
Abstract
BACKGROUND:
Neonatal patients located in incubators are exposed to as many as 159 radiographs until discharge. To reduce the dose exposed to the patient, factors that may cause unnecessary exposure to the patient were judged. When conducting portable X-rays of neonatal patients located in an incubator, it is not easy to determine the exact field size because collimation light is exposed on the acrylic plate, an incubator canopy, and the resulting shadow is reflected on the patient’s body.
OBJECTIVE:
This study aims to measure the organ dose exposed to the patient according to the field size when a portable radiograph is given to a neonatal patient in a neonatal intensive care unit (NICU) incubator.
METHODS:
To identify the absorbed organ dose depending on the radiation field size during portable X-ray examination of neonatal patient, a Monte Carlo N-Particle (MCNP) simulation, a SpeckCalc program, and a neonatal phantom from the ICRP 89 are applied for the calculation. According to the minimal field size (MinFS) standards of the European Commission (EC), the smaller field size is intended to measure tightly from the top of the lung apices to the bottom of the genitals; a larger field size is also calculated by adding 6 cm in width and length.
RESULTS:
Compared to the hospital C condition from the previous study, the larger and smaller field sizes are decreased by an average of 45% and 67%, respectively. Study results also show a 42% reduction in smaller field size compared to the larger field size.
CONCLUSION:
When taking chest and abdomen radiographic images of neonatal patients in incubators, appropriate field sizes are required to prevent inappropriate dose absorption for non-thoracic organs.
Introduction
Neonatal patients are admitted to the Neonatal Intensive Care Unit (NICU) for treatment due to various diseases and physical conditions. At the same time, many general radiographs are performed. As many as 159 radiographs are given to one neonatal patient before being discharged [1–4]. Routine X-ray examination of neonatal patients is performed to check their illness, injection path of drugs, and various disease factors. Minimizing unnecessary radiation exposure to neonatal patients is a crucial issue. Research is being conducted to protect neonatal patients from being exposed to too much radiation. Tissue weighting factors are added to all organs and tissues in the body, which are generally considered to cause cancer by radiation, to be weighted according to their relative sensitivity [5, 6]. These methods are used to calculate the dose of medical exposure depending on the organ and to provide an approximate measurement of the risks that may arise from exposure.
Through the previous study, the organ-absorption dose of neonatal patients was calculated based on changes in object-to-image receptor distance (OID) and source-to-image receptor distance (SID) according to the incubator structure. At this time, the longer SID causes a lower average organ dose in neonatal patients by 36%, and a lower average organ dose by 10% compared to incubators without an acrylic canopy of the incubator [7]. Therefore, it was calculated using the Monte Carlo N-Particle (MCNP) calculation method that lower doses were absorbed by neonatal patients when portable X-ray procedures were performed using an acrylic canopy at the top of the incubator and using short OID and long SID [7].
Based on these studies, we would like to evaluate organ effective dose according to the size of the irradiation field when radiograph is given to a neonatal patient using an incubator structure that could expose a minimum effective dose during portable X-ray. Typically, general radiography increases or decreases the irradiation area as the collimator size is adjusted. At this time, primary radiation has the greatest impact on the patient, showing that out-of-field radiation doses also impact an important role in the patient [8, 9]. According to International Commission on Radiological Protection (ICRP) 128, adjusting the field size using appropriate collimation is essential to reduce unnecessary doses that could be exposed to patients, especially when a radiograph is given to the whole body of a neonatal patient, with the chest, abdomen, and pelvis on one image [10]. Since the radiation dose increases when the irradiation area increases, it is essential to limit the irradiation field size to only the area of diagnostic interest [11–13].
Currently, due to the digitalization of the medical field, computed radiography (CR) and digital radiography (DR) have been actively distributed over the past decades, and post-processing work could improve the quality of images acquired under the overexposure or underexposure conditions [14, 15]. The post-processing work of digital images was radiograph images using wide collimation, and only the necessary areas were selected, increasing the overall radiation dose [11, 14, 15]. Appropriate collimation and field size use is essential because this overall increase in dose could pose a greater risk to neonatal patients undergoing many radiographs.
In addition, a survey of general portable radiograph procedure conditions at a general hospital in the Republic of Korea showed that the size of the X-ray field varies from hospital to hospital and from radiologic technologist to radiologic technologist. Therefore, this study will determine the differences in the radiation exposure dose with the smaller or larger field size of the X-ray exposure to minimize the overall organ-absorbed dose of neonatal patients. The results of the previous study showed the lowest organ-absorption dose in the incubator structure and radiograph condition was used in Hospital C, and this study used MCNP code to find out the amount of radiation exposure to neonatal patients according to the field size.
Materials and methods
As in the previous study, the dose absorbed by the organ (referred to later as ‘organ dose’) was calculated based on factors such as gender, age, weight, height, irradiation area, tube voltage, current time product, filtration degree, irradiation angle, and tissue weighting factor. The location of the radiograph exposure was performed based on neonate views, and a chest and abdominal complex radiography was used to confirm the overall condition of the lungs and abdomen. The incubator structure was set to silicon for the mattress, plastic for the tray to hold the image receptor and the entire structure of the incubator, and acrylic for the upper canopy. The incubator used 70 × 100 × 46 cm3 (W × D × H) based on the Giraffe incubator (GE healthcare, IL, United States), which is used at Hospital C with the lowest organ dose, and 60 kVp, 1.25 mAs, 105 cm SID, and 16 cm OID experimental conditions were conducted (as shown in Fig. 1).
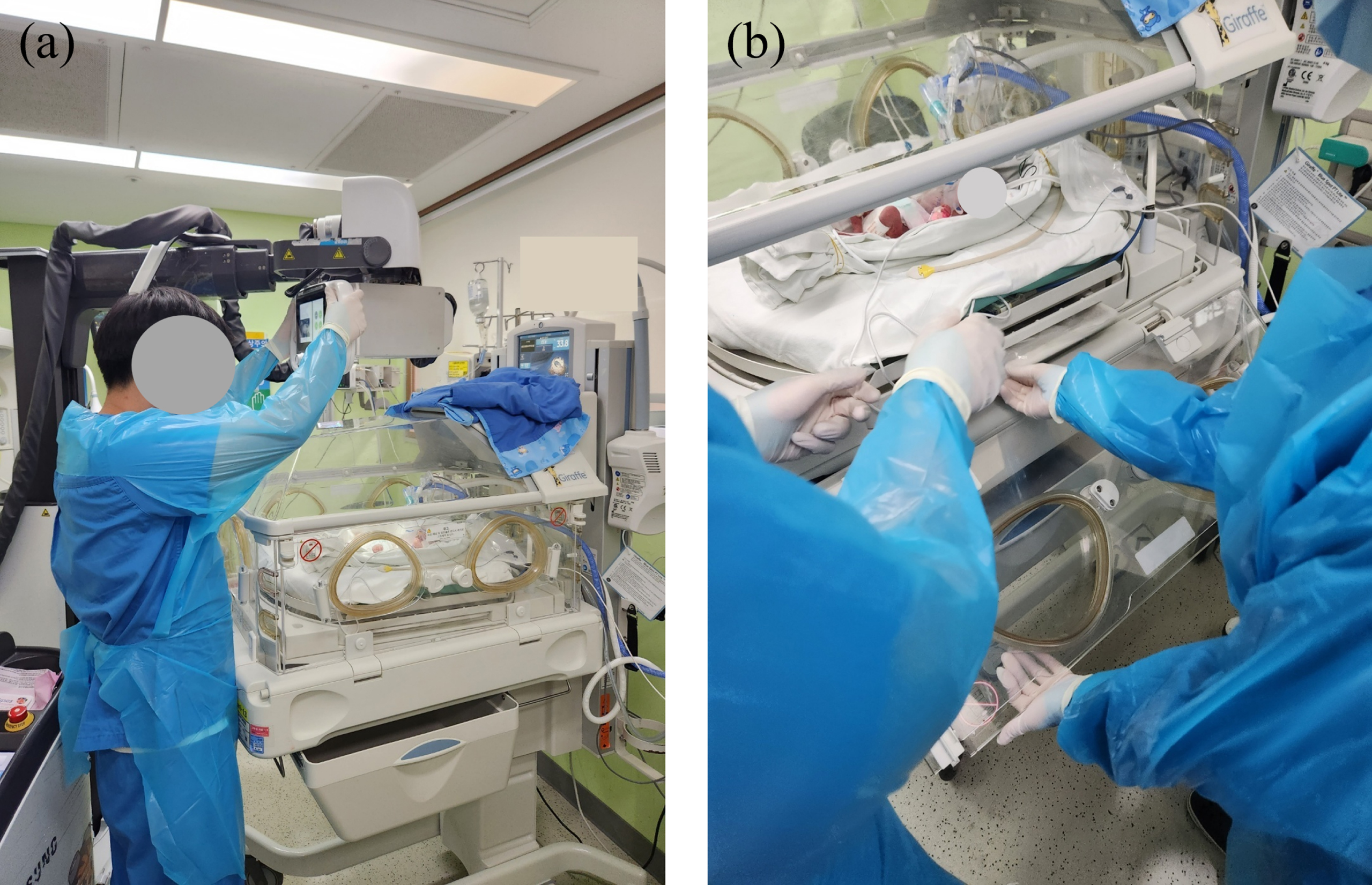
Neonatal patient portable X-ray examination in the incubator (a) by placing X-ray tube over the incubator top and (b) using a plastic tray under the incubator to place the image detector.
ICRP 89 was applied to build the experimental model because it offers MCNP code based on the average newborn information of the physical model [17]. Based on the effects of radiation on the human body, the neonatal phantom evaluated absorption doses for a total of 19 organs using MCNP codes based on the neonatal information of 51 cm in height, 3.5 kg in weight, and 0.24 cm2: lungs, skin, liver, stomach, bladder, testes, brain, esophagus, colon, thyroid, kidneys, pancreas, spleen, thymus, adrenals, gall bladder, heart, small intestine, and genitalia [17]. MCNP simulation was performed using the MCNP5 (Los Alamos National Laboratory, NM, USA) [18, 19]. The Monte Carlo method is software that can simulate bremsstrahlung radiation and calculate the effect of radiation on objects; results can be obtained by repeatedly extracting random samples using probabilistic measurement methods [18, 19].
As with the previous study, the X-ray spectrum was derived from the dose conditions used in the hospital using the SpeckCalc (Institute of Cancer Research, London, United Kingdom) program. The SpeckCalc program would help to obtain the information of a continuous X-ray spectrum under the conditions in the researched hospital and their portable X-ray device. Data on X-ray tubes of the portable X-ray device (Samsung AccE GM85, Samsung Healthcare, Seoul, Republic of Korea) were calculated based on Al inherent filter: 1.4 mm; Cu additional filter: 0.3 mm; target anode angle: 14° [20–22]. The 60 kVp, which is the highest tube voltage value of the hospital setting, was also applied for the calculation. The derived spectral data was calculated as proton source information and added to an MCNP code, calculated using F6 tally [Mev/g] to calculate the dose absorbed by the voxel, and guaranteed a statistical error of less than 5% [23]. As in the previous study, the organ dose was derived by multiplying the derived F6 value by the number of X-rays [7, 24]:
According to minimal field size (MinFS) standards of the European Commission (EC) – “European guidelines on quality criteria for diagnostic radiographic images in pediatrics,” the field size was measured directly from the top of the lung apices to the bottom of the genitals, and from the right to the left flank, under the condition that the patient does not move [25, 26]. The smaller field size was intended to be measured tightly, and the larger field size was calculated by adding 6 cm in width and length in consideration of the patient’s movement [27]. Therefore, the collimator was set to 18 × 25 cm2 (larger field size) and 12 × 19 cm2 (smaller field size) based on the average neonatal view of the newborn.
First, Fig. 2 shows the result of rendering the phantom of a neonatal patient generated based on the MCNP code using the MCNPX visual editor in y = 0 plane and x = 0 plane structures. Looking at Fig. 2(b), it could be seen that a collimator is added in the same structure as in the previous study. Next, Fig. 3 also shows the effect of the radiation dose generated based on the MCNP code using the MCNPX visual editor on patients with the y = 0 plane and x-0 plane structures.
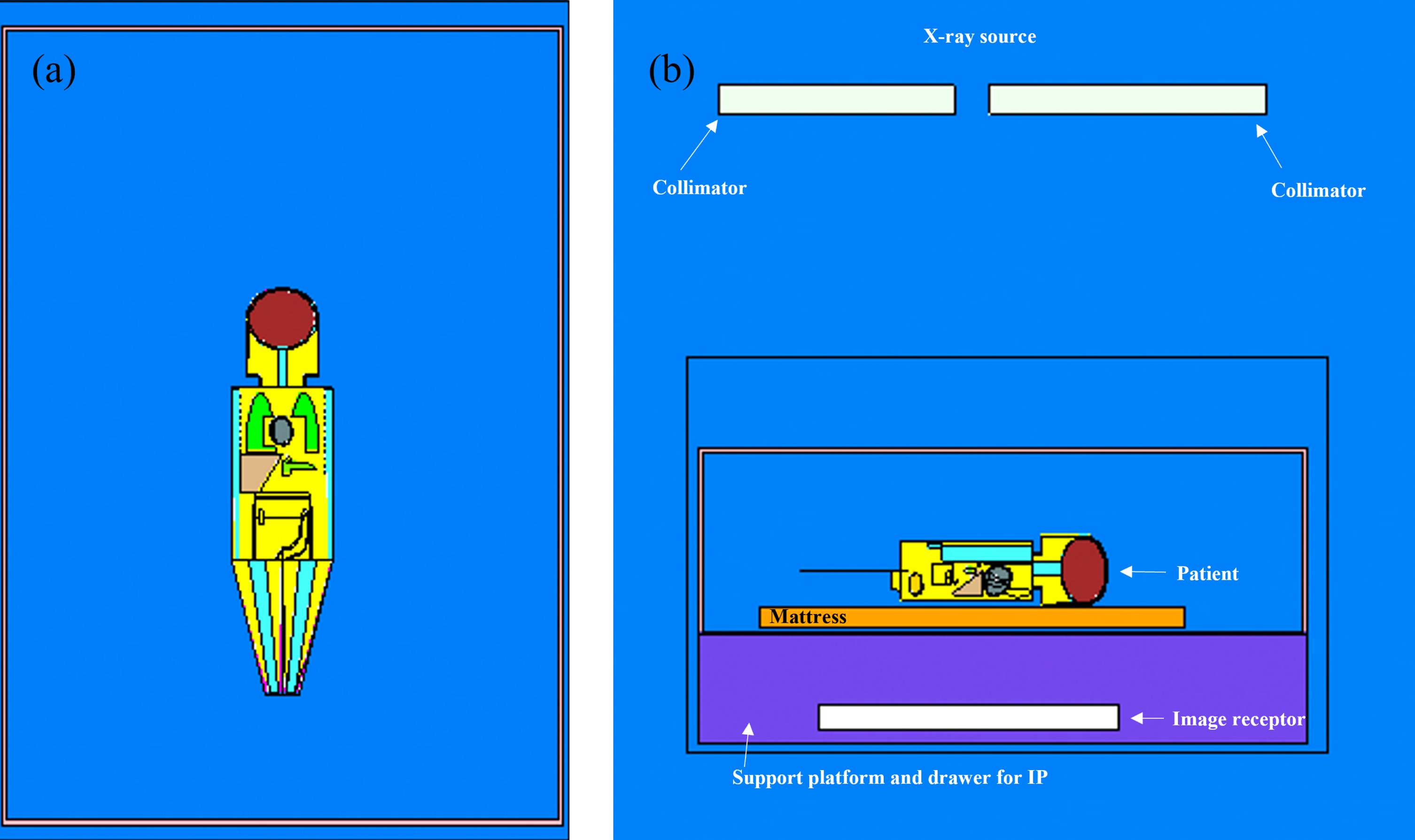
A cross-sectional image of the neonate mathematical phantom inside the incubator at (a) y = 0 and (b) x = 0 plane (rendered by the MCNPX Visual Editor).
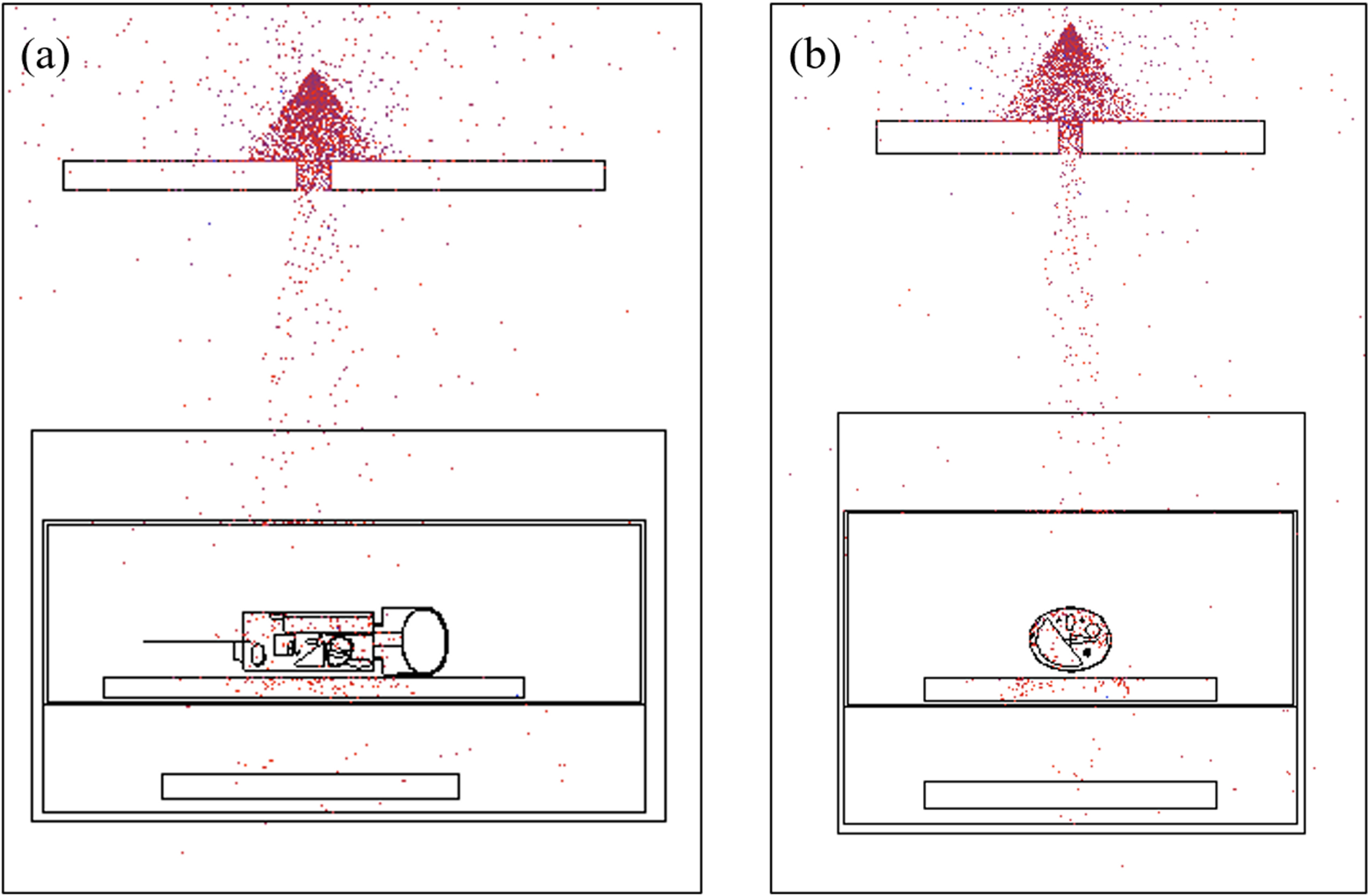
The neonate phantom inside the incubator gets radiation exposure from the X-ray machine at (a) y = 0 and (b) x = 0 plane (rendered by the MCNPX Visual Editor).
When performing a portable X-ray procedure on a neonatal patient located in an incubator, the dose exposed to the patient according to the collimation size is found to have the lowest organ dose when the field size is the smallest. As with the results of the previous study, exposure in the kidneys was highest at 7.23μGy and 4.13μGy, followed by adrenal glands, skin, lungs, and spleen. All results showed less than 1% stochastic error for all organs. Due to the change in field size, all organs absorbed lower doses in the smaller field size (Fig. 4).
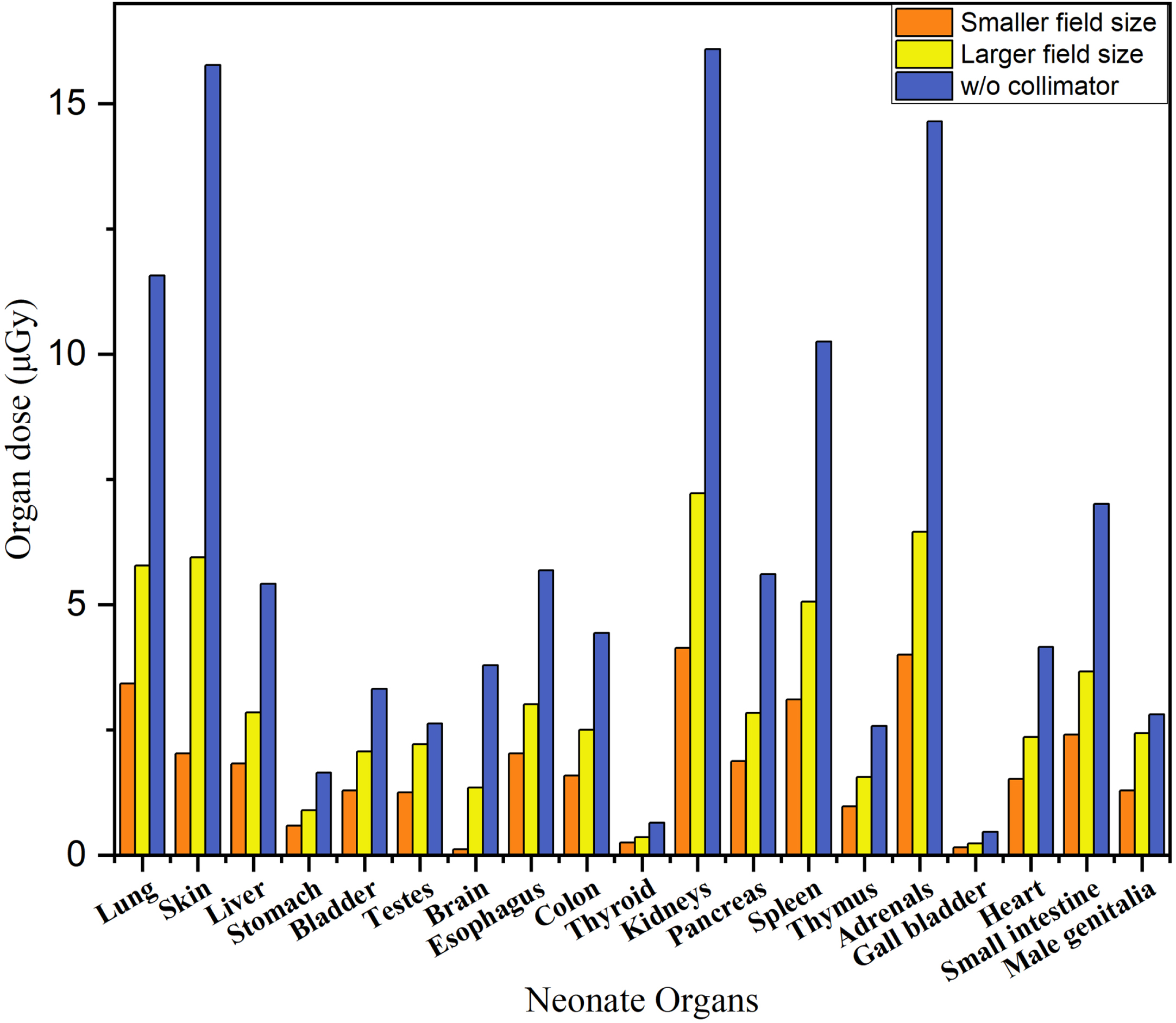
Organ dose (μGy) in a neonatal patient undergoing a portable X-ray procedure calculated from MCNP 5 depends on the radiation field size in the incubator.
Table 1 shows the organ dose (μGy) result from the MCNP simulation. There are three columns: smaller field size, larger field size, and Hospital C result based on the neonatal organs. Hospital C results are generated from the previous study to compare with smaller and larger field size results. In addition, the percentage in the parenthesis is a comparison between smaller or larger field sizes and Hospital C results. Since the organ dose of a smaller or larger field size is lower than Hospital C setting, the result shows negative. As a result, the larger field size showed a 13% to 64% reduction in organ doses depending on the organ compared to collimator-free conditions (Table 1). The smaller field size showed a 52% to 97% reduction in organ doses depending on the organ compared to collimator-free conditions (Table 1).
Organ dose (μGy) derived from the MCNP results of different field sizes: smaller field size (comparison between smaller field size and hospital C), larger field size (comparison between larger field size, and hospital C) and hospital C result
Proper collimation setting not only reduces unnecessary radiation exposure but also improves the quality of radiographic images, which is very important for radiation-sensitive newborns [25–28]. With an X-ray procedure of neonatal patients located in an incubator, it is difficult to assume the exact field size of the patient because collimation light is exposed on an incubator canopy, the acrylic plate, and the resulting shadow is reflected on the neonatal patient’s body. According to the research, 50% to 90% of neonatal radiographic images exceed the appropriate field size [29]. Inadequate collimation can expose excessive radiation to non-thoracic organs, such as the humerus, mandible, and femur [2, 30]. Infants are more sensitive to radiation; therefore, they have a high risk of cancer even with a small dose, and the risk of cancer in these neonatal patients has been shown to increase by 2.5 boys and 2.9 girls per 106 neonatal view radiographs [27, 31, 32]. Even if this is a low probability, the risk is significantly increased when an average of 10 radiographs are performed, or up to 159 radiographs are performed while neonatal patients are hospitalized [1–4].
In this study, the Monte Carlo method was used to simulate organ-absorption doses to neonatal organs according to the field sizes exposed to radiation during portable general radiographs. Based on the giraffe incubator and Hospital C neonates’ radiograph conditions with the lowest organ dose in the previous study, setting the incubator structure, SID, OID, kVp, mAs, and patient phantoms equally, added smaller field size and larger field size to evaluate organ dose.
According to the results of the MCNP simulation study, the organ-absorption dose of neonatal patients located in the incubator was measured to be the highest in the Hospital C conditions without collimation, followed by larger field size and smaller field size. It showed an average decrease of 45% in the larger field size compared to without the collimation setting, and an average decrease of 67% in the smaller field size compared to without the collimation setting (table 1). When comparing the larger field size and the smaller field size, it shows an average 42% decrease (table 1). Reducing the field size using appropriate collimation and field size is considered essential for lowering the overall organ-absorption dose of neonatal patients located in the incubator. Therefore, MCNP simulations have demonstrated that setting an appropriate field size reduces the overall scatter radiation and reduces the dose exposed to patients.
Additionally, according to a study by Donald Frush and Huda Walter, the most important way to reduce patient exposure is to reduce scatter radiation, and the simplest way is to aim the radiation closest to the anatomical structures [2, 33]. In addition, 96% of X-ray procedures are exposed to more than 25% of the field size [34]. In digital systems, it is mentioned that if the background and organs in areas are different from what was not expected in the histogram after radiographic exposure, the overall contrast decreases [33–35]. In addition, it is mentioned that the use of appropriate collimation and field size reduces the dose exposure to patients by 65% [36].
Therefore, setting an appropriate field size reduces the overall scatter radiation, reduces the dose exposed to neonatal patients, improves image quality, and improves contrast and resolution in particular [10, 26, 27, 34, 37]. If the field size is too large, it not only increases the overall amount of scatter radiation, damaging the image resolution, but it also causes irradiation to body parts outside the area of interest. Therefore, it is necessary to maintain the minimum field size to avoid this extreme radiation exposure. According to EC guidelines, the tolerance level for the maximum field size after neonatal periods should be at least 2 cm greater than the minimum field size, but it is recommended that the tolerance level at the edge should be minimized to less than 1 cm for neonatal patients [26]. It is essential to proceed with the radiograph by limiting the beam size to the area of interest.
The various body sizes of patients cause difficulties for radiologic technologists to determine dose conditions. Although using automatic exposure control (AEC) is excellent in exposing patients to appropriate radiation doses, it is not recommended for neonatal patients because the AEC chamber is often larger than the size of the neonatal patient [13]. In addition, AEC is not suitable for pediatric patients because it is characterized by extending the minimum exposure time [26]. Reducing patient movement is just as important a factor as reducing the appropriate field size. The ICRP 122 guidelines state that the benefits of newborns should be exploited for radiograph procedures [38]. Since the newborn patient is calm or asleep after lactation, it is mentioned that using this appropriate time can minimize the patient’s movement, which can reduce appropriate field size and repeated exposure.
The study has demonstrated that lowering the dose exposed to neonatal patients by proposing field size with appropriate collimation use is an essential factor in improving image quality, as well as reducing overexposure to patients. However, there are pros and cons when the field size is applied in clinical practice; the advantage is that the smaller the field size used, the less unnecessary dose exposed to the neonatal patient, allowing the patient to be protected from overexposure. There is also a disadvantage here. A too-tight field size does not contain the necessary organs, increasing the risk of diagnostic errors or requiring a second exposure [10, 34]. In addition, because the size of neonatal patients is so small, it could be difficult not to include body parts other than the chest and abdomen (Fig. 5) [13]. However, the study notes that only 5% of newborn chest radiographs were retaken due to the field size error [38, 39]. Therefore, it is believed that appropriate education, training, and protective rules are needed to implement as low as reasonably achievable (ALARA) safety principles to set minimal field size using ideal collimation.

The radiographic image of the chest and abdomen (neonatal view) of an infant weighing about 1,600 g shows that it is difficult to include only the patient’s chest and abdomen in the image [13].
In this study, the MCNP simulation is used to evaluate the radiation dose absorbed into the organs of radiation vulnerable patients according to the field size during portable general radiographs of neonatal patients located in incubators. As a result, the result shows an average 45% reduction in organ dose on a larger field size and an average 67% reduction on a smaller field size than without collimation condition. Also, the smaller field size shows an average 42% reduction rather to the larger field size. Therefore, there will be many restrictions on examining neonatal patients in an incubator, but radiologic technologists would reduce the dose exposed to patients and minimize the field size to obtain only the necessary information.
Footnotes
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (RS-2023-00242892).