
Abstract
Patients with a life-limiting diagnosis of pulmonary arterial hypertension (PAH) or chronic thromboembolic pulmonary hypertension (CTEPH) need disease-specific information, ability to cope, and functioning social networks. This cohort study investigated the experiences of PAH and CTEPH patients who received information about their diagnosis, treatment, and management, in addition to coping and social support. Sixty-eight adult patients (mean ∓ SD, age 67 ∓ 14; 66% women) were included. A total of 54% of the patients wanted more information. Patients received information mostly in areas concerning medical test procedures, the diagnosis, disease severity, possible disease causes, and how to manage their disease. Coping ability was significantly better in patients who were satisfied with the received information (P= 0.0045). The information given to PAH or CTEPH patients and their communication with healthcare professionals can be greatly improved. Gaps in information and misunderstandings can be avoided by working in cooperation with the patients, their relatives, and within the PAH team.
Keywords
Introduction
Pulmonary arterial hypertension (PAH) encompasses a group of disease processes that cause increased right ventricular load and that commonly lead to right heart failure. PAH patients are faced with the prospect of having a severe, rapidly progressing condition that is fatal if untreated. 1 PAH may be idiopathic (IPAH), hereditary (HPAH), or associated with other conditions, ie, associated pulmonary arterial hypertension (APAH). These conditions include congenital heart disease with left-right shunt, portal hypertension, HIV infection, the use of certain drugs, and rheumatologic systemic disease, which, in this case, often is referred to as “connective tissue disease,” even though the vascular component is substantial. 2 With regard to PAH, the most common connective tissue disorder is systemic sclerosis (SSc), which has a poor prognosis once PAH has developed.3,4 SSc-APAH is often diagnosed at a late stage when the patients have advanced disease with both severe pulmonary and extrapulmonary symptoms. 5 PAH-associated mortality remains high, but advances in diagnostic techniques and targeted pharmacological treatments are contributing to better survival.6,7 Chronic thromboembolic pulmonary hypertension (CTEPH) is another type of pulmonary hypertension (PH), partly with similar symptoms and clinical picture to those of PAH. CTEPH patients may, however, be candidates for pulmonary thrombendarterectomy. 8 In a small group of PH cases in whom pharmacological treatment fails, lung or heart-lung transplantation may be an option. 9 In the initial stages of PAH and CTEPH, symptoms are often vague and unspecific but patients commonly present with unexplained dyspnea, fatigue, and weakness.4,10 Accordingly, many patients see several medical specialists before being diagnosed with PAH, 11 13 A key reason for this is the very low prevalence of PAH and CTEPH and the lack of awareness and knowledge about PAH and CTEPH amongst healthcare professionals. 14
According to data from the Swedish PAH registry (SPAHR), of Sweden's 9.5 million inhabitants, approximately 590 suffer from PAH, including CTEPH. 15 Population-based studies show a PAH prevalence of 15 to 50 individuals per million. 16 About twice as many women as men are affected, and the average age of patients with PAH and CTEPH is between 50 17 and 58 years. 15 Given the poor prognosis for this disease, treatment compliance and follow-up are very important. In addition, patients need to learn to use coping mechanisms to adjust to living with a life-threatening disease. 18 Hence, information that is given to patients after a diagnosis of PAH is essential, 11 as is social support for these chronically ill patients. 19 The latter may have an impact on patient health by influencing the patient's assessment of stressors and subsequent coping behavior. 19
Given the complex presentation and treatment of PAH, it is important that patients are managed by a multidisciplinary specialist team that includes physicians, nurses, physiotherapists, counselors, and others with extensive PAH experience. 2 Relationships must also be established with the patient's community care team, including the primary care facility, as some aspects of routine health and community care can be delivered in these settings.12,20
The illness and treatment strategies in chronic disease tend to fluctuate over time, which means that patients may have new or different information needs at different times in life. 21 A lack of effective communication within and between agencies with no direct involvement with the patient is not uncommon, and this is especially true for younger patients. 22 Healthcare professionals must realize that they play a pivotal role in providing information that helps patients understand and adhere to their prescribed medications, treatments, diet, and exercise regimes. 20 Although it may be unpleasant to talk about difficult matters, there is no excuse for withholding information from patients who want and need it. 23
Notably, there is limited knowledge about PAH and CTEPH, and more scientific research is needed both to better understand how the disease affects the patients psychosocially and to better understand how to support patients with PAH and CTEPH. Other reports have noted the benefits of providing information to these groups of patients11,18 with specific information needs, 24 but currently there are no tools to assess the needs of these patients.
The aim of the present study was to describe the perceptions of received information regarding diagnosis, treatments, and management, as well coping and social support perceived by patients with PAH and CTEPH.
Methods
Design and participants
This descriptive, preliminary survey was performed in May 2013 and was conducted at Skäne University Hospital, one of seven university hospital-affiliated PAH centers in Sweden. All 85 adult PH patients currently being treated or followed-up at the PAH center at Skäne University Hospital were asked to participate. Inclusion criteria were the ability to communicate in Swedish, being free of mental disorders, and not being on the waiting list for lung transplantation.
Ethics
The study conformed to the principles outlined in the Declaration of Helsinki. 25 The project was approved by the directors of the participating departments. The regional ethical review board in Lund, Sweden, approved the study (LU 2011/364). Participation in the study was voluntary, and patients could withdraw from the study at any time without any consequences for future care. Written informed consent was obtained from all participants. The consent form information emphasized that participation was voluntary, and each patient was given sufficient time to consider the decision and to reflect upon participation in the study. Patient confidentiality was guaranteed.
Procedure
Eligible patients who were identified as being part of the PAH cohort were mailed an information letter and an informed consent form to sign. Each mailing included socio-demographic questions plus the questionnaires and return envelope. One reminder was sent after three weeks.
Study measures
The QLQ-INFO25 25-item questionnaire was originally written in English and used to evaluate the received information. 26 Permission to use the Swedish version of the questionnaire was obtained from the European Organization for Research and Treatment of Cancer (EORTC). Face and content validity was tested on a group of Swedish physicians and nurses who work in PAH care, and only a single parenthetic sentence that refers to chemotherapy was deleted from the questionnaire. The questionnaire comprises 25 items that reflect different dimensions of the care process, including information about the disease (four items); medical tests (three items); medical treatments (six items); other healthcare services (four items); and other things that patients can do to stay well, written information, receiving more or less information, and information supplied on CD or tape/ video (eight single items). 26 The instrument uses a four-point Likert scale (from one, not at all, to four, very much) except for four dichotomous (yes/no) response items. It also allows the respondent to add comments about their desire to receive more or less information; these responses are qualitative information. All items and scales are linearly transformed to a 0-100 scale before statistical analysis. 26 Psychometric testing of the version of the QLQ-INFO25 used in this study revealed a standardized Cronbach's alpha of 0.90 for the whole scale and raw Cronbach's alpha values of 0.80 (disease), 0.87 (medical tests), 0.80 (treatment), and 0.70 (other services) for the four subscales.
The Mastery Scale 27 was used to evaluate the patient's coping capacity. The Mastery Scale tool is designed to analyze the degree to which patients feel that they are able to control factors that affect their life situation and thus their quality of life and well-being. It includes seven items and uses a four-point Likert scale; thus, the total score range is from 7 points (minimum score) to 28 points (maximum score). A higher score indicates a greater capacity to cope. The instrument has demonstrated acceptable reliability.27,28 In the present study, Cronbach's alpha was 0.82.
The Social Network and Support Scale (SNASS) (19 items)29,30 was used to map the patients’ social support network and to assess their level of emotional support, practical support, homogeneity, and approachability. Of the 19 items, 17 items were scored as follows: Yes, absolutely = one point; Yes, partly = two points; and No = three points. A lower score indicates stronger social support. 31 Two items are questions: “Which person is most important in your social network?” and “Which person gives you the best support?” The SNASS has shown good validity and reliability.29,32
Statistical methods
Statistical analyses were performed using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA). Univariate associations between components of QLQ-INFO25 and disease duration, the Mastery Scale, and SNASS were assessed using Spearman rank correlations. Univariate associations of components of the QLQ-INFO25 (global score and subscores) across socio-demographic grouping variables were analyzed using the Mann-Whitney U test, the Kruskal-Wallis test, or the Jonckheere-Terpstra test, depending on the nature of the grouping variable (2 groups - Mann-Whitney, >2 groups no ordering - Kruskal-Wallis, >2 groups, ordered - Jonckheere-Terpstra). Results are given as mean ∓ standard deviation (SD) and median and range. The level chosen for statistical significance was P < 0.05. Comments about receiving more or less information were grouped according to content.
Results
Demographic data and other characteristics of the 68 PAH and CTEPH patients.

Idiopathic pulmonary arterial hypertension.
Heritable pulmonary arterial hypertension.
Associated pulmonary arterial hypertension excl systemic sclerosis.
Systemic sclerosis - associated pulmonary arterial hypertension.
Chronic thromboembolic pulmonary hypertension.
Chronic thromboembolic pulmonary hypertension including endarterectomy.
Endothelin receptor antagonists
phosphodiesterase.
Calcium channel blockers.
Prostacyclin derivatives.
Research medications of a randomized blinded controlled clinical trial.
A comparison between patients with or without sclerosis - associated pulmonary arterial hypertension. Mean values ∓ SD, median and range of perceived information (QLQ-INFO25); score range 0-100. A higher score reflects better perceived information.

Associated pulmonary arterial hypertension with systemic sclerosis.
Mann-Whitney U test. *<0.05.
The univariate analyses showed no statistically significant differences between the received information for the four areas of multi-items and the eight single items in terms of age, sex, marital status, or diagnosis. Respondents with a high level of education showed significantly higher global scores (P = 0.04), and, compared to patients with a lower level of education, they wanted to receive more information (P = 0.01). Respondents who had a PAH or CTEPH diagnosis for a shorter time reported receiving more information about treatment compared with those who had a PAH or CTEPH diagnosis for a longer time (P = 0.05).
Spearman rank correlation coefficients of associations between patients’ received information related to mastery and social support.

PAH and CTEPH patients reported that the most important people in their social networks were close relatives (93%) or others, such as friends or people from their church (7%). Those who provided the best support were close relatives (87%) or others, such as friends, neighbors, and people from the healthcare organization or from their church (13%).
Topics on which the patients desired more information (N = 40).
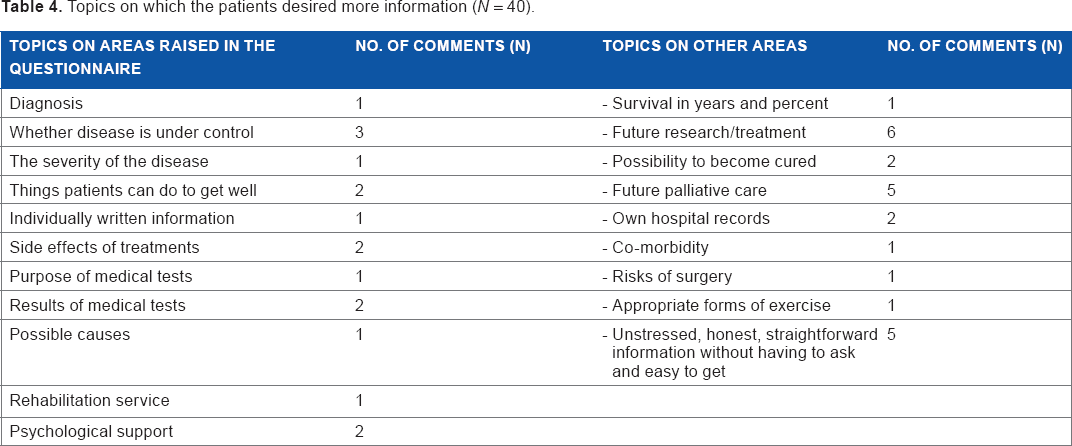
Only one respondent desired less information than that which was provided to them. The respondent commented, “Sometimes you have information about what will happen or what you may have from certain doctors. You may feel worse leaving than coming to the clinic because of that.”
Discussion
The present study examined the perspectives of PAH and CTEPH patients about the information they received about PAH and CTEPH and about disease, treatment, management, social support, and their ability to cope. There is a higher female/male ratio for patients with SSc-APAH, the illnesses of these patients are more severe, and their long-term prognosis is worse than for other PAH subgroups. 33 Patients with SSc-APAH had higher scores in 9 of the 13 areas of received information than other PAH or CTEPH patients; however, these differences were not significant. One important and challenging finding was that although the patients reported that the received information was helpful overall, the mean score of the QLQ-INFO25 was 48.6 out of 100. In all of the areas that measured patients’ perceptions of the received information, the mean score ranged between 2.9-67.3. This means that there is great potential for improving the way that information is communicated to these patients. An important issue to raise is what information and support physicians need to give and at what stage a patient is ready to receive and understand the information being given. It could be speculated if low scores in certain areas may indicate that patients did not receive appropriate information at the time of their diagnosis. However, when the study began, the patients had a PAH or CTEPH diagnosis for an average of 4 years; thus, it is possible that the patients had forgotten or suppressed the information they received at the time of their diagnosis. Notably, though, the results showed no statistically significant differences, except regarding information about treatment, between patients who had a PAH or CTEPH diagnosis for a longer time versus patients who had a PAH or CTEPH diagnosis for a shorter time. Earlier research found that 58% of patients with PAH have cognitive impairment, with memory problems a dominant factor in 40%. 34 Another explanation may involve the patient's prospects for the future, as described by Calman, 35 in that there is a gap between realities on the one hand and hopes and expectations on the other hand. Regardless of speculation about why patients had relatively low scores in several areas of the QLQ-INFO25, healthcare professionals must narrow the gap between perceived and optimal information. One way to accomplish this is to implement person-centered care in which the patient and the provider are partners and healthcare planning is based on a patient's individual circumstances, resources, and obstacles, including how the disease affects their daily lives. Communication is an important part of person-centered care; in addition, care should be planned with the input of the patient, and the healthcare provider/patient relationship should be facilitated by establishing partnerships between patients and healthcare professionals. 36 A prerequisite for PAH and CTEPH care is a PAH team that has diverse skills and experience, and it is important that the team works together closely so that within the team it is clear who provides what information and so that there is follow-up to ensure that the patient understands the information that is given. For serious illnesses, it is important to have bi-directional information sharing and a holistic perspective in which patients, families, and the healthcare teams are included in decision-making and in discussions about autonomy. 37 Having a heavy workload is not an excuse - in fact, a Swedish study has shown that lack of time is not the main obstacle to forging effective teams. Effective teams are achieved by creating a climate of open communication, by having an active formal leader, and by having autonomous co-workers. 38
In the present study, patients who were satisfied with the received information and who found the overall information to be helpful had a significantly better coping ability. No study has measured coping or social network and support in PAH or CTEPH patients, but Wryobeck et al. 39 stated in a review that unsuccessful efforts to cope with PH can result in physiological and psychological disorders. In some areas of received information (QLQ-INFO25), there was a significant association between practical support and the approachability of the patient's social network. The present study did not examine the role of next of kin in terms of received information and the patient's ability to understand the information, but there is evidence that next of kin should be involved early on ie, when the seriously ill patient first meets with healthcare professionals.40,41 One study has shown that the PAH patient's family caregiver plays crucial roles in different ways in the patients contact with the healthcare organization. 42
More than half of the patients in the present study wanted to have more information. One area about which some patients wanted more information was future palliative care. Seriously ill patients need information about what constitutes palliative care and what palliative care can offer. 43 Patients with PAH or CTEPH are entitled to receive accurate but encouraging information, and healthcare professionals must also communicate their prognosis and, at the appropriate time, provide an opportunity to discuss end-of-life issues. 39 Matura et al. 44 found that patients use online peer support on an internet-based PAH discussion board when they seek guidelines and wish to confirm information about PAH or CTEPH. Patients who have experience with PAH or CTEPH could be effective counselors, but the healthcare professionals must also take responsibility for this. One of the aims in developing the QLQ-INFO25 was to have a short patient questionnaire that would work clinically as a tool for patients and for healthcare professionals in terms of initiating discussions about information. 45 We therefore suggest that in the future, the QLQ-INFO25 could provide a basis for communication between patients with PAH or CTEPH and the PAH team. This may be accomplished with an updated version in which, for example, “information provided by video or CD-ROM” is changed to “information available using social media technologies.”
Limitations
One limitation of this study is that in-depth information was not obtained about each patient's clinical condition, and one reason for drop-out was fatigue caused by this serious illness. If the respondent group and the non-respondent group are unequal, the results cannot be generalized. However, in this study, there were no major differences between the respondent group and the non-respondent group.
Many tests were performed because of the explorative nature of the study. However, many of the detected associations had very low P-values, indicating that they are not artifacts of multiple testing. Grinnan et al. 46 found that the prognosis among PAH patients is similar to the prognosis for the most severe forms of cancer; thus, we think that the QLQ-INFO25, which was originally developed for cancer patients, is also suitable for patients with PAH or CTEPH. The face validity was found to be good when the patients understood the wording in the QLQ-INFO25 questionnaire, judged the items to be relevant to the topic, and found the items to be sufficiently clear and readable. The main limitation of this study is its retrospective nature, since there were differences among the patients in terms of the time elapsed since diagnosis. In addition, the study was carried out at a single center. Future studies, particularly multicenter studies, are needed to determine the validity and reliability of the instrument as well as the value of the findings of the present study.
In conclusion, there is great potential for improving and optimizing the exchange of information between PAH and CTEPH patients and healthcare professionals. In general, patients wanted more information, and patient satisfaction with the received information was associated with a better ability to cope. Knowledge gaps and misunderstandings can be avoided by cooperation with the patients and by good communication within the PAH team.
Author Contributions
Conceived and designed the experiments: BI, TS, BE. Analyzed the data: BI, TS. Wrote the first draft of the manuscript: BI. Contributed to the writing of the manuscript: BI, TS, GR. Agree with manuscript results and conclusions: BI, TS, BE, RH, GR. Jointly developed the structure and arguments for the paper: BI, TS, BE, RH, GR. Made critical revisions and approved final version: BI, TS, BE, RH, GR. All authors reviewed and approved of the final manuscript.
Supplementary Data
Abbreviations
Associated pulmonary arterial hypertension excl systemic sclerosis
Chronic thromboembolic pulmonary hypertension
Chronic thromboembolic pulmonary hypertension including endarterectomy
Calcium channel blockers
European Organisation for Research and Treatment of Cancer
Endothelin receptor antagonists
Idiopathic pulmonary arterial hypertension
Heritable pulmonary arterial hypertension
Pulmonary arterial hypertension
Pulmonary hypertension
Phosphodiesterase
Prostacyclin derivatives
The Social Network and Support Scale
Swedish PAH registry
Systemic sclerosis - associated pulmonary arterial hypertension
Footnotes
Acknowledgments
The authors would like to thank RN Liselotte Persson for excellent assistance in collecting and retrieving patient data.