
Abstract
Keywords
Extensor tendon laceration is one of the most common industrial accidents among young manual workers, but it does not receive as much attention in the literature as flexor tendon injury. Treatment protocols available for extensor tendon rehabilitation are often complex and unsuited to young patients whose goal is early return to work, which poses a unique challenge for occupational therapists striving for evidence-based practice and excellence in clinical interventions.
Three clinical approaches to the rehabilitation of extensor tendon repairs are (1) immobilization (IM), (2) early passive motion (EPM), and (3) early active motion (EAM; Tang, 2006). IM is the oldest technique. It involves complete immobilization of the wrist at 40°–45° with the metacarpophalangeal joints (MCP) and interphalangeal joints (IP) at 0° for 3 wk in a splint (Miller, 1942). The potential risk of rupture of a newly repaired tendon treated with an IM protocol is reduced because the patient is neither mobilizing nor required to follow a precise home exercise program when the tendon is at its weakest. Because of its simplicity, IM is often recommended for noncompliant patients (Evans, 1995b). Although IM appears simple to implement, the rehabilitation that follows the immobilization period is frequently complicated by attenuation, extension lags on MCP movement, extrinsic tightness, and adhesions resulting in flexion loss (Newport, Blair, & Steyers, 1990). The complications require intensive therapy and additional treatment to correct (Crosby & Wehbe, 1999).
In the 1980s, EPM was promoted as best practice when it was discovered that passive, “protected” mobilization promoted the intrinsic healing capacity of tendons in experimental dog models (Gelberman et al., 1991; Gelberman, Woo, Lothringer, Akeson, & Amiel, 1982; Takai, Woo, Horibe, Tung, & Celberman, 1991). Evans (1986, 1989) published a controlled EPM treatment protocol that focused on the passive glide of the repaired extensor tendon by using the recoil of elastic bands of a dynamic extension splint. The splint also immobilized the wrist at 40°–45° extension, and the splint’s palmar block allowed full passive extension and maximum 40° active flexion at the MCP joint (Evans, 1986). Several researchers have compared IM with this type of EPM and reported that patients in the latter protocol had better functional outcomes and fewer problems with adhesions (Browne & Ribik, 1989; Chow, Dovelle, Thomes, Ho, & Saldana, 1989; Evans, 1989). Despite its popularity, some authors (Purcell, Eadie, Murugan, O’Donnell, & Lawless, 2000) were critical of the EPM protocol and its dynamic splint because of the rehabilitation regimen’s demanding nature and the cost and time required to fabricate the splint.
In the 1990s, researchers recommended EAM to enhance “gliding” of the healing tendon and reduce the potential for adhesions or tendon “bunching” (Crosby & Wehbe, 1999; Evans, 1995b; Newport, 1998). In clinical practice, the popular active motion premise has led to many labor-intensive and often complex treatment protocols (Newport, 1998). Sylaidis, Youatt, and Logan (1997) proposed a simplified EAM protocol using a splint that positions the wrist joints at 45° extension and MCP joints at 50° flexion. A palmar block on the splint prevents full active flexion but allows active extension of the IP joints of the digits. Patients performed active MCP extension with IP held in either extension or flexion from Day 1 postoperation.
Recovery of Zones V and VI extensor tendon injury of the hand is often plagued by MCP extension lags, extrinsic tightness, and adhesions that prohibit full composite flexion of the digits. Anatomically, Zone V is over the MCP joint and is generally distal to the juncturae tendinum, and Zone VI is over the dorsum of the hand, distal to the extensor retinaculum, and includes the juncturae (Kleinert & Verdan, 1983). Khandwala, Webb, Harris, Foster, and Elliot (2000) conducted a prospective randomized controlled trial (RCT) involving 100 patients with Zone V and VI injuries and compared an EAM blocking splint protocol with an EPM protocol using a dynamic extension splint. The EAM protocol used was similar to that of Sylaidis et al. (1997), except the blocking splint extended only to the middle of the proximal phalanx, leaving the IP free to move. Khandwala et al. (2000) concluded no difference existed in treatment outcomes between the EAM and EPM protocols. However, they advocated EAM as a superior protocol because of its easy-to-wear and less-effort-to-maintain palmar blocking splint. Four RCTs investigated postoperative rehabilitation outcomes for extensor tendon injury in the literature (Bulstrode, Burr, Pratt, & Grobbelaar, 2005; Chester, Beale, Beveridge, Nancarrow, & Titley, 2002; Khandwala et al., 2000; Mowlavi, Burns, & Brown, 2005), but none compared the three accepted clinical approaches (IM, EPM and EAM) together and established the best practice among them.
In this pilot study, we compared the effectiveness of IM developed by Evans (1995b) on the basis of Miller’s (1942) techniques, EPM using a dynamic extension splint (Evans, 1986, 1989), and EAM using a palmar blocking splint (Khandwala et al., 2000) in the management of patients with acute extensor tendon repairs in Zones V and VI. The hypothesis was that the three rehabilitation protocols would have different treatment effects on patients. The findings would contribute to the postoperative management of extensor tendon injuries by occupational therapists.
Method
Patient Recruitment
We estimated the sample size needed for this pilot study on the basis of the primary outcome measure, total active motion (TAM). We estimated that the standard deviation of the TAM was 150° in extensor tendon injury patients and the expected increase in TAM with treatment was 100°. Seven patients were required in each comparison group. To allow for 25% attrition, 27 patients requiring tendon repairs in Zones V and VI were recruited from three teaching hospitals in Western Australia and allocated randomly to the three treatment groups. They were referred to occupational therapy by hand surgeons within 5 days of their operation. The project was approved by the human research ethics committee of the hospitals and informed consent was obtained from each participant. Patients were excluded if they had associated pathology that limited their ability to comply with the assigned protocol or they had only one tendon repaired in the index or little finger.
Treatment Protocols
Postoperatively, all patients were immobilized in a volar plaster slab with the wrist in 30°–45° extension, the MCP joints in 0°–30° flexion, and the IP joints immobilized in neutral. All patients received edema and scar management regardless of their treatment group allocation. In the IM group, patients were fitted with a resting splint and immobilized for 3 wk. Patients in the EPM group were fitted with a dorsal dynamic extension splint and commenced early controlled passive motion in the first 5 days after surgery. The EAM patients were fitted with a simple palmar blocking splint and commenced early active motion in the first 5 days. Figure 1 shows details of the three treatment protocols.
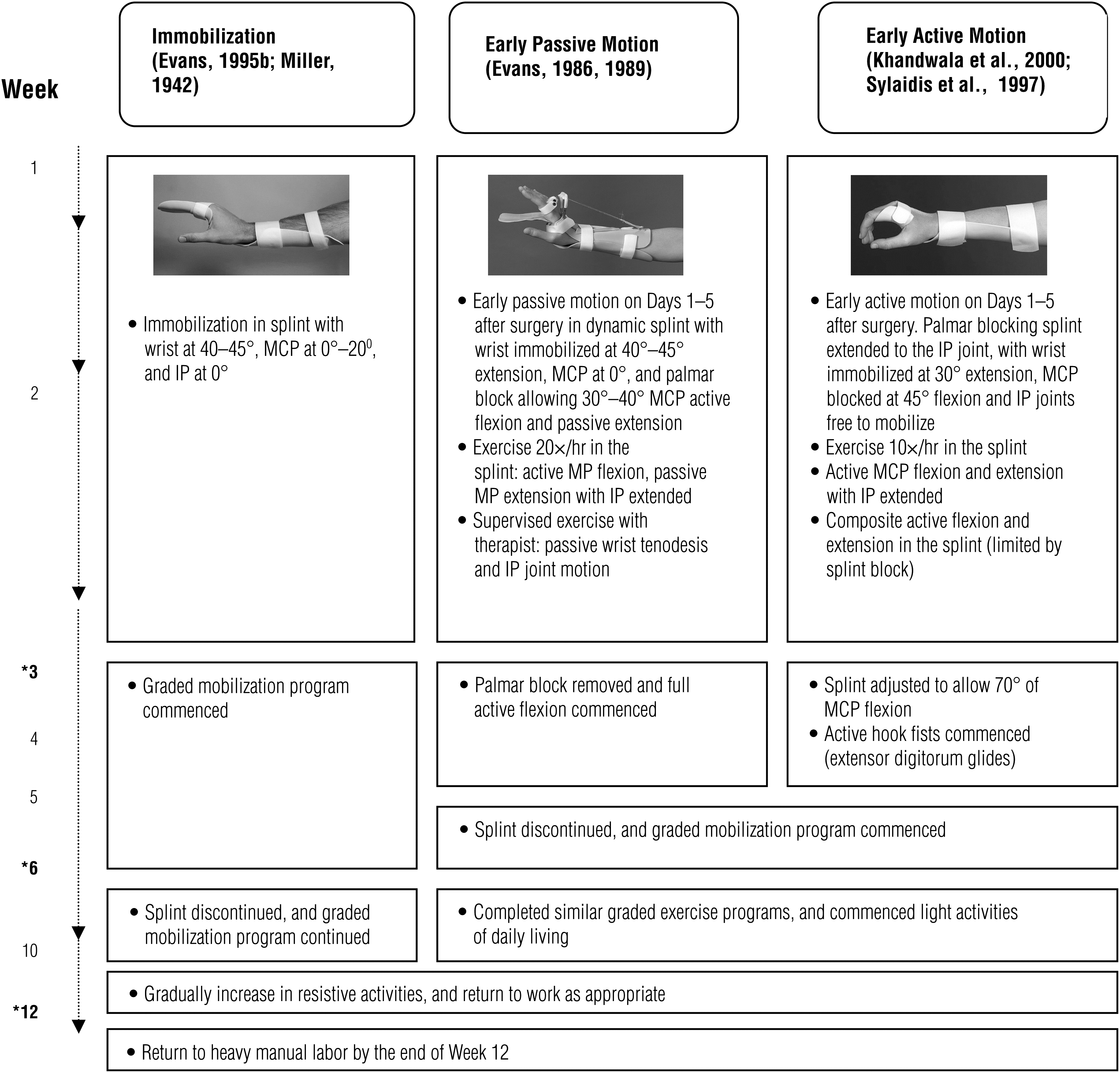
Summary of the three treatment protocols. IP = interphalangeal; MCP = metacarpophalangeal.
A manual was developed to ensure that patients received uniform treatment in each protocol, and it was issued to all the treating therapists. The manual consisted of weekly treatment instructions with photographs, as well as home program handouts for the patients. In developing the manual, we conducted an extensive literature review and adopted best practice in each protocol. An expert panel composed of hand surgeons and senior hand therapists reviewed the treatment manual’s quality. On average, the treating therapists (n = 4) had 2.85 yr (standard deviation [SD] = 1.2) experience in hand rehabilitation. Among patients in the three treatment groups, we found no differences with respect to total contact time with the therapist (mean [M] = 409 min, SD = 93, range = 335–580 min, p = .218) and visits to the clinic per week (M = 1.75, SD = 0.6, p = .32).
Outcome Measures
Before the study began, therapists received training from Barbara Hall on the data collection procedure. During the initial assessment, each patient’s demographic data and vocational history were recorded. Patients were reassessed at 3, 6, and 12 wk on self-reported functional capability, extension lag, range of motion (ROM), and grip strength. ROM measurements for flexion and extension were recorded for the MCP, proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints using a standardized finger goniometer and following American Society of Hand Therapists (1992) techniques. Measurements were converted to TAM for analysis. The TAM score was calculated by subtracting the total extension deficits of finger joints (MCP, PIP, and DIP) from the total finger joint flexion of the same digit (American Society of Hand Therapists, 1992). Functional ability within the past 24 hr was measured by a self-report 10-point visual analog scale (VAS) ranging from 0 (unable to perform any functional task) to 10 (no difficulty to perform functional tasks). Ability to extend the affected finger was measured; 0° indicated ability to fully extend the finger joint, and a positive value indicated an extension lag. Grip strength was measured at Week 12 using a standardized protocol (American Society of Hand Therapists, 1992) with a calibrated Jamar dynamometer (Patterson Medical/Sammons Preston Corporate, Bolingbrook, IL) on both the affected hand and the unaffected hand.
Statistical Analysis
Descriptive statistics were used to profile the patients’ demographic, vocational, and clinical characteristics. Changes within and between groups in TAM, self-reported function, extension lag, and grip strength were assessed by repeated-measures analysis of variance (ANOVA) F tests and post hoc analyses. Because the sample sizes were relatively small, we also applied the corresponding nonparametric Friedman’s test (Portney & Watkins, 2009). We made a Bonferroni adjustment of α level to .017 to reduce the chance of Type I errors in repeated measures. All statistical analyses were performed using SPSS Version 16 (SPSS, Inc., Chicago).
Results
Twenty-seven patients (M age = 30.4, SD = 3.7) consented to participate voluntarily and attended the initial assessment. Nine patients dropped out of treatment at Wk 6: 5 from the IM group and 4 from the EPM group. The defaulters (M age = 33.8, SD = 2.7 yr) declined to continue the rehabilitation or to take part in the exit assessment and claimed that they had already recovered and no further treatment was necessary. At Wk 12, 18 patients (M age = 31.6, SD = 3.8 yr) had completed the rehabilitation program, and a total of 24 injured digits were available for analysis. The patient’s demographic information and the characteristics of their injured fingers are summarized in Table 1. The sample had no fractures of the phalanges, metacarpal, or carpal bones.
Demographic Profile of Patients (N = 18) and Characteristics of Injured Fingers (N = 24) in the Three Treatment Groups
Number in parentheses indicates number of injured fingers.
Metacarpal phalangeal joint capsule damage, infection of interosseous muscle and finger joints.
To assess differences between the three treatment protocols at each time point, we conducted an ANOVA; the results are presented in Table 2. Patients in the EAM protocol appeared to improve to a greater extent at Wk 3, 6, and 12. Post hoc tests indicated that all pairwise differences between protocols were significant, except for immobilization against the passive motion protocol (t[46] = –0.56, p = .581). We also conducted a repeated-measures ANOVA to examine the change in TAM over time and found no apparent violations of statistical assumptions. Significant increasing trends over time were identified in the three comparison groups, suggesting that all patients showed steady improvement during the study period (F[2, 46] = 75.6, p < .001). Similar results were also obtained from the nonparametric Friedman’s test (p < .001).
Results of Total Active Motion (TAM; N = 24)
Note. TAM = Active (MCP + PIP + DIP) flexion − Active (MP + PIP + DIP) extension. n = number of injured fingers; MCP = metacarpal phalangeal joint; PIP = proximal interphalangeal joint; DIP = distal phalangeal joint.
F(2, 21) = 10.11, p = .002. b F(2,21) = 5.29, p = .003. c F(2,21) = 3.76, p = .004.
Patients in EAM were observed to have less extension lag over 12 wk, but the differences among the three groups were not significant (F[2, 46] = 3.45, p = .897): IM, M = 14.6, SD = 2.4; EPM, M = 14.3, SD = 1.9; and EAM, M = 7.87, SD = 1.5. Although EAM patients reported more improvement in function, the mean VAS scores were similar across groups (F[2, 34] = 9.14, p = .073): IM, M = 2.78, SD = 0.56; EPM, M = 3.15, SD = 0.61; and EAM, M = 3.45, SD = 0.63. Moreover, we found no difference in grip strength at Wk 12 among the three groups (F[2, 15] = 6.84, p = .097): IM, M = 34.9, SD = 2.91; EPM, M = 35.6, SD = 2.98; and EAM, M = 38.9, SD = 2.26.
Discussion
An immobilization protocol is routinely prescribed for noncompliant patients because of its low-maintenance splint and straightforward instructions. Some clinicians consider IM an acceptable treatment option for all patients with Zones V and VI extensor tendon injuries (Carl, Forst, & Schaller, 2007; Purcell et al., 2000). However, the risk of active extension lags of the MCP, extrinsic tightness, and adhesions resulting in digital flexion loss may offset the benefits gained from the IM protocol. To reduce the risk of adhesions, participants in this study were immobilized for 3 wk, in contrast to the 4 wk suggested by Bulstrode et al. (2005) and Mowlavi et al. (2005). Our participants showed adequate progress over the 12 wk. When compared with EAM, IM patients appeared to have lower ROM and more extension lags at 3, 6, and 12 wk.
In an RCT, Mowlavi et al. (2005) showed that EPM patients achieved better short-term results in TAM and grip strength than did IM patients, but long-term recovery of patients in 6 mo was found to be similar. Our study also demonstrated that the pairwise comparison of the IM and EPM over 12 wk was not significant. Numerous authors have been critical of EPM splints as being time consuming to fabricate and expensive and inconvenient to wear (Chester et al., 2002; Khandwala et al., 2000; Russell, Jones, & Grobbelaar, 2003). The complexity of the protocol has made it suitable only for motivated patients who have a strong desire to recover and resume normal hand functions (Mowlavi et al., 2005). Further clinical trials to investigate the application of EPM treatment procedures are warranted. The EAM protocol involves fabrication of an uncomplicated blocking splint and easy-to-follow exercise regimens, an approach that would indicate early return to hand functions with fewer tendon-healing complications.
This study’s results suggest that when compared with patients in the EPM and IM groups, patients treated with the EAM protocol achieved greater active ROM, less active extension lag, and better self-report function score. The findings support the commonly held belief that EAM can lead to better recovery in tendon injury (Bulstrode et al., 2005; Carl et al., 2007; Mowlavi et al., 2005; Newport & Tucker, 2005). The literature has shown that experienced clinicians recommend EAM because it enhances intrinsic tendon strength, promotes tendon gliding, and prevents adhesions (Sylaidis et al., 1997; Thomas, Moutet, & Guinard, 1996). The EAM blocking splint used in the study is simpler and more cost-effective to fabricate than the dynamic splint in the EPM protocol (Khandwala et al., 2000).
Over the past 30 yr, several different treatment techniques have been developed, including immobilization of IM patients from between 3 and 6 wk in a splint (Bulstrode et al., 2005; Carl et al., 2007; Evans, 1995a; Mowlavi et al., 2005; Purcell et al., 2000; Russell et al., 2003) and positioning the MP joint at 30°, 45°, or 50° in EAM protocols (Bulstrode et al., 2005; Mowlavi et al., 2005). Russell et al. (2003) compared 65 patients in IM and EPM but did not commence motion for the EPM group until Week 2–3, contrary to the standard practice of mobilizing the fingers by Day 5 after surgery (Evans, 1995b; Gelberman et al., 1982, 1991; Takai et al., 1991). The lack of comprehensive treatment guidelines in the literature has led to many variations in clinical treatment protocols and types of splints used by occupational therapists in their rehabilitation of extensor tendon injuries. The absence of detailed and uniform postoperative treatment protocols affects the clinician’s ability to objectively measure outcomes. The treatment manual used was a detailed and comprehensive guide that facilitated uniformity of the clinical procedures for the protocols. The participating hospitals have continued to use this manual to train hand surgeons and therapists and as a guideline for further research in extensor tendon injuries. A simplified version of the document is provided in the Appendix (available online at www.ajot.ajotpress.net [navigate to this article, and click on “supplemental materials”]); a full version is available from the authors on request).
This study has several limitations. In comparing the treatment groups, Type I or Type II error was a strong possibility because of the small samples in the IM and EPM groups. The α levels were adjusted to .017 to reduce the chance of Type I errors in repeated measures. Although TAM is widely accepted as a reliable indicator of tendon injury recovery, other measures of treatment effectiveness should also be considered. Therefore, we collected and analyzed self-reported function, grip strength, and extension lag but detected no between-group difference, which may be attributed to the small number of patients involved.
The high attrition rate also posed another limitation. The study had 33% loss to follow-up. Similar compliance problems for the same age group in tendon repair rehabilitation have been reported (Carl et al., 2007; Hahn, Konig, & Weihs, 2003; Newport, 1998; Russell et al., 2003). Extensor tendon injury is common among young men, who can be a challenge to treat because of their noncompliance with the rehabilitation protocol (Khandwala et al., 2000). Ultimately, the patient’s goal is rapid return to work. Therefore, we recommend a client-based, personalized approach that acknowledges clients’ life situations and meets their expectations with minimal disturbance to their functional performance and occupational role. Our study suggested that these young men would benefit from the EAM protocol’s simpler splinting and effective exercise program.
The mechanism of injury, occurrence of multiple-digit involvement, complex and simple tendon injuries, associated injuries among patients, and dissimilarities in skills of treating therapists may have contributed to the variability of the outcome measures. Finally, only patients with Zones V and VI tendon injuries were included, so the clinical findings are not applicable to other zones of injury.
In conclusion, the EAM protocol using a palmar blocking splint may be beneficial to patients with Zones V and VI extensor tendon injuries. A large prospective study should be conducted to confirm the pilot findings. The treatment manual developed in this study can be a useful resource for occupational therapists working in extensor tendon rehabilitation.
Supplemental Material
Supplementary material for Comparing Three Postoperative Treatment Protocols for Extensor Tendon Repair in Zones V and VI of the Hand
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2010.09091.pdf for Comparing Three Postoperative Treatment Protocols for Extensor Tendon Repair in Zones V and VI of the Hand by Barbara Hall, Hoe Lee, Rohan Page, Lorna Rosenwax and Andy H. Lee in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We sincerely thank the medical and allied health professionals of Sir Charles Gairdner Hospital, Royal Perth Hospital, Fremantle Hospital, and University of Western Australia.
The research was supported by the Australian Hand Therapy Association Fund, Fremantle Hospital Fund, and Australian Physiotherapy Association Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.