
Abstract
Introduction
In December 2019, a cluster of pneumonia cases of unknown cause appeared in Wuhan City, Hubei Province, China. A new coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; originally named 2019 novel coronavirus, 2019-nCoV) was identified, and the species to which the virus SARS-CoV-2 belongs is Severe acute respiratory syndrome-related coronavirus (SARS-CoV) [1]. The disease caused by SARS-CoV-2 is now officially named COVID-19 by the World Health Organization (WHO). There have been millions of confirmed cases of COVID-19 in the world [2,3]. SARS-CoV-2 belongs to the family of Coronaviridae, which affects three classes of vertebrates: mammals, birds and fish. Based on the genome differences, four coronavirus clusters can be classified, three of which have been recognized and classified as genera (alpha-, beta- and gammacoronavirus) [4]. SARS-CoV-2 is a beta coronavirus and is the member of the coronaviruses family that can infect humans. This coronavirus can lead to a series of complications such as acute respiratory distress syndrome, RNAaemia and acute cardiac injury [5]. Epidemiological studies demonstrated this new coronavirus can spread via human-to-human transmission, and infected travellers were also reported outside the mainland of China [6].
One of the great challenges in SARS-CoV-2-infected patients is that an effective antiviral therapy has not been found. One of the conventional therapy regimes used in the hospitals of Wuhan involved antibiotics, oseltamivir and methylprednisolone (when severe community-acquired pneumonia was diagnosed) [5]. Considering the case-fatality rate and poor prognosis for virus-infected patients with critical symptoms, and the possibility of viral mutations, it is urgently required to seek therapeutic options for COVID-19. Unfortunately, there is no specific and effective therapy at present.
As SARS-CoV-2 is a member of the coronavirus family that include pathogens causing common cold, severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), the lopinavir/ritonavir-based combination therapy used in SARS and MERS coronavirus infections may be effective in the current SARS-CoV-2-infected patients [7–11].
It was reported the regime of lopinavir/ritonavir combined with ribavirin demonstrated a good survival benefit compared with ribavirin alone (28.8% versus 2.4%) [7] in the treatment of SARS. Lopinavir/ritonavir is a compound formulation of lopinavir and ritonavir, as a protease inhibitor, which can suppress HIV replication during the later stages of the HIV growth cycle (after translation and before assembly) [8]. Lopinavir/ritonavir was reported to have a good inhibition effect on MERS coronavirus in vitro [9] and this compound formulation was recommended to be used in the treatment of SARS and MERS [10,11]. Arbidol is a broad-spectrum antiviral that has demonstrated activity against numerous viruses, including influenza A, B and C, and hepatitis B and C. It prevents the virus from entering and/or fusing with intracellular/endosomal membranes [12]. Interferon alphas are commonly used to treat viral infections including SARS. They are modulators of immune response and inhibit viral replications in host cells inducing viral resistance in cells. As such, arbidol may inhibit the first stages of SARS-CoV-2 growth cycle (adsorption and penetration), lopinavir/ ritonavir interferes at later stages and interferon alphas induce viral resistance in cells. The combination of these drugs may exert synergistic action on the suppression of SARS-CoV-2. However, there are few clinical data on the efficacy of lopinavir/ritonavir-based combination therapy in patients with SARS-CoV-2 infection. Here we report a case of SARS-CoV-2-infected patient, which was settled and virological clearance was achieved by using a combination therapy with lopinavir/ritonavir, arbidol and interferon-α1b.
Case report
A 41-year-old Chinese male visited the fever clinic of General Hospital of Central Theater of the PLA (Wuhan, China) due to fever, cough with white phlegm, loss of appetite, general weakness and shortness of breath. This patient had no history of visiting the Huanan Seafood Market. Epidemiological investigation revealed that 5 days prior to attendance at the fever clinic, the patient had attended an internal medicine-cardiovascular clinic where he had been in close contact with another patient who was later tested positive for SARS-CoV-2.
Apart from a history of hypertension, the patient was a healthy non-smoker. After admission, normal physical examination was conducted. His blood pressure was 130/74 mmHg, heart rate was 90 beats/min, respiratory rate was 18 breaths/min and body temperature of 38.3°C. The patient said the onset time of fever was 3 days ago. Lung auscultation revealed coarse breath sounds and slight wet rales in both lungs.
Initial laboratory investigations revealed the followings: white blood cell count 3.1x10 9 /l, haemoglobin 124 g/l, mean red cell volume 86.4 fl, granulocytes 69% and platelets 96x10 9 /l, C-reactive protein 21.9 mg/l, erythrocyte sedimentation rate (ESR) 22 mm/h. The serum levels of alanine aminotransferase (AA) and glutamic oxaloacetic transaminase (GOT) were 30 U/l and 32 U/l, respectively (Table 1). The patient's chest radiography conducted by computed tomography (CT) revealed that there was some ground-glass opacity observed in both lungs (Figure 1A), indicating the evidence of pneumonia. The CT findings were consistent with the initial pulse oxymetric saturation of 97% in ambient air. Special samples were obtained for further laboratory tests. Oropharyngeal specimen and sputum specimens were collected and sent for SARS-CoV-2 detection by a real-time reverse transcriptase polymerase chain reaction (rRT-PCR). Considering the clinical presentation and to avoid the hospital acquired pneumonia, empirical antibiotic therapy with ceftriax-one and azithromycin were initiated on the first day of admission.

Chest CT images
Clinical laboratory results of the patient in hospital
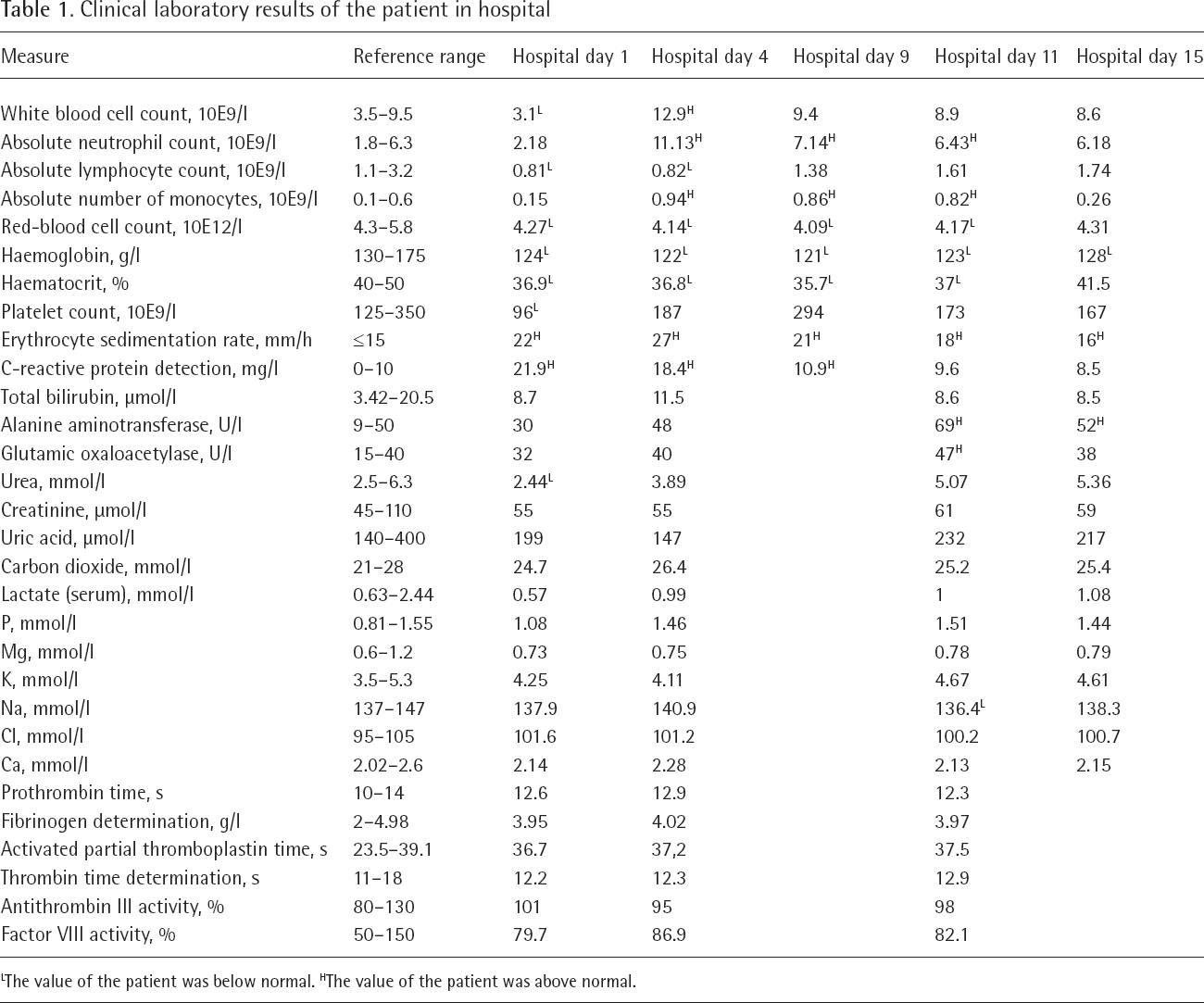
The value of the patient was below normal.
The value of the patient was above normal.
rRT-PCR for the envelope protein (EP) gene, nucleocapsid protein (NP) gene and open reading frame (ORF1ab) gene of the upper respiratory tract sample were performed to confirm SARS-CoV-2 infection at the People's Hospital of Hubei Province (Wuhan, China). The rRT-PCR method was performed as follows: a volume of 120 μl of each sample was used to extract RNA by QIAamp Viral Mini Kit (Cat. No. 52904; Qiagen, West Sussex, UK) according to manufacturer's instructions, and 30 μl elution was obtained for further assay. RNA extractions (9.5 μl) were treated by SARS-CoV-2 Fluorescent PCR Kit (Maccura, Chengdu, China) according to the manufacturer's instructions. This kit was designed for targeting the EP, NP and ORF1ab genes. The PCR conditions of pre-amplification experiment were: 50°C for 30 min, followed by 95°C for 3 min, and 10 cycles at 95°C for 15 s and 60°C for 30 s. After that, 5 μl of PCR solution was mixed with the agents of the kit and RT-PCR was performed using the following programmes: 1 cycle at 95°C for 5 min, 45 cycles at 95°C for 10 s and 60°C for 30 s. The result of initial oropharyngeal sample was uncertain (only the ORF1ab gene was positive) and the result of sputum was reported to be negative. However, the intermittent fever was not stopped during the days of antibiotic therapy (4 days). The chest CT showed some old opacities had decreased but some new ground-glass opacities appeared in the lingular segment of left superior lobe (Figure 1B), which was consistent with atypical pneumonia. The patient's pulse oxymetric saturation was 94% in ambient air at this time. Oxygen supplementation was administered due to the development of pneumonia. Results of initial specimens for pathogen tests were all negative, including influenza A and B virus, legionella pneumophila, mycoplasma pneumoniae, chlamydia pneumoniae, Q-rickettsia, adenovirus, respiratory syncytial virus, parainfluenza virus, coxsackie virus and EB virus antibody. Given the patient had been exposed to a SARS-CoV-2 contact, oropharyngeal samples were constantly sent for virus detection every day. On the 5th day of admission, the genes of NP and ORF1ab in oropharyngeal sample were positive, thus the SARS-CoV-2 infection was confirmed. In addition, the sputum specimen at the second time was still negative. During the antibiotic therapy days, the patient's vital signs remained stable, despite the uncontrollable intermittent fevers (Figure 2) and low oxymetric saturation around 95% (Table 2).

Body temperature (axillary surface) of the patient in hospital
Summary of treatment and main monitoring index for the patient in hospital

Results of the real-time reverse transcriptase polymerase chain reaction. INT, interferon-α1b; LPV, lopinavir/ritonavir; -, negative; +, positive.
When this patient was confirmed as SARS-CoV-2 infected, the antiviral treatment of lopinavir/ritonavir (peroral, lopinavir 400 mg/ritonavir 50 mg, twice per day), arbidol (peroral, 200 mg three times per day) and interferon-α1b (aerosol inhalation, 50 μg twice per day) were initiated. Ibuprofen was also given as needed to manage the fever symptoms. At the same time, the antibiotic therapy was discontinued. After 7 days of antiviral therapy, the patient's clinical condition improved but his appetite did not improve. His body temperature gradually returned to normal level (Figure 2) and his oxygen saturation values improved from 94 to 97% in ambient air (Table 2). Therefore, supplemental oxygen was discontinued. On the 11th day of admission, an oropharyngeal sample was sent for rRT-PCR analysis and a negative result was obtained. The CT results also revealed that opacity lesions in in both lungs were notably absorbed (Figure 1C). In the following 2 days, another consecutive oropharyngeal sample remained negative (Table 2).
The commonly reported side effects of lopinavir/ ritonavir include: increased serum cholesterol and triglycerides, hyperglycaemia and serum amylase. Moreover, arbidol was reported to cause side effects such as increased serum transaminase. According to the above information, laboratory tests were carried out including routine blood test, hepatic function, renal function, electrolytes and blood chemistry every other day. The antiviral therapy continued for 7 days and terminated due to clinical improvements and mild elevation of AA by 69 U/l and of GOT by 47 U/l. The patient remained hospitalized for condition observation and his appetite gradually improved. The patient was discharged on the 16th day of admission after recovery (Figure 1D, Figure 2, Tables 1 and 2).
Discussion
Here we report a case of SARS-CoV-2-induced pneumonia, in which the antiviral therapy of lopinavir/ ritonavir combined with arbidol and interferon-α1b resulted in all the related symptoms resolving.
Though the source of SARS-CoV-2 is inconclusive, the possibility of person-to-person transmission has been reported [7]. The identification of SARS-CoV-2 was delayed because of negative results from oropharyngeal and sputum specimens for the first time. At this time the CT chest result suggested the suspected SARS-CoV-2 pneumonia, while that was inconsistent with the PCR results. For the similar MERS-CoV sampling process, lower respiratory tract specimens such as tracheal aspirate and bronchoalveolar lavage are recommended due to their high virus loads [13]. It was reported that SARS-CoV-2 could be found in the specimens from nasopharynx, oropharynx, stool or even serum [14]. When taking a nasopharynx sample the patient may sneeze easily, and it is not easy to obtain the lower respiratory tract specimens, thus the oropharynx specimen was collected in this case. There were many factors that might affect the PCR results, such as sampling process, specimen storing condition, measuring operation and virus expression in the samples. Therefore, the negative result of virus RNA detection needed to be repeated to ensure a reliable and accurate diagnosis, especially when the medical history or chest CT results indicated a possible SARS-CoV-2 infection. Due to time constraints, we did not sequence the detected genes; however, this is unlikely to invalidate the final diagnosis of SARS-CoV-2 for this patient. This case also suggested that the CT likely indicates SARS-CoV-2 infection earlier than the PCR detection. Thus, CT is recommended to be applied in the presumptive diagnosis of SARS-CoV-2 infection in outbreak areas. It is notable that in our clinic, some finally identified SARS-CoV-2 patients firstly visited the hospital only for abdominal discomfort.
There are still a lot of unknowns about SARS-CoV-2. Through analysing its genome sequences and clinical symptoms, it showed homology with SARS-CoV and MERS-CoV. Based on this, the current therapeutic regimes for SARS-CoV-2 have mainly been adapted from the treatments of SARS-CoV and MERS-CoV, including antibiotics and antiviral therapy. However, an appropriate and effective treatment regimen for SARS-CoV-2 infection has not been established. Many therapeutic active substances have demonstrated inhibitory effects on SARS-CoV or MERS-CoV in vitro [15,16]. The combination of protease inhibitors (lopinavir/ritonavir) with nucleoside analogues (ribavirin) was usually applied in the treatment of SARS-CoV patients. Chu et al. [17] reported lopinavir/ritonavir with ribavirin had a better outcome than the only ribavirin treatment. In the treatment of MERS-CoV, there were two case reports about the combination of lopinavir/ ritonavir and interferon [11,18]. A clinical trial using lopinavir/ritonavir and interferon for MERS treatment was planned in Saudi Arabia [19]. Although the combination of lopinavir/ritonavir and ribavirin displayed good results in SARS-CoV infection, this regimen did not show improved outcomes compared with lopinavir/ritonavir only in our hospital in several cases. Thus, ribavirin was removed from our drug cocktail list. As a replacement of ribavirin, broad-spectrum antiviral arbidol was selected in this case. Arbidol is employed as an anti-influenza drug in several countries, which can block the membrane fusion between virus and target host cells. Indeed, recently it was revealed that arbidol could inhibit Ebola virus in vitro [20]. Moreover, the first reported American SARS-CoV-2-infected patient used remdesivir in his antiviral regimen [14]. This drug is under clinical development for the treatment of Ebola virus infection. Therefore, the final antivirus regimen in our case was a combination therapy with lopinavir/ritonavir, arbidol and interferon-α1b. Although the antiviral decision herein was based on results in vitro and diseases with similar viruses, randomized controlled trials are needed to evaluate the safety and efficacy of antiviral regimen in this case for the treatment of SARS-CoV-2-infected patients. Well-designed clinical trials on new antiviral agents or combinations of known therapeutic agents for patients with SARS-CoV-2 infection are urgently needed. In addition to antiviral regimens, symptom management and supportive care for people infected with SARS-CoV-2 to relieve symptoms should not be ignored as there was no specific therapy for this virus at present.
During the antiviral therapy period, the patient's appetite continuously declined. On the last day of antiviral therapy, this patient even vomited. His liver function showed some abnormal changes at this time, which compelled us to re-valuate the therapy regimen. Considering his clinical improvements, we finally determined to cease the antiviral therapy. To avoid or decrease the side effects of lopinavir/ritonavir or arbidol (both drugs can cause nausea, vomiting and elevated serum transaminase) described on the drug label, we may reduce the dose or dosing frequency in the future therapy. Of course, this point also needs to be validated in the future clinical trials. Corticosteroids are effective in controlling the fever and reversing changes in the chest CT results, but they have the risk of promoting viral replication. Some experts stated that the interferon and systemic steroid in preventing immune-mediated lung injury in the treatment of SARS-CoV infection needed more investigation [21]. As the pneumonia development of the patient in this case was not very severe, we did not administer such drugs during the whole treatment. The interferon-α1b was given by aerosol inhalation in this case, not through subcutaneous injection as the drug label instructed. This is mainly because inhalation is more acceptable than subcutaneous injection for patients. Interferon-α1b inhalation is very common in China for the treatment of respiratory diseases, but it has no strong clinical evidence.
There are several limitations to this case report. Firstly, the age of this patient was not very old and his physical quality was better than many elderly patients. According to the report of the health office of China, the age of most of the SARS-CoV-2-infected people ranges from 40 to 60. Thus, the patient in this case had an age advantage that might have helped his recovery. The possibility of spontaneous improvement was not excluded in this case. Morever, for this patient, hypoxaemia and multiorgan failure were not found despite intermittent fevers that lasted for several days. This suggested that the effects of the antiviral therapy in this case was hard to say. For this reason, further well-designed trials on the efficacy of the reported antiviral regimen here are urgently needed. Secondly, as a single case report, the tolerability of the used antiviral regimen by the patient was not investigated. The tolerability of the patient has a great influence on the final therapy effect, which should not to be overlooked in further studies. Thirdly, the viral loads of the samples were not quantitatively reported, thus the dynamic relations between virus numbers in respiratory tract and time was not determined. The shortcomings of the used PCR method limited the precise evaluation of our reported antiviral regimen. We hope an accurate and quantitative detection method will be established in future studies.
In summary, the results of this case propose that the lopinavir/ritonavir-based triple antivirotic treatment can be applied in some cases of SARS-CoV-2-infected patients, and the gastrointestinal adverse reactions of this regimen should not be overlooked. Further clinical trials evaluating the usage of this combination antiviral therapy are required.
Footnotes
Acknowledgements
We are grateful for the financial support from Health & Family Planning Commission of Hubei Province (Grant No. WJ2017Q031) and Young & Middle-aged Medical Key Talents Training Project of Wuhan (Grant No. 2018-6).
The authors declare no competing interests.