
Abstract
Background
Methods
Results
Conclusions
Introduction
Pre-exposure prophylaxis (PrEP) refers to the use of antiretroviral (ART) medications by at-risk, HIV-uninfected persons to prevent HIV. The only currently approved formulation of PrEP is oral tenofovir disoproxil fumarate/emtricitabine (TDF/FTC), whose efficacy has been demonstrated in several populations [1–3]. Although TDF is generally safe [4], it can cause adverse renal and bone effects, including decreases in bone mineral density (BMD) [5,6]. Several mechanisms for this BMD decline have been proposed, including alteration of gene expression in osteoclasts, altered renal phosphate handling [7] and functional vitamin D deficiency [8–10].
There is a need for greater attention to the impact of PrEP on bone health for several reasons. First, existing results are discordant with regard to the effects of TDF-based PrEP on BMD at different anatomic sites [3,11,12]. For instance, lumbar spine BMD declined in the San Francisco study and both hip and femoral neck BMD declined in iPrEx [11,12]. Second, PrEP patients tend to be young, with 70% and 90% of participants in the iPrEx and TDF-2 studies, respectively, being under 30 years old [1,3]. Since peak bone mass is thought to be achieved at 30 years of age, any detrimental effect on bone health in this population may be especially clinically important. Further, as PrEP becomes more commonplace worldwide and is taken for longer periods of time, it is increasingly important to understand just how large the impact of TDF on BMD is. This is particularly true because PrEP users are defined by their absence of disease, thus warranting heightened vigilance in monitoring for iatrogenic toxicity. Since TDF is also routinely used in the treatment of established HIV and HBV infections, it is also of interest to understand whether the impact of TDF differs in these contexts.
To better characterize the effects of TDF on bone health, we thus conducted a systematic review and meta-analysis with the primary objective of quantifying the effects of daily oral TDF-containing PrEP on the change in BMD in adults and adolescents over 1 year, compared with placebo or no PrEP. Our secondary objectives were to quantify the impact of TDF-containing PrEP on additional bone outcomes including the development of osteoporosis, low bone mass and fractures, and to quantify the impact of TDF on the same bone health outcomes over 1 year when used for treating HIV and HBV.
Methods
We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Prospero identification #CRD42017070552).
Eligibility Criteria
We defined eligible studies as randomized controlled trials comparing TDF-based regimens to placebo, no intervention, or another non-TDF-containing regimen, in participants taking the drug for PrEP, HIV treatment or HBV treatment. We included studies with treatment-naive adolescent (12–17 years old) and adult (≥18 years old) participants. The study had to measure at least one of our bone outcomes of interest (relative and absolute change in BMD, osteoporosis, low bone mass or fractures) at a minimum of 48 ±4 weeks. We included any study published 1997 or later and imposed no restrictions on publication status or language.
Search Strategy
We designed a comprehensive search strategy with the help of an information specialist. The search strategy included search terms for studies assessing our desired intervention (TDF) and design (randomized controlled trials). To maximize sensitivity, we did not include our patient populations (PrEP, HIV or HBV) or outcomes (bone health) as search terms. The full search strategy is included in Additional file 1.
Information Sources
We retrieved publications from MEDLINE and EMBASE electronic databases on 27 June 2018. We conducted hand searching of conference proceedings from the Conference on Retroviruses and Opportunistic Infections (CROI), the International AIDS Society (IAS) meetings, IDWeek, the Infectious Diseases Society of America (IDSA) Annual Meeting, the American Association for the Study of Liver Diseases (AASLD), and the European Association for the Study of the Liver (EASL) from 2014 to July 2018.
Selection of Studies
We compiled and imported search results into Covidence [13], an online software program for facilitating systematic reviews. Two reviewers (BB, SW) independently screened and filtered articles through assessment of titles and abstracts. We then acquired the full text of all articles deemed potentially relevant to further assess eligibility, with resolution of disagreements through consensus.
Data Extraction
Two reviewers (BB, SW) independently extracted information from all articles that fulfilled the inclusion criteria using a standardized data extraction form. Data collected pertained to study characteristics (design, country, target population, funding), intervention (formulation, frequency, dosage) and baseline characteristics of study participants (sex, race, age, body mass index, BMD, risk factors for osteoporosis). The primary measure of effect size sought from each study was the mean difference in percentage change in BMD at 1 year (48 ±4 weeks) between the TDF and non-TDF groups. We also extracted data on absolute change in BMD, as well as rates of developing osteoporosis, low bone mass and fractures. Both unadjusted and adjusted values in the primary data were collected and we noted which, if any, variables were considered in multivariable models. If relevant data were missing or unclear, we made up to three attempts to contact study authors by email for clarification.
Risk of Bias
Included studies were assessed for risk of bias using a checklist we developed based on the CONSORT 2010 Checklist of Information for Randomized Trials [14]. Specifically, we appraised the reported randomization process, concealment of treatment allocation, blinding, attrition, treatment analysis, management of missing data and funding sources. No studies were excluded due to risk of bias. Instead, we performed sensitivity analyses in which studies of unclear and high risk of bias were excluded. We also created funnel plots to assess for publication bias when at least five studies reporting on a specific outcome were available.
Analysis
To quantify decreases in BMD, we pooled the mean difference in percentage change in BMD at 48 ±4 weeks between the TDF and control groups from included studies using DerSimonian random-effects models, with weighting of studies according to the inverse variance method. This was done separately for PrEP, HIV treatment and HBV treatment studies. For the outcomes of osteoporosis, low bone mass and fractures, we planned to calculate rate ratios for each included study by dividing the number of events by the number of person-years of follow-up, and pool results separately for PrEP, HIV and HBV studies using Der-Simonian random-effects models. We used Cochran's Q test to measure heterogeneity between studies at the 0.10 level of significance. We deemed the degree of heterogeneity significant if the I 2 statistic was more than 50%. In post hoc analyses, we examined the pooled mean differences in BMD change at 96 weeks for studies that provided information at that time point. We used RevMan (version 5.3) to produce Forest plots illustrating the pooled results.
Results
Search Results
The database search yielded 5,178 titles. De-duplication by Covidence removed 1,313 articles. We screened 3,865 titles and abstracts, of which 3,666 were excluded. 199 papers were retrieved for full review, of which 167 were excluded due to ineligible outcomes (n=107), interventions (n=19) and populations (n=20). Of the 32 remaining studies, we removed 5 for re-publication of results and 2 because the data of interest could not be obtained from authors. Ultimately, we included 25 distinct papers for final data extraction (Figure 1). Of these, 10 investigated PrEP users [1,3,11,12,15–20] and were included in our primary analyses, while 15 investigated HIV [21–35]. We did not find any HBV studies or new relevant conference proceedings that had not already been published as one of our reviewed studies.

PRISMA protocol for systematic review
Study Characteristics
Among the PrEP articles, nine examined daily PrEP, representing six different trials, while one was an on-demand PrEP study. Study size ranged from 40 to 2,499 participants. The trials were conducted throughout the world (Table 1). Characteristics of the HIV studies are also included in Table 1. TDF was paired with a variety of concomitant antiviral medications in the treatment arms of these studies, and there was similar variability in treatment regimens for the non-TDF comparator groups.
Baseline participant characteristics of included studies

Values are the mean (
Median (IQR). c89.5 were male, 10.5 were transgender women. ABC, abacavir; ATV/r, ritonavir-boosted atazanavir; COBI, cobicistat; DRV/r, ritonavir-boosted darunavir; d4T, stavudine; E/C/F/TAF, elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide; E/C/F/TDF, elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate; EFV, efavirenz; FTC, emtricitabine; LPV/r, ritonavir-boosted lopinavir; MVC, maraviroc; N/A, not applicable; PrEP, pre-exposure prophylaxis; RAL, raltegravir; RCT, randomized controlled trial; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate; 3TC, lamivudine.
Risk of Bias
Results from our risk of bias assessment are shown in Additional file 2. 44% (11/25) of the studies reported proper randomization and 64% of studies (16/25) reported proper concealment of treatment allocation. 73% of studies (18/25) received funding from industry. The degree of attrition varied widely between trials, while approaches to randomization, blinding and analysis of missing data were generally appropriate. Funnel plots for three specific outcomes (BMD loss at the lumbar spine and total hip in HIV patients, as well as fractures in PrEP patients) did not identify definitive evidence of publication bias (Additional files 3 and 4).
Outcomes
BMD
Figure 2 shows the percentage change in BMD at 1 year related to PrEP use. All four PrEP studies [11,12,17,18] reporting on this outcome showed a greater decrease in BMD with TDF compared with controls over 1 year, with a mean difference of -0.82% at the lumbar spine (95% CI=-1.28, -0.37, I 2 =38%) and -0.81 (95% CI=-1.22, -0.40, I 2 =48%) at the total hip. The statistical heterogeneity for these outcomes was moderate.

Change in bone mineral density in PrEP patients at 48 weeks
Nine studies [23,24,26–28,31–34] measured BMD changes over 1 year in people using TDF for HIV. As for the PrEP studies, all showed a larger decrease from baseline in TDF compared with non-TDF treated participants. However, the mean difference was considerably larger than for PrEP-related TDF use, at -1.62% (95% CI=-2.30, -0.95, I 2 =93%) at the lumbar spine, -1.75% (95% CI=-2.08, -1.42, I 2 =83%) at the total hip and -1.30% (95% CI=-1.74, -0.85, I 2 =43%) at the femoral neck (Figure 3). The statistical heterogeneity was high. Our post hoc analysis found that the mean difference at 96 weeks was modestly less than at 48 weeks for the total hip but not for the lumbar spine (Figure 3). A single HIV study [23] performed adjusted analyses, in which models were adjusted for age, sex, ethnic origin, smoking, BMI, HIV RNA and baseline BMD. These results were quantitatively similar to univariate analysis in the primary study, except that the difference in BMD at the lumbar spine was no longer statistically significant.
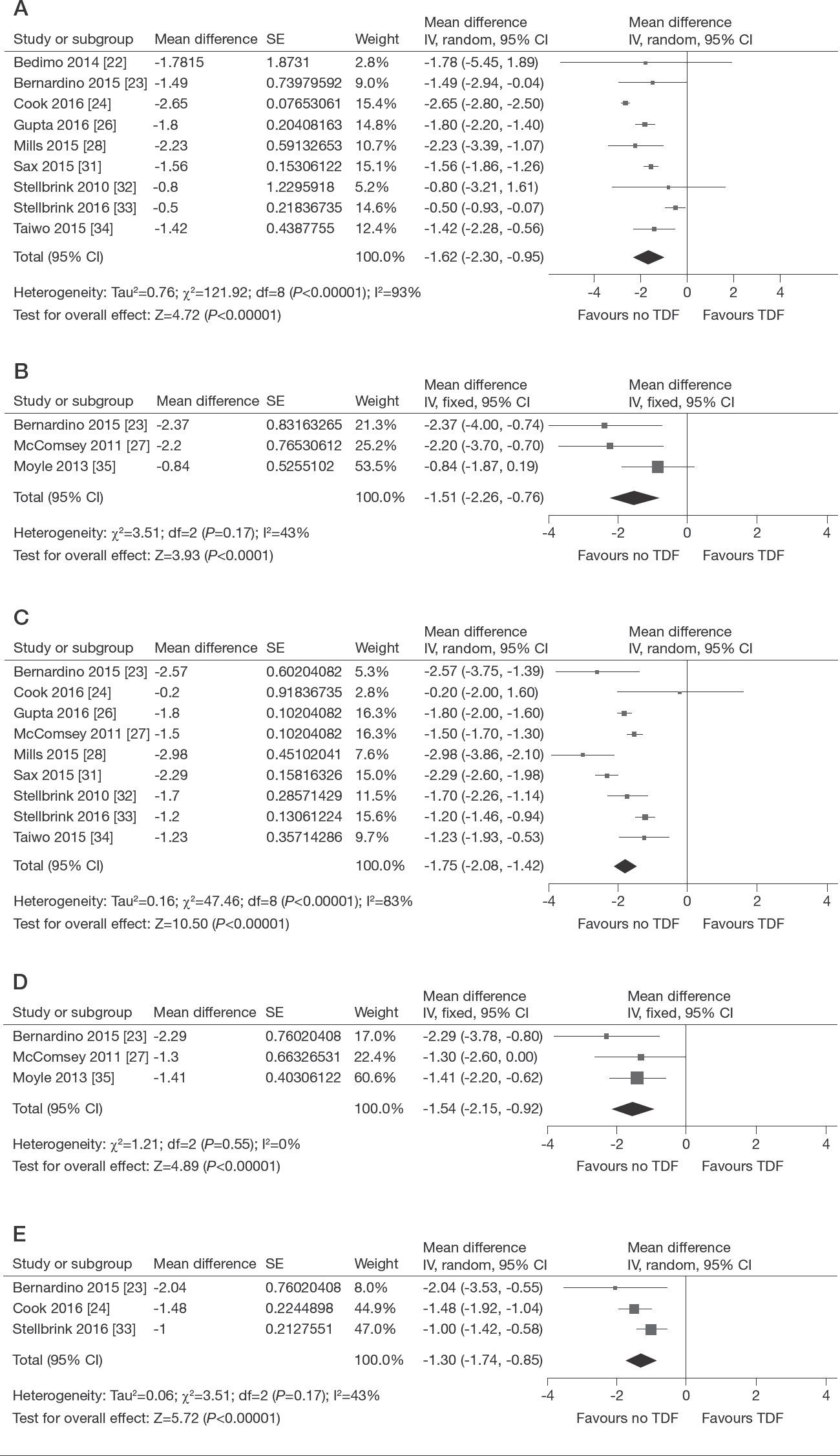
Change in bone mineral density in HIV patients
Fractures
Sixteen studies reported data on fractures, including eight PrEP [1,3,12,15,16,18–20] and six HIV [21,23,25,29–31] articles. However, the total number of person-years of follow-up was only available for five PrEP studies, each of which followed participants for roughly 1–4 years [1,15,16,19,20]. The pooled results for these five studies showed no increase in fractures (RR=1.12, 95% CI=0.72, 1.74, I 2 =26%; Figure 4). Of the nine studies whose fracture results we could not pool due to unclear person-years of follow-up and/or time points, six reported more fractures in TDF groups compared with controls [3,12,23,29–31], two reported more fractures in the non-TDF group [21,25], and one reported no fractures [18]. It is noteworthy that 4/6 studies [23,29–31] reporting higher fracture rates in TDF groups were HIV papers.

Fractures in PrEP patients
Osteoporosis and Low Bone Mass
Four PrEP studies [11,12,17,18] observed greater proportions of TDF participants experiencing ≥3% decline in BMD in comparison to non-TDF groups. Two PrEP studies did not observe significant differences in low bone mass between the two groups [12,18]. One HIV study observed no differences in the incidence of osteoporosis in the TDF group compared with control at 48 weeks [23]. A second HIV study reported little change in the prevalence of osteoporosis in the TDF group compared with control at 96 weeks [35].
Sensitivity Analysis
Removing studies with unclear risks of bias did not qualitatively change our results regarding mean differences in BMD (Additional file 5), but did decrease statistical heterogeneity among HIV studies (decreased to I 2 =50% for lumbar spine and I 2 =66% for total hip). The effect size for the impact of TDF on BMD was somewhat greater at the lumbar spine and total hip, while it was negligibly less at the femoral neck in HIV patients.
Discussion
In this systematic review and meta-analysis, we found that TDF-based regimens decreased BMD more than placebo or non-TDF-containing regimens at 48 weeks, whether used as PrEP or HIV treatment. TDF did not, however increase the number of fractures when used as PrEP. We did not find enough data on osteoporosis or low bone mass to comment on effects of TDF on the incidence of these conditions, likely because of the relatively short duration of follow-up in each study. We were also unable to find any HBV articles that fit our inclusion criteria. The magnitude of the BMD decreases that we found is clinically significant, as they approach the 1.9–2.1% decreases observed over 2 years in healthy women undergoing menopause [36], and the 3% decreases seen in patients on 1 year of glucocorticoids [37], both of which are among the most dramatic risk factors for osteoporosis known.
The findings of our review are consistent with previously published findings. For instance, a meta-analysis of adverse events in randomized TDF/FTC-based PrEP studies found no difference between treatment and placebo [38]. Moreover, current and previous TDF use has been found to be an independent risk factor for decreased BMD in studies of HIV-positive patients [39].
Our study highlights the need for physicians to anticipate and properly manage the adverse bone effects of TDF, regardless of the context in which it is used. Current recommendations for HIV patients to improve bone health include smoking cessation, weight-bearing exercises and optimizing vitamin D and calcium intake [6,40]. Vitamin D and calcium supplements have been shown to increase BMD by 1.73% at the total hip and 0.78% at the lumbar spine in HIV patients on ART [41]. For patients at higher risk of fractures, bisphosphonates have been found to increase BMD at the lumbar spine and total hip [42]. Among HIV-positive patients, bisphosphonates can increase lumbar spine BMD by 2.84% and total hip by 2.12% after 48 weeks of use, which is slightly greater in magnitude than the BMD loss associated with TDF identified in our review. Mouse models suggest that drugs that increase adenosine concentrations such as dipyridamole may hold promise for reversing tenofovir-related bone loss [43].
Importantly, however, guidelines for TDF-based PrEP use contain few recommendations on bone health [44]. This absence may in part be because the magnitude of BMD loss is thought to be smaller than in HIV, as borne out by our systematic review, and because PrEP is generally viewed as a time-limited intervention whose impacts on BMD may be reversible on discontinuation. Indeed, in a cohort of men who have sex with men discontinuing PrEP, participants experienced a mean BMD increase of 1.81% at the lumbar spine and 1.13% at the total hip by 1 year of stopping PrEP [45]. The observed increases in BMD are comparable to the decreases found in our study.
However, the young age of many PrEP users and expanding rollout of PrEP underscores the importance of addressing this issue more systematically. In addition, most current data likely underestimate the effects of TDF on BMD, because adherence to study drug among participants in the clinical trials was poor. For instance, in a pharmacokinetic subanalysis of the iPrEx trial, tenofovir diphosphate was detectable in only 51% of tested samples from participants randomized to active drug [3]. Indeed, a striking finding from our meta-analysis is that the magnitude of TDF-related BMD loss in PrEP trials was considerably smaller than in HIV trials.
An alternative explanation for this difference is that the larger degree of BMD loss in the setting of HIV infection may be related to immune reconstitution inflammatory syndrome (IRIS). A possible mechanism is that antiretroviral treatment-related T-cell reconstitution leads to RANKL and tumour necrosis factor (TNF)-α production by T- and B-cells, and subsequently bone resorption [46]. The time-limited nature of IRIS may explain why BMD loss typically stabilizes after 96 weeks of TDF use in people living with HIV [47–50], a finding corroborated by the modest attenuation in BMD loss seen at 96 weeks compared with 48 weeks among HIV studies in this review. Because patients taking TDF for PrEP do not experience IRIS, this explanation could partly explain why the magnitude of TDF-related BMD loss in PrEP studies was less than that in HIV studies.
Importantly, one strategy that has been advanced to address TDF-related bone loss is to replace TDF with tenofovir alafenamide (TAF), a prodrug known to cause less renal and bone toxicity because it concentrates more efficiently in leukocytes [31]. A 5,400-person trial is currently examining the efficacy of TAF/FTC compared with TDF/FTC as PrEP in gay, bisexual and other men who have sex with men, as well as transgender women, and preliminary results suggest that it is non-inferior at preventing HIV acquisition [51]. However, a potential disadvantage of TAF-based PrEP is that as a newer formulation, its cost will be considerably higher than that of generic TDF/FTC and will be protected by patents for several years to come. Lower cost interventions to mitigate TDF-related bone toxicity are needed, potentially including calcium and vitamin D supplementation [10,41]. We have previously found very high acceptability of such an intervention among PrEP users in Toronto and Vancouver [52], and the findings from this systematic review could assist in the sample size calculations for clinical trials in this area in the future.
Of note, although our search did not yield any HBV studies that fit our inclusion criteria, an open label study of switching HBV patients from TDF to TAF found that BMD increased at 12 and 24 weeks [53]. This effect results from the decreased plasma concentrations of tenofovir diphosphate achieved with the TAF formulation, which decrease deleterious impacts on bone. Similarly, a randomized controlled trial comparing TDF with TAF in both treatment-naive and experienced HBV patients found less decrease in BMD among TAF patients compared with those on TDF [54,55].
Strengths of our study are our inclusion of only randomized trials to enable direct within-study attribution of differences in bone health to TDF, our broad search strategy that included conference abstracts and hand-searching of outcomes to maximize sensitivity, and our stratification of studies according to PrEP, HIV and HBV indication. Our study also has limitations that warrant discussion. For example, our ability to assess for publication bias through funnel plots was limited both because the total number of studies available was modest, and because some identified articles were missing important information. We were also limited in the number of meta-analyses we could perform, most notably for fractures, because many studies did not specify the total person-years of follow-up, precluding calculation of event rates. However, the available results suggest that publication bias is unlikely, and we attempted to contact authors at least three times regarding missing results. Further, statistical heterogeneity in the HIV studies that we pooled was high, although this decreased after excluding trials at high or unclear risk of bias. This could be because we did not perform a meta-analysis of individual patient data and were thus unable to disaggregate results by age, sex, menopausal status and other important cofactors. Finally, the length of follow-up time varied in the PrEP studies, and all likely needed to be much longer in order to appropriately quantify TDF-related fracture risk.
To conclude, our review found that TDF use decreased BMD considerably more than did comparators, when used as PrEP and HIV treatment. The clinically significant declines in BMD within a relatively short follow-up time suggest the need for population-level BMD monitoring and interventions. Future studies should investigate how bone-building interventions can be safely and effectively implemented to mitigate TDF-induced bone loss across patient populations.
Footnotes
Acknowledgements
The research was funded by the Keenan Research Summer Student program. DHST is supported by a New Investigator Award from the Canadian Institutes of Health Research/Ontario HIV Treatment Network. All authors have seen and approved the final submitted version of the manuscript. All authors contributed significantly to the work, as follows: DHST conceived the study idea; DHST designed the protocol together with AMC and SM; BB and SW conducted database searches, selected eligible articles for inclusion, conducted the statistical analysis, and wrote the original draft of the manuscript; all authors provided input into and approved the final version of the manuscript. The authors would like to acknowledge David Light-foot (St. Michael's Hospital, Toronto, ON, Canada) for assisting with the literature search and Roger Bedimo (Infectious Disease Section, VA North Texas Health Care System, Dallas, TX, USA), Paul Cook (Brody School of Medicine at East Carolina University, Greenville, NC, USA), Moupali Das (HIV and Emerging Viruses, Gilead Sciences, San Francisco, CA, USA) and Lut Van Damme (Global Health Program - HIV, Bill & Melinda Gates Foundation, Seattle, WA, USA) for their help in data acquisition.
BB, SW and SM have nothing to disclose. AMC is supported by a Tier 1 Canada Research Chair in Musculoskeletal and Postmenopausal Health. In the past 3 years, DHST's institution has received research support for investigator-initiated research studies from Gilead and ViiV Healthcare. DHST is a Site Principal Investigator for clinical trials sponsored by GlaxoSmithKline.