
Abstract
Background
Methods
Results
Conclusions
Introduction
The HIV epidemic among people who inject drugs (PWID) in Switzerland had its peak in the late 1980s [1,2], contributing to one of the highest AIDS death rates in Europe in 1988 [3]. Already in the late 1970s pharmacological and psychotherapeutic components of drug addiction treatment programmes were initiated in Switzerland by a network of specialized institutions and authorized private physicians [4,5].
In addition, during the early 1990s, harm reduction programmes also included the distribution of clean needles to reduce HIV transmission among PWID. It was estimated that almost 16,000 new infections were prevented by these measures [1]. In 1996, highly active antiretroviral therapy (HAART) became available and over the years turned HIV infection into a manageable chronic disease. Life expectancy of people living with HIV increased rapidly over the last two decades and is approaching life expectancy of the HIV-negative population in resource-rich countries [6–8]. Although life expectancy of PWID remains reduced, HIV-positive PWID are approaching life expectancy of HIV-negative PWID retained in care [8–10].
Long-term survivors (LTS) are a group of persons diagnosed with HIV before HAART was available and who survived a long period, some more than 15 years after HIV diagnosis. Having survived this traumatic episode in the history of the HIV epidemic, with many of their peers with an HIV diagnosis dying soon thereafter and experiencing stigma for a long period, can lead to mental health problems, including depression. Beside this, PWID LTS live with the additional burden of drug addiction. Drug dependency has multifactorial causes: genetic, socioeconomic, mental disorders and peer influence. For most PWID, abstinence is not a realistic goal. This makes understanding long-term social and mental health outcomes of HIV-positive PWID a pertinent task.
Few cohorts have data on people living with HIV over three decades and fewer have included information about social and mental well-being, making it particularly difficult to study the population of LTS. The population of PWID among LTS is even more difficult to study, due to the early peak of the HIV epidemic among PWID and the large number of PWID lost to follow-up [10].
The goal of this study is to detect and quantify differences concerning certain indicators of social and mental well-being between PWID and persons who most likely acquired HIV through sexual contacts, that is, men who have sex with men (MSM) and heterosexuals (HET), among LTS. To refine the heterogenous control group of all MSM and HET, we selected those HET who are phylogenetically linked with PWID, and hence presumably shared a social network with PWID at the time they were infected [11–14]. We first describe the population of all HIV-positive PWID in the Swiss HIV Cohort Study (SHCS) and distinguish in a further analysis those PWID who stopped using intravenous drugs, those who were enrolled in opioid substitution programmes (OSP) and all other PWID. We focus on social aspects 15 years post HIV diagnosis, including the ability to work, incarceration and mental well-being.
Methods
Swiss HIV Cohort Study
The SHCS is a prospective multicentre cohort study enrolling individuals aged 18 or older living with HIV in Switzerland [15]. Baseline demographic information is collected at study entry. In biannual follow-up visits, clinical, laboratory and social well-being information is collected. In addition, we used information of the genotypic-resistance-test (GRT) database of the SHCS, which was shown to have a good coverage of difficult to reach and marginalized populations [16].
Study Populations
LTS were defined as SHCS participants diagnosed prior to 1996 who survived and were retained in the SHCS at least 15 years after diagnosis. PWID were defined as participants who most likely acquired HIV through needle sharing when using intravenous drugs as well as participants who reported injection drug use between 1980 and the diagnosis date. The group of PWID LTS was further divided into three groups based on participants’ self-reporting on participation in OSP and injection of drugs outside of OSP: PWID who did not report any injection drug use or participation in OSP 15 years post HIV diagnosis, termed Former PWID, PWID who are using drugs exclusively in OSP 15 years post HIV diagnosis, termed PWID in OSP and PWID reporting injection drug use outside of OSP or PWID with missing information about drug use or participation in OSP 15 years post HIV diagnoses, termed Other PWID. The group of MSM/HET participants consists of all SHCS participants who most likely acquired HIV through sexual contacts. This control group of MSM/HET participants was divided into: HET participants who are phylogenetically clustered with PWID (clusteredHET) and MSM, and HET not in the group of clusteredHET, termed MSM/HET not clustered (MSM/HETnc). We did not include SHCS participants most likely infected through sources other than intravenous drug use or sexual contacts, for example, blood products or mother-to-child infection, in any analysis.
To determine HET phylogenetically clustered with PWID, a maximum-likelihood phylogenetic tree using the GRT database of the SHCS was constructed (Additional file 1). For every HET participant, we take the smallest possible cluster in the tree containing at least one PWID participant. We determine the maximal pairwise cophenetic distance of these clusters, where the cophenetic distance between two tips is the sum of the branch lengths connecting the two tips [17]. If the maximal pairwise cophenetic distance in this cluster is smaller than 0.045, the participant is defined as clusteredHET, otherwise not (Figure 1). See Figure 2 for the selection of the study populations.

Illustration of the definition of HET phylogenetically clustered with PWID, denoted by clusteredHET

Flow chart to illustrate the different populations of interest
Definitions
The diagnosis year was defined using the earliest information available: either a documented positive HIV test or the registration year of the SHCS. A history of hepatitis C (HCV) was defined as a positive antibody response or a positive HCV RNA test. A history of hepatitis B (HBV) was defined as a positive anti-HBc antibody response. Suboptimal adherence to ART was defined as reporting missing more than one dose per week. Cognitive complaints were defined as answering ‘yes, definitely’ to one of the three questions: ‘Is the patient aware of frequent memory loss in normal daily life?’, ‘Does the patient experience difficulties in paying attention in normal daily life?’ or ‘Is the patient aware of slowing down in reasoning or solving problems?’ [18,19]. Depression and intake of antidepressants was based on patients’ self-reporting. Work ability was based on the physicians’ judgement, percentage of income obtained through work was based on self-reported information [20]. Physical activity was assessed in two ways: via a question on whether the participant was actively doing household chores and whether the participant reported undertaking sport activity at least once a week, with a sport activity defined as at least 10 to 20 min of rapid walking or fitness [21]. As a proxy of high-risk sexual behaviour [22–25], we analysed condomless sexual intercourse, defined as self-reported inconsistent condom use with casual partners.
Statistical Analysis
First, we compared all PWID LTS and clusteredHET LTS with the control group of MSM/HETnc LTS, respectively. Second, we compared the three groups of PWID, that is, PWID in OSP, Former PWID and Other PWID, with the control group of MSM/HETnc, respectively. All analyses were performed using data collected at least 15 years post HIV diagnosis: follow-up per year refers to the average number of follow-up visits and CD4+ T-cell nadir to the smallest CD4+ T-cell value 15 years post HIV diagnosis. Opportunistic infection, suboptimal adherence to ART, cognitive complaints, depression, intake of anti-depressants, hospitalization for psychiatric reasons, incarceration and condomless intercourse refer to at least one such event 15 years post HIV diagnosis. Full ability to work, all income through work, active in household and active in free time refers to the median of all follow-up visits 15 years post HIV diagnosis. We performed unadjusted as well as adjusted logistic regression models with correction for the HIV diagnosis year, stratified into four periods: 1980–1986 (that is, before availability of any ART), 1987–1989 (the peak years of the HIV epidemic among PWID in Switzerland), 1990–1992 (before the large roll-out of supervised injectable heroin programmes) and 1993– 1995 (Additional file 2). In a sensitivity analysis, we stratified by male and female participants to understand the impact of gender (Additional file 3).
Results
Study Populations
Of all 20,370 SHCS participants, 5,686 participants were classified as PWID. Of those, 1,663 (29.2%) were LTS, with 581 (34.9%) belonging to the group of Former PWID LTS, 423 (25.4%) to the group of PWID LTS in OSP and 659 (39.6%) to the group of Other PWID LTS. Of the 14,684 SHCS participants not in the group of PWID, 621 (4.2%) were in the group of clusteredHET and 13,196 (89.6%) in the group of MSM/HETnc (7,689 MSM and 5,507 HETnc participants). Moreover, 205 (33.0%) of clusteredHET and 2,018 (15.3%) of MSM/HETnc (1,328 MSM and 690 HETnc participants) were LTS (Figure 2).
Basic Characteristics of People who Inject Drugs and LTS in the SHCS
In 2018, 1,309 (23.0%) PWID were still alive and actively participated in the SHCS. All others were either lost to follow-up (1,634, 28.7%) or had died (2,743, 48.2%), with the main causes of death being HIV/AIDS-related (1,284, 46.8%), overdose of narcotics (137, 5.0%) and suicide (88, 3.2%). Of the 1,663 (29.2%) PWID classified as LTS, the majority was male (1,026, 61.7%) and most were of White ethnicity (1,580, 95.0%). The median year of birth of PWID LTS was 1962 and the median diagnosis year was 1987. The median follow-up time of PWID LTS was 19.9 years. In 2018, 810 (48.7%) PWID LTS were still alive and retained in the SHCS, 471 (28.3%) died and 382 (23%) were lost to follow-up. The main cause of death among PWID LTS was HIV/AIDS-related (54, 11.5%), followed by overdose of narcotics (26, 5.5%) and suicide (15, 3.2%). See Table 1 for the basic characteristics of PWID, PWID LTS and PWID not in the group of PWID LTS.
Basic characteristics of PWID in the SHCS

Basic characteristics of people who inject drugs (PWID) in the Swiss HIV Cohort Study (SHCS). LTS, long-term survivors.
Description and Comparison of Characteristics of PWID LTS, clusteredHET LTS and MSM/HETnc LTS
Basic Demographic and Clinical Characteristics
The majority of patients were male in the group of PWID LTS (1,026, 61.7%) and MSM/HETnc LTS (1,600, 79.3%), and female in the group of clustere-dHET LTS (145, 70.7%; Table 2). The overall CD4+ T-cell nadir varied between the groups (PWID LTS: 113.5, clusteredHET LTS: 150.0, MSM/HETnc LTS: 147.5) as well as the occurrence of opportunistic infections (PWID LTS: 75.9%, clusteredHET LTS: 69.8%, MSM/HETnc LTS: 63.9%). Hepatitis C was diagnosed in 93.0% PWID LTS (1,479/1,591), 18.2% clustere-dHET LTS (37/203) and 10.0% MSM/HETnc LTS (201/2,002).
Characteristics of PWID LTS, clusteredHET LTS and MSM/HETnc LTS in the SHCS

Description of the three groups of long-term survivors (LTS): people who inject drugs (PWID), men who have sex with men (MSM)/heterosexuals (HET) not phylogenetically clustered with PWID (HETnc) and HET clustered phylogenetically with PWID (clusteredHET). ART, antiretroviral therapy; SHCS, Swiss HIV Cohort Study.
Characteristics 15 Years Post HIV Diagnosis
ClusteredHET LTS and PWID LTS had significantly less follow-up visits as compared with MSM/HETnc LTS (adjusted OR for not reaching the anticipated two follow-up visits per year: 2.6 [1.8,4.0]; P<0.001, for clusteredHET LTS and 1.5 [1.3,1.7]; P<0.001, for PWID LTS). A comparison of CD4+ T-cell measurements showed that the first CD4+ T-cell count as well as the CD4+ T-cell nadir 15 years post HIV diagnosis was significantly lower for PWID LTS as compared with MSM/HETnc LTS (adjusted OR for first CD4+ T-cell count <200 cells/ml: 1.7 [1.3,2.1]; P<0.001, and CD4+ T-cell nadir <200 cells/ml: 1.3 [1.1,1.5]; P<0.001). Significantly more PWID LTS suffered from an opportunistic infection, namely 411 (24.7%) compared with 282 (14.0%) for MSM/HETnc LTS (adjusted OR=1.4 [1.1,1.6]; P=0.001). There was a significant difference concerning self-reported depression among PWID LTS and MSM/HETnc LTS (59.4% versus 43.3%, adjusted OR=1.8 [1.6,2.1]; P<0.001) as well as hospitalization for psychiatric reasons (10.2% versus 5.4%, adjusted OR=2.3 [1.8,3.0]; P<0.001). Moreover, 7.0% of MSM/HETnc LTS and 30.6% of PWID LTS (adjusted OR=6.9 [5.6,8.6]; P<0.001) were incarcerated at least once. Compared with 59.0% of MSM/HETnc LTS, 25.4% of PWID LTS (adjusted OR=0.27 [0.23,0.31]; P<0.001) and 48.3% of clusteredHET LTS (adjusted OR=0.63 [0.47,0.84]; P<0.001) had full work ability. Similar results were obtained for the income through work. In addition, PWID LTS reported less activity in the household and less activity in free time, more cognitive complaints and worse adherence to ART as compared with MSM/HETnc LTS. Condomless intercourse was more often reported in the case of MSM/HETnc LTS as compared with PWID LTS or clusteredHET LTS. In most of the tested variables, the differences between PWID LTS and MSM/HETnc LTS were more pronounced (higher odds ratio) compared with the differences between clusteredHET LTS and MSM/HETnc LTS (Table 2 and Figure 3).
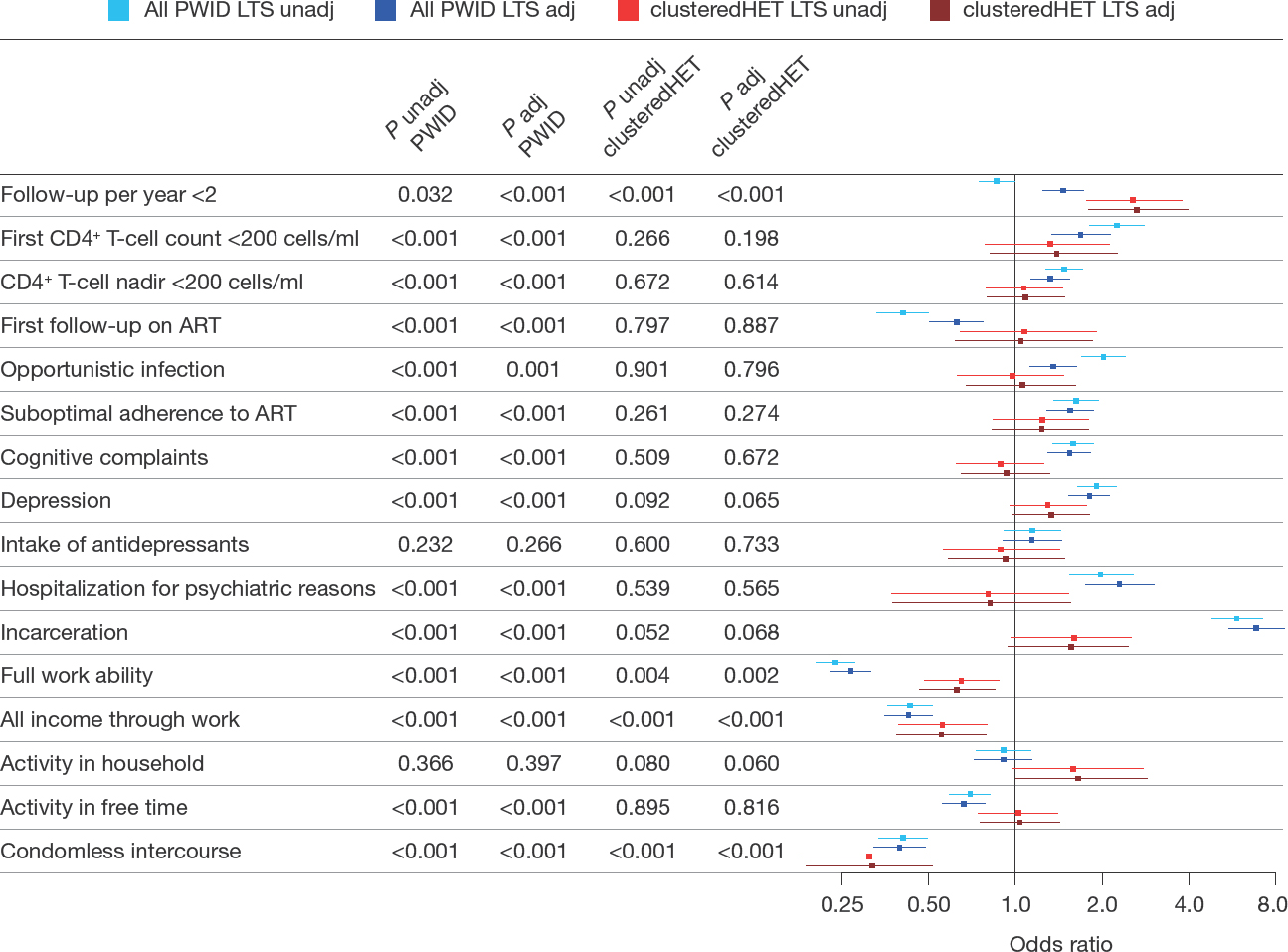
Comparison between PWID with MSM/HETnc (reference) as well as clusteredHET
Description and Comparison of Characteristics of Former PWID LTS, PWID LTS in OSP and other PWID LTS with clusteredHET LTS and MSM/HETnc LTS
Basic Demographic and Clinical Characteristics
The percentage of male participants was 56.1% in Former PWID LTS, 59.8% in PWID LTS in OSP and 67.8% in Other PWID LTS. The median number of follow-up years was 21.8 for Former PWID LTS, 21.4 years for PWID LTS in OSP and 16.4 years for Other PWID LTS. The overall CD4+ T-cell nadir was 132 for Former PWID LTS, 100 for PWID LTS in OSP and 109 for Other PWID LTS (see Table 3 for more baseline characteristics).
Comparison of Former PWID LTS, PWID LTS in OSP and Other PWID LTS

Description of the three groups of people who inject drugs (PWID) long-term survivors (LTS): Former PWID, PWID in OSP and Other PWID. ART, antiretroviral therapy; OSP, opioid substitution programme.
Characteristics 15 Years Post HIV Diagnosis
The median number of follow-up visits per year was 1.3 (0.7, 2.0) in Other PWID LTS, 2.0 (1.4, 2.6) in Former PWID LTS and 1.8 (1.2, 2.5) in PWID LTS in OSP. The occurrence of opportunistic infections varied between the groups (Former PWID LTS: 21.9%, PWID LTS in OSP: 30.5%, Other PWID LTS: 23.5%) as well as the percentage reporting suboptimal adherence to ART (Former PWID LTS: 17.3%, PWID LTS in OSP: 29.2%, Other PWID LTS: 28.5%; Table 3). Moreover, the percentage of patients with mental health problems varied between the groups, including self-reported depression (Former PWID LTS: 51.7%, PWID LTS in OSP: 64.3%, Other PWID LTS: 68.9%) and cognitive complaints (Former PWID LTS: 41.1%, PWID LTS in OSP: 51.0%, Other PWID LTS: 54.8%).
In addition, 15.1% of Former PWID LTS, 32.2% of PWID LTS in OSP and 43.2% of Other PWID LT S were incarcerated at least once. These differences were refected in the respective comparison of these three groups with MSM/HETnc LTS controls (Figure 4). There was a significant difference in sub-optimal adherence to ART when comparing PWID LTS in OSP (adjusted OR=2.0 [1.6,2.6]; P<0.001) and Other PWID LTS (OR=2.0 [1.5,2.6]; P<0.001) to MSM/HETnc LTS, but not for comparing Former PWID LTS and clusteredHET LTS with MSM/HETnc LTS. Similarly, while a significant difference between PWID LTS in OSP and Other PWID LTS and MSM/ HETnc LTS was observed with respect to, for example, self-reported depression, full work ability or activity in free time, no or a weaker difference was observed when comparing Former PWID LTS or clusteredHET LTS with MSM/HETnc LTS (Figure 4).

Comparison of the three groups of PWID LTS (Former PWID LTS, PWID LTS in OSP and Other PWID LTS) with MSM/HETnc (reference) as well as clusteredHET LTS
Discussion
Our results show that, although HIV transmission among PWID has virtually stopped in Switzerland, special care for HIV-positive PWID is still needed. We found significant differences in many psychosocial aspects of PWID LTS compared with long-term survivors among MSM/HETnc, more than 15 years post HIV diagnosis. Of note, the group of PWID LTS is very diverse, with around one-third of PWID LTS not reporting any injection drug use 15 years post diagnosis and around one quarter reporting injection drug use solely in OSP. On the one hand, this indicates that the majority of PWID LTS benefited from programmes offered to PWID. On the other hand, more than one-third of PWID LTS reported injecting drug use outside of OSP more than 15 years post HIV diagnosis. This calls for action in this most vulnerable subgroup of Other PWID, also refected by our finding that Other PWID had significantly more problems regarding social and mental well-being as compared with Former PWID or PWID in OSP. In total, around one-quarter of PWID LTS had full work ability 15 years post diagnosis, which shows the success of re-integration programmes targeted to PWID. The proportion of Former PWID regaining full work ability was 3x higher as compared with PWID in OSP and Other PWID, highlighting differences between these subgroups of PWID LTS. In comparison, more than half of all MSM/HETnc LTS regained full work ability 15 years post HIV diagnosis. Aspects regarding the ability to work as collected in the SHCS were studied in detail by Elzi et al. [20], who showed that regaining full ability to work depends on achieving viral suppression, absence of mental health issues, and other psychosocial factors. Also, we found that suboptimal adherence and depression, as well as hospitalization for psychiatric reasons was more common in PWID compared with MSM/HETnc LTS and was less pronounced in PWID classified as Former PWID, that is, PWID reporting no injection drug use any more. Moreover, potential barriers of reintegration to work in PWID LTS certainly include legal problems, as around one-third of PWID LTS have been incarcerated at least once 15 years post HIV diagnosis. In addition, cognitive problems, as were reported by almost half of all PWID LTS, could be another barrier to a successful integration into working life and related social well-being factors.
We compared the group of PWID LTS and those HET LTS who are phylogenetically linked with PWID in HIV molecular analyses, that is, people who did not report drug use and who most likely acquired HIV through sexual contacts with an HIV-positive PWID, denoted as clusteredHET. This novel method of choosing an epidemiological control group by analysing phylogenetic clusters is superior to selecting a control group by purely demographic characteristics such as the diagnosis year or age. Proximity in the phylogenetic tree can be interpreted as proximity in the underlying HIV transmission network and hence, the underlying social network at the time of transmission [11–14]. Analysing clusteredHET LTS might shed light on problems resulting from sharing a particular social network and hence disentangling the effect of using intravenous drugs. The comparison of social factors among PWID LTS, clustered-HET LTS and MSM/HETnc LTS revealed significant differences in the ability to work, incarceration and cognitive complaints. The differences between PWID LTS and MSM/HETnc LTS were more pronounced as compared with the differences between MSM/HETnc LTS and clusteredHET LTS.
Our results suggest that achieving social well-being, including the ability to work and the absence of incarceration, is more difficult for PWID compared with people from similar social networks who do not inject drugs. This is of particular note, as we only consider social factors more than 15 years post HIV diagnosis. Reintegration into normal working and social life hence seems to be more difficult for people who had or still have problems with intravenous drugs compared with their peers who did not inject drugs, which was also refected by our distinction of different groups of PWID: Former PWID were in many aspects comparable with the control group of clusteredHET in contrast to PWID in OSP and Other PWID who had more problems regarding social and mental well-being. This calls for an increased social support for the population of PWID who are already infected with HIV, in particular, in the case where they still use injection drugs. More effort into reintegration of PWID LTS into normal social and working life is needed, even for those PWID who were infected a long time ago and do – from a clinical perspective – well.
This study has several strengths and limitations. Of particular value is the wide variety of information regarding social aspects, including the ability to work, incarceration and mental well-being, included in the routine follow-up questionnaire of every SHCS participant. In addition to clinical and demographic information, the SHCS biobank allowed retrospective sequencing leading to a well-sampled GRT database. Using the GRT database, we could select a control group close to PWID in the transmission network but potentially without a history of intravenous drug use. One drawback is, however, that certainly not all clusteredHET selected with our approach shared a social network with PWID at the time of infection and, moreover, the type and duration of interaction between PWID and the clusteredHET is unknown. Some of the clusteredHET might have been misclassified and are actually PWID, although a systematic misclassification is unlikely due, for example, to the much lower prevalence of HCV among clusteredHET compared with PWID. One further drawback is that we called all participants who were diagnosed before 1996 and who remained retained within the SHCS for at least 15 years ‘long-term survivors'. With this definition, we group participants diagnosed in 1985 with those diagnosed in 1995, although life expectancy was much higher for those diagnosed only 1 year before the introduction of HAART. We decided to use this definition as all participants who were diagnosed before 1996 faced the situation of being diagnosed with an incurable, deadly disease at that time. We corrected for the HIV diagnosis year (using four periods: 1980–1986, 1987–1989, 1990–1992, 1993–1995) to account for this potential confounding factor in the adjusted models. One inevitable drawback of this study is the high proportion of PWID with loss-to-follow-up in the SHCS. Although the SHCS made a huge effort to complete data about death cases by going through death notices, in many cases it is unknown what happened to PWID lost to follow-up. One further limitation is that there was no formal assessment of the quality of life in the SHCS and many variables, including depression and cognitive problems, rely on self-reporting of the participants. This makes it difficult to compare our study with other studies, where a validated quality of life score was used, for example, by Miners et al. [26]. In addition, there are no questions about stigma, discrimination [27] or life satisfaction in the SHCS questionnaire. Inclusion of these variables would make it possible to compare the quality of life of people living with HIV with the uninfected population.
In conclusion, even 15 years post HIV diagnosis, there are significant differences regarding social and mental well-being between PWID and other SHCS sub-populations. While more than half of all MSM/HETnc LTS had full work ability, this applied to one-quarter of PWID LTS, with considerable differences between Former PWID, PWID in OSP and Other PWID. Moreover, PWID LTS were 4x more often incarcerated as compared with MSM/HETnc LTS in the period 15 years post HIV diagnosis until the most recent follow-up visit. In addition, we found more severe mental health issues among PWID as compared with other SHCS participants. For most tested variables, differences between PWID LTS and MSM/HETnc LTS were more pronounced compared with the differences between PWID LTS and clusteredHET LTS, indicating that HET who most likely shared a social network with PWID at the time of HIV infection are more vulnerable as compared with other non-PWID SHCS participants. Moreover, PWID who still inject drugs outside of OSP 15 years post HIV diagnosis have more issues regarding mental health, were more often incarcerated and had lower work ability as compared with PWID who did not inject drugs any more.
Footnotes
Acknowledgements
Conceived and designed the study: KK, RDK, HFG. Performed the analysis: KK. Verified the definitions and analytical methods: AM, PB, RDK, HN, SEC, NB. Collected and contributed data: HFG, JAR, EB, AC, MC, AB, JB, SY, TK, MP, LNW, RW. Wrote the paper: KK. All authors read and approved the final manuscript. This work was supported by the Swiss National Science Foundation (Grant # BSSGI0_155851). HFG was supported by SNF grant 179571. Furthermore, this study has been financed within the framework of the Swiss HIV Cohort Study, supported by the Swiss National Science Foundation (grant #177499), by the SHCS research foundation by the Yvonne Jacob Foundation (to HFG), by the clinical research priority programme of the University of Zurich “Viral infectious diseases, ZPHI” (to HFG). HFG has received an unrestricted research Grant from Gilead to the SHCS Research Foundation. The SHCS was approved by the ethics committees of the participating institutions (Kantonale Ethikkommission Bern, Ethikkommission des Kantons St. Gallen, Comité Départemental d'Éthique des Spécialités Médicales et de Médicine Communataire et de Premier Recours, Kantonale Ethikkommission Zürich, Repubblica et Cantone Ticino–Comitato Ethico Cantonale, Commission Cantonale d'Éthique de la Recherche sur l'Être Humain, Ethikkommission beider Basel for the SHCS and Kantonale Ethikkommission Zürich for the ZPHI), and written informed consent was obtained from all participants.
Further acknowledgements can be found in Additional file 4.
HFG has received unrestricted research grants from Gilead Sciences and Roche; fees for data and safety monitoring board membership from Merck; consulting/ advisory board membership fees from Gilead Sciences, ViiV, Merck, Sandoz and Mepha. EB has received fees for his institution for participation in advisory boards from MSD, Gilead Sciences, ViiV Healthcare, AbbVie and Janssen. MC has received research and travel grants for his institution from ViiV and Gilead. AC has received unrestricted educational and research grants from MSD, Gilead and ViiV. The remaining authors declare no competing interests.