
Abstract
Postconcussion syndrome (PCS) affects physical, cognitive, and emotional functioning. Existing reviews of interventions to address PCS are limited to psychological and rehabilitation interventions and to child and adolescent populations. We conducted a systematic review integrating current evidence about interventions for adults with PCS. The inclusion criteria were intervention studies of adults (ages ≥18 yr) with PCS that evaluated recovery from PCS symptoms and focused on functional outcomes; 10 studies met the criteria. Included studies demonstrated medium to high levels of evidence and investigated psychotherapy, counseling, social support, self-management strategies, individualized rehabilitation, hyperbaric oxygen interventions, and group-based cognitive–behavioral therapy. Outcomes included reduced postconcussion symptoms, improved cognitive function, enhanced quality of life, and increased community integration. The evidence supports psychotherapy, counseling, and social support interventions as being beneficial for cognitive and emotional functions in adults with PCS.
Increased awareness about concussions has contributed to a growth in research addressing this topic (Bonds et al., 2014). One emerging emphasis is on the persistent residual symptoms of concussions, referred to as postconcussion syndrome (PCS). The Centers for Disease Control and Prevention estimated that 1.4 to 3.8 million concussions occur each year in the United States (Laker, 2011). Although studies of PCS have reported major differences in the incidence of this syndrome among people with concussions, the most commonly reported incidence is between 10% and 15% of concussions (Jotwani & Harmon, 2010; Prigatano & Gale, 2011). Lingering PCS symptoms may last for months after a concussion and can compromise daily life participation (Lundin et al., 2006; Røe et al., 2009).
Occupational therapy emphasizes participation in daily life for people with head injury as an important intervention outcome (Golisz, 2009). There is a lack of comprehensive systematic reviews integrating evidence about interventions for adults with PCS. The objectives of this review were to search the current literature systematically and to synthesize findings objectively on different interventions addressing physical, cognitive, and emotional functioning in adults with PCS. The intent was to identify interventions that have produced favorable outcomes in reducing PCS symptoms and supporting participation in daily activities.
Background
Occupational therapy practitioners contribute to the fulfillment of participation in daily life for people with many conditions, including concussions and other forms of mild traumatic brain injury (mTBI; Law, 2002). Participation in daily life includes many areas of occupation, such as activities of daily living (ADLs), work, education, and social participation (American Occupational Therapy Association, 2014). PCS affects different aspects of participation and should be addressable through individualized occupational therapy interventions. Occupational therapy practitioners work with people who have PCS to manage symptoms and hasten a return to daily life activities by designing interventions meeting the unique needs and abilities of each individual. Identifying evidence-based updates for PCS management provides practitioners with an opportunity to assist their clients more effectively. Using individualized interventions paired with new evidence, occupational therapy practitioners can support people with PCS as they face challenges to participation caused by diverse and lingering symptoms.
PCS is defined in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM–IV) as three or more symptoms that persist at least 3 mo after the precipitating concussion event (American Psychological Association, 1994), although researchers have considered symptoms to be persistent as early as 10 days (McCrory et al., 2013) or 28 days (Rose et al., 2015) after concussion. Symptoms of PCS vary in frequency and duration and may include headache, fatigue, dizziness, irritability, sleep disturbance, reduced concentration, impaired memory, sensitivity to light and noise, slowed thinking, and anxiety (Ryan & Warden, 2003). The vast majority of concussion symptoms resolve within 10 days after injury (McCrory et al., 2013), but a subgroup of people with concussion experience symptoms for weeks or months and thus meet the criteria for PCS (Røe et al., 2009). The persistent symptoms of PCS cause physical discomfort, increase the risk of emotional sequelae, and limit participation in daily activities (Lundin et al., 2006).
PCS adversely influences participation in ADLs and quality of life in people of all ages, including adults. The prevalence of PCS symptoms in adults has been estimated at 6%–30% at 3 mo and 1%–23% at 6 mo after a concussion (Røe et al., 2009; Spinos et al., 2010). Persistent concussion symptoms can be challenging to manage, affecting the person’s capability to assume a daily routine, keep a job, and engage in leisure activities (Bottari et al., 2008). For example, driving a motor vehicle requires full attention and concentration, and impaired concentration and slowed reaction time after a concussion increase the risk of a motor vehicle crash, endangering the driver, passengers, and others in the community. The repercussions of PCS for adults’ daily routine and work productivity should not be underestimated; therefore, providing education and support for seeking medical advice is important.
Management of PCS includes a combination of medical, cognitive, and rehabilitation strategies that target lingering symptoms. No comprehensive reviews have attempted to establish the outcomes of interventions for working adults in terms of PCS symptom resolution and functional improvements. Previous reviews that addressed PCS management were limited to a specific intervention type, such as psychological interventions (Al Sayegh et al., 2010) or rehabilitation interventions (Leddy et al., 2012), and were restricted to specific age groups, often children and adolescents (Gilmore et al., 2015). Adults over age 18 represent an important population of people with concussion, and yet no systematic reviews have endeavored to integrate the evidence on effective PCS interventions for this population. In addition, the role of occupational therapy in the management of PCS has not been clearly defined in the literature.
We conducted a systematic review of the literature to provide occupational therapy practitioners and other health professionals with access to current evidence on effective interventions for adults with PCS. The research question was as follows: What evidence supports the effectiveness of different intervention strategies for adults with PCS? We hypothesized that a comprehensive systematic review of published studies would identify all interventions effective in attenuating PCS symptoms and improving participation in ADLs.
Method
Search Strategy and Data Sources
We applied the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for structured implementation of the systematic review process (Moher et al., 2009). The review included comprehensive electronic and manual searches for articles published between 2005 and 2015 in which PCS was the primary focus. This 10-yr period marks a significant increase in research studies addressing PCS.
The electronic search was led by a librarian coauthor (Julie Hartwell) using a combination of key words and search terms (Table 1). The main databases used in this review were PubMed, CINAHL, PsycINFO, ProQuest, and OTseeker. Filters for data range, language, and age were applied to retrieve appropriate studies. Study design filters were applied when available to locate randomized controlled trials (RCTs). Database search results were exported and saved to a citation management tool for review. The manual search was conducted by examining bibliographic lists of included articles and other reviews.
Key Words and Search Terms for the Systematic Review of Interventions to Address the Needs of Adults With PCS
Note. PCS = postconcussion syndrome; TBI = traumatic brain injury.
Inclusion and Exclusion Criteria
Articles eligible for inclusion in the review involved studies with participants ages 18 or older with a PCS diagnosis. Disparities exist in the definition of PCS, with two medical classification systems—the International Classification of Diseases (10th ed.; ICD–10; World Health Organization, 1992) and the DSM–IV—establishing different diagnostic criteria. Both ICD–10 and DSM–IV diagnostic criteria were used in this review to control for the inconsistencies in defining PCS in the literature. Many intervention studies used an established diagnosis of mTBI, not PCS, to define their target sample; studies of participants with mTBI who had persistent concussion symptoms were included in this review. A full list of the inclusion and exclusion criteria appears in Table 2.
Inclusion and Exclusion Criteria
Note. mTBI = mild traumatic brain injury, PCS = postconcussion syndrome.
Eligibility criteria also included published studies written in English that addressed medical, rehabilitative, cognitive, or supportive therapy for PCS with outcome measures of PCS symptoms, functional performance, or participation in ADLs. The primary outcomes in this review were number and category of PCS symptoms, because lingering PCS symptoms are the main underlying cause of physical and emotional challenges for affected individuals. The secondary outcomes were functional performance of daily activities and related outcomes such as community integration and quality of life. These outcomes are also important and reflect the impact of PCS on the individual’s ability to resume a daily routine and engage in activities after injury.
The research team examined the abstracts of all studies that resulted from the electronic and manual searches for initial review and screening to determine eligibility for inclusion. Articles that could not be assessed on the basis of title or abstract content were reviewed in full text. The full text of articles meeting inclusion criteria on the basis of the initial review and screening was downloaded for further analysis.
Quality Appraisal and Level of Evidence
We evaluated quality and level of evidence for all included studies. We appraised quality on the basis of study design. We used the 11-item Physiotherapy Evidence Database (PEDro) scale for assessing the quality of randomized controlled studies (Moseley et al., 2002). RCTs with a PEDro score of 9–11 were considered excellent quality; 6–8, good quality; 4–5, fair quality; and <4, poor quality (Teasell et al., 2013).
For included studies that did not use an RCT design, we used the nine-item Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomized and observational studies (Wells et al., 2009). Studies with an NOS score of 7–9 were considered excellent quality; 4–6, good to fair quality; and 0–3, poor quality.
We also assessed the level of evidence for included studies using the Oxford Centre for Evidence-Based Medicine (OCEBM) guidelines for levels of evidence (Howick et al., 2011). The OCEBM levels range from Level 1, representing systematic reviews, to Level 5, denoting mechanistic reasoning. All included studies were assigned a number indicating the level of evidence.
Results
Search Results
Systematic electronic and manual searches yielded 158 studies from PubMed, CINAHL, PsycINFO, and the Cochrane Libraries. The initial review of titles and abstracts led to the exclusion of 95 articles. The remaining 51 articles were reviewed in full text, and 10 articles met all inclusion criteria. Figure 1 presents the PRISMA flowchart of search results and article selection.
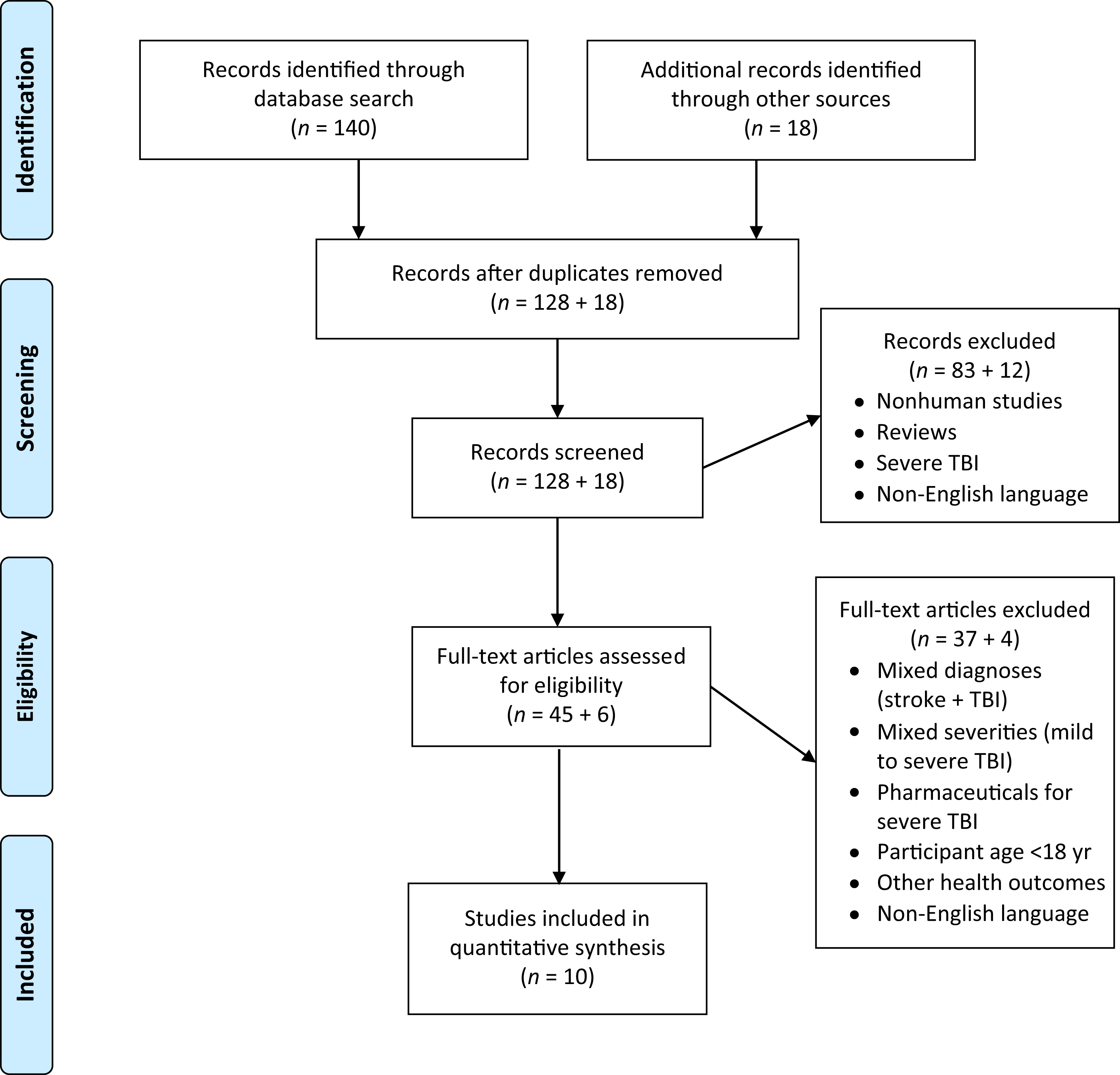
Flowchart of search results and article inclusion.
Included Studies
The 10 studies included for analysis in this review had varying sample sizes (range = 20–395 participants) and number of participants per group. The studies involved a total of 858 adults with concussion or mTBI that resulted in persistent concussion symptoms. The mean age of all participants was 35 yr (mean [M] age range = 23–47 yr). The majority of participants were men (M = 65%, range = 25%–100%) and had been employed before the injury (M = 78%, range = 30%–100%). Participants were mostly civilians (n = 675) in seven studies and mostly military personnel (n = 183) in three studies. Main causes of the concussions or mTBI included motor vehicle crashes and falls for civilian participants and improvised explosive device blasts for military personnel. The study designs also varied; 7 were RCTs, and 3 used nonrandomized designs, including 1 pretest–posttest, 1 cohort, and 1 cross-sectional design. All included studies used prospective data collection, and a variety of instruments were used to evaluate intervention outcomes.
Outcomes Measured
The outcomes of interest in this review were PCS symptoms and functional performance. Eight studies focused on evaluating all PCS symptoms (Bergman, 2011; Cifu et al., 2014; Elgmark Andersson et al., 2007; Kjeldgaard et al., 2014; Miller et al., 2015; Moore et al., 2014; Rees & Bellon, 2007; Wolf et al., 2012). Two studies examined only one category of PCS symptoms, either cognitive symptoms (Boussi-Gross et al., 2013) or emotional and behavioral symptoms (Tiersky et al., 2005).
Included studies evaluated a variety of functional outcomes, including functional health and well-being (Elgmark Andersson et al., 2007; Kjeldgaard et al., 2014; Miller et al., 2015; Moore et al., 2014), participation in ADLs (Cifu et al., 2014), and community integration (Elgmark Andersson et al., 2007; Moore et al., 2014; Tiersky et al., 2005). Some studies evaluated quality of life after implementation of the intervention (Boussi-Gross et al., 2013; Cifu et al., 2014; Elgmark Andersson et al., 2007; Miller et al., 2015).
Quality and Level of Evidence of Included Studies
The quality of included studies ranged from fair to excellent (Table 3). The 7 RCTs had PEDro scores of 5–10 points, indicating fair to excellent quality (Boussi-Gross et al., 2013; Cifu et al., 2014; Elgmark Andersson et al., 2007; Kjeldgaard et al., 2014; Miller et al., 2015; Tiersky et al., 2005; Wolf et al., 2012). Elgmark Andersson et al. (2007) was the lowest scoring RCT, with 5 points for criteria met; this study had a high risk of bias (including attrition, performance, and reporting bias) for one or more key PEDro domains (Higgins et al., 2011). The 3 nonrandomized studies had NOS scores of 5–8, indicating good to high quality (Bergman, 2011; Moore et al., 2014; Rees & Bellon, 2007). The included studies had moderate to high scores on methodological research implementation. The level of evidence ranged from fair (Level 4) to high (Level 2) based on the OCEBM guidelines.
Quality Appraisal of All Included Studies
Note. + = meets the established criterion; − = does not meet the established criterion; PEDro = Physiotherapy Evidence Database.
Intervention Content
We grouped interventions into five categories: (1) psychotherapeutic interventions, (2) social work interventions, (3) rehabilitation and individualized interventions, (4) self-management strategies, and (5) hyperbaric oxygen (HBO) therapy. Three studies included psychotherapeutic interventions (Kjeldgaard et al., 2014; Rees & Bellon, 2007; Tiersky et al., 2005), 4 RCTs tested the efficacy of HBO therapy (Boussi-Gross et al., 2013; Cifu et al., 2014; Miller et al., 2015; Wolf et al., 2012), and the 3 remaining studies evaluated the effectiveness of a social work intervention (Moore et al., 2014), individualized rehabilitation (Elgmark Andersson et al., 2007), and self-management strategies (Bergman, 2011). The control group in all included studies received either a different dose of the intervention being tested or conventional medical care. We provide a brief discussion of these interventions to offer insights into the effectiveness of each for adults with PCS.
Psychotherapeutic Interventions.
Psychotherapeutic interventions included psychodynamic, psychoanalytic, cognitive, and behavioral therapies. Three studies evaluating psychotherapeutic intervention strategies had good quality (Kjeldgaard et al., 2014, PEDro score = 8; Rees & Bellon, 2007, NOS score = 5; Tiersky et al., 2005, PEDro score = 8).
Two studies evaluated the effectiveness of cognitive–behavioral therapy (CBT), which substitutes maladaptive patterns of thinking and behavior with desirable patterns. Tiersky et al. (2005) conducted an RCT to test the effectiveness of individualized CBT with a sample of 20 adults (M age = 47) with PCS. The intervention group received 33 sessions of CBT over 11 wk. Individualized CBT led to a significant decrease in PCS symptoms and an increase in emotional functioning (Tiersky et al., 2005). Kjeldgaard et al. (2014) conducted an RCT with 90 participants (M age = 34) with mTBI who had lingering headaches. The intervention group received nine weekly sessions of group-based CBT. Group-based CBT did not alter postconcussion headaches, although it did yield improvements in quality of life, psychological distress, and overall symptoms (Kjeldgaard et al., 2014).
The third study of a psychotherapeutic intervention strategy evaluated the effect of psychotherapy coupled with counseling on recovery from PCS (Rees & Bellon, 2007). The researchers conducted a longitudinal pretest–posttest study with 20 adults with PCS (M age = 31). Both psychotherapy and counseling yielded a significant reduction in postconcussion symptoms, including agitation, irritability, and suicidal thoughts, and improvements in cognitive and affective symptoms. These interventions used a holistic approach with multiple therapeutic strategies, including sessions in which information was given, counseling based on client-centered CBT was used, and problem-solving strategies were practiced.
Social Work Interventions.
Social work services include linking clients to support groups and counselors to expand clients’ social support network. One study with excellent quality (Moore et al., 2014, NOS score = 7) found that providing social work interventions led to improvements in symptoms after a concussion. Moore et al. (2014) tested the effectiveness of the Social Work Intervention for Mild Traumatic Brain Injury (SWIFT) program with 64 adults (M age = 40) with mTBI. The intervention group received the SWIFT program and the control group treatment as usual. The SWIFT program strategically provided clients with reassurance, education, and follow-up guidelines, leading to greater use of medical services. The intervention group maintained preinjury community functioning, whereas the control group significantly declined in social functioning and community interactions. These findings suggest that social work interventions can help people with mTBI and postconcussion symptoms resume roles in their community.
Self-Management Strategies.
Self-management strategies are techniques clients can use to reduce the effects of residual illness on daily functioning and quality of life. One study with high quality (Bergman, 2011, NOS score = 8) explored different self-management strategies used by adults (M age = 40) who had prolonged symptoms after concussion. Bergman (2011) recruited 30 participants with symptomatic mTBI and 30 control participants without head injury. Participants with mTBI reported that self-management strategies were effective in relieving symptoms. In addition, there was a significant relation between overall reports of being bothered by symptoms and the use of self-management strategies such as activities or thoughts (e.g., make a list, use a calendar, rest), complementary therapies (e.g., prayer, relaxation), and exercise. Participants with PCS symptoms were more likely to use self-management strategies compared with control participants, and these strategies led to symptom relief and reduced symptom severity.
Rehabilitation and Individualized Interventions.
Rehabilitation and individualized interventions have proved effective in addressing functional concerns related to many disorders, and 1 study with fair quality (Elgmark Andersson et al., 2007, PEDro score = 5) evaluated the benefits of early rehabilitation intervention (including occupational therapy, physical therapy, and social work) for adults with PCS. Elgmark Andersson et al. (2007) conducted an RCT with 395 participants (M age = 33) with mTBI, 263 who were examined by rehabilitation professionals and 131 who received regular care. Individualized intervention did not appear to improve symptoms 1 yr after injury compared with the control condition. This study has important limitations, including a high dropout rate and variability in duration of baseline evaluation, so a conclusive determination about the effectiveness of individualized rehabilitation for PCS is not possible.
Hyperbaric Oxygen Therapy.
HBO therapy involves inhaling oxygen-enriched air in a closed chamber with increased atmospheric pressure (Gill & Bell, 2004). The human lungs absorb more oxygen under these conditions, and more oxygen in the bloodstream is hypothesized to trigger the release of growth factors and thus support healing (Tibbles & Edelsberg, 1996). Four RCTs with high-quality PEDro scores (9–10) tested HBO therapy with people with PCS, mainly military personnel (Boussi-Gross et al., 2013; Cifu et al., 2014; Miller et al., 2015; Wolf et al., 2012). Of the 3 studies, 3 did not show significant improvements after HBO therapy (Cifu et al., 2014; Miller et al., 2015; Wolf et al., 2012). The intervention groups received varying doses of HBO therapy between 1.5 and 2.4 absolute atmospheric pressure (ATA) units (2 ATA = twice the atmospheric pressure at sea level). The intervention did not yield any significant improvements or differences between intervention and control groups.
One HBO intervention study (Boussi-Gross et al., 2013), however, reported significant differences between the study groups. Boussi-Gross et al. (2013) conducted an RCT with a crossover design in a sample of 56 adults (M age = 44) with PCS. The intervention group was evaluated once after 2 mo of HBO therapy, and the crossover group was evaluated twice: once after a 2-mo control period and once after subsequent 2-mo HBO therapy. Both groups received 40 HBO sessions at 1.5 ATA. All participants with PCS experienced significant improvements in cognitive functioning and quality of life compared with the control period.
Discussion
Reports of therapies used to manage PCS abound in the literature. Among the most frequently prescribed interventions are physical and cognitive rest and exercise. Rest is important after injury because physical exertion after a concussion leads to exacerbation of symptoms (Majerske et al., 2008; Moser et al., 2012). After adequate rest, light aerobic exercise, such as walking on a treadmill or stationary cycling, has been recommended to further reduce symptoms (Leddy et al., 2016). Studies examining these interventions were not included in this systematic review because they did not meet our rigorous eligibility criteria. For example, this review included only studies focusing on the adult population and excluded studies with children or adolescents (e.g., Majerske et al., 2008; Moser et al., 2012). Interventions that mainly focus on rest followed by light exercise are commonly used for the management of PCS, and if combined with some of the interventions presented in this review, they may yield greater benefits for adults living with lingering PCS symptoms.
This review examined the evidence supporting interventions effective in addressing the needs of adults with PCS. The findings of this review provide support for our hypothesis because we identified interventions effective in attenuating PCS symptoms and improving participation in ADLs. Interventions demonstrating significant positive outcomes included psychotherapeutic interventions, social work interventions, and self-management strategies. Psychotherapeutic and social work approaches were the most effective interventions for adults with PCS. CBT and psychotherapy educate and empower clients to understand and cope with their challenging health problems (Anson & Ponsford, 2006). These therapeutic strategies validate clients’ complaints of persistent symptoms and aid them in identifying appropriate mechanisms to cope with lingering symptoms (Potter & Brown, 2012). Social work interventions were also beneficial for adults with PCS; social workers provided PCS clients with education about lingering symptoms, the recovery process, and coping strategies to manage prolonged symptoms. Other research has confirmed a positive effect of social work interventions on psychological recovery after severe brain injury (Gan et al., 2006).
Self-management interventions have been reported to be beneficial for people with various health conditions (Funnell, 2010). Other studies have evaluated the effectiveness of self-management strategies for people with mTBI (Kendrick et al., 2012) and acquired brain injury (Brenner et al., 2012; Damush et al., 2011). These studies have yielded mixed results, but the majority have supported the effectiveness of self-management strategies for people with head injury. For example, 2 studies found that self-management strategies improved daily functioning (Kendrick et al., 2012) and enhanced self-efficacy, self-management behaviors, and specific aspects of quality of life (Damush et al., 2011). A third study, however, did not show similar benefits (Brenner et al., 2012). Self-management strategies may have promise; further studies are needed to confirm the effectiveness of such strategies for adults with PCS.
Studies that have specifically explored the effectiveness of occupational therapy and rehabilitation interventions for adults with PCS are limited. Only 1 intervention study was identified as using occupational therapy in the management of PCS (Elgmark Andersson et al., 2007). A scoping review of the occupational therapy literature on mTBI and PCS identified only 3 intervention studies that focused on occupational performance after injury (Cogan, 2014). These 3 studies tested the effectiveness of Cognitive Orientation to daily Occupational Performance (CO–OP; Dawson et al., 2009), multidisciplinary rehabilitation (Ghaffar et al., 2006), and a self-management program (Kendrick et al., 2012). CO–OP and self-management interventions yielded significant improvements in the occupational performance of participants with PCS. These studies did not meet the inclusion criteria for analysis in this review because they included participants with mixed diagnoses or severe head injury or adolescents. Although the evidence is limited on the effectiveness of occupational therapy for adults with PCS, clinical practice guidelines for mTBI management are available (Marshall et al., 2012) and provide occupational therapy practitioners and other health professionals with information about care for people with mTBI and, by extension, PCS.
Studies of HBO therapy yielded mixed results, with only 1 of 4 studies demonstrating a beneficial effect for adults with PCS (Boussi-Gross et al., 2013) and 2 studies showing greater improvements in PCS symptoms for the comparison group, who received 1.2–1.3 ATA, than the intervention group, who received 1.5–2.4 ATA (Miller et al., 2015; Wolf et al., 2012). These findings support use of lower pressure doses to test the efficacy of HBO therapy in future research.
Limitations
This review included studies that used a mix of research designs and analyses, with the majority having medium to high quality. Limitations of the reviewed studies involved small sample sizes (9 of the 10 studies had fewer than 100 participants), unequal gender ratios (the majority of participants were men, especially in military samples), and varied outcome measures, thereby limiting the ability to synthesize results across studies. However, this review integrates a variety of intervention strategies that have a beneficial effect on adults with PCS in terms of alleviating symptoms and improving functional performance. We recognize that our findings will be enhanced by future research examining the effectiveness of PCS interventions using large, representative samples.
Implications for Occupational Therapy Practice
PCS has diverse symptoms that adversely affect daily functioning and work productivity. Each person with PCS is unique, and understanding the experience of adults with persistent symptoms is an important first step toward designing an optimal intervention plan. The findings of this systematic review have the following implications for occupational therapy practice:
Occupational therapy practitioners should follow an individualized approach to the management of PCS, taking into consideration clients’ preferences and needs.
Occupational therapy interventions designed for adults with PCS should include education and counseling about persistent symptoms to enable clients to understand their situation and reduce the stress associated with lingering symptoms.
Interventions for adults with PCS should incorporate suggestions for self-management strategies to cope with symptoms and to be more active in everyday life.
Occupational therapy practitioners should consider referring clients with PCS to trained psychologists who are able to provide psychotherapeutic interventions such as psychotherapy and CBT.
Working as part of a multidisciplinary team promotes advocacy and interprofessional collaboration among occupational therapy practitioners and other health care professionals and assists clients with PCS to optimize successful management of their lingering symptoms and achieve a return to regular activities.
Implications for Future Research
Additional high-quality intervention studies of PCS management for adults are needed to confirm the findings reported in this review. Future studies of PCS interventions for adults should use a unified PCS definition and diagnosis (e.g., ICD–10 criteria), recruit larger samples, evaluate outcomes of functional performance and work productivity, and conduct repeated follow-up assessments. Future research should seek to develop and test the effectiveness of individualized, multidisciplinary interventions using a combination of strategies shown to be beneficial for adults with PCS.
Conclusion
The findings of this systematic review suggest that CBT, psychotherapy, social work, and self-management interventions are effective in the management of PCS and may be useful as adjunct therapies to enhance the common intervention practice of cognitive and physical rest followed by a graded aerobic exercise program used in the treatment of uncomplicated concussion. HBO therapy requires trained technicians, special equipment, and physical space to deliver, which can be expensive and less feasible in some medical settings. Psychotherapeutic interventions do not require specialized tools, although extensive and specialized training is required to provide them. CBT, psychotherapy, social work, and self-management interventions appear to be beneficial for adults with lingering postconcussion symptoms, perhaps by helping them understand their condition and supporting them to adopt alternative coping strategies to deal with persistent symptoms. Studies with rigorous designs are needed to evaluate the effectiveness of interventions, including occupational therapy interventions, for PCS in adults with mTBI or concussion.
Footnotes
*
Indicates studies that were systematically reviewed for this article.