
Abstract
The present paper presents a review of the literature examining the efficacy of eszopiclone for treating insomnia. The purpose of the paper was to evaluate both the statistical and clinical efficacy of eszopiclone for treating insomnia. Both subjective and objective assessments of insomnia were evaluated across various sleep variables. Additionally, the efficacy of eszopiclone for treating insomnia comorbid with other conditions (sleep disordered breathing, psychiatric diagnoses, peri/post-menopause, rheumatoid arthritis), transient insomnia, and across diverse samples (adults, older adults, and samples pooled by race) was reviewed. Finally, the impact of eszopiclone use on daytime functioning was examined.
Keywords
Introduction
Insomnia involves difficulty initiating and/or maintaining sleep, or nonrestorative sleep. 1 In addition to impaired nocturnal sleep, individuals diagnosed with insomnia experience impairments in daytime functioning. Insomnia can result from endogenous abnormalities in sleep (primary insomnia), it can co-occur with other conditions that also disrupt sleep (comorbid insomnia), or be symptomatic of other conditions (secondary insomnia). Regardless of the etiology, insomnia places a strain on society. Difficulty sleeping is a significant concern with almost two-thirds of the population complaining of poor sleep in general. 2 While 4% of the population report receiving a diagnosis of insomnia, only 2% report receiving treatment. Consequently, there is a need for efficacious approaches to treating insomnia. The traditional pharmaceutical approach to treating insomnia has been the use of benzodiazepines. Recently, nonbenzodiazepine agents have begun to replace benzodiazepines for the treatment of insomnia.
The present paper presents a review of the literature examining the efficacy of eszopiclone for treating insomnia. The purpose of the paper was to evaluate both the statistical and clinical efficacy of eszopiclone for treating insomnia. Both subjective and objective assessments of insomnia were evaluated across various sleep variables. Additionally, the efficacy of eszopiclone for treating insomnia comorbid with other conditions (sleep disordered breathing, psychiatric diagnoses, peri/post-menopause, rheumatoid arthritis), transient insomnia, and across diverse samples (adults, older adults, and samples pooled by race) was reviewed. Finally, the impact of eszopiclone use on daytime functioning was examined.
Eszopiclone
Eszopiclone (Lunesta®) is a short-acting, nonbenzodiazepine hypnotic agent that was approved by the Food and Drug Administration for the treatment of insomnia on December 15, 2004. Eszopiclone is a pyrrolopyrazine derivative of the cyclopyrrolone class. 3 Eszopiclone has a single chiral center with an (S)-configuration. 3 The chemical structure of eszopiclone is unrelated to pyrazolopyrimidines, imidazopyridines, benzodiazepines, barbiturates, or other drugs with known hypnotic properties. 3
Pharmacology and Pharmacokinetics
Pharmacology
The precise pharmacology, or mode of action, of Eszopiclone is unknown. Eszopiclone is hypothesized, however, to exert its effect by interacting with GABA-receptor complexes at binding domains that are close to, or coupled with, benzodiazepine receptors. Once eszopiclone binds to the GABA-receptor complex, chloride transmission increases, which, in turn, depresses the central nervous system, resulting in sedation. 4
Pharmacokinetics
The pharmacokinetics of eszopiclone have been studied in healthy subjects (adults and older adults) and those with hepatic or renal disease. In healthy participants, the pharmacokinetic profile was examined after single doses administered up to 7.5 mg and after once-daily administrations of 1, 3, and 6 mg for 7 days. 3
Absorption and Distribution
Eszopiclone is rapidly absorbed in healthy adults with time to peak absorption of approximately one hour. 5 Peak absorption was delayed by approximately one hour when eszopiclone was administered after a high fat/heavy meal, which may affect the drug's impact on sleep onset latency. 3 Eszopiclone is shown not to accumulate after sequential once-daily administrations. 6 The blood-to-plasma ratio for eszopiclone of less than one suggests no selective uptake by red blood cells. 3
Metabolism and Elimination
Metabolism of eszopiclone essentially occurs through oxidation and demethylation. The primary plasma metabolites do not significantly bind to the GABA receptors. 3 In vitro studies show that CYP3A4 and CYP2E1 enzymes are involved in the metabolism of eszopiclone. 3
Eszopiclone has a half-life (t1/2) of approximately six hours. 7 Less than 10 percent of eszopiclone is excreted as an unchanged drug in the urine. 3 Older adults (65+) have a prolonged elimination time of approximately nine hours 3 which has implications for dosing in older adults.
Indications and Dosage
Eszopiclone is indicated for individuals who experience adverse sleep onset latency and/or sleep maintenance insomnia. The recommended adult doses include 1 mg, 2 mg, and 3 mg oral tablets. The recommended starting dosage for adults (age 18-64) is 2 mg immediately before bedtime. Dosage can be raised to 3 mg if clinically indicated. 3 The 2 mg dose is recommended for older adults with sleep maintenance difficulties, while a 1 mg dose is recommended for older adults whose primary complaint is delayed sleep onset. 3 Due to the double systemic exposure in patients with severe hepatic impairment, the recommended starting dosage of eszopiclone in these patients is 1 mg per night. 3 Studies have shown that the 2 mg dose produces the most consistent improvements in sleep maintenance.8,9
Efficacy Research
Seventeen studies were examined in detail (concise summaries are presented in Table 1). Literature searches were conducted using ISI Web of Science, PsychInfo, and PubMed databases and included the search terms “eszopiclone”, “eszopiclone + efficacy”, “eszopiclone + adherence”, and “Lunesta”. Abstracts and articles published from June 2002 to December 2008 were reviewed. Clinical trials, secondary analyses, and conference abstracts are reported. Additionally, the most current product information was retrieved from the manufacturer Sepracor, Inc. When the data was available, the improvements in sleep are denoted in this paper by a “+” to indicate an increase or a “-” to indicate a decrease in the specific outcome.
Review of research studies.
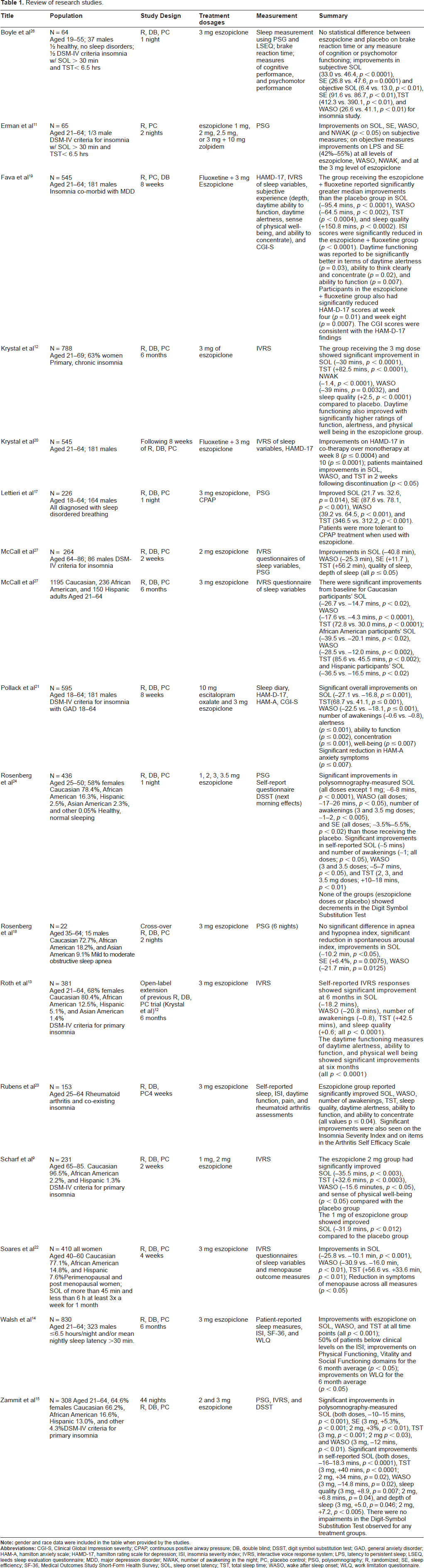
The majority of studies evaluate the efficacy of eszopiclone for treating adult participants diagnosed with primary insomnia.10–15 Additionally, outcomes were assessed in older adults.9,16 As insomnia often presents with other disorders, it was necessary to review studies that involved insomnia comorbid with other disorders such as individuals with sleep disordered breathing,17,18 psychiatric diagnoses,19–21 peri/post-menopausal women, 22 individuals with rheumatoid arthritis, 23 and transient insomnia. 24 Additionally, race has been found to be a potential mediator in the response to medications and may be driven by genetic differences, environmental differences (i.e. cultural and dietary habits), and fundamental differences in the pathogenesis of diseases. As a result, it was important to examine the effectiveness of eszopiclone in a sample pooled by race. 25
Sleep was primarily assessed using subjective measures, including self-report questionnaires, sleep diaries, and interactive voice response systems. Sleep was assessed objectively using polysomnography in seven of the reviewed studies.11,15–18,24,26 Polysomnography (PSG) is a recording of brain wave changes, eye movements, muscle tone, respiration, electrocardiogram, and leg movements during sleep. The sleep variables assessed by the studies included the time it takes to fall asleep (sleep onset latency; SOL), the number of times an individual awakens (number of awakenings; NWAK), the time spent awake during the night after initial sleep onset (wake time after sleep onset; WASO), the total time spent asleep (total sleep time; TST), and the efficiency of the sleep defined as a ratio of time spent sleeping to time spent in the bed (sleep efficiency; SE). In addition to the assessment of statistical significance, clinical significance was assessed using the criteria of clinically improved sleep consisting of less than 31 minutes of sleep onset latency and wake time after sleep onset and a sleep efficiency greater than 85% for older adults and 90% for adults. The efficacy of eszopiclone doses ranging from 1 to 3.5 mg were examined with the majority of studies employing the 3 mg dose. All clinical trials were funded by Sepracor, Inc.
Primary Insomnia
Non-Elderly Participants
In a randomized, double-blind, placebo-controlled study, the effects of 3 mg of eszopiclone versus placebo were examined with 788 adults ages 21-69 with primary, chronic insomnia over a two week period. 12 Interactive voice response systems indicated that the group receiving the 3 mg dose showed significant improvement in sleep onset latency (SOL; -30, p < 0.0001), total sleep time (TST; +82.5, p < 0.0001), number of awakenings (NWAK; -1.4, p < 0.0001), wake time after sleep onset (WASO; -39, p = 0.0032), and sleep quality (+2.5, p < 0.0001) compared to placebo. The results were also clinically significant with patients reporting less than 31 minutes of SOL or WASO following treatment. Daytime functioning also improved in the eszopiclone group relative to baseline with significantly higher ratings of function, alertness, and physical wellbeing.
Zammit and colleagues 15 conducted a randomized, double-blind, placebo-controlled study examining the effects of 2 mg, 3 mg, or placebo using polysomnography (PSG) and patient reports. 308 participants with chronic primary insomnia (ages 21-64) received treatment for 44 consecutive nights followed by two nights of single-blind placebo. Participants treated with eszopiclone showed significant improvements in polysomnography-measured mean SOL (2 mg, -10, 3 mg, -15, both doses p < 0.001), SE (3 mg, +5.3%, p < 0.001; 2 mg, +3%, p < 0.01), TST (3 mg, p < 0.001; 2 mg p < 0.03), and WASO (3 mg, -12, p < 0.01). Self-reported sleep also showed significant improvements in mean SOL (3 mg, -13.9, 2 mg, -10.4, both doses p < 0.0001), TST (3 mg, +48, p < 0.0001; 2 mg, +18, p = 0.02), WASO (3 mg, -7.9, p = 0.02), sleep quality (3 mg, +6.4, p = 0.007; 2 mg, +5.4, p = 0.04), and depth of sleep (3 mg, +5.2, p = 0.046; 2 mg, +7.3, p < 0.005). Although statistically significant, both the 2 and 3 mg doses did not result in significant clinical improvement overall. Participants did see a reduction in polysomnography-measured SOL below 31 minutes for both doses, but WASO and SE for both polysomnography and self-report measures did not meet criteria for clinically significant improvement. Daytime functioning was assessed using the Digit-Symbol Substitution Test and a self report measure of daytime alertness and ability to function. There were no impairments in the Digit-Symbol Substitution Test observed for any treatment groups. There were no significant differences in average self-reported daytime functioning between those receiving the placebo and the treatment groups.
Roth and colleagues 13 assessed the efficacy of eszopiclone to treat primary insomnia during the six months following a six-month double-blind eszopiclone study. 12 381 participants completed the study (ages 21-64). Sleep was assessed using an interactive voice response system. Participants who were previously treated with placebo in the Krystal and colleagues 12 study, showed rapid improvements in sleep compared to their baseline at the end of the previous study when treated with 3 mg of eszopiclone. At six months, participants showed improved SOL (-18.2), WASO (-20.8), number of awakenings (-0.8), TST (+42.5), and sleep quality (+0.6; all p < 0.0001). Participants showed clinically significant improvement in WASO (less than 31 minutes) but not for SOL. The daytime functioning measures of daytime alertness, ability to function, and physical wellbeing also all showed significant improvements at six months (all p < 0.0001).
A study by Walsh and colleagues 14 provides the first double-blind, placebo-controlled clinical trial of pharmacotherapy for insomnia to demonstrate improvements in quality of life, reduced limitations at work, and global insomnia severity. 548 participants (212 male), ranging in age from 21-64, received 3 mg of eszopiclone and 280 (111 male) received placebo. Six months of eszopiclone treatment at 3 mg resulted in significant improvements from baseline versus placebo on self-report measures of SOL, WASO, and TST for six months (all p < 0.0001). Insomnia Severity Index scores were significantly better than placebo at one, three, and six months (p < 0.0001, with high effect sizes, ~0.8). In addition to statistically significant improvements in sleep, the results indicate the participants reported clinically significant improvement in their sleep with median SOL and WASO less than 31 minutes at all time points. There were also significant improvements in daytime symptoms based on the Epworth Sleepiness Scale and Fatigue Severity Index with small to medium effect sizes (0.22-0.36) at all time points. Compared to placebo, there were mixed improvements in daily functioning, assessed using the Work Limitations Questionnaire, with small effect sizes. Improvements did not tend to hold for all six months of the study. Health outcomes were measured using the Medical Outcomes Study Short-Form Health Survey (SF-36). There were significant improvements (all at p < 0.05) in the domains of Vitality, Social Functioning, Physical Functioning, Bodily Pain, and the Mental Health component compared to placebo. However, these improvements had small effect sizes and were not consistent at all time points. The study indicates that there is potential for short lived benefits following discontinuation of the medication; however, the extent of this effect is not well known based on the findings.
A study by Erman and colleagues 11 reports the results of a randomized placebo controlled crossover study of eszopiclone to determine the effect on polysomnography. The study compared placebo, 1, 2, 2.5, or 3 mg of eszopiclone to 10 mg of zolpidem, a non-benzodiazepine sleep medication, among 65 individuals (aged 21-64; 1/3 male) with primary insomnia. On polysomnographic measurement, significant (p < 0.05 for all) improvements compared to placebo were observed in all treatment groups for latency to persistent sleep (LPS; 13.1-16.8) and SE (42%-55% improvement). Significant improvements for PSG measured WASO and NWAK were only seen in the 2.5 mg and 3 mg eszopiclone groups (p < 0.05). These improvements were also significant compared to 1 mg eszopiclone. Zolpidem showed a significant improvement in SE compared to placebo and to 1 mg of eszopiclone. However, for WASO there was no significant improvement compared to placebo and 1 mg of eszopiclone. Patient-reported measures of SOL, TST, WASO, NWAK, quality of sleep, and depth of sleep improved significantly (all p < 0.05) compared to placebo at 2 mg and 3 mg doses. Zolpidem also showed a significant improvement compared to placebo on all measures (SOL, TST, WASO, NWAK, quality of sleep and depth of sleep). The results showed that in addition to statistical significance, the participants treated with eszopiclone experienced clinically significant improvement in the median SOL for all doses, WASO for all doses except 1 mg, and SE for the 2.5 and 3 mg dose.
Boyle and colleagues 26 conducted two cross-over, randomized, placebo-controlled studies of healthy volunteers and patients with primary insomnia and assessed performance on driving skill, cognitive, and psychomotor tasks. 32 individuals in each study (between the ages of 19-55, total 37 males) were administered 3 mg of eszopiclone for a single night and tasks were completed in the morning following approximately 10 hours of sleep. In the study of healthy volunteers, subjective sleep measurement was obtained using the Leeds Sleep Evaluation Questionnaire, a visual analogue scale where 50 was equal to no improvement, and objective measurement of sleep was obtained using polysomnography. The healthy volunteers receiving eszopiclone improved significantly (p < 0.0001) compared to placebo on measures of ease of getting to sleep (34.4 vs. 45.5) and quality of sleep (34.7 vs. 48.0). There were no significant changes on measures of ease of awakening from sleep and behaviour after waking. In the insomnia study, significant improvements (p < 0.0001) were made on subjective measures of ease of getting to sleep (33.0 vs. 46.4) and quality of sleep (26.8 vs. 47.6). There were no significant difference on ease of wakening and behavior after waking. Objective measures of sleep improved significantly (p < 0.01) compared to placebo on measures of SOL (6.39 vs. 12.95), WASO (26.61 vs. 41.09), TST (412.26 vs. 390.07), and SE (91.6 vs. 86.67). In both studies, measures of driving ability, cognitive performance, and psychomotor functioning were not impaired in comparison to the placebo group. The study suggests that daytime functioning is not significantly impaired by eszopiclone and, specifically, driving behaviour remains un-impaired despite eszopiclone use.
In summary, the majority of studies examining the efficacy of eszopiclone for treating primary insomnia in adults found statistically significant improvement in sleep as measured by both polysomnography and self-report measures. Statistically significant improvement was seen for SOL, WASO, TST, SE, and sleep quality for all studies assessing these variables. Eszopiclone appeared less efficacious in reducing the number of awakenings; only three of the six studies reviewed showed improvement. Interestingly, in terms of clinical significance, the results are mixed. Clinically significant improvement in SOL was seen for some11,12,14,15 but not all studies 13 while WASO showed improvement for some11–14 but not all studies. 15 In addition to assessing sleep, the majority of studies examined the effects of eszopiclone on daytime functioning. Functioning was typically assessed using one or two items. Some studies showed improvement on daytime functioning variables such as self-report ratings of alertness.12,13 Other studies did not demonstrate improved daytime functioning but rather, lack of impaired daytime functioning.15,26 One study, examined multiple components of daytime functioning including sleepiness, fatigue, health outcomes, and work limitations. 14 Overall, while improvement was seen for daytime sleepiness and fatigue, the effect sizes for health outcomes were small and not consistent over time.
Older Adults
A randomized, double-blind, placebo-controlled, multi-centered study was conducted by Scharf and colleagues. 9 231 participants (ages 65-85) with primary insomnia received 1 mg, 2 mg, or a placebo over a two week period. Self-report measures obtained using an interactive voice response system indicated that the eszopiclone 2 mg group had significantly improved SOL (-35.5, p < 0.003), TST (+32.6, p < 0.0003), WASO (-15.6, p < 0.05), and sense of physical well-being (p < 0.05) compared with the placebo group. The group receiving 1 mg of eszopiclone showed improved SOL (-31.9, p < 0.012) compared to the placebo group. Both the 1 and 2 mg treatment groups did not report clinically significant improvement in their sleep (SOL and WASO was greater than 31 minutes on average).
McCall and colleagues 16 conducted a randomized double-blind, placebo controlled study of the effects of eszopiclone among older adults, aged 64-86, with primary insomnia. 264 participants (86 males) were randomized to two weeks of 2 mg of eszopiclone or placebo. Eszopiclone was predictive of improvements from baseline on polysomnographic measurement of latency to persistent sleep (-40.8), WASO (-25.3), SE (+11.7%), and TST (+56.2) compared to placebo (all p < 0.05). Improvements were also made in subjective self-report measures of SOL (-40.8), WASO (-31.3), and TST (48.6), as well as quality and depth of sleep, and the overall Insomnia Severity Index score (all p < 0.05). In general, the results indicate that there was no clinically significant improvement in sleep. PSG measured SOL was clinically improved (less than 31 minutes) but subjectively measured SOL, both PSG and subjectively measured WASO, and SE were not clinically significant. There were no significant differences on measures of daytime functioning, including ability to function, daytime alertness, and sense of wellbeing between the eszopiclone and placebo groups. While eszopiclone did not result in any significant daytime impairments, neither did it result in any significant improvements.
Insomnia Concomitant with other Conditions
Sleep Disordered Breathing
Discomfort and difficulty initiating sleep is often associated with the use of continuous positive airway pressure (CPAP) and can result in reduced quality of clinical sleep studies and reduced compliance to CPAP treatment. Hypnotics are generally not recommended for this population as they generally result in respiratory depression. However newer, non-benzodiazepine medication, offers the possibility for improved study quality and improved CPAP compliance. The following two studies reviewed eszopiclone for these uses.
In a cross-over, randomized, double-blind, placebo-controlled study by Rosenberg and colleagues, 18 3 mg of eszopiclone was administered to 22 individuals (15 males) with mild to moderate obstructive sleep apnea (aged 35-64). Participants underwent six nights of polysomnographic recording. There were significant improvements (p < 0.05) in the number of spontaneous arousals, the time from lights out to the start of the first consecutive ten minutes of sleep (latency to persistent sleep, LPS; -10.2 min), SE (+6.4%), TST (+29.9 min), and WASO (-21.7 min) but no significant effect on NWAK. There was clinically significant improvement for average SOL (less than 31 minutes) but not WASO or SE. The use of eszopiclone did not significantly worsen apnea or hypopnea.
Lettieri and colleagues 17 conducted a double-blind, placebo-controlled study of the effects of administering eszopiclone to participants prior to undergoing a sleep study. The researchers were interested in whether the administration of eszopiclone could improve sleep duration and continuity during a polysomnography study. The sample included individuals ranging from 18-64 years old who met criteria for sleep disordered breathing. 226 individuals (164 males) were randomized to 3 mg of eszopiclone or placebo 60 minutes prior to undergoing one of three nights of polysomnography: diagnostic, split-night, or CPAP titration. Eszopiclone resulted in statistically significantly (p < 0.05) larger improvements compared to placebo regardless of type of polysomnography on SOL (-21.7 vs. 32.6), SE (87.6 vs. 78.1), WASO (39.2 vs. 64.5), and TST (346.5 vs. 312.2). Clinically significant improvements were seen for SOL (less than 31 minutes) but not for WASO or SE. Eszopiclone did not significantly affect apnea-hypopnea index scores compared to placebo.
Psychiatric Diagnoses Depression
Fava and colleagues 19 conducted a randomized, double-blind, placebo-controlled, parallel-group study examining the efficacy of fluoxetine + eszopiclone versus placebo + eszopiclone in treating insomnia and depression. 545 participants aged 21-64 were enrolled in the 8 week study. The participants met the criteria for both DSM-IV major depressive disorder and insomnia. Participants were started on a 20 mg dose of fluoxetine hydrochloride and a 3 mg dose of eszopiclone. At week four, investigators had the option of titrating the fluoxetine daily dose from 20 to 40 mg depending on the participant's symptoms. Sleep and daytime functioning were assessed using an interactive voice response system and the Insomnia Severity index. Depression was assessed using the 17-item Hamilton Rating Scale for Depression (HAM-D-17) and the Clinical Global Impression Severity (CGI-S) and Symptom Improvement (CGI-I) items. The group receiving the eszopiclone + fluoxetine reported significantly greater median improvements than the placebo + fluoxetine group in SOL (-95.43, p < 0.0001), WASO (-64.5, p < 0.002), TST (p < 0.0004), and sleep quality (+150.8, p < 0.0002). The results were clinically significant for SOL and WASO (median less than 31 minutes). The Insomnia Severity Index scores were significantly reduced in the eszopiclone + fluoxetine versus the placebo + fluoxetine group (p < 0.0001). Daytime functioning was reported to be significantly better in terms of daytime alertness (p = 0.03), ability to think clearly and concentrate (p = 0.02), and ability to function (p = 0.007). Participants in the eszopiclone + fluoxetine group also had significantly reduced HAM-D-17 scores at week four (p = 0.01) and week eight (p = 0.0007). The CGI scores were consistent with the HAM-D-17 findings.
An article by Krystal and colleagues 20 was a follow-up to a previous randomized placebo controlled study of eszopiclone and fluoxetine for 545 patients (aged 21-64; 181 males) with DSM-IV diagnoses of insomnia and major depressive disorder. Following 8 weeks of 3 mg eszopiclone and fluoxetine or placebo and fluoxetine, patients continued to receive fluoxetine and complete sleep measures. Two weeks after discontinuation of eszopiclone, patients maintained improvements in SOL, WASO and TST (p < 0.05). Significantly more improved scores were observed between the cotherapy and monotherapy groups on the Hamilton Depression Rating Scale (p < 0.0001). This study suggests that improvements in sleep with eszopiclone are maintained after discontinuation of medication and may provide a particular benefit to individuals with co-morbid major depression.
Anxiety
A study by Pollack and colleagues 21 represents the first double-blind, placebo controlled study investigating the effects of pharmacotherapy for individuals diagnosed with insomnia and generalized anxiety disorder who are treated with an SSRI. All participants met DSM-IV criteria for general anxiety disorder and insomnia. 595 individuals (196 male) ranging in age from 18-64 were randomized to treatment with eszopiclone and escitolpram oxalate (an SSRI used for the treatment of anxiety and depression) or placebo and escitolpram oxalate. Participants completed self-report sleep and quality of life questionnaires throughout the study and the Hamilton Anxiety Scale, the Hamilton Depression Rating Scale, Clinical Global Impression of Improvement scales, Insomnia Severity Index, Hospital Anxiety and Depression Scale, Quality of Life Enjoyment Satisfaction Questionnaire, and the Sheehan Disability Scale at weeks 1, 2, 4, 6, 8, and 10. Cotherapy resulted in significant improvements from baseline compared to placebo and escitolpram on SOL, TST, WASO, number of awakenings, daytime alertness, ability to function, and ability to concentrate at all time points between baseline and the termination of treatment at week eight (all p < 0.05). At termination of active treatment, cotherapy compared to placebo plus escitolpram resulted in improvement from baseline of: SOL (-27.1 vs. -16.8), TST (68.7 vs. 41.1), WASO (-22.5 vs -18.1), and number of awakenings (-0.6 vs. -0.8). Two weeks following active treatment, there were no longer any significant improvements on these variables. Clinically significant improvement in SOL (less than 31 minutes) was seen for SOL at weeks 6 and 8 and for WASO at weeks 1, 2, 4, 6, 8, and 10. Improvements were reported on the Hamilton Anxiety Scale at all measurement points (all p < 0.05), and improvements were made on the Clinical Global Impressions of Improvement at all measurement points between weeks 1 and 8 (p < 0.05). Improvements were made on the Hamilton Depression Rating Scale (sleep items excluded) 4, 6, and 8 (p < 0.05). There were no significant improvements on the Quality of Life Enjoyment Satisfaction Questionnaire, the Clinical Global Impression of Severity of Illness Score, and the Sheehan Disability Scale. This study indicated that co-therapy of eszopiclone and escitolpram oxalate may enhance improvements on measures of anxiety.
Menopausal Transition
A study by Soares and colleagues 22 involved a double-blind, placebo controlled study of the use of eszopiclone among peri and post-menopausal women. 410 women ranging in age from 40-60 with insomnia were randomly assigned to 3 weeks of 3 mg eszopiclone or placebo. There were significant (all p < 0.01) average improvements compared to placebo on SOL (-25.8 vs. -10.1), WASO (-30.9 vs. -16.0), and TST (+56.6 vs. +33.6). There were clinically significant improvements in WASO (less than 31 minutes). Significant improvements were also observed on self-report measures of sleep quality, sleep depth, daytime alertness, ability to function, ability to concentrate, and physical well being (p < 0.05). The eszopiclone group reported fewer awakenings due to hot flushes, greater improvement on the Montgomery Asberg Depression Rating Scale scores (p < 0.05), and physician global assessments of menopause scores (p < 0.001). Eszopiclone also resulted in improvements on the total Greene Climacteric Scale score and the vasomotor and psychological subscores, vasomotor and physical domains of the menopause-specific questionnaire, and family life/home domain of the Sheehan Disability Scale (all p < 0.05).
Rheumatoid Arthritis
An abstract presented by Rubens and colleagues 23 involved a randomized, double-blind, placebo-controlled study with patients (25-64 years) diagnosed with rheumatoid arthritis and co-existing insomnia. 153 participants were randomized to receive eszopiclone 3 mg or placebo treatment for four weeks. The group receiving eszopiclone self-reported significantly improved SOL, WASO, NWAK, TST, sleep quality, daytime alertness, ability to function, and ability to concentrate (all values p < 0.04). Significant improvements were also seen on the Insomnia Severity Index and on items in the Arthritis Self Efficacy Scale.
Transient Insomnia
Rosenberg and colleagues 24 conducted a randomized, double-blind, placebo-controlled study assessing the effects of 1, 2, 3, 3.5 mg eszopiclone or placebo on transient insomnia. 436 healthy, normal sleeping participants between the ages of 25 and 50 years of age were recruited into the study from multiple centers. Transient insomnia was induced via the ‘first night effect’ of testing in a sleep laboratory. The efficacy of treatment and next morning effects was assessed using polysomnography, self-report, and the Digit Symbol Substitution Test. Using polysomnography, participants receiving the eszopiclone had significantly less SOL (all doses except 1 mg; ~6-8, p < 0.0001), less WASO (all doses; ~17-26, p < 0.05), fewer number of awakenings (3 and 3.5 mg doses; ~1-2, p < 0.005), and greater SE (all doses; ~3.5%-5.5%, p < 0.02) than those receiving the placebo. SOL, WASO, and SE did not meet clinical criteria for insomnia (greater than 31 minutes of SOL and WASO or SE less than 90%). Self-reported sleep was assessed using a morning questionnaire. Participants receiving eszopiclone reported significantly less SOL (-5) and fewer number of awakenings (all doses; -1, p < 0.05), less WASO (3 and 3.5 doses; -5-7, p < 0.05), and increased TST (2, 3, and 3.5 mg doses; +10-18, p < 0.01). SOL and WASO also not meet clinical criteria for insomnia for self-report measures. None of the groups (eszopiclone doses or placebo) showed decrements in the Digit Symbol Substitution Test.
Racial Comparisons
McCall and colleagues 25 examined the efficacy of 3 mg of eszopiclone for treating primary insomnia in Caucasian, African American, and Hispanic samples over six months. The study was an extension of an earlier six month trial. The study design was randomized, double-blind, placebo-controlled involving 1195 Caucasian, 236 African American, and 150 Hispanic adults aged 21-64 years. Sleep was assessed using an interactive voice response system. There were significant improvements from baseline for Caucasian participants’ SOL (-26.7 vs. -14.7, p < 0.02), WASO (-17.6 vs. -4.3, p < 0.0001), TST (72.8 vs. 30.0, p < 0.0001); African American participants’ SOL (-39.5 vs. -20.1,p < 0.02), WASO (-28.5 vs. -12.0, p < 0.002), TST (85.6 vs. 45.5, p < 0.002); and Hispanic participants’ SOL (-36.5 vs. -16.5, p < 0.02). Only the WASO for Caucasian and Hispanic participants met the criteria for clinical significance (less than 31 minutes of wake time).
Discussion of Efficacy Studies
Positive sleep outcomes were associated with eszopiclone use in the majority of reviewed studies. However, the magnitude of the improvement in sleep varied. Greatest improvements were seen for SOL, WASO, and TST with fewer studies showing improvements in the number of awakenings. Improvements were seen for both subjectively and objectively measured sleep although not necessarily for the same sleep variables. The majority of studies (14 out of 17) relied on subjective reports while 7 used objective measures. Additionally, while statistically significant improvement in sleep was seen for the majority of studies, clinically significant improvement was not as pervasive. Of the 14 studies where clinical significance could be derived, only 8 demonstrated clinically significant improvements in SOL and WASO and only 1 out of 4 studies showed clinically improved sleep efficiency (greater than 90% for adults and 85% for older adults).
Next day functioning was assessed in the majority of the studies, typically through the use of one to two items assessing self-reported daytime functioning on a likert scale. Consequently, there were few objective measures of daytime functioning and the measures used were limited in scope. The majority of studies assessing self-reported daytime functioning showed small improvements in daytime functioning compared to placebo but these improvements were not consistent over time. The objective assessments of daytime functioning (e.g. the Digit Symbol Substitution Test) assessed one facet of daytime functioning and indicated no increased impairment of functioning but did not show improvement of functioning.
The length of studies varied, ranging from a minimal data collection period of one night to a period of six months. The majority of studies used a 3 mg dose of eszopiclone, one used 2 mg, and four studies compared various doses. In the studies comparing various dose levels, the 1 mg dose was generally found to be less effective than higher doses.9,11,15,24 Both 1 and 2 mg doses were used in studies involving older adults. More improvement was seen across various sleep variables for the 2 mg dose compared to the 1 mg dose. Interestingly, although the older adult sample showed statistically significantly improved sleep, there was little clinically significant improvement. For participants experiencing sleep disordered breathing, Rosenberg and colleagues 18 found that the use of eszopiclone did not worsen apnea or hypopnea and was safe to use among this population during polysomnographic studies. However, more research is needed with larger samples in order to conclude that eszopiclone is safe among low and moderate obstructive sleep apnea individuals and to determine whether it could be used among severe cases with obstructive sleep apnea. Additionally, eszopiclone was found to not significantly affect apnea-hypopnea index scores compared to placebo and according to Lettieri and colleagues, 17 resulted in more usable and better quality polysomnographic recordings. Studies examining the use of eszopiclone for insomnia comorbid with psychiatric diagnoses saw improved sleep/mood scores for individuals diagnosed with major depressive disorder19,20 or generalized anxiety disorder. 21 Additionally, peri and postmenopausal women 22 and patients diagnosed with rheumatoid arthritis 23 saw improved sleep and symptoms when treated with 3 mg of eszopiclone. In addition to the treatment of primary insomnia, eszopiclone was shown to be efficacious in the treatment of transient insomnia. 24 Finally, while the majority of studies did not report culturally-specific data, one study found similar improvements in sleep with eszopiclone for Caucasian and African American adults while Hispanic participants experienced comparably less widespread improvement. 25
Safety and Tolerability
Adverse Events
Common adverse events associated with eszopiclone use have been reported to be mild in nature and include: unpleasant taste, headache, dry mouth, somnolence, and dizziness (see Table 2):12,27 A six month study of a nightly 3 mg dosage reported serious adverse events occurred in less than 1% of the eszopiclone group and included gastrointestinal disorder and chest pain. 12 More serious adverse events seem to be very rare but a case study reported hallucinations when an individual was unable to obtain eight or more hours of sleep before becoming active. 28
Safety and tolerability.

A possible link has been identified between sleep medications and depression, in general, and specifically with eszopiclone and depression. An analysis of reports published by the FDA indicates that 32 of the 802 individuals administered eszopiclone, developed depression according to DSM-IV criteria. 29 These findings contrast with results from placebo use, where 3 out of 294 individuals developed insomnia.
Adverse events reported to poison control centers in the state of Texas include drowsiness/lethargy among 46.7% of the reported cases, and less than 5% for all of the following: agitation/irritability, ataxia, tachycardia, slurred speech, hyperglycemia, confusion, dizziness/vertigo, lacrimation, nausea, respiratory depression, throat irritation, and vomiting. 30 At exceptionally high levels (30 times standard dosing), overdose prolonged coma may occur. This was reported in a case report of an elderly woman who intentionally overdosed and fell from a two-story window (empty bottles of amitriptyline/perphenazine were also found. 31
Concerns have arisen regarding a potential link between the use of hypnotic medication and subsequent development of cancer. Significantly higher rates of skin cancer and tumors of unknown malignancy have been reported in studies of eszopiclone, zaleplon, ramelteon, and zolpidem compared to placebo. 32 The product packaging reports rat studies in which thyroid gland follicular cell adenomas and carcinomas developed at a dose of 100 mg/kg/day. 3 However, other rat studies have not found increases in tumors.
Drug Interactions
Interactions may occur with substances that affect the major metabolic pathway for the elimination of eszopiclone (CYP3A4) and increase or decrease the effects of eszopiclone. When the potent CYP3A4 inhibitor, ketoconazole, was coadministered with eszopiclone there was a 2.2 increase in the area under the curve. 3 Despite the lack of data, other systemic azole antifungals that inhibit the CYP3A4 pathway (traconazole, fluconazole, voriconazole, and IV miconazole) may increase the effects of eszopiclone. Special consideration should be taken when prescribing eszopiclone to individuals who may be taking these medications. 33 Large meals or heavy meals may also be a concern since they may reduce the effects of eszopiclone. 3
The combination of eszopiclone and any CNS depressant may pose a risk to the patient. Industry packaging reports that coadministration of eszopiclone and ethanol at 0.7 g/kg resulted in psychomotor impairment for up to 4 hours. 3 Particular care should be taken when providing any potentially dangerous medication, eszopiclone included, to patients with suicidal ideation, suicidal history, or major depressive disorder. When such co-ingestions with eszopiclone were reported to poison control centers they have most often been related to cases of attempted suicide (78.8%). 30 It should be noted that in events reported to poison control centers with co-ingestion (mean dosage of 36.9 mg) 18.8% of cases resulted in moderate to severe outcomes and no event resulted in death.
A cotherapy study of eszopiclone and the anti-depressant fluoxetine did not show any significant interaction and a non-significant number of CNS related adverse events were reported following discontinuation of the two medications. 20 The cotherapy of the anti-anxiety medication escitalopram oxalate also did not result in significantly more CNS adverse events. 21
Tolerance/Dependence
A lessening in the therapeutic effects of a drug following prolonged use (tachyphylaxis) is common with sleep medications following several weeks of use. No reports of tolerance to eszopiclone could be found in the current literature. Research has shown that the effects of eszopiclone are maintained at 2, 6, and 12 months without any symptoms of tolerance.12,13,19,20 Another major concern with pharmaceutical sleep aids is the worsening of insomnia following discontinuation of medication, known as rebound insomnia. 34 In the three studies where post-treatment effects were reported there was no evidence of rebound insomnia.20–22 Hallucinations, seizures, and perceptual disturbances are common adverse events of hypnotic withdrawal but no such events have been reported in association with eszopiclone in the literature. According to the manufacturer, the following uncomplicated sedative/hypnotic withdrawal (DSM-IV criteria) symptoms were reported during clinical trials following active medication discontinuation: anxiety, abnormal dreams, nausea, and upset stomach. 3 These events were all reported at 2% or less.
Patient-Focused Perspectives
Quality of Life
Based on the studies reviewed, eszopiclone has limited to no effect on reducing daytime functioning including cognitive performance, driving related skills, coordination, and subjective measures of concentration, alertness, and ability to function.12,19,26 Minor memory impairments and cognitive deficits are reported on the product labelling among samples of healthy and insomnia participants within nine hours of taking the medication. 3 Eszopiclone has been associated with predicted improvements in quality of life, work limitations, and productivity. 14
Patient Satisfaction/Acceptability
The range of adverse events associated with a specific medication may pose a serious threat to treatment adherence. The relatively benign range of adverse events associated with eszopiclone likely support higher rates of treatment adherence. Unpleasant taste has been frequently reported as a potentially hindering side effect of eszopiclone. There was a somewhat higher rate of discontinuation among eszopiclone participants than placebo in the studies reviewed; however the overall rates of adherence suggest that eszopiclone is generally acceptable among patients.11,17–19,21,22,26,27 Discontinuation due to adverse events ranged from 1%-9% among those receiving eszopiclone.
Economic Cost
A 30 day supply of eszopiclone currently (May, 2008) costs approximately $170, out-of-pocket without medication coverage, based on a sample of U.S. online retailers.35,36 When considering chronic insomnia this cost clearly increases. As of April 2007, a six month use of eszopiclone was estimated to cost US$ 497.15 per patient, which included drug cost, dispensing fee, physician visit and time loss to receive care. 37 Any cost analysis of insomnia treatment needs to take into account the costs to society and to the individual. Insomnia has been linked to negative effects on medical expenses, work absenteeism, productivity, quality of life, and memory.38–40 The use of a 3 mg prescription of eszopiclone that results in remitted insomnia symptoms is predicted to reduce overall health care costs and lost productivity.37,41 One researcher estimated net savings as $245.13 in healthcare costs and $184.19 in productivity per patient over six months (in 2006 dollars). Based on an estimated prevalence of 10% of the U.S. population having chronic insomnia, there are approximately 30.5 million people in the United States currently suffering from the condition.42,43 Not all insomnia will be responsive to eszopiclone and it may not be the most appropriate form of treatment for all patients.
No studies were found directly comparing eszopiclone to psychological interventions. Cognitive/behavioral interventions and pharmacological interventions have been shown to have nearly equivalent efficacy for the treatment of short-term insomnia although behavioral interventions showed greater improvement in sleep onset latency. 44 Fifty minutes of cognitive/behavioral treatment tends to cost $150 and will last 6 to 10 sessions. In the short run, the costs of cognitive/behavioral treatments exceed that of eszopiclone or any other sleep medication. 44 However, in chronic insomnia, there is likely both a financial and therapeutic advantage for cognitive/behavioral treatments over pharmacological approaches which are not recommended for of the treatment of longterm insomnia. Cognitive behavioral treatment often results in improvements in sleep that are maintained once therapy ceases. Conversely, there is a need for medication to be continued in order to maintain the therapeutic effects of the medication. 45
Conclusions
In summary, the review of the literature shows that, overall, eszopiclone is efficacious for the treatment of primary insomnia in adults, with insomnia comorbid with other disorders, and with specific populations. The small number of studies investigating the use of eszopiclone with disorders comorbid with insomnia or with specific populations prevents us from drawing broad conclusions from the results but, instead, present introductory findings that will hopefully lead to further research on these specific disorders/populations. While improvements in sleep were seen with eszopiclone use, the improvements are not uniform across all sleep variables and are not consistent across objective/subjective outcome measures. While many of the studies demonstrated statistically significant improvement in sleep, there was considerably less clinically significant improvement suggesting that many participants would continue to meet clinical criteria for insomnia following treatment with eszopiclone. In addition to nocturnal sleep complaints, impairment of daytime functioning is symptomatic of insomnia. The majority of studies used limited measures to assess daytime functioning and showed limited improvement or simply lack of impairment in daytime functioning. Further research that employs ecologically valid measures of daytime functioning is needed to determine if the use of eszopiclone results in improvements in the daytime symptoms of insomnia.
The review of the literature suggests that common adverse events associated with eszopiclone use have been mild in nature. No reports of tolerance associated with eszopiclone were found in the current literature. The length of the majority of studies ranged from two weeks to two months. Studies of longer duration are required in order to discern the development of tolerance, or rebound insomnia once eszopiclone is discontinued. Additionally, many individuals report suffering from insomnia for years (i.e. 20-50 years) and report using sleep medication for the long-term treatment of insomnia. Therefore, the research to date, does not address the benefits/costs of eszopiclone for treating insomnia that is long-term in nature. Finally, there is a dearth of studies comparing the use of eszopiclone with psychological interventions. Given the durability of psychotherapeutic effects, it would be helpful to examine the cost/benefits associated with eszopiclone use versus behavioral interventions over the long term.
Disclosure
The authors report no conflicts of interest.