
Abstract
In Canada, 53.4% of head injuries treated in emergency departments in 2001 occurred among children ages 10–14 yr; similarly, among youth ages 15–19 yr, 42.9% of emergency department visits were accounted for by head injury (Kelly et al., 2001). Concussion is a pathophysiological injury induced by biomechanical forces caused by impact to the head, neck, or body (McCrory et al., 2013). Approximately 30% of youth who sustain a concussion do not recover in the average time span of 1 mo and continue to experience prolonged symptoms (Zemek et al., 2016). These symptoms include a constellation of physical, cognitive, and emotional symptoms and fatigue. According to the International Statistical Classification of Disease and Related Health Problems (World Health Organization, 2010), persistent concussion syndrome is defined as symptoms of concussion that persist beyond 1 mo.
The landscape of concussion treatment, in Canada specifically, has been summarized as being inconsistent in training and knowledge on traumatic brain injury; often recommending unnecessary, costly, and unsubstantiated treatment; and lacking alignment with evidence-informed guidelines (Ellis et al., 2017). Within the scarce public sector services available, management of persistent concussion is often constrained by limited appointments and a consultative approach. There is a clear gap between the current service delivery model and the needs of this population to enable return to meaningful activity. In this pilot study, we aimed to assess the feasibility of a clinically informed, group-based intervention for youth experiencing persistent concussion symptoms.
Activity restrictions in the form of physical and cognitive rest have typically been prescribed as part of evidence-informed guidelines for youth experiencing concussion symptoms (McCrory et al., 2013). Although this recommendation may be valuable in the acute phase (7–10 days), prolonged inactivity in the persistent phase (>1 mo) may contribute to secondary psychosocial challenges (Paniccia & Reed, 2017; Reed et al., 2015), including reduced meaningful interactions with friends, teammates, teachers, and coaches (Broshek et al., 2015; Jonsson & Andersson, 2013). A significant shift in clinical recommendations has occurred whereby prolonged rest and inactivity are discouraged and symptom-limited activity is encouraged to promote recovery (Grool et al., 2016; Imhoff et al., 2016; Reed et al., 2015).
Research has indicated that youth with persistent concussion experience limited occupational repertoires; they do not engage in the same number of occupations as prior to their concussion, have difficulty participating, or avoid reintegrating out of fear of symptom exacerbation (Paniccia & Reed, 2017). These challenges can affect their self-efficacy, that is, an individual’s perceived confidence in her or his abilities (Jonsson & Andersson, 2013). These findings underscore the importance of shifting from symptom-focused recovery to examining occupation-based factors such as self-efficacy and participation in meaningful activities.
Persistent concussion is also being recognized as a form of autoregulatory dysfunction (e.g., stress response) in which the brain does not achieve baseline levels of homeostasis (Ellis et al., 2016; Leddy et al., 2007). Heart rate variability (HRV) is an objective neurophysiological indicator of autonomic nervous system functioning (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology [hereinafter, Task Force], 1996). HRV is quantified by measuring variation in the time intervals between heartbeats. Increased variability in heart rate (i.e., increased HRV) is demonstrative of healthy neurophysiological function, whereas decreased HRV may reflect challenges adapting to and being flexible in the environment. In studies of young adult athletes with persistent concussion symptoms, reduced HRV was found compared with control participants, suggesting a delayed return to homeostasis (Ellis et al., 2016; Leddy et al., 2007). Investigating HRV in addition to functional measures could provide a holistic understanding of persistent concussion symptoms in youth.
Management of persistent concussion symptoms in youth can benefit from an approach that promotes safe levels of physical and cognitive activity during recovery while also addressing the emotional toll of symptoms. Western yoga practice is rooted in hatha yoga and meditation and comprises physical postures to lubricate joints, muscles, and ligaments and breathing techniques of inhalation and exhalation (Collins, 1998). Mindfulness-based yoga (MBY) differs from hatha yoga in that people are invited to scan their bodies and become more familiar with and accepting of the sensations they feel in varying physical postures (Kabat-Zinn, 2006). This present-focused sensory awareness fosters explicit awareness of the body, without active judgment, and training in cognitive decentering, the ability to relate to physical sensations and thoughts as mental events rather than facts or statements of truth (Fresco et al., 2007). Rather, individuals are encouraged to come back to their breath and center themselves in the present moment (Kabat-Zinn, 2006).
Past research using MBY interventions has demonstrated benefits in physical and psychological functioning (e.g., decreased stress, increased self-efficacy; Deshpande et al., 2009). A pilot study by Azulay et al. (2013) examined the effects of mindfulness-based stress reduction in adults with persistent concussion symptoms and found increased quality of life and perceived self-efficacy. MBY thus has the potential to shift the focus away from symptoms while building self-efficacy and enhancing participation in daily activities.
The potential links among self-efficacy, participation, and HRV can enhance the understanding of occupation-based domains and neurophysiological homeostasis in youth with persistent concussion symptoms. The objectives of this study were twofold: (1) to evaluate the feasibility of a novel intervention for youth with persistent concussion symptoms and (2) to explore the potential impact of MBY on occupation-based (self-efficacy and participation) and neurophysiological (HRV) measures.
Method
Design
Research ethics board approval and informed consent were obtained prior to data collection. This pilot study used a case series, repeated measures design. Occupation-based (self-efficacy, participation) and neurophysiological (HRV) measures were collected before, immediately after, and 3 mo after the MBY intervention. HRV was also measured during the MBY intervention.
Participants
Participants were recruited from hospital and community-based outpatient settings. Participants were included in the study if they were ages 13–18 yr, were English speaking, and had experienced postconcussion symptoms for >4 wk. Exclusion criteria were neurological disease, diagnosed cardiac issues, and unmanaged psychiatric diagnosis (i.e., mental health issue not being managed by a physician or allied health professional).
Measures
Children’s Assessment of Participation and Enjoyment.
The Children’s Assessment of Participation and Enjoyment (CAPE; King et al., 2007) is a 55-item questionnaire that examines how children and youth (ages 6–21) participate in leisure and recreation activities. It examines five dimensions of participation: diversity (number of activities done), intensity (how often), with whom the activity is done, where the activity takes place, and level of enjoyment of each activity. Higher scores indicate increased participation. Internal consistency is α = .32–.76, and test–retest scores are .67–.86 (Imms, 2008).
Self-Efficacy Questionnaire for Children.
The Self-Efficacy Questionnaire for Children (SEQ–C; Muris, 2001) is a 24-item questionnaire in which participants rate their perceived ability to accomplish a task on a scale ranging from 1 (not at all) to 5 (very well). The questions cover three domains of self-efficacy: social, academic, and emotional. In a sample of 373 adolescents, Cronbach’s α was .85–.88 (Muris, 2001).
Heart Rate Variability.
HRV measures were calculated using standard time and frequency domain parameters set out by the Task Force (1996). Time domain variables provide an overall measure of variability and complexity of interval times between heartbeats. Frequency domain measures describe the periodic oscillations of the heart rate signal to reflect the power (magnitude) of sympathetic and parasympathetic systems in driving change in HRV (see supplemental material for definitions of variables; available online at http://otjournal.net; navigate to this article, and click on “Supplemental”).
Postconcussion Symptom Inventory.
The Post Concussion Symptom Inventory (PCSI) is a 21-item self-report measure in which symptom severity is rated on a scale of 0 (not at all) to 6 (severe) in physical, cognitive, emotional, and sleep domains (Sady et al., 2014). Internal consistency is .79–.93 for the subscales and .94 for the total symptom score (Sady et al., 2014).
Godin Leisure-Time Exercise Questionnaire.
The Godin Leisure-Time Exercise Questionnaire (GLTE; Godin & Shepard, 1997) is a self-report measure that assesses weekly physical activity engagement by asking respondents to indicate how many times per week they engage in strenuous (heart beats rapidly), moderate (not exhausting), or mild (minimal effort) exercise. Reliability is moderate (r = .62; Helmerhorst et al., 2012).
Intervention
The MBY intervention took place in a group setting at a children’s rehabilitation hospital. All sessions were carried out by the second author (Ruby Knafo), who is both an occupational therapist and a certified yoga instructor. The components of each MBY session were as follows:
Mindfulness meditation: Attention was anchored on the sensations of breathing and the body, training the mind to notice when distraction and thinking occur. Thoughts, feelings and emotions, and physical sensations are regarded as passing states (impermanent). Participants were encouraged to use mental noting (i.e., labeling thoughts as “planning,” “remembering,” or “thinking” without attaching value or judgment) to aid in disengaging from rumination and returning to the breath.
Physical yoga postures: All postures were novice level and included standing, supine, prone, and seated stances. Modified postures were offered to match participants’ comfort level.
Procedure
All data collection took place at the children’s rehabilitation hospital, carried out by the primary author (Melissa Paniccia). Before intervention, a demographic information form was used to collect data on age, sex, concussion history, and history of mental health issues. The CAPE, SEQ–C, PCSI, and GLTE and a 24-hr HRV recording were collected at pretest, posttest, and 3-mo follow-up. In the absence of baseline measures for concussion symptoms and physical activity, participants were instructed to reflect on a perceived baseline at the time of preintervention data collection for the PCSI and GLTE. A participant satisfaction survey (Larsen et al., 1979) was also administered postintervention. A 45-min HRV recording was collected during each of the eight MBY sessions. The Polar RS800CX watch and chest strap (RS800cx; Polar Electro, Kemple, Finland) were used to collect HRV data.
Data Analysis
HRV data were analyzed with Kubios Version 2.0 (Biosignal Analysis and Medical Imaging Group, Kuopio, Finland), and a very low filter was used to remove ectopic heartbeats and noise. Window frames were 300 s, 50% overlap, 4-Hz interpolation rate. Power spectral density analysis was used to derive frequency domain variables. Visualization analysis was suitable for the following reasons: Low power increases Type I error, overestimating true effects (Button et al., 2013), and in case series methodology, visualizations are considered the most suitable approach to gleaning information from preliminary, exploratory studies (Kooistra et al., 2009). Line graph visualizations were explored to depict trends in occupation-based measures. Missing data within the HRV visualizations were a result of lack of attendance or loss of data because of recording malfunction. Line graph visualizations with linear line-of-best-fit trend lines were used to depict changes in HRV for each participant.
Results
Participants (N = 8) were ages 13–17 yr and had experienced persistent concussion symptoms for >4 wk. Two participants did not complete the study (because of distance from hospital [n = 1] and commencing university [n = 1]), and their data were excluded from the analysis. Five participants were girls. Table 1 provides descriptive information on participants included in the study analysis (N = 6).
Participant Demographic Information and Injury Characteristics
Participant had a postinjury mental health diagnosis of major depressive disorder.
Participant had a preinjury mental health diagnosis of generalized anxiety disorder.
Self-Efficacy and Participation
Trends of increased self-efficacy were found from pre- to postintervention across academic (e.g., self-confidence completing homework and asking teachers for help), social (e.g., expressing opinion, managing conflict), and emotional (e.g., controlling one’s feelings, calming down) domains (Figure 1). Regarding participation, no trends were found in diversity, location, intensity, and enjoyment of activities.
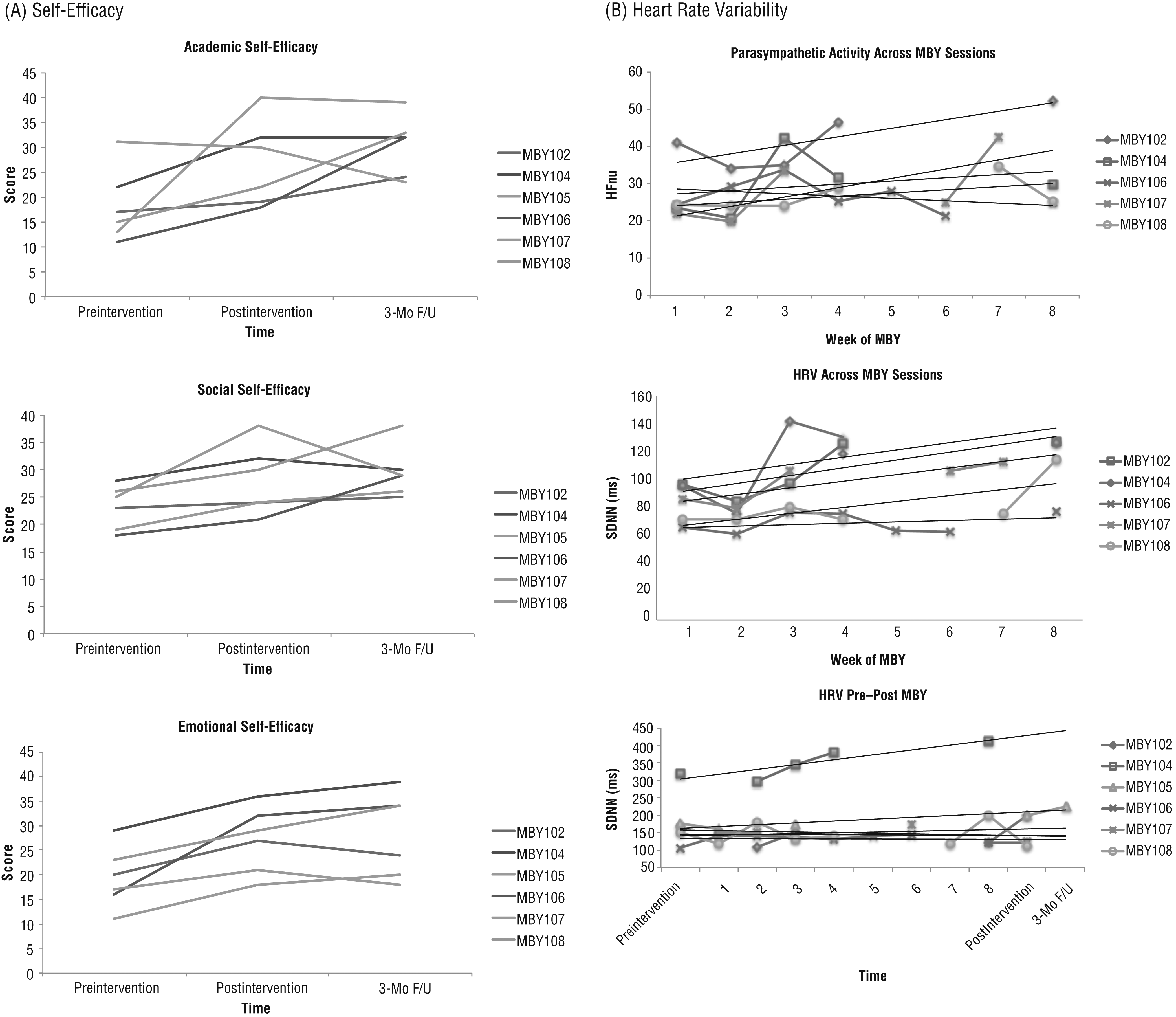
Primary outcome measure scores at pretest, posttest, and 3-mo follow-up. (A) Self-efficacy scores in academic, social, and emotional domains. (B) Trends in HRV within the 45-min MBY sessions and across 24-hr recordings at pretest, posttest, and 3-mo follow-up.
Heart Rate Variability
Within time domain variables, standard deviation of the NN (R-R) intervals (SDNN) appeared to gradually increase from the first to last session of MBY (Figure 1). Other time-domain measures (proportion of NN50 divided by the total number of NN [R-R] intervals, root mean square of the successive differences) revealed a mix of directionality in trends (3 increased, 2 decreased, 1 remained the same). Within frequency domain variables, HFnu (indicative of parasympathetic activity) also showed trends of gradual increases from the first to last session of MBY (Figure 1). Across the 24-hr recordings, SDNN appeared to gradually increase from preintervention to 3-mo follow-up.
Concussion Symptoms and Physical Activity
Trends of decreased symptoms on the PCSI across all four domains (physical, cognitive, emotional, fatigue) were found after the MBY intervention and were maintained at 3-mo follow-up (Figure 2). At preintervention, elevated mild exercise (e.g., easy walking) and no reports of strenuous exercise were reported compared with perceived baseline ratings. At postintervention, trends of mild and strenuous exercise went in opposite directions; mild exercise appeared to decrease and strenuous exercise increased, and this trend was maintained at 3 mo (Figure 2).
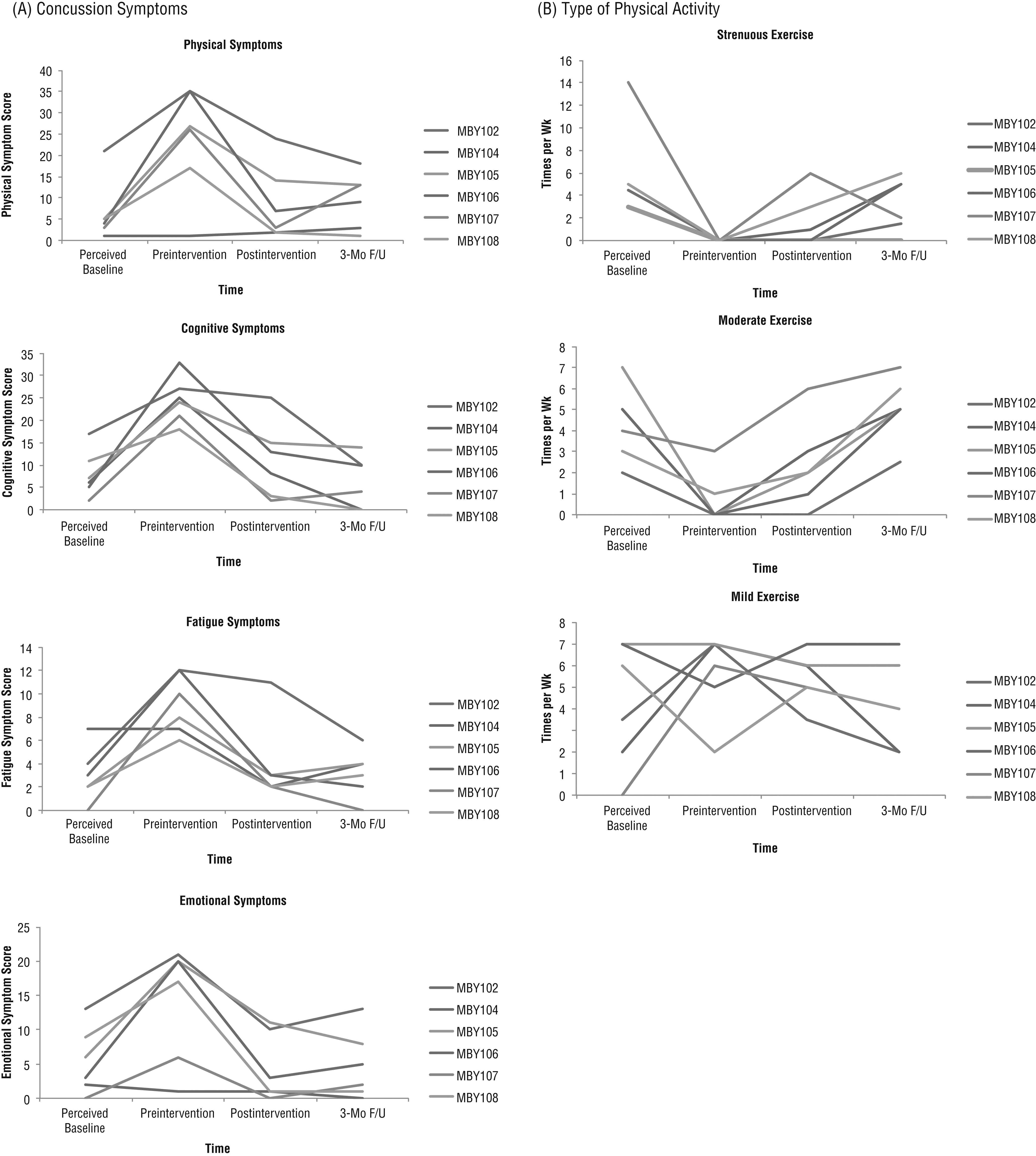
Secondary outcome measure scores at pretest, posttest, and 3-mo follow-up. (A) Concussion symptom severity scores in the physical, cognitive, emotional, and fatigue domains across time. (B) Physical activity ratings of mild, moderate, and strenuous exercise across time.
Feasibility: Data Collection and Participant Compliance and Satisfaction
Participants were expected to attend a total of 11 sessions, three assessment sessions (pre, post, and 3-mo follow-up) and eight MBY intervention sessions. All 6 participants attended the three assessment sessions, which took 1 hr. No participants expressed difficulty or fatigue in completing the measures. The intervention sessions lasted 1.5 hr (heart rate monitor setup plus 45-min MBY session); no participants refused heart rate data collection. No participants needed to leave, take a break, or modify postures during any of the MBY sessions.
Attendance was 83%–100% for five of the MBY sessions and 50%–67% for the other three. Lack of attendance was unrelated to intervention engagement (e.g., graduation, exams or assignments, out-of-town vacation). Participants completed satisfaction surveys postintervention with the following results: 4/6 rated MBY as “meeting all their needs” and 2/6 rated it as “most of their needs were met,” 6/6 would “recommend MBY to family or friends in need of similar help,” 3/6 each indicated that MBY “helped somewhat” or “helped a great deal,” and 5/6 would “definitely” do MBY again.
Discussion
This pilot study supports the feasibility of a group-based MBY intervention for youth with persistent concussion symptoms. Participants demonstrated preliminary trends of increased self-efficacy, decreased symptoms, and improved neurophysiology. Conclusions cannot be drawn from improvements seen in this study because persistent concussion in youth can resolve as a function of time. However, this study demonstrates a replicable process for a larger scale trial; data collection time and methods, participant attendance, and satisfaction were reflective of good clinical uptake for this population.
In the cost-constrained health care environment of treating concussions in youth, developing novel and feasible intervention protocols is crucial to address the needs of this complex population and implement service delivery models that focus on cost-effective specialized treatment. Although not the focus of this pilot work, group intervention settings enable participants to learn from one another, creating a social atmosphere of shared experiences (Henderson & Pehoski, 2006). In their comments on the participation satisfaction survey, participants alluded to the benefits of a group intervention; one noted that it “helped me get cleared to walk/ride a bike. It also is a good program for people with concussions to know they aren’t alone” and “helped calm down any anxious feelings.” Given the limited sessions clinicians are given within the consultative model, this intervention approach can begin to address some of the current practice limitations to ensure that this population is supported in multiple life domains (e.g., safe physical activity, psychosocial function, development of coping strategies).
Because of the exploratory nature of this study, and to protect this vulnerable population of youth, clinicians, researchers, and ethics specialists decided on a protocol that was minimally intensive and time consuming (to decrease the risk of symptom exacerbation). Whereas most mindfulness programs have a home practice component, our program did not; evidence-informed guidelines in the province of Ontario recommend conservative treatment of youth with persistent concussion (Ontario Neurotrauma Foundation, 2014), so this protocol was specifically modified to provide a frequency and intensity that were not overly exerting to address fatigue, anxiety, and significant physical deconditioning. We therefore modified the intensity and frequency of this MBY intervention from adult recommendations of 2 hr, 1×/wk for 10 wk to 45 min, 1×/wk for 8 wk. In the context of the time commitment to come to the hospital for 11 sessions, this protocol was both feasible and realistic.
Persistent symptoms may be maintained by real-life functional factors (e.g., changes in academic performance, participation in leisure activities) that extend beyond the pathophysiology of the injury (Stein et al., 2016). Youth with persistent concussion symptoms likely experience difficulties in verifying and evaluating their own abilities because of changes in their daily occupational repertoire (Paniccia & Reed, 2017). These difficulties may explain the change in self-efficacy seen across academic, social, and emotional domains. We found no significant trends of change in participation in and enjoyment of daily leisure activities. However, MBY was administered in a group setting in which participants had the opportunity to consistently see other youths going through the same experiences.
This pilot study found preliminary trends of improved HRV over the course of the eight MBY sessions and from pre- to postintervention. It is unclear whether this result reflects an appropriate reaction to concussion as a stressor or whether it exceeds typical neurophysiological responses in creating a more detrimental state for the individual. Nonetheless, safe physical activity may enable changes in neurophysiology, and recent shifts in managing persistent concussion have suggested that low-intensity mind–body interventions (without exacerbation of symptoms) may assist with autoregulatory function (Leddy et al., 2007) and can alleviate the occupational costs associated with inactivity and prolonged rest (Paniccia & Reed, 2017). Because of the pilot nature of this study, youths were not excluded if they were receiving other interventions concurrently. Thus, participation in other interventions may have played a role in these neurophysiological findings.
MBY does not explicitly address postconcussion symptoms; however, reports of decreased symptoms were found across all domains. This finding highlights the need to consider functional and occupation-based approaches in enabling recovery rather than pervasive attention to symptoms. Finally, the positive changes observed in participants’ physical activity repertoire were also promising. Whether MBY acted as a safe catalyst to reintegrate previous forms of activity or whether the effect of time contributed to symptom resolution is still unclear.
Limitations and Future Research
This study was a descriptive analysis of a small, repeated measures case series; thus, findings cannot be generalized to the larger population of youth with persistent concussion symptoms. We did not account for the social environment in which MBY was carried out (i.e., group-based setting). For example, participants were instructed to arrive 30 min before the start of each MBY session to return their HRV equipment and be suited with new equipment. During this time, participants occupied the same space as other youths, with opportunities to talk about their day or their experiences, which may have played a role in the findings. In addition, we did not use neuropsychological assessment in this study, which would have made a significant contribution because attentional control (i.e., sustained attention) is a key component of the mindfulness training in MBY. Given the limited resources and diverse array of measures collected, this additional consideration was not feasible. Future research including a control group and measures that account for social interaction and potential neuropsychological gains would allow more rigor in further exploring the potential of this intervention.
Implications for Occupational Therapy Practice
In the context of evidence-informed recommendations for the optimal level of rest, a “sensible approach” has been recommended that involves a gradual reintegration into previous forms of activity (Stein et al., 2016). MBY is sensible in that it is a biopsychosocial approach that marks a significant shift away from the focus on symptoms. Green et al. (1997) explained that for people who experience concussion to live a functional daily life, a tolerance and acceptance of symptoms needs to occur to facilitate coping. In this study, no symptom data were collected (with the exception of HRV) during the 8-wk intervention, deemphasizing the focus on symptom reporting. MBY may act as a form of “safe doing” in which youth can be engaged in activities that target both physical and psychosocial aspects in a way that allows them to establish coping mechanisms for their current symptoms but does not result in exacerbation. Our findings have the following implications for occupational therapy practice:
Group-based interventions may be a feasible way to offer MBY for youth continuing to recover from concussion.
MBY has potential as a clinical intervention for youth with persistent symptoms because it provides low-intensity exercise along with training on acceptance of the present moment.
MBY supports occupation-based rehabilitation in building self-efficacy in the key domains of academic, social, and emotional functioning.
Supplemental Material
Supplementary material for Mindfulness-Based Yoga for Youth With Persistent Concussion: A Pilot Study
Supplementary material, sj-pdf-1-aot-10.5014_ajot.2019.027672.pdf for Mindfulness-Based Yoga for Youth With Persistent Concussion: A Pilot Study by Melissa Paniccia, Ruby Knafo, Scott Thomas, Tim Taha, Alysha Ladha, Laura Thompson and Nick Reed in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
This work was funded by the Canadian Institutes of Health Research (127048), the Ontario Neurotrauma Foundation, and the Ontario Brain Institute. The Ontario Brain Institute is an independent nonprofit corporation funded partially by the Ontario government. The opinions, results, and conclusions are those of the authors, and no endorsement by the Ontario Brain Institute is intended or should be inferred. This study was registered at ![]() (NCT03217695).
(NCT03217695).
This work was originally featured in the first author’s doctoral thesis as part of a larger body of work on neurophysiological variation. The authors thank the Rehabilitation Sciences Institute at the University of Toronto for their support throughout the doctoral program. We also acknowledge the efforts of the members of the Canadian Institutes of Health Research NeuroCare Team and the members of the Concussion Centre (Bloorview Research Institute), and specifically Katherine Wilson. Finally, occupational therapy students Alliana Bagtas and Teija Hunt are thanked for their contribution to data collection. We are grateful to the youths and families for their participation in this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.