arc arrangement customizing in each case based on tumor localization. Because all of the patients selected for our study were initially treated with GKRS using MR-only planning, as is common practice in GKRS planning, and then replanned with VMAT. In addition, we had to make a standard coplanar arc of VMAT planning for each case due to the low number of cases with different tumor localizations. Therefore, the VMAT technique with coplanar four full arcs was preferred in our study. However, low isodose spill as V4 Gy of the brain can be reduced by choosing different arc numbers and customizing angles of arc for each patient. In addition to this, non-coplanar beams could also provide better GI values with the downside of extending the total treatment time because non-coplanar beam delivery on LINAC requires couch rotation, which can only be performed inside the vault.
GKRS utilizes 192 small circular beams to produce a sphere-shaped dose distribution (shot). All these beams are non-coplanar, which helps to produce superior dose fall-off (low GI) and low dose spill. Due to the size limit of each shot (with the largest diameter at 16 mm), GK needs multiple shots to cover a large target through sphere packing. This is advantageous when the target is close to a critical structure, or it is a high priority to minimize brain volume receiving medium and high doses. However, it leads to substantially longer beam-on time, as much as five times longer than with LINAC. In this study, the beam-on time for GKRS was 20.43 minutes; on the other hand, the mean beam-on-time was 4.80 minutes for LINAC. This analysis is also consistent with the data by Prendergast et al. [20]. They reported an average treatment time of ∼1.2 minutes for various dose fractions ranging from 5 Gy to 16 Gy. It should be remembered that the source of new cobalt at about 4 Gy / minute will reduce the irradiation time by 40%. In addition, the couch rotation usually has a larger isocenter run-off than gantry and collimator rotations, and its movement could trigger patient movement. The OBI on LINAC is excellent for initial patient positioning, and the time required to set up an isocenter on LINAC using CBCT is comparable with that required for the GKRS frameless approach. Although longer beam-on time in GKRS would compare negatively against new developments in LINAC SRS, if one compares the total procedure time, including simulation, treatment planning, and patient-specific quality assurance, the total procedure time of the GKRS compares favorably [21]. Dosimetric studies also reveal a tradeoff between the speed of VMAT and the degree of low dose spill to normal brain [22, 23], as well as the potential for targeting errors due to rotational setup uncertainties [24]. The relatively shorter treatment of LINAC per fraction could be considered advantageous in patients who cannot tolerate SRS for a longer time due to comorbidities.
While LINAC-based systems offer mfSRS with 80% prescription isodose, the GKRS system can deliver a higher maximum and cumulative radiation dose to the treatment volume using a 50% isodose line [25]. Prior studies showed that higher maximum dose and dose heterogeneity of target might play an essential function in a highly beneficial radiobiologic pathway, especially in late-responding tissue such as benign tumors, resulting in a delayed vascular response [26, 27]. The dose heterogeneity of hfGKRS with 50% isodose line may be advantageous in treating solid neoplasm, unlike the LINAC-based systems, which is 80% ∼90% isodose line [28].
Last, we recognize that this study also has several limitations. First, it is a dosimetric comparison study including only a limited number of meningioma patients. Second, we were unable to assess whether the volume of low dose spillage area had a clinical effect on the neurocognitive functions. More clinical studies were warranted.
Conclusion
Both VMAT and GKRS techniques enable to treat large sbMNGs with mfSRS or hfSRS. With both systems, it is possible to achieve dose distributions that conform closely to the shape of the intracranial target, thus sparing the maximum amount of normal brain. However, the GKRS system reveals more effective lower normal brain tissue doses. The advantage of shorter beam-on-time in VMAT could be advantageous in patients who cannot tolerate longer treatments due to comorbidities.
Source of funding
There is no funding for this work.
Conflict of interest
The authors declare that they have no conflict of interest.