
Abstract
Immune thrombocytopenia (ITP) is an acquired hemorrhagic condition characterized by the accelerated clearance of platelets caused by antiplatelet autoantibodies. A platelet count in peripheral blood <100 × 109/L is the most important criterion for the diagnosis of ITP. However, the platelet count is not the sole diagnostic criterion, and the diagnosis of ITP is dependent on additional findings. ITP can be classified into three types, namely, acute, subchronic, and persistent, based on disease duration. Conventional therapy includes corticosteroids, intravenous immunoglobulin, splenectomy, and watch-and-wait. Second-line treatments for ITP include immunosuppressive therapy [eg, anti-CD20 (rituximab)], with international guidelines, including rituximab as a second-line option. The most recently licensed drugs for ITP are the thrombopoietin receptor agonists (TRAs), such as romiplostim and eltrombopag. TRAs are associated with increased platelet counts and reductions in the number of bleeding events. TRAs are usually considered safe, effective treatments for patients with chronic ITP at risk of bleeding after failure of first-line therapies. Due to the high costs of TRAs, however, it is unclear if patients prefer these agents. In addition, some new agents are under development now. This manuscript summarizes the pathophysiology, diagnosis, and treatment of ITP. The goal of all treatment strategies for ITP is to achieve a platelet count that is associated with adequate hemostasis, rather than a normal platelet count. The decision to treat should be based on the bleeding severity, bleeding risk, activity level, likely side effects of treatment, and patient preferences.
Keywords
Introduction
Immune thrombocytopenia (ITP) is an acquired hemorrhagic condition characterized by the accelerated clearance of platelets caused by antiplatelet autoantibodies such as anti-glycoprotein (GP) IIb/IIIa.1,2 Autoreactive B- and T-cells have important roles in antibody generation in ITP patients. 3 GPIIb/IIIa is one of the major target antigens recognized by platelet-reactive CD4 + T-cells.4–6 A platelet count in peripheral blood of <100 × 10 9 /L is the most important criterion for the diagnosis of ITP.1,2 However, the platelet count is not the sole diagnostic criterion, and the diagnosis of ITP is dependent on additional findings. ITP can be classified into three types, namely, acute, subchronic, and persistent, based on disease duration. 2 ITP in adults tends to be subchronic/persistent, relapsing, and very often, refractory to treatment. 7
Conventional therapy includes corticosteroids, intravenous immunoglobulin (IVIg), splenectomy, and watch-and-wait.1,2 Initially, 70%-80% of patients respond to corticosteroids, and 10%-30% attain durable remission. 2 Splenectomy is avoided in young children because of infection risk and because the prevalence of spontaneous resolution of ITP is high. 8 Second-line treatments for ITP include immunosuppressive therapy [eg, anti-CD20 (rituximab)], 9 with international guidelines including rituximab as a second-line option.10,11
In contrast to immunosuppressive therapy, physiological therapy was recently introduced. 12 These drugs include thrombopoietin receptor agonists (TRAs), such as romiplostim and eltrombopag.13–16 TRAs are associated with increased platelet counts and a reduced number of bleeding events. TRAs are usually considered as a safe and an effective treatment for patients with chronic ITP at risk of bleeding after failure of first- or second-line therapies.
Herein, we discuss the accepted therapies available for ITP, as well as potential for the use of alternative drugs and novel treatments. We also describe the pathogenesis and clinical manifestations involved in the development and progression of ITP.
Assessment of the Literature
Reference articles were identified by an internet search of the PubMed database. The search key words were idiopathic thrombocytopenic purpura and immune thrombocytopenia.
Pathophysiology
The most commonly identified antigenic targets of ITP autoantibodies are GPIIb/IIIa and GPIb/IX; a considerable number of ITP patients have antibodies directed to multiple platelet antigens. 17 Several lines of evidence link T-cells to the pathogenesis of ITP. The T-cell changes implicated include excessive activation and proliferation of platelet antigen-reactive cytotoxic T-cells, production of abnormal helper T-cells (Th), and abnormalities in the number and function of regulatory T-cells (Tregs).18–21 Platelet-reactive CD4+ T-cells have been found in the blood samples of ITP patients, with the major target antigen being GPIIb/IIIa. 4
CD4+ Th cells are divided into four main subsets (1, 2, 3, and 17) according to the type of cytokines they produce.22,23 Th1 cells are involved mainly in macrophage activation and production of interferon gamma and interleukin (IL)-2. Th2 cells are involved mainly in secretion of IL-4 and IL-10, the humoral immune response, and inactivation of several macrophage functions. 22 Th3 cells generate transforming growth factor-β1. Th17 cells generate IL-17 and modulate immune responses.22,24 Several studies have found evidence supporting polarization of Th cells in the immune response in patients with chronic ITP.21–30 Those reports have suggested that a peripheral regulatory mechanism controlling these GP-reactive T-cells is necessary to prevent autoimmunity (Fig. 1).20,31
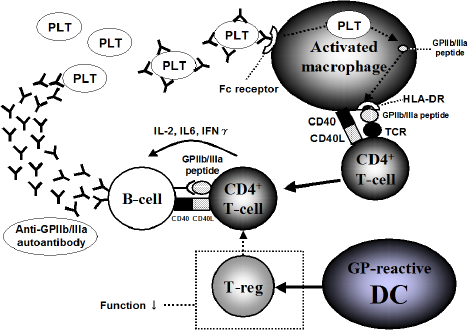
Pathogenesis of ITP. Activated macrophages in the reticuloendothelial system transfer the antigenic information such as GPIIb/IIIa peptide to autoreactive CD4+ T-cells. autoreactive CD4+ T-cells and antibody-producing B-cells maintain antiplatelet autoantibody production in ITP patients. there exists a continuous pathogenic loop in ITP. treg in ITP has less functional strength than it used to.
CD4+ Tregs have critical roles in the maintenance of peripheral tolerance by suppression of the activation and proliferation of many cell types.32,33 Tregs are divided into two subtypes, namely, naturally occurring Tregs and induced Tregs, based on their ontogeny and mode of action. Naturally occurring Tregs are generated in the thymus gland and constitutively express cytotoxic T-lymphocyte-associated antigen-4 and transcription factor forkhead-box p3 (Foxp3). 20 The previously mentioned Th3 cells are Foxp3 negative, but these cells are included in Tregs. 34 A reduction in Treg function has been reported in several autoimmune diseases. 33 Some studies in ITP patients have also shown reduced levels of Foxp3 and abnormal function of Tregs.35–37
The major physiological role of B-cells is antibody production.38,39 The number of circulating B-cells secreting anti-GPIIb/IIIa antibodies has been reported to be increased in patients with ITP.40,41 The dysregulation of B-cell development has also been associated with ITP. 28 Serum concentrations of B-cell activating factor were shown to be significantly increased in patients with active ITP. 42 B-cells are also efficient at presenting antigens, including low concentrations of antigens, to T-cells.28,39 These findings suggest that a rational approach to ITP treatment could involve B-cell depletion, such as with rituximab.38,39
The spleen plays an important role in pathways leading to thrombocytopenia. This organ is the primary site of antibody production, as well as being important in the clearance of antibody-coated platelets (Fig. 2).43–46
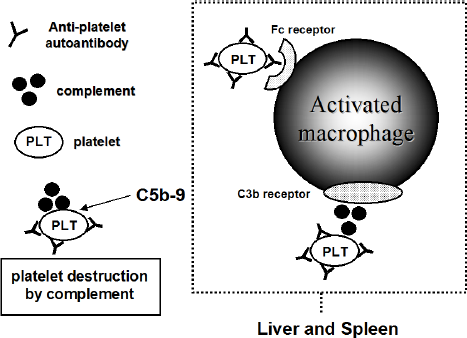
Mechanisms leading to the thrombocytopenia. Human macrophages express Fc receptor that binds IgG specifically. Liver and spleen are dominant organs for the clearance of IgG-coated platelets. There is also direct cytotoxicity by complement such as C5b-9.
Human macrophages express several Fc receptors that bind IgG specifically. 47 There are two classes of Fc receptors: high affinity (FcγRI) and low affinity (FcγRII, FcγRIII). Removal of opsonized platelets is dependent on low-affinity receptors.48,49
Clinical Features
Findings such as attack of fever, bone or joint pain, infection with human immunodeficiency virus, morphologic abnormalities of the skeleton or soft tissue, nonpetechial rash, lymphadenopathy, abnormal hemoglobin level, white blood cell count, abnormal white cell morphology, a family history of low platelets, or easy bruising are not typical of ITP and should prompt additional diagnostics such as bone marrow evaluation to rule out other disorders.2,10,11
Most children have bruising or purpura, although they are asymptomatic. 50 There may be tiny red spots or larger areas of purpura. Pediatric ITP often occurs ~2 weeks after a viral infection. Most children with ITP recover within six weeks. ITP is acute in 70%-80% of children and chronic in 20%-30%.
In adults, 51 ITP arises gradually and does not usually follow a viral illness. Symptoms are highly variable: no symptoms, purpura, mild bleeding, or severe bleeding. Unlike pediatric ITP, most adults with ITP continue to have a low platelet count indefinitely (chronic ITP). However, the differences between ITP in adults and children are not as clear as suggested here.
Laboratory Measurements
A presumptive diagnosis of ITP can be made if patient history, physical examination, complete blood count, and examination of peripheral blood smears do not suggest other causes of thrombocytopenia (Table 1). There is no gold standard test that can reliably establish the diagnosis. It remains unclear whether bone marrow examination is necessary for all patients with ITP. 10 Assays for antibodies for specific platelet GPs are not recommended routinely because levels of platelet-associated IgG are elevated in ITP and non-ITP. 17 However, existence of anti-GPIIb/IIIa antibody may be useful for the diagnosis of ITP (Table 1). 40
Diagnosis of ITP.

Differential Diagnoses
The diagnosis of primary ITP is one of exclusions. Thrombocytopenia can be caused by systemic disease, infection, drugs, or primary hematologic disorders. 10 Bleeding after surgery, dentistry, and trauma must be considered when estimating the possible duration of chronic thrombocytopenia or an alternative bleeding disorder. Differential diagnoses can classify patients into two groups. One group includes patients with ITP, such as systemic lupus erythematosus, whereas the other includes patients with non-ITP, such as aplastic anemia and leukemia. Although aplastic anemia may present initially as isolated thrombocytopenia, it is followed within days, weeks, months, or even years by anemia and leukopenia. Moreover, leukemia never presents as isolated thrombocytopenia. International consensus documents and guidelines should be consulted regarding differences between primary ITP and the other conditions.10,11
Treatment
Initial Management
Determination of the threshold for a minimum platelet count or specific age at which a typical patient with ITP should be treated is difficult. 11 The goal of all treatment strategies for ITP is to achieve a platelet count that is associated with adequate hemostasis, rather than a normal platelet count. 11 Therefore, if a bleeding symptom is not found, treatment may not be needed. Patients should be treated with platelet-enhancing agents if the platelet count is <30 × 10 9 /L and mucosal bleeding has started, although a threshold of 30 × 10 9 /L may not be suitable for children. Treatment may also be appropriate if: follow-up cannot be assured; there are concerns regarding the activity or risk of bleeding; and there is a need for procedures associated with bleeding risk. In conclusion, the decision to treat should be based on bleeding severity, bleeding risk, activity level, likely side effects of treatment, and patient preferences.51–54
First-Line Therapy
Corticosteroids
Corticosteroids remain the most commonly used first-line therapy for ITP. Treatment is initiated with prednisolone or prednisone (1-2 mg/kg per day, p.o., single or divided doses). Approximately, two-thirds of patients achieve a complete or partial response with corticosteroids at these doses, with most responses occurring within the first week of treatment. 55 In general, corticosteroids are initially effective. A study comparing high- and low-dose corticosteroids in adult patients found that low-dose therapy was initially more effective, although long-term effects have not been determined.11,56 However, because of their side effects, long-term corticosteroids should be avoided in children with acute ITP. 11
IVIg
IVIg therapy is administered to patients requiring rapid or urgent elevation of platelet count (eg, intraoperative or life-threatening bleeding). IVIg increases the platelet count in 70%-80% of treated patients, often within days. Several IVIg regimens have been employed, but many hematologists prefer the convenience of a 1 g/kg/day infusion for 1-2 days. 57 IVIg also affects humoral and cellular immunity by influencing the expression and activity of Fc receptors. 58 Although its incidence is low, intracerebral hemorrhage remains a severe side effect of IVIg. 11
Anti-D Immunoglobulin
Anti-D immunoglobulin (anti-D) binds to Rh(D) antigen on erythrocytes, thereby leading to clearance of antibody-coated cells and inhibiting the clearance of opsonized platelets by the reticuloendothelial system. 59 Therefore, anti-D is effective only in RhD positive individuals. Anti-D has been reported effective in approximately 50%-70% of patients treated with this agent. 60 If anti-D is chosen as therapy, care must be taken because of the risk of severe hemolysis that has been reported with some products. 11 However, subcutaneous administration abolishes the risk of hemolysis in most patients. Avoidance of use of anti-D in patients with a positive direct antiglobulin test has been recommended. 61 In addition, fatal renal failure and disseminated intravascular coagulation are reported as side effects of anti-D.11,62
Management of Helicobacter pylori-associated ITP. Secondary ITP can occur in patients with H. pylori infection. 10 The eradication therapy should be administered in patients who are found to have H. pylori infection. 11
Second-Line Therapy
Splenectomy
Splenectomy is considered by some scholars to be the gold standard treatment for ITP. In particular, it is recommended as a second-line treatment for adults unresponsive for corticosteroid therapy. Initially, 65%-70% of patients show a complete response, whereas 60%-70% show a long-term response.45,63 Types of splenectomy are open splenectomy and laparoscopic splenectomy, but the latter is associated with fewer complications than the former. 64 Splenectomy-related complications include infection, bleeding, thrombosis, and relapse. 65 In particular, the risk of infection is the major cause of mortality after splenectomy. 66
Rituximab
Rituximab is a chimeric monoclonal antibody that targets CD20 B-cell surface antigen.9,26,67,68 Several studies have reported significant responses before and after splenectomy with the use of rituximab.67–71 Despite targeting CD20 on B-cells, the mechanism of action of rituximab may involve more complex immunologic modulation. 72 In one report, successful therapy correlated with normalization of distribution of T-cell subsets, 26 and in another report, it correlated with reappearance of normal numbers and function of Tregs. 73 Adverse effects of rituximab include infusion reactions, serum sickness, and cardiac arrhythmia. Rituximab can also be used off-license as a second-line option in certain types of refractory ITP, but long-term safety is not known. 74 In addition, a recent meta-analysis could not find that rituximab was effective. 75
Third-Line Therapy
TRAs
Thrombocytopenia may result not only from platelet destruction but also from antibody-mediated damage to megakaryocytes. 45 Thus, ITP in some patients may be due to impaired production of platelets. 45 Therefore, recombinant human TPO (rhTPO) has been administered in some ITP patients,76,77 and as a result, the improvement in thrombocytopenia has been remarkable. However, all clinical trials with rhTPO were stopped after development of antibodies against rhTPO was observed in healthy volunteers. 78 Since then, the development of TRAs has progressed. Two of these new TRAs, such as romiplostim and eltrombopag, have been licensed for use in patients with chronic ITP. Binding of TRAs to the thrombopoietin receptor results in activation of intracellular signaling pathways such as JAK-STAT and mitogen-activated protein kinase (MAPK) that lead to increased production of platelets. 79 Although TRAs may markedly improve thrombocytopenia, their safety is questionable, as shown by an increasing list of severe side effects. 75
Romiplostim
Romiplostim is a recombinant fusion protein peptibody composed of two IgG1 constant regions (Fc fragments) linked to a peptide domain containing four binding sites for the thrombopoietin receptor. 80 Some evidence on the use of romiplostim in adults with ITP suggests that it increases the platelet count and reduces bleeding.81–84 Romiplostim-related adverse effects have been mild-moderate and not led to treatment cessation.15,85 Rare adverse effects include mild-to-moderate postinjection headache, fatigue, and arthralgia.81,85 Serious adverse events that continue to be under investigation include increased reticulum cells in the bone marrow, 86 increased proliferation of leukemic blasts, 87 and thrombosis. 88 However, the frequency of these adverse events appears to be low.
Eltrombopag
Eltrombopag is a small nonpeptide molecule that binds to the thrombopoietin receptor via its trans-membrane domain and activates JAK-STAT and MAPK intracellular pathways to increase platelet production.79,89,90 Once-daily oral administration of eltrombopag was found to be effective and safe in patients with chronic ITP.13,91,92 Patients with chronic ITP and platelet count <30,000/μL received eltrombopag (50 mg/day) or standard of care for six months in a double-blind phase III study. 16 Prevalence of adverse events in adult ITP was 73% for patients receiving eltrombopag compared with 25% for patients receiving placebo. 92 All adverse events were mild-moderate in severity, and increases in the prevalence of nasopharyngitis and level of alanine amino-transferase were the most frequently reported adverse events in the eltrombopag group. 92 The most common adverse events of eltrombopag in childhood ITP were headache, infection of the upper respiratory tract, and nasopharyngitis. 93 Long-term safety and efficacy of eltrombopag has been investigated in the EXTEND study, which enrolled 301 patients, with 84 and 28 patients being treated for ≥3 and ≥4 years, respectively. 94
New Agents
Anti-CD40 Ligand Monoclonal Antibody
The GPIIb/IIIa-reactive T-cell is a target for therapeutic strategies involving selective suppression of the pathogenic autoimmune response in ITP patients. One strategy is disruption of a costimulatory signal by blocking the interaction between CD40 on antigen-presenting cells and CD40 ligand (CD40L) on activated CD4+ T-cells; this interaction is essential for T-cell priming and the T-cell-dependent humoral immune response. 95 Therefore, anti-CD40L antibody could be effective against ITP. 96
IDEC-131 is a humanized monoclonal antibody against human CD40L. It binds to the trimer of CD40L on T-cells with high specificity and activity, thereby preventing CD40 signaling. 97 Kuwana et al 98 reported that CD40/CD40L blockade therapy by IDEC-131 could be effective against refractory ITP through selective suppression of autoreactive T- and B-cells to platelet antigens. Another trial with anti-CD40L monoclonal antibody showed an overall response of 24% in 46 refractory patients with ITP. 99 Anti-CD40L antibody could become a therapeutic strategy against ITP.98–100
Anti-CD20 Monoclonal Antibody
Veltuzumab is a humanized anti-CD20 monoclonal antibody with complementarity-determining regions identical to rituximab. It has unique characteristics in terms of significantly improved complement-dependent cytotoxicity. 101 Veltuzumab is active at a fraction of the conventional clinical dose of rituximab, and survival studies in lymphoma models have shown significantly higher potency of this antibody over rituximab. 101 Additional studies are needed to assess the efficacy and safety of anti-CD20 antibody as first-line therapy in adults with ITP. 102 Low-dose veltuzumab (s.c.) appears to be convenient, well-tolerated, and with promising effects against relapsed ITP. 103
Spleen Tyrosine Kinase Inhibitor
Spleen tyrosine kinase (Syk) is a cytoplasmic protein-tyrosine kinase that associates with the Fcγ receptor in various inflammatory cells. 104 Syk can couple immune-cell receptors to intracellular signaling pathways that regulate cellular responses to extracellular antigens and anti-gen-Ig complexes of particular importance to the initiation of inflammatory responses. 105 ITP patients have accelerated clearance of circulating IgG-coated platelets via Fcγ receptor-bearing macrophages in the spleen and liver. A pilot study found that the Syk inhibitor R788 restored platelet counts to ≥50% in adults with refractory ITP. 106 In addition, adverse events were gastrointestinal (diarrhea, nausea, emesis). 106 However, the progressive condition with this drug is unclear now.
Other New Agents
Trials of several drugs for the treatment of ITP are now underway. The list of new drugs/molecules and studies related to these drugs is included in Table 2. 24 , 74 , 77 , 78 , 89 , 90 ,100–103,107–116
New drugs of ITP.

Conclusion
ITP is an acquired hemorrhagic condition characterized by the accelerated clearance of platelets caused by antiplatelet autoantibodies such as anti-GP IIb/IIIa. The platelet count in peripheral blood is <100 × 10 9 /L. ITP can be classified into three types, namely, acute, subchronic, and persistent, based on disease duration. ITP in adults tends to be sub-chronic/persistent, relapsing, and very often, refractory to treatment. Conventional therapy includes corticosteroids, IVIg, splenectomy, and watch-and-wait. Initially, 70%-80% of patients respond to corticosteroids, and 10%-30% attain durable remission. Splenectomy is avoided in young children because of infection risk and the high prevalence of spontaneous resolution of ITP. Second-line treatments for ITP include immunosuppressive therapy (eg, rituximab). Third-line therapies include TRAs, such as romiplostim and eltrombopag. TRAs are associated with increased platelet counts and reductions in the number of bleeding events. TRAs are considered as a safe and an effective treatment for patients with chronic ITP at risk of bleeding after failure of first- or second-line therapies. Determination of a threshold minimum platelet count or specific age at which a typical patient with ITP should be treated is difficult. The goal of all treatment strategies for ITP is to achieve a platelet count that is associated with adequate hemostasis, rather than a normal platelet count. Therefore, if bleeding symptoms are not found, treatment may not be needed. Patients should be treated with platelet-enhancing agents if the platelet count is <30 × 10 9 /L and mucosal bleeding has started, although a threshold of 30 × 10 9 /L may not be suitable for children. Treatment may also be appropriate if follow-up cannot be assured, if there are concerns for bleeding due to high levels of activity, or if there is a need for procedures associated with bleeding risk.
New therapies and recommendations have emerged in the last decade. However, deciding who should be treated with which treatment option and for how long is not known. The decision to treat should be based on bleeding severity, bleeding risk, activity level, likely side effects of treatment, and patient preference. A flowchart detailing the management and therapeutic options for ITP is illustrated in Figure 3. It can provide guidance, but should not replace clinical judgment.2,10,11,75

Treatment algorithm for ITP.
Author Contributions
Conceived the concepts: SN. Wrote the first draft of the manuscript: SN. Developed the structure and arguments for the paper: SN. Made critical revisions: SN. The author reviewed and approved of the final manuscript.