
Abstract
Purpose
The purpose of this review was to summarize current treatment guidelines and recently published studies about the efficacy and safety of antihypertensive therapy in elderly patients.
Methods
A literature research (MEDLINE) was performed with respect to the prevalence of hypertension in the elderly, the underlying pathophysiological mechanisms and current treatment options.
Results
Hypertension affects up to 70% of the population aged 65 years and older and results in a significant increase of cardiovascular morbidity and mortality. Antihypertensive drug therapy reduces the risk of cardiovascular complication and end organ damage not only in younger, but also in elderly patients. The most frequently applied classes of antihypertensive medication are diuretics, beta-blockers, ACE-inhibitors, angiotensin II-AT1-receptor blockers, calcium channel blockers, alpha-adrenergic receptor antagonists, centrally acting drugs and vasodilators. Side effects of antihypertensive medication have to be considered especially in the vulnerable elderly patients. The recently published HYVET study added important information on the value of antihypertensive therapy in patients at an age of 80 years or older. In the treatment group with indapamide and periondopril (compared to the placebo group) the risk of stroke was reduced by 30%, all-cause mortality by 21% and cardiovascular mortality by 23%.
Conclusion
Co-morbidities and age related changes of pharmacokinetics and pharmacodynamics require a very distinct choice of therapy in elderly people. Individual drug classes might be of advantage in certain conditions, including diabetes mellitus, renal dysfunction, heart failure and stroke.
Introduction
In the industrialized countries of the world life expectancy revealed a continuous increase during the last decades, which also results in an increase in age-associated diseases and disabilities. Epidemiological studies could demonstrate that hypertension, coronary heart disease, congestive heart failure, atrial fibrillation, and stroke all increase with increasing age. 1 Hypertension itself further enhances the risk for cardiovascular complications, stroke, cognitive decline and mortality.1,2 The manifestation of hypertension at an advanced age is due to complex biological changes in the vascular architecture and the neurohumoral system. 1 Degenerative mechanisms in the vessel wall lead to a dilatation of elastic arteries, an increase in intimal media thickness and in vascular wall stiffness, a decreased elastic artery compliance, and a rise in peripheral vascular resistance.1,3 These structural changes result in an increase in systolic and a decrease in diastolic blood pressure, the rise in pulse pressure is known as a further predictor for cardiovascular outcome.3,4 Diastolic blood pressure reflects the trend of arterial resistance, while systolic blood pressure is influenced by the left ventricular ejection fraction and the reflection of the sphygmic wave. As a consequence of the age-associated loss in elasticity of the aorta and the large arteries the capacity of the arterial wall to distend during the systolic phase decreases and results in an increase of systolic and pulse blood pressure. 4 In the elderly a high systolic and a low diastolic blood pressure value thus indicate a higher rigidity of the arterial wall, the increase in pulse blood pressure summarizes the adverse prognostic values of an elevated systolic and a low diastolic blood pressure.
Age related humoral changes further increase the risk for hypertension. Sympathetic system activity is higher, plasma renin activity reduced and salt sensitivity more pronounced at an advanced age. Because of the overall increase in the prevalence of overweight and obesity, insulin resistance and the metabolic syndrome enhance the risk for hypertension also in the elderly population.5,6
Hypertension affects 50%–70% of the population aged 65 years and older and about 80% of the population aged 80 years and older. 7 Although elderly with hypertension are known to have a significantly increased cardiovascular risk, they still continue to have poorer blood pressure control than younger people.8,9 The risk of stroke, coronary artery disease, heart failure and mortality is related to the level of blood pressure in a continuous fashion for values as low as 115/75 mm Hg as the optimal blood pressure. In the Multiple Risk Factor Intervention Trial the risk of fatal stroke for those with systolic blood pressure over 180 mm Hg was about 15 times as high and the risk of fatal ischemic heart disease 7 times as high as the rates among those with optimal blood pressure. 10 The mortality risk is doubled for every 20 mm Hg rise in systolic blood pressure and 10 mm Hg rise in diastolic blood pressure from the level of 115/75 mm Hg. 11 This increase in the cardiovascular risk with increasing blood pressure values was found in all age groups, but the strength of the association seems to decline with increasing age.12,13 It is assumed, that an isolated increase in diastolic blood pressure, easily controllable by antihypertensive therapy, is of less prognostic values in elderly, compared to systolic hypertension, which indicates arterial stiffness. 4
Numerous studies could demonstrate that antihypertensive treatment reduces cardiovascular complications in the younger, and also in the elderly population.14–16 According to current treatment guidelines,17–21 the goal of treatment of hypertension in the elderly is to lower blood pressure to less than 140/90 mm Hg and to less than 130/80 mm Hg in older patients with diabetes.17,18 Blood pressure goals are further determined by the level of proteinuria in those with renal disease. 22 The ESH-ESC Guidelines on management of hypertension emphasize that elderly patients benefit from antihypertensive therapy in terms of reduced cardiovascular morbidity and mortality. 21 The effect of a tight control of systolic hypertension with a treatment target < 130 mm Hg compared to systolic blood pressure targets of <140 mm Hg was studied in the Cardio-Sis trial in patients with a mean age of 67 ± 7 years. 23 After two years the risk of cardiovascular events and death from any cause was significantly lower in the tight treatment arm, while side- effects revealed no difference between the two treatment groups. The Cardio-Sis trial thus underlines the importance of systolic blood pressure control in the elderly.
Side-effects of antihypertensive medications and drug-drug interactions have to be considered in the therapeutic regimen especially in case of a vulnerable elderly patient. Pharmacokinetics and pharmacodynamics of antihypertensive drugs are altered during aging and the risk of adverse reactions increases. The decision to initiate blood pressure lowering drugs should be made on the basis of the absolute cardiovascular risk, which is mainly determined by aging itself.19–21
The most frequently applied classes of antihypertensive medication are diuretics, beta-blockers, angiotensin-converting enzyme (ACE)-inhibitors, angiotensin II-AT1-receptor blockers (ARBs), calcium channel blockers, alpha-adrenergic receptor antagonists, centrally acting drugs and vasodilators. Particularly the renal risk is of importance in the choice of the therapeutic regimen. Blood levels of potassium, sodium and creatinine should be monitored regularly. Most of the antihypertensive drugs predispose elderly to symptomatic orthostatic hypotension, syncope or falls. For elderly patients the treatment principle “star low, go slow” should therefore be considered also in the antihypertensive medication. 24
This review summarizes studies on the efficacy and safety of antihypertensive therapy in elderly patients and describes possible advantages of distinct substances for patients with diabetes mellitus, renal dysfunction, stroke and heart failure.
Therapeutic Options in Antihypertensive Therapy
Life-style recommendations
In patients with diagnosis of hypertension non-pharmacological interventions, including a low salt diet, exercise and reduced alcohol intake, should be recommended. The PREMIER trial evaluated the effect of three procedures in 810 participants with above optimal blood pressure and stage 1 hypertension. 25 Behavioral intervention according to established recommendations was compared to recommendations plus DASH (Dietary approaches to stop hypertension) diet and to an advice only procedure. 25 The age of the study population was around 50 years. After 6 months the prevalence of hypertension was 26% in the advice only group, 17% in the established recommendations and 12% in the established plus DASH diet group. Unfortunately, patients adherence to life-style recommendations is generally poor, and especially in elderly, these recommendations have to be adapted to the patients individual situation. The Trial of Nonpharmacological Interventions in the Elderly (TONE) study, which enrolled older patients with hypertension with systolic blood pressure less of than 145 mm Hg who were taking one antihypertensive medication, demonstrated that patients in the reduced sodium diet arm had a mean decrease in systolic blood pressure of 3.6 mm Hg compared to 0.8 mm Hg in the control arm. 26 A low sodium diet was associated with a reduction in the need for antihypertensive medication. However, because of age-associated changes in renal tubular and humoral function, the risk to develop hyponatremia is increased in the elderly, especially when the medications enhance salt loss. 27
Life-style recommendations include the maintenance of a healthy body weight to reduce the cardiovascular risk. It is widely assumed that body weight tends to increase with increasing age, peaks between the age of 50 and 59 years, and then decreases. The value of this observational data remains a matter of debate regarding the bias, that obese patients reveal a high premature mortality and a shorter life-expectancy, compared to non-obese patients with a significantly higher chance to reach an advanced age. 5 Studies on the effect of voluntary weight loss in the elderly are scarce, but suggest that even a small weight reduction may show beneficial effects on cardiovascular complications. 28 Because aging is associated with a progressive increase in abdominal fat with various negative health consequences, 29 weight loss should be focused on patients with visceral obesity. 6 Malnutrition and a loss of muscle mass as possible side-effects of an inadequate weight reduction program could be harmful in vulnerable geriatric patients. 30
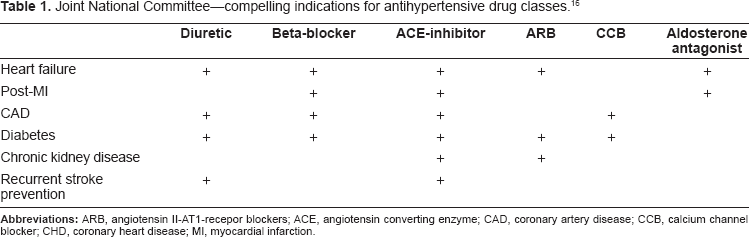
Joint National Committee–-compelling indications for antihypertensive drug classes. 16
Moderate aerobic exercise, such as walking, jogging, or swimming for 30 to 45 minutes three to four times per week, is generally recommended.30,31 Especially exercise programs have to be adapted to the function capabilities and comorbidities of the elderly patient. 32
Antihypertensive medication
In general, treatment guidelines for hypertension offer the best available recommendations for optimal therapy.18–21 The main reason for antihypertensive therapy is to reduce the burden of cardiovascular complications, end organ damage and renal failure. Comorbidities and age related changes of pharmacokinetics and pharmacodynamics require a very distinct choice of therapy in elderly patients. Various antihypertensive drugs differ with respect to their haemodynamic effects, fluid volume, sympathetic nervous system, renin-angiotensin-system, electrolytes and metabolic side-effects. Two or more drugs are often required to attain the recommended treatment targets. The combination of drugs with complementary mechanisms of action may not only improve blood pressure control, but also the tolerability of the medication because of the lower dosage of the single drugs. Antihypertensive treatment is highly efficacious in patients with systolic as well as diastolic hypertension.31,33,34
Diuretics
Randomized controlled trials could demonstrate that thiazide diuretics and long-acting dihydropyridine calcium channel blockers are the drugs of choice in the treatment of isolated systolic hypertension. 35 Diuretics were also applied in the recently published HYVET trial, which could clearly demonstrate the advantage and the safety of antihypertensive therapy in patients aged 80 years or older. The diuretic indapamide and the angiotensin converting enzyme inhibitor perindopril were used as antihypertensive medication. 31 More serious adverse events occured in the placebo compared to the active treatment arm. At the 1.8-year follow-up, a 30% reduction in fatal or nonfatal stroke, a 39% reduction in fatal stroke, a 21% reduction in all-cause mortality, a 23% reduction in death from cardiovascular causes, and a 64% reduction of heart failure could be observed in the active treatment group. The results of the HYVET trial are of great clinical importance especially with respect to the previously inconclusive data on the benefits of antihypertensive therapy in patients at an age of 80 years or older. Possible harmful effects of antihypertensive therapy in the elderly were extensively discussed, but could hardly be answered because many published studies about the efficacy of antihypertensive medication have either excluded the age group of 80 years or older or the elderly study population was too small to detect an advantage of active treatment. A formerly published meta-analysis about antihypertensive medication in patients of 80 years and older described a reduction in the risk of stroke of 36%, but also an increase in the risk of death from any cause of 14%. 36 The HYVET trial thus added very important data on the safety of antihypertensive therapy in patients at an age of 80 years or older. One limitation is, however, that the participants of the HYVET trial were rather healthy, the numbers of those reporting smoking, alcohol intake and with previous cardiovascular events were low. Patients with a serum creatinine value over 150 micromol/L were excluded from the study. 37
In the ALLHAT trial, which included 33357 participants with a mean age of 67 years, chlorthalidone was effective in reducing stroke and the combined cardiovascular end-point.
In the chlorthalidone group, compared to treatment with amlodipine and doxazosin, the occurrence of new-onset heart failure was found to be significantly reduced.38,39
Beta-blockers
According to the results of a Cochrane analysis, which included 13 trials with more than 90 000 participants, the available evidence does not support the use of beta-blockers as first-line drugs in the treatment of hypertension. 40 With respect to stroke prevention there seems to be a trend towards a worse outcome compared to calcium-channel blockers, ACE-inhibitors and thiazide diuretics. According to the latest NICE guidelines (National Institute for Health and Clinical Excellence, www.nice.org.uk/CG034) beta-blockers are therefore considered as third- to fourth-line agents in the treatment of hypertension.
The use of beta-blockers is still recommended for selected older patients with hypertension with concomitant conditions, especially CAD and heart failure, or in the context of combination therapy.17–19 The recently published SENIORS study investigated the effect of nebivolol, a beta-blocker with vasodilating effects on mortality and cardiovascular hospital admission in 2128 patients aged ≥70 years of age with heart failure. 41 Hypertension was diagnosed in 61.1% of the patients treated with nebivolol and in 62.3% of the control group. Mean duration of follow-up was 21 months. All cause mortality was 15.8% in the nebivolol and 18.1% in the control group, cardiovascular mortality and cardiovascular hospital admission were 28.6% in the nebivolol and 33% in the control group. The beneficial effects of nebivolol appeared after 6 months of treatment and continued to increase with longer treatment duration.
Despite these favourable effects of beta-blocker therapy, side effects, especially a worsening of peripheral vascular disease, airway obstruction and the reduction of heart rate, have to be considered in the treatment of the polymorbid elderly patient, but weighted against the benefits on survival in patients with CAD.
ACE-inhibitors and ARBs
Agents that inhibit the activity of the renin-aldosterone system have been shown to be effective in blood pressure lowering and especially in end organ protection. Younger people have a more active renin-angiotensin-system than older individuals, and the inhibition of the renin-angiotensin system might differ between younger and elderly patients. 42
A meta-analysis of ACE-inhibitors in patients with heart failure, however, demonstrated that treatment with an ACE-inhibitor reduces the mortality rate and the need for heart failure related hospitalization, 43 and the advantages of the therapy with ACE-inhibitors were comparable between patients older and younger than 60 years of age. The second Australian National Blood Pressure Study (ANBP2) with 6083 hypertensive patients aged 65–74 years could show superiority of treatment with ACE-inhibitors compared to diuretics in men. 44 The Heart Outcomes Prevention Evaluation, 45 Losartan Intervention for Endpoint Reduction in Hypertension Trial, 46 Prospective Randomized Enalapril Study Evaluating Regression of Ventricular Enlargement, 47 and Effects of Amlodipine and Lisinopril on Left Ventricular Mass and Diastolic Function 48 all demonstrated reduction of left ventricular hypertrophy in elderly people with systolic hypertension, which was more pronounced in the group treated with ACE-inhibitors or ARBs compared to beta-blockers and calcium channel blockers. The Study on Cognition and Prognosis in the Elderly found that treatment with candesartan resulted in a reduction of cardiovascular events of 64% in patients with no history of stroke. 49 Elderly patients with hypertension and a history of heart failure, left ventricular hypertrophy and ischemic heart disease should be treated with an ACE-inhibitor or ARB. 17 ARBs as a class of antihypertensive drugs introduced a few years ago, show similar efficacy in lowering blood pressure compared to other classes of antihypertensive agents, but reveal some benefits superior to other antihypertensive agents. 50 In the MOSES trial eprosartan was of advantage compared to nitrendipine in patients with established cerebrovascular disease. 51
Renin Antagonist (Aliskiren)
Direct renin inhibition offers a new concept in antihypertensive therapy. 52 Aliskiren is a non-peptide with high affinity for the active site on the renin molecule. In contrast to other antihypertensive drugs the plasma renin activity is effectively blocked by aliskiren. The safety of aliskiren was investigated in a study including 355 patients aged 65 years or older with systolic hypertension. 53 Treatment with aliskiren 75 mg, 150 mg and 300 mg was compared to lisinopril 10 mg. Blood pressure was significantly lowered in all groups, but more patients in the aliskiren arm could reach the treatment target.
Calcium channel blockers
Treatment with long-acting dihydropyridine calcium channel blockers is highly effective in reducing cardiovascular morbidity and mortality. 54 Calcium channel blockers are of benefit especially in elderly people with isolated systolic hypertension.36,55 Various calcium channel blockers were applied in different clinical trials (nitrendipine: Syst EUR; amlodipine: ALLHAT, ASCOT, PREVENT; extended release verapamil: CONVINCE). 55 Nifedipine acts by inhibiting the trans-membrane influx of calcium into cardiac and vascular smooth muscle cells and reveals predominantly vasodilatory effects on arteries. According to the JNC 7 long-acting dihydropyridine calcium channel blockers are not recommended if angina or blood pressure are not controlled by beta-blocker therapy alone, or when beta-blockers are contradicted. 19 The Systolic Hypertension in Europe Trial (Syst-Eur) with participants of 60 years or older investigated whether antihypertensive therapy of isolated systolic hypertension could reduce cardiovascular complications.35,54 Antihypertensive treatment was started with nitrendipine. Active antihypertensive therapy reduced the rate of stroke by 42% and all fatal and non-fatal cardiovascular complications by 31%.
Alpha-adrenergic receptor antagonists
In the ALLHAT trial treatment with the alpha-blocker doxazosine resulted in a higher risk of stroke and a higher rate of heart failure than in the chlorthalidone group. 38 Alpha-blockers are not recommended as first line antihypertensive substances. A recently published study demonstrated an increase in left ventricular diameter associated with doxazosine therapy. 56 Prior administration of diuretics could prevent the manifestation of heart failure. Doxazosine is added to the antihypertensive therapy in patients with resistant hypertension. 57 Alpha-blockers are not only used in antihypertensive therapy, but also for obstructive urinary symptoms. The administration has to be considered in the therapeutic regimen.
Centrally acting antihypertensive substances
The action of monoxidine and rilmenidine is mediated by imidazoline I1 receptors located in the ventrolateral medulla and results in a fall in adrenalin, noradrenalin and renin levels.58,59 The antihypertensive activity of these substances is caused by vasodilation and reduced peripheral vascular resistance. Side effects are sedation and dry mouth. For monoxidine and rilmenidine no rebound (withdrawl) phenomenon could be found, which was a problem in clonidine treatment. Moxonidine and rilmenidine are considered as preferable to classic alpha2-adrenoreceptor stimulants (clonidine, alpha-methyl-DOPA) because of their lower side-effects, which is due to a weak affinity for the alpha2-adrenoreceptor. Centrally acting antihypertensive substances are not recommended as first line antihypertensive therapeutics, also because no data are yet available from prospective long-term outcome studies.
Patients Preference and Place in Therapy
With respect to the antihypertensive treatment regimen clinical guidelines are adapted to co-morbidities and the occurrence of cardiovascular complications and end-organ lesion. Especially in elderly side-effects and drug interactions have to be carefully considered. No more than three antihypertensive drugs should be prescribed for octogenarians, and particular attention must be paid to the renal risk. Serum levels of potassium, sodium, and creatinine must be monitored regularly.
Diabetes mellitus
Hypertension affects up to 60% of all diabetic patients and increases the risk of diabetic macro- and microvascular late complications. In type 2 diabetes hypertension is typically part of the metabolic syndrome of insulin resistance, in type 1 diabetes hypertension occurs in the course of diabetic nephropathy. Many studies could clearly demonstrate that antihypertensive therapy is highly effective to reduce cardiovascular complications and microvascular disorders. Treatment target is a blood pressure values <130/80 mm Hg in all diabetic patients and <125/75 mm Hg in patients with nephropathy. Especially with respect to nephropathy ACE-inhibitors and ARBs were found to be of advantage. 60 Metabolic side-effects have to be considered during therapy with diuretics and beta-blockers.
Renal dysfunction
Renal damage is characterized on the basis of a reduction in glomerular filtration rate and by the presence of increased levels of urinary albumin excretion. 61 The lowering of blood pressure and urinary albumin excretion seems to slow the progression of an impaired kidney function. Especially for patients with type 2 diabetes, the documentation of a beneficial effect of antihypertensive treatment on kidney function is extremely high. 62 The Seventh Joint National Committee recommends a systolic blood pressure of less than 130 mm Hg for patients with chronic kidney disease and for diabetic patients. 19 A meta-analysis suggested that non-diabetic proteinuric patients might benefit from even lower systolic blood pressure values (110–119 mm Hg) with respect to the kidney function, 63 but this goal pertained only to patients younger than 60 years of age. Major clinical trials about the influence of antihypertensive therapy on kidney function have excluded patients older than 70 years.
In general antihypertensive regimens that inhibit the RAS seem to provide greater end-organ protection that other antihypertensive substances.22,64 The combination of ACE-inhibitors and ARBs in the COOPERATE study resulted in a better reduction of proteinuria and a lower progression rate to doubling of serum creatinine or end-stage renal disease than monotherapy. 65
Stroke
Hypertension is the most important controllable risk factor for stroke. There is a strong relationship between blood pressure values and stroke mortality above blood pressure values of 115/75 mm Hg. Blood pressure lowering is highly effective in the primary and secondary prevention for stroke. No so-called J-shaped relation could be demonstrated between blood pressure and stroke. 66 In the INVEST study with 22000 participants not the risk of stroke, but of myocardial infarction, rose progressively with a diastolic blood pressure below 70 mm Hg. 67 Because the heart is perfused primarily in during diastole, an intensive lowering of diastolic blood pressure could compromise cardiac perfusion. 67
Meta-analysis indicate, that blood pressure lowering itself, but not the classes of antihypertensive substances, are of primary importance in stroke prevention,14,15,34 but the results of various intervention trials suggest that distinct antihypertensive treatment regimens might be more favorable, especially in elderly patients. Thiazide therapy for any given fall in blood pressure were found to result in a better reduction of stroke risk than do beta-blockers as a class. 68 The Systolic Hypertension in the Elderly Study, SHEP, could demonstrate that chlorthalidone-based antihypertensive therapies significantly decreased the risk of stroke in elderly patients with isolated systolic hypertension. 69 Recently published studies, such as the LIFE and MOSES study, suggest benefits of ARB therapy in stroke prevention.50,51 In a meta-analysis including 26 trials with 200 000 patients antihypertensive drugs that raise angiotensin II concentrations were highly effective in stroke prevention. 70
During an acute stroke antihypertensive medication leading to a possible increase of intracranial blood pressure and thus treatment with vasodilators should be prevented.
Heart failure and coronary heart disease
Left-ventricular hypertrophy, heart failure and atrial fibrillation are complications of hypertension with a strong impact on stroke, cardiovascular morbidity and mortality. Antihypertensive therapy with diuretics, ACE-inihbitors, ARBs and beta-blockers are of advantage in heart failure patients.14,43,45–47 Therapeutic strategies that block the renin-aldosterone system might be more effective in preventing new-onset atrial fibrillation.71,72
Cognitive decline
Hypertension increases the risk of cognitive decline and dementia. Antihypertensive therapy could thus reduce the risk of cognitive decline, but various antihypertensive substances in different trials revealed controversial study results. In the Syst-Eur study the risk of dementia after the 8 years follow-up period was reduced for 55% in the nitrendipine group compared with placebo. 73 In the SCOPE 49 and SHEP trial 69 no differences in the cognitive state could be demonstrated between active treatment and control group.
Conclusion
The prevalence of hypertension increases with increasing age and is strongly related to cardiovascular complications and an enhanced mortality rate. Degenerative changes of the arterial wall result primarily in an increase of the systolic blood pressure. Numerous studies could demonstrate that antihypertensive therapy reduces the risk of cardiovascular events and stroke also in elderly patients. A recently published meta-analysis included 147 trials about the effectiveness of blood pressure lowering in patients with a mean age at entry between 57 and 67 years. 14 The central question of the meta-analysis was the definition of special effects of antihypertensive substances beyond the blood pressure lowering effect. Beta-blockers revealed a protective effect given shortly after a myocardial infarction and calcium channel blockers a minor additional effect in the prevention of stroke. For a given reduction in blood pressure all classes of blood pressure lowering drugs showed similar effects in reducing cardiovascular events and stroke.
According to current treatment guidelines first choice substances for blood pressure lowering are diuretics, ACE-inhibitors and Angiotensin II-AT1-receptor blockers (ARBs) and beta-blockers.18–21 Alpha-adrenergic agonists and vasodilators should be administered in form of a combination therapy and according to special indications. 74 Side-effects of antihypertensive medications and drug-drug interactions have to be considered in the therapeutic regimen especially in case of a vulnerable elderly patient. Particularly the renal risk is of importance in the choice of the therapeutic regimen, and blood levels of potassium, sodium and creatinine should be monitored regularly.
Further randomized clinical trials will have to determine whether new antihypertensive substances, such as renin antagonists, are of advantage to reduce end organ damage in elderly patients.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material