
Abstract
BACKGROUND:
SRS and SRT are precise treatments for brain metastases, delivering high doses while minimizing doses to nearby organs. Modern linear accelerators enable the precise delivery of SRS/SRT using different modalities like three-dimensional conformal radiotherapy (3DCRT), intensity-modulated radiotherapy (IMRT), and Rapid Arc (RA).
OBJECTIVE:
This study aims to compare dosimetric differences and evaluate the effectiveness of 3DCRT, IMRT, and Rapid Arc techniques in SRS/SRT for brain metastases.
METHODS:
10 patients with brain metastases, 3 patients assigned for SRT, and 7 patients for SRS. For each patient, 3 treatment plans were generated using the Eclipse treatment planning system using different treatment modalities.
RESULTS:
No statistically significant differences were observed among the three techniques in the homogeneity index (HI), maximum D2%, and minimum D98% doses for the target, with a p > 0.05. The RA demonstrated a better conformity index of 1.14±0.25 than both IMRT 1.21±0.26 and 3DCRT 1.37±0.31. 3DCRT and IMRT had lower Gradient Index values compared to RA, suggesting that they achieved a better dose gradient than RA. The mean treatment time decreased by 26.2% and 10.3% for 3DCRT and RA, respectively, compared to IMRT. In organs at risk, 3DCRT had lower maximum doses than IMRT and RA, but some differences were not statistically significant. However, in the brain stem and brain tissues, RA exhibited lower maximum doses compared to IMRT and 3DCRT. Additionally, RA and IMRT had lower V15Gy, V12Gy, and V9Gy values compared to 3DCRT.
CONCLUSION:
While 3D-CRT delivered lower doses to organs at risk, RA and IMRT provided better conformity and target coverage. RA effectively controlled the maximum dose and irradiated volume of normal brain tissue. Overall, these findings indicate that 3DCRT, RA, and IMRT are suitable for treating brain metastases in SRS/SRT due to their improved dose conformity and target coverage while minimizing dose to healthy tissues.
Introduction
Stereotactic techniques are a type of advanced radiation therapy that has been more widely applied in recent years in the treatment of brain metastases by delivering a large dose of radiation on a single fraction dose or, multi-fraction (2-5 fractions) [1–3]. Modern, linear accelerators equipped with Multileaf collimator (MLC) and onboard imaging systems are capable of SRS/SRT delivery with high precision. Different radiotherapy modalities such as three-dimensional conformal radiotherapy (3D-CRT), intensity-modulated radiotherapy (IMRT), and volumetric modulated arc therapy have widely been used for stereotactic radiosurgery (SRS) treatment in brain metastases [3]. 3D-CRT is a treatment method that utilizes multiple radiation treatment ports that are shaped to the outer contour of the target volume [4, 5]. Intensity-modulated radiation therapy (IMRT) utilizes MLC in a dynamic sweeping or step-and-shoot mode, where the intensity of radiation beams is modulated [6]. RapidArc® (RA) is an advanced radiotherapy technique developed by Varian Medical Systems in Palo Alto, CA [7]. It delivers highly precise volumetric-modulated arc therapy (VMAT) and was clinically presented by Otto in 2008 [7, 8]. RA is a specialized form of IMRT that administers radiation in a single 360-degree rotation around the patient, resulting in highly conformal dose distributions [8, 9].
RA enhances target volume coverage while minimizing exposure to healthy tissue by simultaneously changing the dose rate, gantry rotation speed, and MLC leaves during treatment delivery [9, 10].
The use of these techniques in SRS/SRT for brain metastases has been proven and discussed in several literature, while other literature studied the comparison between these techniques and showed differences in plan quality.
Hamilton et al [11] used 3DCRT with a single isocenter using multiple non-coplanar arcs and multiple noncoplanar conformal static fields for SRS in intracranial lesions. They found that using multiple noncoplanar conformal static fields reduces the amount of normal tissue that receives high and intermediate doses and provides a uniform dose within the tumor volume compared to a single isocenter and multiple arcs. However, this technique is not effective for tumor shapes lacking rotational or mirror symmetry axis [11]. In another study by Cardinale et al [12], analyzed the effectiveness of IMRT plans versus conventional arc therapy and 3D-CRT plans on three intracranial target shapes that were not spherical. The study’s findings indicated that IMRT led to better dose conformity and reduced the amount of radiation delivered to healthy tissue [12]. Elhateer et al. [13] compared Helical Tomotherapy (HT), Fixed-field (IMRT), and non-coplanar (3DCRT) - for the treatment of eight meningiomas located at the base of the skull. The study found that HT provided the most effective target coverage and dose homogeneity. Compared to 3DCRT, both HT and fixed-field IMRT improved the protection of organs at risk, but this came at the cost of a lower CI [13]. Chi Huang et al. [14] evaluated the use of SRS with single-isocenter VMAT with conventional multi-isocenter dynamic conformal arc therapy (DCAT) and 3DCRT on 17 patients with 2 to 5 brain metastatic. They found VMAT plans showed equivalent or better conformity index and improved quality of coverage compared to DCAT/3D-CRT plans. The study of Wang et al. [15], found that critical organ doses in both RapidArc (RA) and intensity-modulated radiation therapy (IMRT) were deemed acceptable. However, RA plans were found to result in higher doses to the critical organs when compared to IMRT plans. Despite this, the RA technique demonstrated higher conformity and gradient index than the IMRT technique for brain radiosurgery. Roa et al. [16] found that IMRT, 1-arc RA, and 2-arc RA plans demonstrated similar clinical outcomes in terms of dosimetric conformity, homogeneity, and organs-at-risks (OARs) sparing. The same was found in another study by Ruschin et al. [17], which concluded there was no significant difference in terms of conformity index, homogeneity index, or mean dose to the normal brain between IMRT and VMAT. However, VMAT was found to have a shorter treatment time compared to IMRT. Recent studies evaluated some of these techniques and compared them with Gamma Knife (GK) and CyberKnife (CK). KIM et al. [18] found that VMAT led to improved conformity, similar dose fall-off, similar low and moderate isodose spill, and similar mean dose for treating multiple metastases. The study concluded, that the use of VMAT can produce similar results to GK (Gamma Knife) plans, but with increased efficiency, particularly when using a high-intensity linac. On the other hand, Dong et al. [19] compared CK, Linac-based VMAT, and GK for 10 patients with large brain tumors (>3 cm). The study observed that GK showed a lower Paddick gradient index and brain tissue volume receiving 15 Gy (V15) compared to CK and VMAT. The conformity index was similar among all techniques. The study concluded that GK radiosurgery demonstrated significantly better sparing of normal brain tissue near the target compared to Linac-based VMAT. Another study by Zhang et al. [20] found that noncoplanar volumetric modulated arc therapy (VMAT) is a more efficient treatment option for brain metastases that are located far from organs at risk (OARs) when compared to IMRT and coplanar-VMAT. Additionally, noncoplanar VMAT demonstrated a similar dose falloff to CyberKnife at high-dose levels, but a slower falloff at moderate-to-low dose levels. Furthermore, noncoplanar VMAT plans require fewer monitor units and a shorter beam on time compared to CyberKnife plans [20]. The observed variations in previous studies might be influenced by the precise location of the targeted area and its proximity to critical brain structures. These factors can impact the differences in radiation dose distribution among various treatment techniques. Our study sought to evaluate effective treatment techniques for brain metastases using Stereotactic Radiosurgery (SRS) or Stereotactic Radiotherapy (SRT). Our objective was to contribute to the existing literature by investigating treatment outcomes with three specific techniques: 3D-CRT, IMRT, and RA. This comparative analysis enhances the overall evidence and understanding of the advantages and limitations of these treatment modalities by determining the optimal treatment strategy based on observed dosimetric differences and overall effectiveness.
Methods
This section outlines the study’s methods and provides detailed information on the data collection process, treatment planning techniques, dose calculation algorithms, and statistical analyses performed to compare the dosimetric outcomes among the patients.
Material
The study included ten patients with brain metastases with an average volume of 1.37 cc and a range of 0.1-7 cc. Seven patients received stereotactic radiosurgery (SRS) and three received patients with stereotactic radiotherapy (SRT). The total prescribed dose was in the order of 18 to 25 Gy. (CT) scan with a slice thickness of 1.25 mm was performed on the patients. Magnetic resonance imaging (MRI) images were used to fuse with CT for accurate delineation of the target. A radiation oncologist used axial MRI slices to delineate the gross tumor volume (GTV) for each patient after confirming the fusion. Critical organs, such as the normal brain, brainstem, optic chiasm, right and left optical nerves, and right and left eyes were also contoured.
Treatment planning
For each patient, 3 plans were generated using the Eclipse treatment planning system (Varian Medical Systems, Palo Alto, USA). Anisotropic Analytical algorithm (AAA) dose calculation algorithm is used for the three techniques, (3DCRT, IMRT, RA). Table 1 displayed the number of beams and isocenters used for each patient in the three techniques (3DCRT, IMRT, and RA).
Number of Beams/Arcs, and isocenters that were used for each patient in three different techniques
Number of Beams/Arcs, and isocenters that were used for each patient in three different techniques
For 3DCRT plans, 7-9 static fields are distributed co-planner and noncoplanar, avoiding entrance from the other brain hemisphere, Gantry angles are selected based on the best beam eye view and small SSD. noncoplanar fields are settled by moving the couch every 25-30 degrees. parallel opposing fields are excluded, and no more than 2 fields are set for the same plane. different collimator angles are optimized for each field, for best fitting of MLC to the Planning Target Volume (PTV). Jaws are adjusted to fit the PTV with a 2 mm margin while the MLC are fitted with zero margins, in some patients one or more of the jaws are optimized manually to fit with 1 mm or zero margins to the PTV to protect OAR or enhance the conformity from one side.
IMRT plans used the same number of fields, gantry angles, and collimators as 3DCRT plans. Two ring structures around the PTV are created, the first 5 mm just beyond the PTV and the other 2 cm from the GTV and cropped from the first ring, these two ring structures aim to control the dose gradient beyond the PTV and limit the 50% isodose within the first 5 mm from the PTV. Another PRV structure is created as Brain-PTV to limit the 12 Gy to the normal brain tissues. Dose constraints for the PTV are tabulated, the prescribed dose was defined as the Minimum constraint while the maximum constraint was defined as not exceeding 120-125% of the prescription. OARs constraints are defined to minimize OAR dose.
Rapid Arc (RA) plans were generated using 6 to 10 noncoplanar arcs, which are distributed to be 25–30 degrees apart. The arcs may be minimized or excluded to avoid the other hemisphere of the brain. Different collimator angles are used for each arc and fitted to the planning target volume (PTV) with a 1 mm margin.
All plans are normalized to the 3D dose maximum of the plan, and the dose prescribed to the isodose line value that covers 99% of the PTV volume.
The study compared the plan quality between three techniques based on target coverage, conformity index (CI), Homogeneity Index (HI), gradient index (GI), dose delivered to normal brain tissues, and Treatment time (TM). Maximum (Max) doses to organs at risk were also determined using the dose-volume histograms (DVH) of each plan.
The volumes (V3Gy, V6Gy, V9Gy, V12Gy, and V15Gy) of normal brain tissues were extracted. Minimum and maximum dose metrics for GTV were defined as D98% and D2%, which represent the dose received by 98% and 2% of volume [21]. The Conformity Index (CI) and Homogeneity Index (HI) were evaluated using The Radiation Therapy Oncology Group 1993 (RTOG) [22]. CI was expressed as the ratio between the prescription isodose volume (PI) to the target volume (TV).
CI was expressed as the ratio between the prescription isodose volume (PI) to the target volume (TV). The conformity index must fall within the range of 1.0 and 2.0 to be considered acceptable, and if this range is achieved, it indicates that there is no deviation from protocol [22]. Keeping the ratio below 1.2 is recommended to reduce the volume of tissue that is exposed to an ablative dose [22].
The Homogeneity Index (HI) is a quantitative measure used to assess the uniformity of dose distribution within a target volume. It is calculated based on the prescription isodose line, which is chosen to encompass the tumor margin [23]. The HI is determined by dividing the maximum dose within the treatment volume by the prescription dose. If the homogeneity index is equal to or less than two, the treatment adheres to the protocol requirements [22, 24]. This index provides valuable information about the consistency of dose delivery within the target volume.
Another evaluation tool was the gradient index (GI). the Gradient Index was calculated by using the Paddick GI formal, which was defined by the ratio between the volume of the 50% isodose (V50) and the Volume receiving 100% of the prescription dose [25]. A lower GI value indicates a sharper transition between the high-dose region (target volume) and the surrounding normal tissue [26]. Paddick et al. (2006) discuss that a GI value below 3 is considered indicative of a good plan [25, 26].
The study also recorded delivery parameters, which included monitor units (MUs) and beam-on time (BT). These parameters are important for evaluating the efficiency and practicality of each treatment technique.
Statistical analysis
A normality test was conducted using the Shapiro-Wilk test to test the normal distribution of the data. The study compared the three treatment techniques using one-way repeated measures (RM) ANOVA for parametric data and Friedman’s test for non-parametric data. To identify which treatment techniques differed from each other, pairwise comparisons were conducted using the Bonferroni test correction for parametric data and the Wilcoxon test for non-parametric data. A p-value less than 0.05 was considered statistically significant for all tests, while a p-value greater than 0.05 indicated no significance. The data results were reported as mean values±standard deviations (SD).
Results
The study found that all three techniques (3DCRT, IMRT, and RA) were clinically acceptable with a comparable normalization value of 78.6%, 81.9%, and 82.2% respectively. However, variations in dosimetric parameters were observed among the techniques. Figures 1–3(a, b, and c) displayed the dose distributions and dose-volume histograms (DVHs) as an example of three techniques. Figure 1 illustrated the axial dose distributions around GTV in both the axial and coronal planes for each technique. Additionally, Fig. 2 presented a comparison of the dose-volume histograms (DVH) for the gross tumor volume (GTV) using three different techniques. in this figure, The DVH plots show the relationship between the radiation dose delivered to the GTV and the volume of the GTV receiving that dose. Furthermore, Fig.3 (a, b, and c) provided a detailed explanation of the dose-volume histograms (DVHs) exported from the Eclipse treatment planning system for each technique: 3DCRT, IMRT, and RA respectively. The DVHs offer a quantitative representation of the radiation dose distribution within the target volume and surrounding normal tissues for each treatment technique.
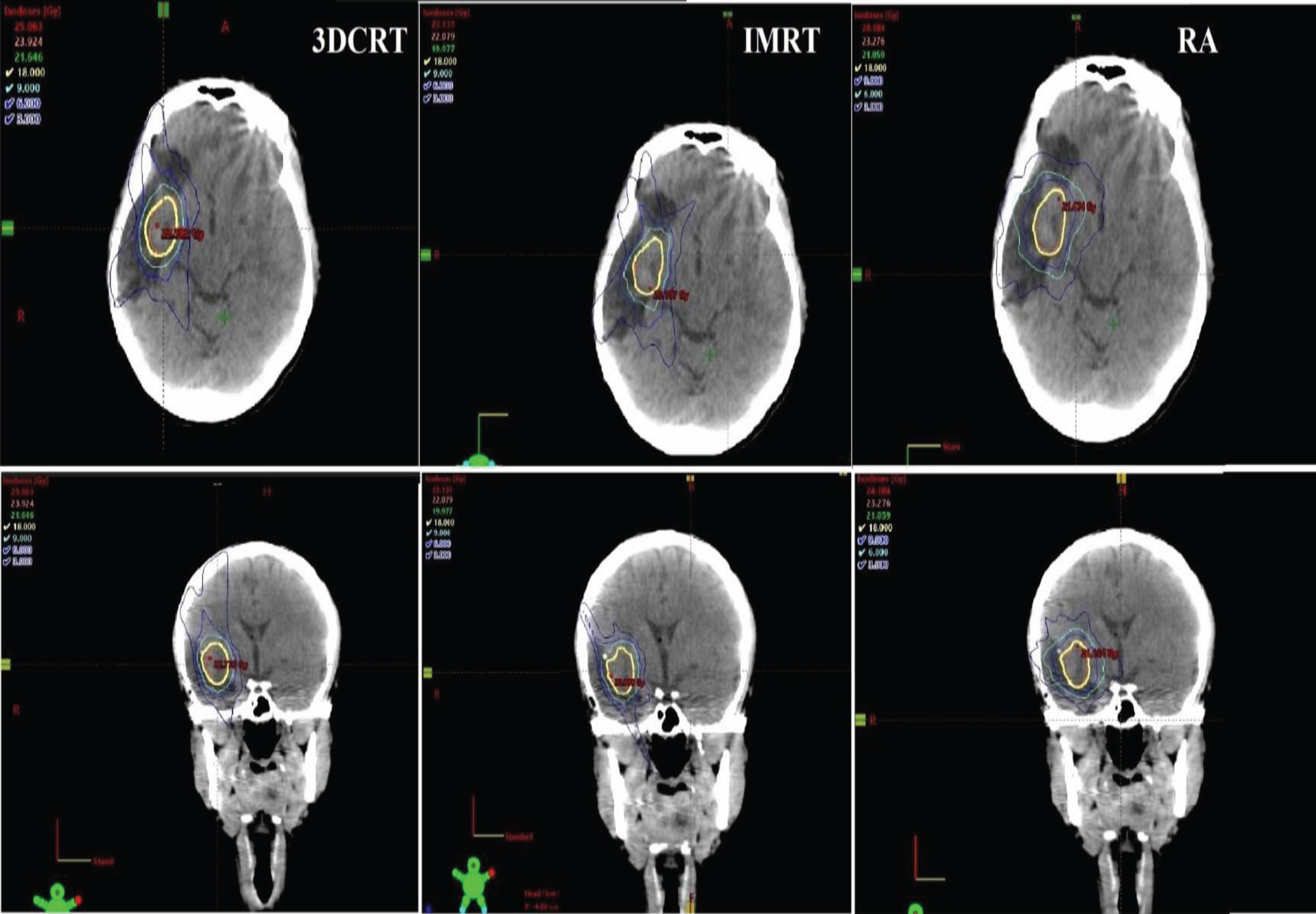
A comparison of the dose distributions between the three techniques for a representative patient in the axial and coronal planes.
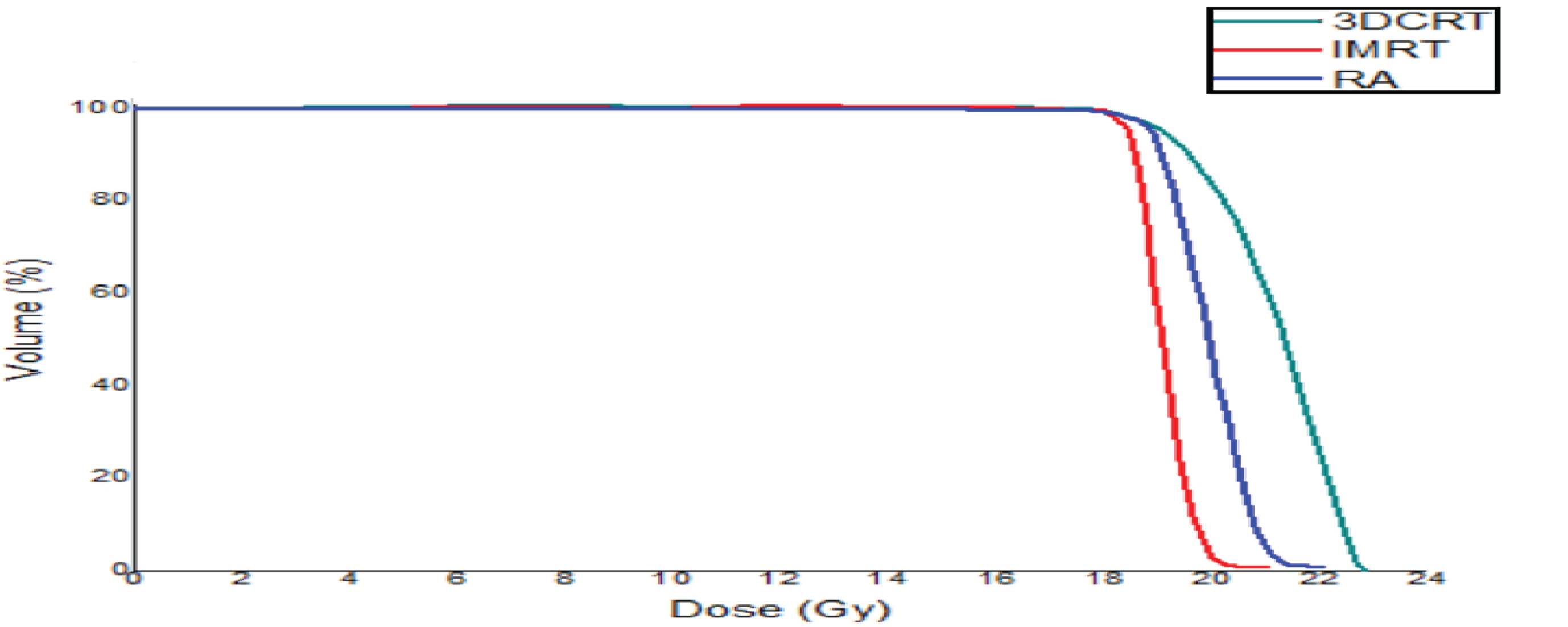
A comparison of the dose-volume histogram (DVH) for GTV between the three techniques for a representative patient.

(a, b and c). The dose-volume histogram (DVH) for the same patient for 3DCRT, IMRT, and RA techniques respectively.
Table 2 presented the dosimetric parameters results obtained from analyzing the dose-volume histogram for GTV. According to Table 2, there was no statistically significant difference in the mean dose between RA and IMRT techniques, P = 0.36. The mean dose values of 3DCRT were higher when compared to both RA and IMRT. The difference in mean dose values between 3DCRT and RA was statistically significant, with a p = 0.024. However, there was no significant difference between 3DCRT and IMRT, with a p = 0.24.
Compare the dosimetric parameters results for GTV between the three techniques (Mean±SD)
Compare the dosimetric parameters results for GTV between the three techniques (Mean±SD)
The maximum dose (D2%) and minimum dose (D98%) did not show any statistically significant differences among the three techniques, as the p-value >0.05. However, 3DCRT had a higher maximum dose (D2%) compared to both RA and IMRT. Figure 4, illustrated the mean dose, maximum dose (D2%), and minimum dose (D98%) dose comparison between 3DCRT, IMRT, and RA techniques for each patient respectively.

Mean dose, maximum dose (D2%), and minimum dose (D98%) dose comparison between 3DCRT, IMRT, and RA techniques respectively.
In terms of the conformity index, the study found significant differences in the conformity index (CI) between 3DCRT and RA (P = 0.02), and no statistically significant differences between RA with IMRT, P = 0.60, or between IMRT with 3DCRT, P = 0.074. The RA technique demonstrated better conformity than both IMRT and 3DCRT techniques, with conformity index (CI) values of 1.14±0.25.
Concerning the homogeneity index, no statistically significant difference was observed between the three techniques P > 0.05, all techniques showed a homogeneous dose.
The study found that the dose gradient index (DGI) was lower value for both 3DCRT (6.76±4.34) and IMRT (6.92±4.48) compared to RA (9.03±7.55). The difference in DGI values between 3DCRT and RA was statistically significant, with a P = 0.008. However, there was no significant difference between IMRT and RA, with a P = 0.06. Figure 5, showed the CI, HI, and GI values for each patient for each of the three techniques. Table 2 also provided the monitor units (MUs) and treatment time (TM) for the three treatment techniques. The mean MUs for IMRT and RA were significantly higher compared to 3DCRT, as evidenced by p-values of 0.005 and 0.022, respectively. Additionally, the mean treatment time for 3DCRT was significantly shorter than for RA and IMRT, with times of 11.67 minutes, 14.21 minutes, and 16.07 minutes, respectively, with p-values of 0.022 and 0.005.
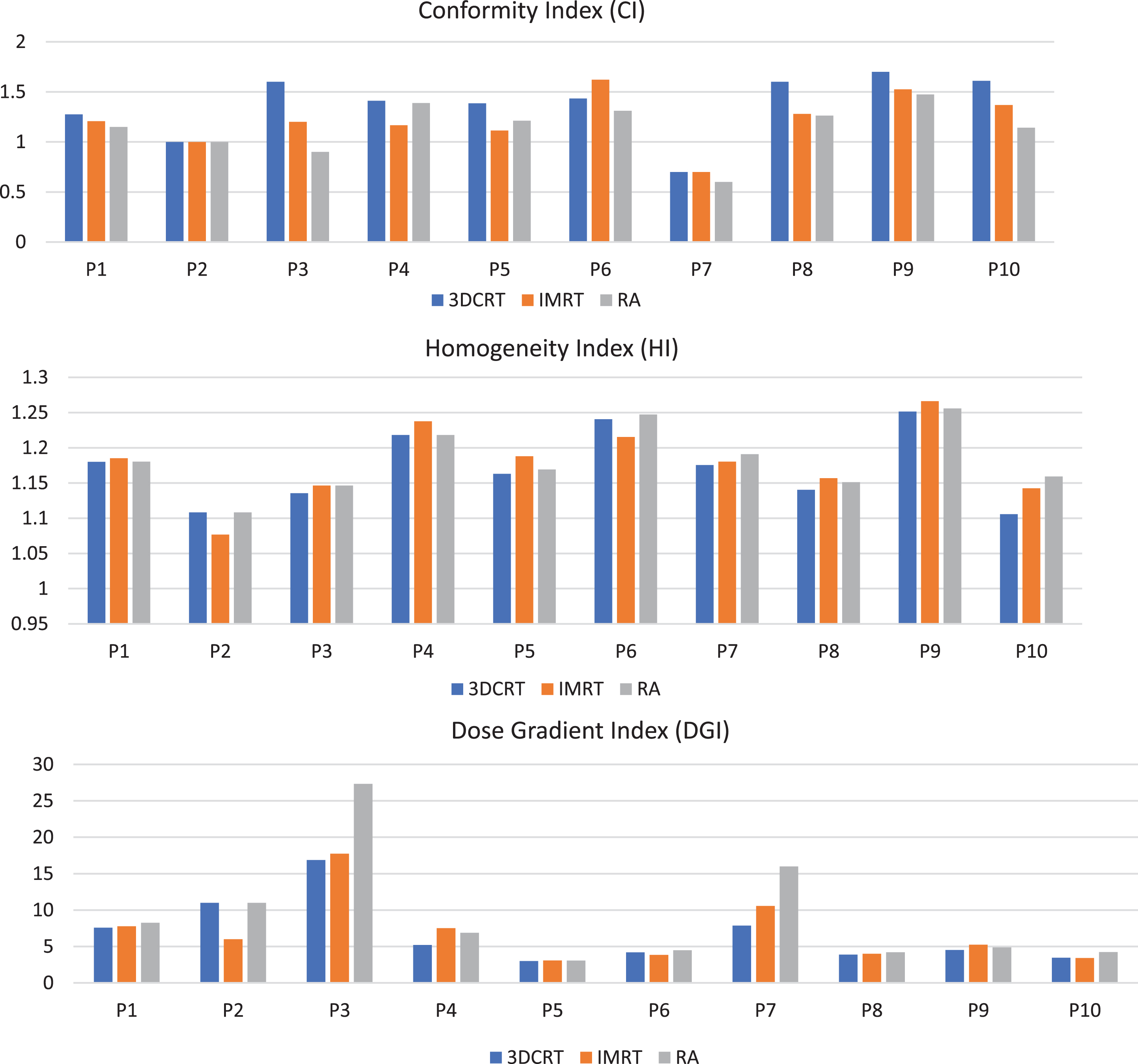
Conformity Index (CI), Homogeneity Index (HI), and Dose Gradient Index (DGI) comparison between 3DCRT, IMRT, and RA techniques respectively.
Table 3 displayed the results of the analysis of normal brain tissue doses and the brain volume ranging from V15 Gy to V3 Gy for each of the three techniques, along with p-values. Figure 6, displayed the irradiated volumes of normal brain tissue with the dose among the three techniques. Based on Table 3, there were no statistically significant differences in the mean brain dose for the three techniques. Despite this, IMRT had a lower mean dose compared to both 3DCRT and RA. The maximum dose was lower in RA (22.95±2.69 Gy) compared to 3DCRT (25.17±3.32 Gy) and IMRT (23.4±2.69 Gy), but the difference between RA and IMRT was not significant with p-value=0.34. The dose delivered to the brain volume ranging from V15 Gy to V9 Gy did not show any statistically significant difference among the three techniques. Nonetheless, we found statistically significant differences between the techniques for V6 Gy and V3 Gy, with RA having lower values compared to IMRT and 3DCRT.

Compared the irradiated volumes of normal brain tissue for 3DCRT, IMRT, and RA techniques.
Comparisons of dosimetric Parameters between 3 techniques for Normal Brain Tissue (Mean±SD)
Our results showed that mean and maximum doses, delivered to OARs were very low for all techniques. However, significant differences were observed between the techniques.
Table 4 presented (mean values±standard deviation (SD) data on the mean, and maximum doses delivered to OARs for three different techniques. The table also includes p-values that indicate any statistically significant differences in dose delivery between the techniques.
Comparison of dose metrics (Mean and Maximum doses) Gy for organs-at-risk (OARs) among three
Comparison of dose metrics (Mean and Maximum doses) Gy for organs-at-risk (OARs) among three
Based on Table 4 the mean dose delivered to the right eye was lowest for 3DCRT (0.028±0.018) and highest for RA (0.15±0.11), with IMRT falling in between (0.030±0.016). The p-value for the mean dose indicated that there was a statistically significant difference between all techniques (p = 0.001). Despite this, there was no statistically significant difference between 3DCRT and IMRT (p = 0.54). The maximum dose was highest for RA (0.35±0.19), followed by IMRT (0.26±0.10) and then 3DCRT (0.20±0.12). Even so, there was no statistically significant difference between any of the techniques (p = 0.065).
For the right lens, there was a statistically significant difference in the mean dose between all techniques (p = 0.006). RA resulted in a higher mean dose (0.134±0.092 Gy) compared to 3DCRT (0.038±0.029 Gy) and IMRT (0.020±0.010 Gy). However, there was no statistically significant difference between 3DCRT and IMRT (p = 0.10). The maximum dose delivered was highest for RA (0.17±0.12 Gy), followed by IMRT (0.015±0.010 Gy) and then 3DCRT (0.014±0.010 Gy), there was a statistically significant difference between all techniques (p = 0.003). Even so no statistically significant difference between IMRT and 3DCRT (p = 0.88).
The left eye received the lowest mean dose with 3DCRT (0.022±0.013 Gy) followed by IMRT (0.025±0.016 Gy) and the highest dose with RA (0.11±0.09 Gy). The p-value for the mean dose indicated that there was a statistically significant difference between the three techniques (p = 0.007). On the other hand, there was no statistically significant difference between 3DCRT and IMRT (p = 0.59). For the maximum dose, the left eye received the highest dose with RA (0.25±0.17 Gy), followed by IMRT (0.10±0.08 Gy), and the lowest dose with 3DCRT (0.09±0.04 G). The p-value showed that there was a statistically significant difference between RA and 3DCRT (p = 0.008). No statistically significant difference between the (3DCRT Vs IMRT p = 0.88) and (IMRT Vs RA p = 0.051).
In the left Lens, RA resulted in significantly higher mean and maximum doses, (0.102±0.075 Gy, 0.13±0.11) compared to both 3DCRT (0.019±0.008 Gy, 0.025±0.023 Gy), and IMRT (0.0213±0.013 Gy, 0.015±0.012 Gy) respectively, p < 0.05. However, there was no significant difference between 3DCRT and IMRT in mean and maximum doses, p > 0.05.
In terms of the right optic nerve, there was no significant difference between techniques in mean and maximum doses, p = 0.062 and p = 0.38 respectively. Despite this, RA resulted in higher values in mean and maximum doses (0.23±0.14 Gy, 0.54±0.24 Gy) compared to both 3DCRT (0.12±0.065 Gy, 0.44±0.22 Gy) and IMRT (0.15±0.091 Gy, 0.51±0.16 Gy. In the left optic nerve, RA resulted in a significantly higher mean dose (0.16±0.096) compared to both 3DCRT (0.035±0.014) and IMRT (0.041±0.016) (p = 0.003). The maximum with RA were also significantly higher (0.314±0.16 Gy) than 3DCRT (0.084±0.011 Gy,) and IMRT (0.10±0.079 Gy) respectively, p < 0.05.
As for optic chiasma, there were no significant differences in any of the dose metrics between the treatment techniques. Mean and maximum doses, for 3DRCT (0.21±0.074 Gy, 0.91±0.47 Gy) were lower than IMRT (0.24±0.10 Gy, 1.11±0.810 Gy) and RA (0.40±0.24 Gy, 1.12±0.91) respectively.
Regarding Brainstem, no significant differences were observed between the three techniques for mean and maximum doses, p > 0.05. However, RA had a lower maximum dose (3.91±1.42 Gy) compared to IMRT (4.83±2.33 Gy) and 3DCRT (4.20±1.93 Gy). While in the mean dose, IMRT resulted in lower values (0.43±0.12) than 3DCRT (0.44±0.16 Gy) and RA (0.45±0.11 Gy).
We conducted a study to compare the dosimetric outcomes of three techniques 3DCRT, IMRT, and RA used for stereotactic radiosurgery (SRS) and stereotactic radiotherapy (SRT) for brain metastasis, with the aim of contributing to the existing literature on the topic.
The study concluded that 3DCRT, IMRT, and RA were all considered clinically acceptable, but there were differences in the dosimetric parameters observed among these techniques. Similar findings have been reported in studies that compared the dosimetric performance of three different techniques (Cardinale et al. [12], Elhateer et al. [13], Wang et al. [15], Roa et al. [16], Ruschin et al. [17]).
Based on our study results, we found that in terms of target coverage, the three techniques were dosimetrically similar with comparable normalization values. There were no statistically significant differences observed in minimum dose (D98%) or maximum dose (D2%). In terms of mean dose higher mean doses were found in 3DCRT plans in comparison with the IMRT and RA which is statistically significant. These attributed to intensity-modulated techniques can minimize hot areas within the target volume.
The study found differences in the conformity index (CI) between the three techniques, indicating that the techniques varied in their ability to deliver conformal dose distribution to the target area. The RA technique was found to have better conformity than both IMRT and 3DCRT techniques. This is attributed to the use of a dynamic MLC system, which gives more control of radiation beam intensity. Also, optimization of the collimator angle for each arc and the use of multiple collimations help to enhance dose modulation in different axes, according to the direction of the MLC. RapidArc utilizes all available beam angles, allowing it to produce an optimal dose distribution that leads to superior treatment plans compared to IMRT [27].
In contrast, 3DCRT has higher values of CI with statistically significant differences from RA. This can be explained as 3DCRT uses a fixed number of radiation beams, which limits its ability to conform to the shape of the target area. Only some sub-fields could be added to enhance dose homogeneity. Similarly, IMRT uses multiple radiation beams with varying intensities, but may not be able to achieve the same level of conformity as RA in certain cases. However, the study also found that there were no statistically significant differences in CI values between RA and IMRT, indicating that the two techniques may be equally effective in certain cases, this agreement with Roa et al. [16] and Ruschin et al. [17]. Our result is well matched with Baumert et al. [28] who compared IMRT and 3DCRT in SRS for 10 patients. They found that IMRT demonstrated improved RTOG conformity over 3DCRT in only 6 out of the total patients. However, in 4 cases, the conformity index did not show any improvement when comparing IMRT and 3DCRT. On the other hand, when using the Paddick conformity index, they observed an improvement in conformality for IMRT over 3DCRT in all cases. Jackie et al. [29] found IMRT more effective than a 3D-conformal static technique and dynamic conformal arcs in the treatment of intracranial lesions, in terms of dosimetric benefits for SRS. It is worth noting, however, that these studies did not take into account the potential benefits of the recently tested RA technique. Ammar et al. [30] involved ten patients with brain lesions and utilized both the RTOG and Paddick conformity equations. The results indicated that IMRT demonstrated superior conformity compared to both 3DCRT and Dynamic Arc techniques for all patients in the study. Despite the higher conformity values observed with the RA and IMRT techniques in our study, the 3DCRT technique is also considered to have acceptable conformity. This is because using more fields provides greater control over the shape and intensity of the radiation beam, resulting in a better fit to the tumor’s shape and surrounding healthy tissue.
In terms of the homogeneity index, there was no statistically significant difference in the homogeneity index among the three radiation therapy techniques. Furthermore, all three techniques were found to be effective in achieving a homogeneous uniformity of dose distribution to the target volume.
The same was found in the study by Roa, et al. [16], the results indicate that there were no significant differences in dosimetric conformity and homogeneity between IMRT, and RapidArc plans. On the other hand, Ammar et al. [30] found that homogeneity was better in IMRT than in 3DCRT and Dynamic Arc techniques. Ding, et al. [31], found that target dose homogeneity was significantly improved in the IMRT plan compared to 3DCRT. However, in dose distribution, IMRT demonstrated an equivalent radiobiological effect to 3DCRT.
In regard to the dose gradient index (DGI), according to our results, both 3DCRT and IMRT techniques had lower DGI values compared to RA, suggesting that they achieved a better dose gradient than RA. The lower DGI values observed for 3DCRT and IMRT can be explained through the definition of the DGI used which is the ratio of half prescription isodose volume to the prescription isodose volume. In 3DCRT the 100% isodose volume is much higher than in IMRT and RA due to poor conformity and aiming of covering 99% of the target volume by prescription isodose through normalization. This results in lower DGI and higher CI index values. While in IMRT and RA, better CI could be achieved with higher values of DGI than 3DCRT. However, this limits high doses within the target volume other than spilling it in the area around. Moreover, the study by Reynolds, et al. [32] that dose gradient is highly influenced by tumor size and shape. Our findings indicated that there is a correlation between the gradient index values and tumor size. Figure 7, illustrated the changes in gradient index as tumor size varied. Notably, patient 5, with a tumor size of 7 cc, exhibited low gradient index values across all three techniques, indicating a more favorable dose gradient. Conversely, patient 3, who had a tumor size of 0.1 cc, demonstrated higher gradient index values. Specifically, the RA technique yielded a gradient index value of 27.33, surpassing the values obtained from the other techniques. These results imply an inverse relation between tumor size and gradient index values. Reynolds, et al. [32] also mentioned the DGI value also affected the volume of normal brain tissue doses. In our study, we found RA had lower maximum doses, V6Gy and V3Gy values for normal brain tissues compared to 3DCRT and IMRT, despite 3DCRT and IMRT techniques exhibiting a better dose gradient. This reflects better CI and low-dose spillage with RA than 3DCRT and IMRT. Furthermore, the V15 Gy, V12 Gy, and V9 Gy values were lower in RA and IMRT as compared to 3DCRT.

The impact of tumor size on the gradient index (GI) values for three techniques.
As per our study, 3DCRT and RA resulted in shorter treatment times and fewer monitor units (MUs) than IMRT. Figure 8, displayed the treatment time for each patient for the three techniques. The mean treatment time decreased by 26.2% and 10.3% for 3DCRT and RA plans, respectively, compared to IMRT. However, in the case of patients 1 and 3, it was found that RA required higher MUs and longer treatment times compared to IMRT. This is because RA in these patients had to use two isocenters, which can result in more arcs being used that require more MUs and longer treatment times.
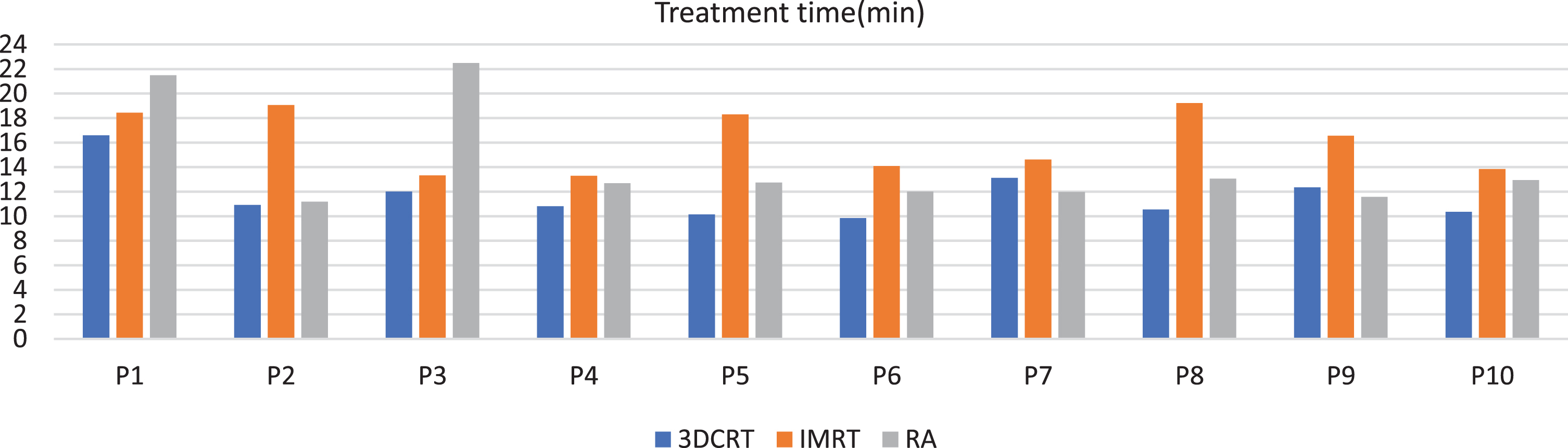
Compare the treatment times for the three radiation techniques.
The study compared the doses delivered to (OARs) for three techniques. The OARs considered in this study were optics, brain stem, and normal brain tissue. The study found that maximum and mean doses delivered to OARs were very low for all techniques. However, Table 4 in our study indicated that the maximum doses of most OARs were lower in 3DRT compared to IMRT and RA, although some differences were not statistically significant. This could be explained as exit dose and dynamic MLC in IMRT and RA maybe increase the dose to organs at risk. This is because these techniques use multiple radiation beams and beam angles, which can result in more scattered radiation reaching the organs at risk. Moreover, in RA, the radiation beam is modulated and delivered in a continuous manner, it can lead to scattering and exit dose, particularly in cases where the gantry rotates through a full arc or half arc. The scattering can increase radiation delivered to surrounding healthy tissue. In contrast, 3DCRT with static MLC and a fixed angle can avoid organs at risk by delivering radiation from a limited number of fixed angles, which can reduce the amount of scattered radiation that reaches the organs at risk. One more factor-affecting dose received by OAR is the Proximity to the target volume. In our study, OARs were considered far enough from the target volume, which can be easily spared in 3DCRT, by selecting appropriate angles where exit doses can be manually optimized. As regards to Brain stem which was considered the nearest OAR to the target volume, The maximum dose for the brain stem was found to be lower in RA compared to 3DCRT and IMRT. Baumert et al. [28] found that IMRT provided superior sparing of OARs, particularly for OAR located within or near a concave planning target volume (PTV) compared to 3DCRT. Wang et al. [15] observed slightly higher critical organ doses in RA than in IMRT, potentially due to increased leakage and transmission through the MLC. In contrast, static beam alignment techniques prioritize minimizing critical organ exposure. A systematic search by Buciuman, et al. [33] compared the dosimetric properties of VMAT and IMRT in the head and neck. The study mentioned that IMRT with fixed angles can have longer delivery times, which can increase patient exposure to low-dose radiation and require higher monitor unit (MU) values. This study also mentioned that since the number of MUs provided directly correlates with the amount of scattered radiation that reaches the healthy tissues, a lower number of MUs results in a lower dose to the distant healthy tissues. Additionally, a dynamic Multi-Leaf Collimator (MLC)-based delivery technique in IMRT typically requires more Monitor Units (MUs) compared to a Static MLC (SMLC) method [34]. It should be noted that in our study the mean MUs in IMRT and RA increased by 48.6%, and 35.3% respectively when compared to 3DCRT. However, the specific factors influencing the difference in maximum dose to OARs between these techniques may vary depending on the shape of the target and treatment plan characteristics. In some cases, the use of 3DCRT may result in a lower maximum dose of OARs compared to IMRT and RA, while in other cases the opposite may be true.
Certain limitations should be considered in our study. One limitation of our study was the small sample size, as we only had 10 patients. However, it is worth noting that several other studies have also used a similar number of participants or fewer and have been able to publish their results. Nonetheless, a larger sample size would have increased the statistical power and precision of our study. Another limitation that should be emphasized is that, in our investigation, the locations of the brain metastases were different among the cases, which may have affected the dosimetric results of the three radiation therapy techniques evaluated.
Conclusion
The study indicated that 3DCRT delivered lower doses to organs at risk compared to IMRT and RA in stereotactic radiosurgery (SRS) and stereotactic radiotherapy (SRT) for brain metastases. However, RA and IMRT techniques provided better dose conformity, and low dose spillage compared to 3DCRT. Despite no statistically significant difference in the mean normal brain dose of the three techniques, the RA technique was more efficient in controlling the maximum dose and irradiated volumes of normal brain tissue. Both 3DCRT and RA techniques have demonstrated enhancements in reducing the number of monitor units (MU) and treatment time compared to IMRT. Although smaller MUs and shorter beam times are important factors to consider when deciding on the most appropriate SRS/SRT for brain metastasis, they should not be the primary considerations. Other plan quality metrics, such as the homogeneity index (HI), gradient index (GI), and conformity index (CI), should also be carefully evaluated to ensure that the optimal SRS/SRT plan is selected.