
Abstract
This systematic review examines the efficacy of yoga as a neuromuscular intervention for community-dwelling populations at risk for falls to determine its utility for use in occupational therapy intervention. Populations included older adults and adults with traumatic brain injury (TBI), cerebrovascular accident (CVA), dementia and Alzheimer’s disease (AD)–type dementia, multiple sclerosis (MS), and Parkinson’s disease (PD). Benefits of yoga include improved posture control, improved flexibility of mind and body, relaxation, and decreased anxiety and stress. A systematic review of the literature was conducted to understand the salutary benefits of yoga for clients who are at risk for falls because of neuromuscular issues. Moderate evidence supports the use of yoga to decrease the risk for falls for community-dwelling older adults and people with CVA, dementia and AD-type dementia, and MS. Studies involving people with TBI and PD did not include strong enough evidence to be able to make a clear classification.
More than 800,000 older adults are hospitalized each year because of falls (Centers for Disease Control and Prevention [CDC], 2016). The risk for falls increases exponentially after an adverse health event, as a progressive disease advances, or with neuromuscular changes seen with aging adult populations. With an increasing risk for falls, overall decreased levels of physical activity, increasing levels of anxiety, and decreased quality of life (QOL) are typically reported (Stenhagen et al., 2014). Community-dwelling older adults and people with traumatic brain injury (TBI), cerebrovascular accident (CVA), dementia and Alzheimer’s disease (AD)–type dementia, multiple sclerosis (MS), and Parkinson’s disease (PD) are reported to be at high risk for falls (World Health Organization [WHO], 2006). Although the cause of falls may vary, balance deficits as a result of sensory–motor issues often contribute to this problem (Berg & Cassells, 1992; NIH, 2013).
The CDC (2016) has recommended increasing physical activity to decrease the risk for falls. Systematic reviews support the benefits of yoga to improve balance. The benefits of yoga for people at high risk of falls with movement dysfunction as a result of neurological disorders and age-related neuromuscular changes as well as age-related balance deficits have not been systematically examined. This systematic review seeks to address that gap in knowledge by exploring the efficacy of yoga as an intervention to be used as an adjunct or a modality with occupational therapy with populations at risk for falls with underlying neuromuscular and age-related balance deficits.
Risk for Falls With Increasing Age and Neuropathology
In 2014, the CDC reported 29 million falls among adults age 65 or older (CDC, 2016). Falls are the leading cause of nonfatal injuries for people ages 18–85 yr in the United States, with one in five sustaining a serious injury. In addition to aging, the five most common neurological conditions that pose a high risk for falls are dementia and AD, MS, PD, CVA, and TBI because of primary and secondary sensory–motor deficits (Berg & Cassells, 1992; NIH, 2013; WHO, 2006). Additionally, increasing age and a decline in postural balance increase susceptibility to fall-related injuries (Pizzigalli et al., 2016). The most common fall-related risk factors include age, muscle weakness or impaired motor function, impaired sensory and perceptual function, low vision, impaired mental status, and impaired balance because of a lack of exercise or a neurological condition (NIH, 2013).
Neuropsychophysiological differences exist across this group of conditions contributing to an increased risk for falling (WHO, 2006). Balance deficits are a central concern shared by typically aging older adults and those with neurological disorders as a result of underlying neuromuscular dysfunction or decline. Falls account for the greatest number of injuries for older adults (Berg & Cassells, 1992). People with AD face a 3 times greater fall risk than community-dwelling older adults (Sheridan & Hausdorff, 2007). Inadequate motor responses, muscle weakness, and spasticity compromise balance for people with MS, contributing to a high risk for falls (Cattaneo et al., 2002). Additionally, increasing severity of PD is correlated with an increased risk of falls (Pickering et al., 2007). Falls are also considered the most common medical complication after a CVA or TBI at inpatient rehabilitation settings (McKechnie et al., 2016; Weerdesteyn et al., 2008). Although these populations have increased hospital admissions as a result of falls, the injuries frequently receive more attention than the underlying cause (Lovarini et al., 2013).
Yoga and Balance
Yoga, an ancient Indian practice, incorporates breathing (pranayama), poses (asanas), and meditation (dhyana) to influence a person’s physical, mental, and spiritual well-being to promote health and relaxation (American Osteopathic Association, 2016). Different schools of yoga emphasize one or a combination of the three aspects of the practice (Meyer et al., 2012). Practice that focuses on breathing and meditation seeks to affect the person’s mental and spiritual well-being. Practice that incorporates yoga poses, which are performed slowly and are synchronized with breathing exercises, promotes an iterative process of coordination of the mind and body. This physical and mental coordination continuously strengthens attention, concentration, endurance, voluntary muscle control, and flexibility of the whole being.
Studies have validated the use of yoga as a holistic approach to enhance inner peace, strength, flexibility, and control of mind and body, resulting in improved balance among diverse populations (Jeter et al., 2014). Yoga is also known to affect muscle tone and reaction time (Mishra et al., 2012). In addition, the flexibility in being able to adapt this practice to different levels of function, such as engaging on the floor, in sitting, or in standing, allows people of any functional level to start and progress at their own pace. Overall, irrespective of the type of yoga practiced, the focus is on promoting mind–body unity to improve health and well-being. Its utility in improving function and psychological well-being, combined with its cost-effectiveness and adaptability, makes it a suitable modality for use with a clinical population with neuromuscular dysfunction or decline.
Use of Yoga in Occupational Therapy
Occupational therapy uses a holistic approach in rehabilitation to ensure optimum health and independence in occupations (Hooper et al., 2015), which is synchronous with the overall holistic philosophy of yoga that seeks to address mind–body unity. Yoga, used as an adjunct or modality in occupational therapy intervention, helps reinforce and promote mind–body unity in overcoming the physical and mental barriers of people at risk for falls (Meyer et al., 2012). This use of yoga promotes independence in activities of daily living (ADLs) and QOL.
Safe and stress-free participation in meaningful ADLs is reported to be a challenge for people with balance deficits and increased risk for falls (Berg & Cassells, 1992). Left untreated, stress, anxiety, and neuromuscular decline become progressive issues that further limit engagement in meaningful tasks and negatively affect people’s life and health. The flexibility in adapting the level and intensity of yoga practice across age, experience, and functional level promotes its use as a suitable and efficient modality in clinical settings and in the community (Jeter et al., 2014). An added strength is its potential to contribute to long-term clinical outcomes through availability of community resources after discharge.
The practical, physical, functional, and cost-effective benefits of practicing yoga make it a versatile tool for clinical use in occupational therapy. Moreover, it can be used as a preemptive measure to help maintain balance skills and address fall prevention for older adults. A systematic review of existing literature to understand the benefits of yoga for fall prevention with older adults and people with neuromuscular impairment provides the rehabilitation community and the field of occupational therapy with a summary of findings about a valuable modality that has the potential to support holistic care.
Method
Following an agreed-upon protocol, peer-reviewed journal articles were selected for this systematic review by members of the research team and a librarian. The following search engines were used to identify articles of interest for this systematic review: PubMed, CINAHL, and Google Scholar. The overarching aim was to examine the effects of yoga on balance for people at risk for falls as a result of neuromuscular dysfunction or decline. Typically, because of neuromuscular dysfunction and decline, older adults and people with neurological conditions such as TBI, CVA, dementia and AD-type dementia, PD, and MS are at risk for falls and subsequent injury. For this reason, the inclusion criteria included movement disorders, dyskinesia, yoga, tardive dystonia, muscle stretching exercise, mobility limitation, musculoskeletal diseases, nervous system diseases, motor skills disorders, perceptual disorders, postural balance, hemiparesis, neurological disorders, stroke, traumatic brain injury, and community-dwelling older adults. This review used yoga as a categorical term and did not account for the types of yoga used by the different studies included. The various types of yoga mentioned in the studies used breathing and poses to enhance balance skills. These categories were sought to engage in an in-depth understanding of this population and yoga as an intervention of interest. Search terms included motor skills disorders, movement disorders, dyskinesias, tardive dystonia, musculoskeletal diseases, perceptual disorders, mobility limitation, nervous system diseases, yoga, and postural balance.
To eliminate the risk of duplicating previous studies, all systematic reviews that addressed the effect of yoga and balance were screened in the Cochrane Database of Systematic Reviews, and systematic reviews were excluded from subsequent searches in other databases. Articles published before 2001 were excluded to allow for current evidence to be presented. Studies examining use of yoga with pediatric populations or in combination with another intervention were not included in this systematic review. Articles relating to fibromyalgia and rheumatoid arthritis were also excluded to eliminate the possibility of confounding variables as a result of chronic pain. Articles were screened and eliminated on the basis of the inclusion criteria, exclusion criteria, research design, population studied, the use of yoga as an intervention, and inclusion of a balance measure such as the Berg Balance Scale (BBS; Berg et al., 1992), the Mini–Best Balance Evaluation System Test (MBT; Franchignoni et al., 2010), and the one-leg stand test.
Studies with a quantitative research design and an adult population were further assessed for eligibility and were included in this systematic review or excluded with reason. Overall consensus by the research team was used as the final determinant for inclusion decisions. Figure 1 shows the flow of articles though the process. The analyzed studies were categorized by levels of evidence according to the American Occupational Therapy Association (AOTA; 2015) Guidelines for Systematic Reviews:
Level I: systematic reviews, meta-analyses, randomized controlled trials (RCTs)
Level II: two groups, nonrandomized studies (e.g., cohort, case control)
Level III: one group, nonrandomized (e.g., before and after, pretest and posttest)
Level IV: descriptive studies that include analysis of outcomes (single-subject design, case series)
Level V: case reports and expert opinion that include narrative literature reviews and consensus statements.
To assess for risk of bias, the included studies were evaluated for selection bias, performance bias, detection bias, attrition bias, and reporting bias.
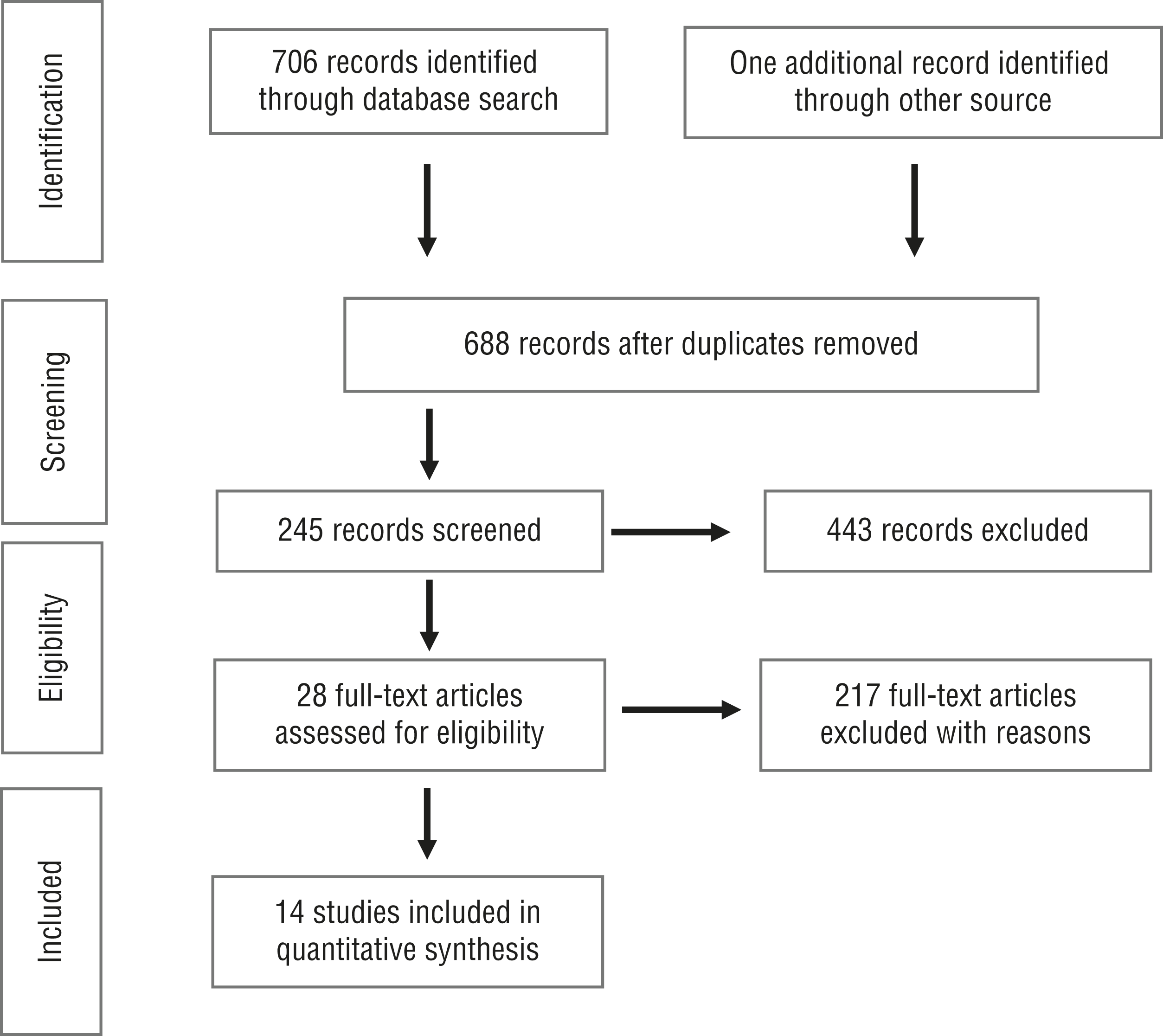
Flow diagram for studies included in the systematic review.
Results
Fourteen studies were assessed to evaluate the effects of yoga as a neuromuscular intervention on balance with people who are at risk for falls. The population of people at risk for falls was divided into six areas: TBI, CVA, dementia and AD-type dementia, MS, PD, and community-dwelling older adults. To quantitatively assess the impact of yoga intervention on balance, 10 studies used the BBS, 2 studies used the one-leg stand test, 1 study used the Tinetti Scale (Tinetti et al., 1986), 1 study used the MBT, 1 study used the Activities-specific Balance Confidence Scale (Botner et al., 2005), and 1 study used a battery of fall scales developed by Finlayson et al. (2009). (Several studies used more than one balance test.)
Each subpopulation at risk for falls was assessed on an individual basis and collectively to see how balance improved for those undergoing yoga as an intervention. When subpopulations were assessed individually, varying strengths of evidence were found for each. When the collection of studies was examined as a whole to represent the umbrella of conditions and disorders that result in falls, 13 studies found statistically significant results for improvement of balance with the use of yoga. The RCT done by Immink et al. (2014) on the status of people with CVA after participating in yoga once per week for 10 wk did not report statistical significance.
The remaining 13 articles, which represented people at risk for falls as a whole, consisted of 5 studies with Level I evidence, 1 study with Level II evidence, 5 studies with Level III evidence, 1 study with Level IV evidence, and 1 study with Level V evidence. Fewer than half of the studies evaluated in this body of evidence qualified as Level I, and those were distributed among the different conditions (Table 1). Overall, we found moderate evidence supporting the use of yoga to improve balance for people at risk for falls.
Study Outcomes, by Condition
Traumatic Brain Injury
Only 1 article examined participants with TBI. Schmid, Miller, et al. (2016) conducted a mixed-methods case study to evaluate the effect of yoga as an intervention on balance, endurance, gait speed, and flexibility in people who had experienced a TBI. This Level V study found that upon completion of an 8-wk yoga program (twice per week), participants demonstrated an improvement in balance (as measured by the BBS), number of repetitions on the chair-to-stand test, endurance, and speed. Although all participants exhibited improvement as a result of engaging in yoga, this study alone is insufficient evidence to clearly justify the use of yoga as an intervention for people with TBI.
Cerebrovascular Accident
Two studies assessed the outcomes of a yoga-based intervention program in poststroke patients. Schmid et al. (2012) produced Level I evidence through a prospective randomized pilot study to evaluate the effects of a yoga-based intervention (2×/wk for 8 wk) on balance, balance self-efficacy, fear of falling, and QOL after stroke. The study found that participants in the therapeutic yoga intervention significantly improved in balance scores between baseline and the 8-wk mark. Immink et al. (2014) used an RCT with Level I evidence to assess the efficacy of yoga for motor function and balance, mental health, and QOL outcomes in people with chronic poststroke hemiparesis. Yoga intervention was administered once per week for 90 min. The BBS outcomes revealed no significant main effects or interactions with a regression model that accounted for 80% of the variance. However, the study found significant improvement in perceived motor function on the Stroke Impact Scale (Version 3.0; Duncan et al., 2003) for participants who received the yoga intervention. Improvements in motor function and balance observed by patients in their ADLs were not captured with motor function measures. In summary, with the different outcomes regarding significant improvement in 1 of the Level I studies, these 2 studies present limited evidence.
Dementia and Alzheimer’s Disease–Type Dementia
Three studies assessed the effectiveness of yoga in patients with dementia and AD-type dementia (Fan & Chen, 2011; Gallego et al., 2011; McCaffrey et al., 2014). In a Level III study, Fan and Chen (2011) examined the effects of the Silver Yoga (SY) exercise program in elderly people with dementia living in long-term care facilities. After 12 wk (3×/wk) of the SY exercise program, scores on the one-leg stand test to assess balance were significantly improved for the experimental group. Gallego et al. (2011) analyzed the effects of a hatha yoga program on patients with AD using the Tinetti Scale in a Level III study. The participants participated in hatha yoga classes 2 times per week for 12 wk, and the study reported improvements in positioning, movement skills such as balance, understanding of instructions, and confidence. McCaffrey et al. (2014) examined the feasibility of older adults with AD in completing the Sit ‘N’ Fit Chair Yoga Program in a Level III study (twice per week for 8 wk). Outcomes were measured using the BBS. All participants completed the program, and positive changes were seen across all physical measures, with improvements in balance being statistically significant. These studies present strong evidence with 2 quasi-experimental studies (Level III) and a single-group nonrandomized design study (Level III).
Multiple Sclerosis
Four articles addressed MS. Ahmadi et al. (2013) used a Level I RCT to determine the effect of hatha yoga sessions for 8 wk (3×/wk, 60–70 min/session) on balance for 31 female participants with MS. Ahmadi et al. (2010) used a Level I RCT and evaluated the effects of short-term yoga programs (3×/wk for 8 wk) on balance for 21 female participants. Guner and Inanici (2015) used a Level II case-control study to evaluate the effects of a 12-wk biweekly 60-min yoga program on balance and other factors for 8 participants with MS. Salgado et al. (2013) used a Level III pretest–posttest design study to evaluate the effects of a comprehensive 16-wk yoga program (5×/wk) for 6 men and 16 women with MS. All 4 studies found a significant improvement in balance scores, as measured by the BBS, compared with either a baseline measurement or a control group (Ahmadi, 2010, 2013; Guner & Inanici, 2015; Salgado et al., 2013). The combined strength of the levels of evidence from these studies, which consist of 2 Level I studies, 1 Level II study, and 1 Level III study, indicates strong evidence supporting the use of yoga for people with MS to improve balance.
Parkinson’s Disease
One study exploring the effects of yoga on balance in people with PD was examined. Colgrove and colleagues (2012) carried out a Level I randomized controlled pilot study with 13 participants who engaged in 60-min yoga sessions twice per week for 12 wk. At the end of the intervention phase, the yoga intervention group showed statistically significant improvements in balance. With only 1 Level I study, the findings present insufficient evidence supporting the use of yoga as an intervention for balance with people with PD.
Community-Dwelling Older Adults
Three studies examined the effects of yoga on balance for community-dwelling older adults: a Level I RCT (Tiedemann et al., 2013), a Level IV single-armed pilot study (Schmid et al., 2010), and a Level III cohort study (Kelley et al., 2014). The RCT, with 54 participants, ages 60–75 yr (mean [M] = 68), reported significant improvement in the yoga intervention group compared with the control group after 12 wk of yoga (2×/wk) in standing balance, sit-to-stand test, 4-m walk, and one-leg stand test with eyes closed. The pilot study reported significant improvements in static balance for the 14 participants, ages 69–87 yr (M = 78), who engaged in yoga for 12 wk (2×/wk). The cohort study, whose participants, ages 65–78 yr (M = 72), participated in yoga for 12 wk (2×/wk), reported significantly improved balance, mobility, and gait speed. These studies present moderate evidence as a result of the inclusion of 1 Level I study and varying levels of evidence in the other studies.
Risk of Bias
All 14 studies included in this systematic review were evaluated for risk of selection bias, performance bias, detection bias, attrition bias, and reporting bias with the use of methods described by Higgins et al. (2011). Potential for selection bias was further divided into random sequence generation and allocation concealment. Random sequence generation was not evident in 8 studies. Allocation concealment was not detected in 10 studies. Potential for performance bias was identified in 13 studies that lacked blinding of participants and personnel. Potential for attrition bias was minimal and noted in only 3 studies; in these 3 studies, participants withdrew after 6 wk of participation. Potential for reporting bias was identified in 4 of the studies. A risk-of-bias table (Table 2) was generated based on the AOTA (2015) guidelines, assessing each article’s study design and analyzing the outcomes.
Risk-of-Bias Analysis
Note. Categories for risk of bias are as follows: + = low risk of bias; ? = unclear risk of bias; – = high risk of bias. Risk-of-bias table format adapted from “Development of AMSTAR: A Measurement Tool to Assess the Methodological Quality of Systematic Reviews,” by B. J. Shea, J. M. Grimshaw, G. A. Wells, M. Boers, N. Anderson, C. Hamel, . . . L. M. Bouter, 2007, BMC Medical Research Methodology, 7, p. 10. https:/doi.org/10.1186/1471-2288-7-10
Discussion
The purpose of this systematic review was to examine the efficacy of yoga as an intervention for balance retraining in populations at risk for falls. The populations under investigation included people with TBI, CVA, dementia and AD-type dementia, MS, and PD as well as community-dwelling older adults because of a demonstrated increased risk for falls as a result of impaired motoric skills contributing to balance dysfunction in these groups. With this cumulative population in mind, 14 articles were evaluated. Of these articles, 6 were Level I evidence, 1 was Level II, 5 were Level III, 1 was Level IV, and 1 was Level V. Of the 14 articles evaluated, 13 showed evidence that yoga had a positive impact on balance in the population at risk for falls. The remaining article found observable improvements; however, it lacked statistical significance in improved balance scores.
The study finding no significant improvement in balance, Immink et al. (2014), addressed stroke. This RCT administered yoga once a week for 10 wk and failed to achieve statistically significant improvement in functional outcomes for mobility and balance with the yoga intervention group. This result was possibly a result of the study’s limited once per week frequency of intervention. In addition, participants reported observable improvements in balance while engaging in ADLs; however, these improvements were not captured with the set of motor function outcome measures used in the study. These motor function outcome measures may have lacked sensitivity in capturing the perceived gains of the participants.
Limitations
Common limitations of the 14 studies assessed in this systematic review include small sample size (5 studies), lack of random sampling (9 studies) or blinding (13 studies), and lack of control group (8 studies). Fewer than half of the studies evaluated qualified as Level I. Additional limitations were including only articles in English, limiting the article search to three databases, and having too few studies for TBI or PD to obtain clear classifications. Therefore, the addition of more rigorous studies would provide a deeper understanding of the relationship between yoga and balance among people at risk for falls, especially those with TBI and PD, for occupational therapy practitioners who are interested in using yoga as an intervention. In addition, the studies that aided in the final conclusion of this systematic review did not assess retention of gains from yoga after discharge from the study. Incorporating such an analysis would greatly enhance the understanding of the clinical significance of the use of yoga as a modality to address development and maintenance of skills versus a modality that would help people regain and retain skills over time.
Implications for Occupational Therapy Practice and Research
The pooled data of the 14 studies indicate that engaging in yoga was beneficial for all participants after CVA, dementia and AD-type dementia, and MS, as well as participants who were community-dwelling older adults who were at risk for falls. This improvement potentiates the use of the old and widely used practice of yoga as an intervention to strengthen and improve balance. However, improving a person’s balance is not the only important factor in preventing falls. Schmid, Van Puymbroeck, et al. (2016) reported that in addition to improving balance, providing occupational therapy education to increase a person’s awareness of fall risk was pivotal in reducing falls. Previous studies have shown that yoga without education to reduce fall risk or education without yoga did not reduce falls overall for people with chronic stroke (Falk-Kessler et al., 1991; Schmid et al., 2012). However, the combination of yoga and education resulted in a significant reduction in falls (Schmid, Van Puymbroeck, et al., 2016). This finding indicates that the use of yoga as a resource for people with CVA, along with increasing awareness of fall risk factors, is most beneficial in decreasing the frequency of fall-related injuries and improving quality of life. Further research is needed to assess the validity of an intervention program that combines the use of yoga with fall prevention education in other populations such as people with dementia, MS, or PD and community-dwelling older adults.
The findings of this review have the following implications for occupational therapy practice and research:
Yoga has the potential to be an effective modality for use in occupational therapy intervention for improving balance in people with CVA, dementia and AD-type dementia, and MS as well as community-dwelling older adults at risk for falls when it is administered at least twice per week for at least 8 wk.
More studies need to assess the combination of yoga with occupational therapy intervention targeted toward fall risk education for populations other than people with CVA, such as people with TBI, dementia and AD-type dementia, MS, and PD and community-dwelling older adults, for reducing falls overall.
Future higher level studies need to be completed to provide more definite conclusions regarding the effectiveness of the use of yoga as an intervention to improve balance, particularly for people with TBI and PD.
Retention of gains over time after discharge from yoga needs to be included in future studies to better inform practitioners and guide clients in the specific benefits of yoga for maintenance of gains.
Assessing the length, frequency, and type of yoga programs that are most effective would provide and validate the benefits of yoga for precise neuromuscular impediments of known etiology.
Conclusion
This systematic review examined the efficacy of yoga as a neuromuscular intervention with community-dwelling populations at risk for falls. The purpose was to understand the salutary benefits of yoga with clients who are at risk for falls because of neuromuscular issues to determine its utility for use in occupational therapy intervention. Benefits of yoga included improved posture control, improved flexibility of mind and body, relaxation, and decreased anxiety and stress. The review found moderate evidence to support the use of yoga to decrease the risk of falls among community-dwelling older adults and people with CVA, dementia and AD-type dementia, and MS. Studies involving people with TBI and PD did not include strong enough evidence to be able to make a clear classification.
Footnotes
Acknowledgments
The authors thank Janet Burk and Miranda James for their contributions to this review. This study was conducted at University of Texas Medical Branch, Galveston.
*
Indicates studies that were systematically reviewed for this article.