
Abstract
Background
HIV viral load (VL) and resistance testing are limited in sub-Saharan Africa, so individuals may have prolonged time on failing first-line antiretroviral therapy (ART). Our objective was to describe the evolution of drug resistance mutations among adults failing first-line ART in Zambia.
Methods
We analysed data from a trial of VL monitoring in Lusaka, Zambia. From 2006 to 2011, 12 randomized sites provided either routine VL monitoring (intervention) or discretionary (control) after ART initiation. Samples were collected prospectively following the same schedule in each arm but analysed retrospectively in the control group. For those with virological failure (VF; >400 copies/ml), HIV genotyping was performed retrospectively on baseline (BL) and on all subsequent specimens until censored due to study completion, withdrawal or death.
Results
Of 1,973 enrollees, 165 (8.4%) developed VF. 464 genotype results were available including 132 (80%) at BL, 116 (70%) at VF and 125 (76%) had at least one result between VF and censoring. Major nucleoside reverse transcriptase inhibitor (NRTI) or non-nucleoside reverse transcriptase inhibitor (NNRTI) mutations increased from 26% (BL) to 82% (VF) to 89% at last genotype (LG). M184 mutations increased from 2% to 59% to 71%; K65R from 2% to 11% to 13%; 2 or more thymidine analogue mutations from 1% to 3% to 12%. Among those on a failing tenofovir disoproxil fumarate (TDF)-based regimen, TDF resistance increased from 42% to 58%.
Conclusions
We found substantial resistance to NRTIs and NNRTIs at VF with incremental increases after VF while still on a failing first-line ART; this resistance may compromise attainment of the UNAIDS 90-90-90 goals.
Introduction
In much of sub-Saharan Africa, access to routine HIV viral load monitoring and drug resistance testing remains limited [1]. As part of the global strategy to achieve 90% viral suppression, the World Health Organization recommends routine viral load monitoring to detect virological failure (VF) before clinical symptoms of disease progression and to reduce the accumulation of antiretroviral drug resistance mutations [2]. Drug resistance increases the need for alternative antiretroviral therapy (ART) regimens that may be less effective and more expensive, with less favourable toxicity profiles and greater pill burden. Further, it may limit the effectiveness of pre-exposure prophylaxis and first-line ART if resistant subtypes are transmitted within communities. At a population level, such resistance could threaten the success of rapidly expanding HIV programmes in sub-Saharan Africa to achieve the UNAIDS 90-90-90 goals since most first-line ART still includes non-nucleoside reverse transcriptase inhibitors (NNRTIs) [3].
With limited testing available in clinical settings, data on HIV drug resistance has been extrapolated from research studies and surveillance data [4]. In the multi-country PASER-M cohort study, for example, NNRTI resistance was high at VF (80%); the M184V mutation was present in 70%; K65R was detected in 7 adults (11%); and tenofovir resistance increased to 30% with continued VF [5,6]. In the TenoRes study, tenofovir resistance was found in nearly 60% of adults on tenofovir-based first-line ART at the time of VF [7]. In a small study from Uganda, high rates of NNRTI resistance were reported after 1 (50%, 8/16), 2 (69%, 9/13) and 3 (60%, 6/10) years following the initiation of first-line ART [8].
Although these insights into HIV drug resistance in Africa have been valuable, there are limitations to studies thus far. Most have been cross-sectional in design and thus unable to compare resistance to baseline pro-files [8,9]. Convenience sampling has limited generalizability. Information about the evolution of resistance mutations over time in sub-type C viruses among participants who remain on a failing ART regimen due to delayed recognition of VF has not been well described. We seek to address these gaps by analysing data from a large cluster-randomized trial of routine viral load monitoring in Zambia [10,11]. Our objective was to describe the evolution of drug resistance mutations from ART over time among HIV-infected adults failing first-line ART. The trial cohort created a unique opportunity to answer this study question, since samples were collected prospectively at regular intervals while participants remained on a failing first-line regimen, but they were analysed for drug resistance retrospectively.
Methods
Study design
Our current study is a secondary analysis of data collected during a cluster-randomized trial of routine viral load monitoring on all-cause mortality and HIV disease progression. The full methods of that trial have been reported elsewhere [10,11]. Briefly, we randomized 12 facilities in Lusaka, Zambia to one of two strategies for detecting treatment failure among adults initiating ART. Participants were enrolled between December 2006 and May 2008 and followed for up to 36 months. At the intervention sites, participants received routine viral load monitoring at 3 months, 6 months, and every 6 months thereafter. At the control sites, participants were evaluated for treatment failure using clinical and immunological criteria per the standard of care recommended by the Zambian Ministry of Health. When these findings were found to be conflicting, ‘discretionary’ viral load testing was used to determine treatment failure at the control sites [12]. All participants had a similar schedule for specimen collection; however, in the control arm, virological testing was not part of clinical care and was therefore conducted at the end of the study.
Patients were eligible to participate if they met criteria for ART initiation according to the Zambian national guidelines, which at that time required either CD4+ T-cell count <350 or World Health Organization clinical stage 3 or 4. Exclusion criteria included prior ART exposure except for prevention of mother to child transmission, serious illness requiring hospitalization at time of ART initiation, or comorbidities that may limit participation in study procedures. Participants were prescribed ART according to the prevailing clinical guidelines from the Zambian Ministry of Health. First-line regimens comprised two nucleoside reverse transcriptase inhibitors (NRTIs; zidovudine [ZDV], lamivudine [3TC], emtricitabine [FTC], tenofovir disoproxil fumarate [TDF], stavudine [D4T]) and an NNRTI (nevirapine [NVP] or efavirenz [EFV]) in the following combinations: ZDV+3TC+NVP, ZDV+3TC+EFV, D4T+3TC+NVP, D4T+3TC+EFV, TDF+FTC+NVP and TDF+FTC+EFV. The protocol was approved by the University of Zambia Biomedical Research Ethics Committee (Lusaka, Zambia) and institutional review boards at the University of Alabama at Birmingham (Birmingham, AL, USA) and the University of North Carolina at Chapel Hill (Chapel Hill, NC, USA). The study was registered on clinicaltrials.gov (NCT00929604).
Analysis cohort
For this secondary analysis, we included only participants who experienced VF, diagnosed by viral load testing either prospectively, over the course of the trial (intervention arm) or retrospectively, using stored specimens at the end of the trial (control arm). VF was defined as the first of two consecutive viral loads greater than 400 copies/ml plasma RNA 6 months after ART initiation with a buffer of 30 days for tests drawn just before 6 months. HIV-1 viral loads were measured with Roche Amplicor HIV-1 RNA Monitor kit (version 1.5; Roche Molecular Diagnostics, Pleasanton, CA, USA). After VF was identified, HIV genotyping for antiretroviral drug resistance was performed on the baseline (that is, enrolment) specimen and all subsequent specimens on first-line therapy until the participant changed to second-line therapy or was censored due to study completion, withdrawal or death. The VF genotype was reported from the first of the two viral loads over 400 copies/ml in all but five cases; the confirmatory viral load was used for the genotype in these five cases because two were below the genotype viral threshold, one was not stored, and two had technical failure; all were performed within 90 days of the first VF viral load (range: 25–87). The threshold of detection for the genotype assay – set at the time of study design – was a viral load of 1,000 copies/ml HIV-1 RNA, which was extracted, amplified and sequenced using Sanger sequencing on an Applied Biosystems 3130xl instrument [13]. The sequence fragments were aligned using Sequencher software version 5.0 (Gene Codes Corporation, Ann Arbor, MI, USA). Base calling was conducted automatically with a 25% threshold for mixed bases. All chromatograms were also inspected visually to ensure base calling accuracy. Fasta sequences were submitted to the Stanford HIV Drug Resistance Database in 2016 to predict drug susceptibilities (version 8.2), and the Stanford susceptibility classifications were reported directly from the program.
Statistical analysis
We performed univariate descriptive statistics on the total study population and those experiencing VF (Table 1). We analysed mutations at time of VF and cumulatively through the last available genotype on a failing first-line regimen; if a mutation was detected at one time point, it was considered present at all subsequent time points. The mutation frequencies were tabulated as a percentage of those participants who experienced VF and had a genotype. Baseline resistance as any NRTI or NNRTI mutation versus none was compared with c 2 tests at each month and year of study enrolment and categorized by year quarter to determine if baseline resistance increased over the study. Survival curves of time to VF were created using Kaplan–Meier analysis comparing any baseline NRTI or NNRTI mutation to none. All analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC, USA).
Baseline characteristics

Total missing data: prevention of mother to child transmission (PMTCT) 161, body mass index (BMI) 32, creatinine clearance (Cr Cl) 148, haemoglobin (Hgb) 69, WHO Stage 86, CD4 66, viral load (VL) 5, nucleoside reverse transcriptase inhibitor (NRTI) 1. Virological failure missing data: BMI 1, Cr Cl 15, Hgb 2, WHO Stage 9, CD4 5, NRTI 1.
Only participants with virological failure were sub-typed. d4T, stavudine; EFV, efavirenz; NNRTI, non-nucleoside reverse transcriptase inhibitor; NVP, nevirapine; TDF, tenofovir disoproxil fumarate; ZDV, zidovudine.
NRTI mutations were categorized according to the protocol developed by Tang et al. [14]. This approach included 34 surveillance drug-resistance mutations at 15 reverse transcriptase (RT) positions (M41L, K65R, K67NGE, T69D, T69ins, K70RE, L74VI, V75MTAS, F77L, Y115F, F116Y, Q151M, M184VI, L210W, T215YFISCDVE, K219QERN), as well as K65N, T69del and K70QGT. The thymidine analogue mutations (TAMs) were M41L, D67NG, K70R, L210W, T215YF and K219QE. The NNRTI mutations were analysed based on the 18 surveillance drug-resistance mutations at 11 RT positions (L100I, K101E, K103NS, V106AM, V179F, Y181CI, Y188LCH, G190ASEQV, P225H, M230L, P236L). Additional mutations were included that have a similar predicted phenotypic effect (L100V, K101PH, V179LD, Y181V, G190V, M230I) or have important implications for future therapy (E138AGKQ). The Pan-NNRTI category for Table 2 includes any key mutations for second-generation NNRTI resistance: L100I, K101EP, Y181, Y188L, G190, M230L.
Cumulative reverse transcriptase mutations on failing first-line antiretroviral therapy

Data are n (%). NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; TAMs, thymidine analogue mutations.
Role of the funding source
The funders had no role in the design, analysis or writing of this article; however, representatives from the US Centers of Disease Control and Prevention reviewed a final draft of the manuscript prior to submission.
Results
Of 1,973 participants enrolled in the parent trial, 165 (8.4%) developed VF over 4,446 person-years of study follow-up. Participants who developed VF had a median age of 32.1 years and 60% were women. Subtype C was the predominant HIV-1 virus (93%), and 57% had a baseline plasma HIV viral load greater than 100,000 copies/ml. In the VF group, 63% had WHO stage III or IV disease at enrolment; the median CD4+ T-cell count was 126 cells/mm3 (IQR: 57–182). 84% started an NVP-based regimen, while the remaining 16% started an EFV-based regimen. The NRTI backbones included ZDV (51%), d4T (32%) and TDF (16%). In Table 1, we compared baseline characteristics of our analysis cohort (that is, those with VF) to all trial participants. When stratified by NRTI backbone, 10% on ZDV had VF, compared with 8% on d4T and 6% on TDF (P=0.15). When stratified by NNRTI, 9% of those on NVP had VF compared with 5% with EFV (P=0.02).
Among the 165 participants with VF, 464 HIV genotype results were available, including 132 (80%) at baseline and 116 (70%) at time of VF. 125 (76%) participants had at least one genotype between VF and time of censoring, which was defined as a switch to second-line therapy, death, withdrawal from the study or completion of study follow-up. The median time from ART initiation (that is, baseline) to the VF genotype was 356 days (IQR: 175–553). The median time from VF genotype to last available HIV genotype, prior to the switch to a second-line regimen, was 202 days (IQR: 139–461). Thus, our analysis cohort represents a cumulative 191 person-years on a failing first-line ART regimen. Reasons for missing genotype results included: viral load below the threshold for HIV genotyping, unavailable sample from the visit or laboratory technical failure (Figure 1).

Flowchart of the 165 participants with virological failure and their 464 genotype tests
Of the 132 participants with HIV genotype results at ART initiation, 36 (27%) had a major NRTI or NNRTI resistance mutation (Table 2). This included 30 (23%) with at least one NNRTI mutation, including K103N (n=13, 10%) and pan-NNRTI resistance (n=12, 9%). In addition, 13 (10%) had an NRTI mutation at baseline, including M184 (n=3, 2%) and K65R (n=2, 2%). Presence of NNRTI resistance at ART initiation did not affect the time to VF (Figure 2). Baseline resistance did not change over the course of study enrolments (P=0.6). Women who reported using prevention of mother to child transmission (PMTCT) services in the past had twice the baseline rate of NNRTI resistance (42%) compared with men (20%) and women not reporting prior PMTCT exposure (16%).
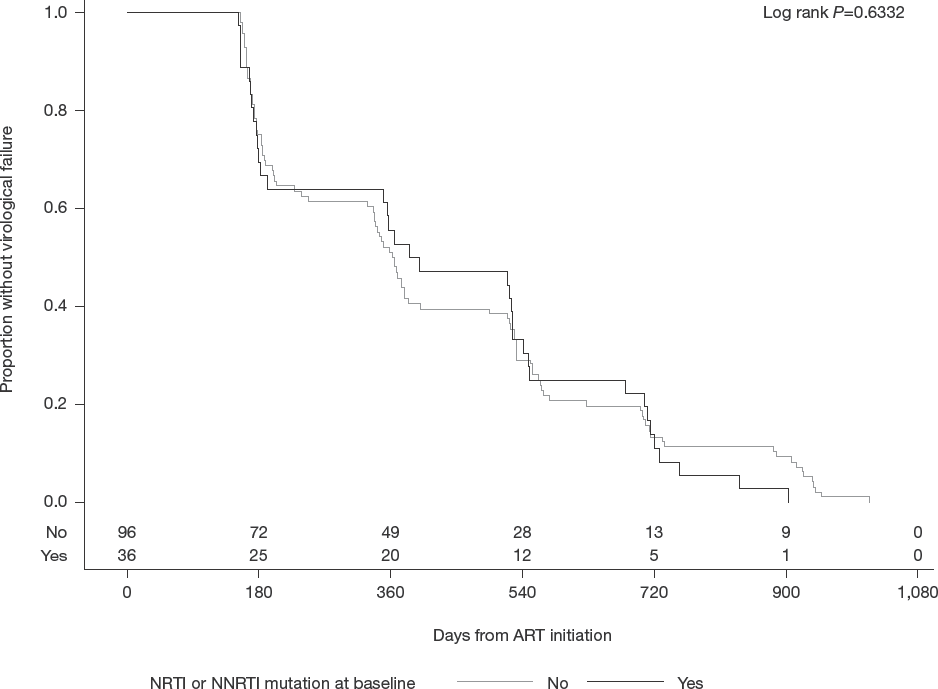
Time to virological failure following antiretroviral therapy initiation, stratified by any major NRTI or NNRTI mutations on baseline genotype
We examined results from both the HIV genotype results at VF (n=116/165, 70%) and the last available genotype (LG; n=151/165, 92%). At VF, 81% (94/116) had a major NRTI or NNRTI mutation, which increased to 89% (134/151; Table 2). M184 mutations increased from 2% at baseline (BL) to 59% at VF to 71% at LG; 12% of participants had 2 or more TAMs. 15% of those with VF on TDF or ZDV developed TAMs, compared with 6% of participants on d4T (P=0.14). K65R mutations increased from 2% (BL) to 11% (VF) to 13% (LG); K65R mutations arose in 46% (12/26) on TDF, 10% (5/48) on d4T, and 4% (3/76) on ZDV. At VF, 81% had at least one major NNRTI mutation and 52% had a pan-NNRTI mutation. Pan-NNRTI mutations were highly prevalent in participants taking NVP (83/89; 93%). The viral load monitoring arm had less accumulation of TAMs compared with the control arm in the last genotype (7% versus 16%; Additional file 1). Prolonged failure over 9 months on a first-line regimen increased mutation frequency for M184V, TAMs and pan-NNRTI mutations (Additional file 2); however, the majority of mutations had already accumulated by the time virological failure was detected.
Predicted drug susceptibilities were greatly reduced at VF and further with the last available genotype (Figure 3). FTC/3TC susceptibility decreased from 98% at baseline to 39% at VF to 26% at LG. ZDV susceptibility decreased from 98% (BL) to 91% (VF) to 77% (LG). TDF decreased from 98% (BL) to 87% (VF) to 77% (LG); among those on a failing TDF-based regimen, TDF resistance increased from 42% (8/19, VF) to 58% (15/26, LG). 70% developed resistance to second-generation NNRTIs. Rilpivirine susceptibility or potential low-level resistance decreased from 84% (BL) to 38% (VF) to 30% (LG). High level resistance increased from 3% (BL) to 29% (VF) to 43% (LG). Etravirine susceptibility or potential low-level resistance decreased from 91% (BL) to 53% (VF) to 42% (LG); likewise, the high-level resistance increased from 0% (BL) to 4% (VF) to 10% (LG). Except for the accumulation of TAMs leading to increased ZDV resistance, there was no difference in stratified analysis of resistance by the control versus intervention arm of the parent cluster randomized trial (Additional file 3).

Predicted drug resistance at baseline, virological failure and last available genotype
Discussion
In this study of adult patients initiating NNRTI-based ART in Zambia, over 90% of participants did not experience VF in their first 36 months of HIV treatment. Our observed rate of VF (8.4%) over 3 years is in line with the 90-90-90 goals set forth by the Joint United Nations Programme for HIV/AIDS (UNAIDS) [15]. Nearly 20% of those who experienced VF had no detectable resistance mutations, suggesting non-adherence with minimal drug exposure. Of the remaining 80% with antiretroviral drug resistance, the majority of the resistance mutations could be detected by the time of VF, which increased further with prolonged time on a failing first-line ART regimen.
The rates of VF observed in our pragmatic study were encouraging and similar to other reports from the region. A recent surveillance study from Rwanda found 12% of ART initiators experienced VF at 12 months [16]. In ANRS 12249 trial, based in South Africa, high rates of 12-month viral suppression (97%) were achieved using a combination of TDF+FTC+EFV as first-line therapy [17]. That our study had a slightly higher estimate for VF was not surprising, given the ‘real world’ clinical settings we sought to replicate and longer follow-up. Early during study enrolment, in accordance with Zambian treatment guidelines at the time, we relied heavily on older ART regimens that incorporated NVP and non-TDF NRTIs, agents that may be less durable than currently recommended first-line regimens, especially at higher viral loads [18].
Using Sanger sequencing, we observed a high prevalence of pretreatment drug resistance among individuals with eventual VF, particularly for NNRTIs (23%). We did not perform baseline genotypes on participants who did not experience VF; as a result, we were unable to directly compare pretreatment drug resistance on VF. However, this prevalence is higher than what has been observed in other regional studies including the most recent regional estimates (8–15%) in the 2017 World Health Organization Drug Resistance report [4]. Several factors may have contributed to the high levels of pre-treatment NNRTI drug resistance in our sample. First, as we only have pre-treatment data on those with virological failure, we may have selected the group with higher levels of pre-treatment drug resistance. Interestingly, the rate of VF was not significantly different between those with NRTI or NNRTI baseline resistance and those without. The ANRS 12249 trial in South Africa had similar findings: no association between pre-treatment drug resistance and virological suppression was detected over 16 months [17]. Other explanations include an older national programme, which has been associated with higher levels of transmitted resistance [19]; we did not see an association between time of enrolment and baseline resistance. The prevalent use of peripartum NVP for PMTCT – part of the standard of care for many years in Zambia – also likely contributed to the higher levels of pre-treatment NNRTI resistance [20].
By the time VF was detected, many of the key damaging mutations had already accumulated. This finding suggests that WHO-recommended 6-month interval for viral load monitoring may not be optimal. There is often further delay for the turnaround time for results to reach the referring facility – between 3 and 31 days in one recent study of seven sub-Saharan African countries [21]. These data do not account for further delays for the result to be acted upon clinically. Further implementation research should focus on the optimal use of viral load monitoring.
Our results also highlight the need for interventions that prevent VF and thus resistance. Similar to our findings, a recently published report from Lesotho found that 85% of adults failed first-line therapy with detectable resistance mutations [22]. Of those adults with a detectable viral load after 6 months of ART, 64% remained unsuppressed after an expanded adherence counselling intervention. HIV treatment facilities and the research community should focus on tools for early detection of poor adherence and implementation of effective, scalable interventions to improve adherence with a renewed focus on preserving first-line therapy. The Bill and Melinda Gates Foundation recently published a summary of the most promising, scalable interventions including peer counselling, adherence clubs, and short message service (SMS) possibly paired to electronic dose monitors [23]. The hope of expanded access to viral load testing, including point of care viral load testing, to improve early detection of non-suppressed patients will require effective adherence interventions to help those patients achieve viral suppression after early detection. The need to adapt such adherence packages to local settings must be weighed against other competing priorities within the UNAIDS 90-90-90 goals.
Our study offered a unique opportunity to observe the accumulation of HIV resistance mutations among patients on failing first-line therapy. Over considerable intervals between VF and the last available genotype (median 202 days; IQR 139–461), we observed modest increases in antiretroviral resistance. Predicted TDF resistance increased from 42% to 58% in those failing TDF-based regimens, similar to the TenoRes study and a recently published meta-analysis of tenofovir-based first-line failures in sub-Saharan Africa [7,24]. TAMs increased more than NNRTI resistance mutations with prolonged failing on first-line regimen. For those on d4T-based regimens, predicted tenofovir resistance did not change. In a small cohort of 26 patients with subtype C virus followed 6–12 months after VF on d4T or ZDV regimens, K65R mutations doubled from 12% to 23% [25]; predicted TDF resistance doubled from roughly 20% to 40%, which is higher than another recently reported small study from Mozambique [26]. A slightly larger study of 63 adults including 28 with sub-type C and 18 on tenofovir-based ART showed that resistance to tenofovir and ZDV increased from 10% to 30% with continued VF, however, resistance on tenofovir-based ART or the emergence of TAMs while on tenofovir was not reported [6].
The resistance patterns observed in our last available genotypes could threaten Zambia's recently reported success of 90% viral suppression among those on ART [4]. The NNRTI resistance of 87% to EFV is particularly concerning for the potential for transmitted drug resistance to first-line therapy; as such, increasing rates of pretreatment drug resistance has led international agencies to consider integrase-based first-line therapy in certain countries [4]. Further, it may compromise the effectiveness of future injectable NNRTIs. Importantly, acquired NRTI mutations also affect second-line ART options [27]. 15% of those taking TDF-based regimens developed two or more TAMs by VF. This finding was unexpected since tenofovir has not traditionally been associated with TAM emergence [24]; however, it was similarly observed in secondary analysis of the TenoRes collaboration. In that study it was attributed to substitutions from prior ART, however, in our study ART-naive participants initiated first-line ART; this finding should be further evaluated in future studies of sub-type C. There is ongoing debate over the roles of resistance and adherence in second-line failure since no second-line ART randomized trials have achieved 90% viral suppression [27–30]. Interestingly, two clinical trials of second-line regimens enrolled participants of whom over 95% had baseline NNRTI resistance [29,30], compared with the 80% NNRTI resistance at VF observed in our cohort, which suggests that 20% were non-adherent enough not to get resistance versus less than 5% in second-line trials. This discrepancy suggests that enrolment into these second-line trials may select for more adherent participants and may not be representative of the general population failing first-line ART regimens. The benefits of treatment as prevention are less likely to accrue if second-line therapy does not achieve full viral suppression [27,28].
Strengths of this study include its large sample size, its prospective design, and lengthy longitudinal follow-up. Despite the older treatment regimens, including ones incorporating d4T and NVP, our results are still relevant to understanding the evolution of resistance mutations and potential circulating resistance patterns in Zambia. Our findings are also relevant to second- and third-line regimens in settings where the majority of viruses are subtype C. We acknowledge limitations as well. For example, HIV resistance tests were performed retrospectively, as dictated by the protocol, which contributed to missing genotype results, thus we chose to analyse new mutations at key time points rather than individual accumulation rates. No genotypes were run on those that did not have VF limiting our analysis of pretreatment drug resistance. Samples could not be repeated if volumes were found to be inadequate or if specimens were lost. As with all genotype assays, we were limited by the lower limit of detection for viral concentration; we are unable to comment on those individuals who were not virologically suppressed but had less than 1,000 viral copies per ml. We relied on consensus sequencing, which can only detect resistance mutations comprising >25% of the circulating viral population [31]. Because of this effect, our results are likely a conservative estimate of the true resistance that may be present. Newer techniques can double the detection of resistance in minor variants [17]. Recent data also suggests that genotype might not predict phenotype as well for second-generation NNRTIs in subtype C HIV-1 infection [32].
In summary, in this study of virological failure on first-line ART in Zambia, we found significant resistance to NRTIs and NNRTIs at the time of virological failure, which increased with prolonged failing on first-line regimens. These data highlight the urgent need for effective adherence strategies, earlier detection of VF including distinguishing poor adherence from resistance, and access to newer drug classes. Each of these challenges must be addressed if the ambitious 90-90-90 goals set forth by international agencies and local governments are to be met.
Footnotes
Acknowledgements
We thank Suwilanji Silwamba (CIDRZ, Lusaka, Zambia) for technical assistance with HIV sequencing. This study was supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through a multicountry grant to the Elizabeth Glaser Pediatric AIDS Foundation from the U.S. Centers for Disease Control and Prevention (cooperative agreement U62/CCU12354) and an administrative supplement to the U.S. National Institutes of Health (U01 AI069452). Additional support for investigators, trainees, and research administration was provided through the National Institutes of Health (T32 AI007001, K24 AI120796, P30 AI050410, P30 AI027767). The funders had no role in the design, analysis or writing of this article. This study was presented as poster 537 at Conference on Retroviruses and Opportunistic Infections, 4–7 March 2018 in Boston, MA, USA.
The authors declare no competing interests.
Additional file 1: A table showing cumulative reverse transcriptase mutations on failing first line antiretroviral therapy, by monitoring arm of parent, cluster randomized trial can be found at ![]()