
Abstract
Occupational therapy practitioners can improve the hotel experience of people with disabilities through advocacy, consultation with hotels, and direct intervention with clients.
People with disabilities travel for reasons similar to those of people with no disabilities, including for leisure and work participation (Shi et al., 2012). In addition, access to travel improves the quality of life of people with disabilities (Kinney & Coyle, 1992). Research demonstrates, however, that people with disabilities travel less often than people without disabilities (Cole et al., 2016). One barrier is that travel often includes a hotel stay and, despite improvements in hospitality services for people with disabilities since the initial passage of the Americans With Disabilities Act of 1990 (ADA; Pub. L. 101-336), hotel accessibility remains a challenge (Grady & Ohlin, 2009).
Research shows that people with disabilities face challenges related to the physical environment, accessibility, and poor customer service during hotel stays (Grady & Ohlin, 2009). Therefore, restrictive attitudes and the environment in hotels may limit participation for people with disabilities during their stays. This restricted participation may ultimately limit their engagement in occupations and decrease their quality of life. This perspective, stemming from Oliver’s (1995) Social Model of Disability, informs us that social disability does not result from a bodily impairment; instead, it occurs because of an interaction between the person and the environment. The Person–Environment–Occupation–Performance (PEOP) theoretical model (Baum et al., 2014) further supports this perspective by considering how personal factors intersect with environmental factors to influence occupational participation. The PEOP model adds the consideration of personal factors, including physiological, cognitive, spiritual, neurobehavioral, and psychological ones (Baum et al., 2014). The consideration of differences in personal factors, including type of disability, is important to understanding occupational participation. This holistic perspective provides guidance for occupational therapy practitioners who want to address travel with their clients.
We were unable to find research in the occupational therapy literature that has explored the experiences of people with disabilities during hotel stays. The majority of studies exist in the field of the hospitality and tourism (Cole et al., 2016; Poria et al., 2011; Shi et al., 2012) and have focused only on people with physical disabilities or on the managerial implications for hotels (Daniels et al., 2005; Darcy & Pegg, 2011). The literature lacks information that explores the diversity of disability experiences, the personal and environmental factors that affect occupational participation, and the impact on occupational participation of the intersection of personal and environmental factors. The primary purpose of this study was thus to explore how people with various disabilities experience hotel stays. The secondary purpose was to identify opportunities for occupational therapy intervention.
Method
Design and Procedure
To emphasize the perspective of people with disabilities, we chose a phenomenological approach involving individual in-depth interviews. The first author (Morgan R. Stasell), a graduate student at the time, conducted semistructured interviews with participants under the supervision of the second author (Molly M. Bathje), a faculty member with experience conducting research interviews. Stasell had received previous training in how to conduct interviews during graduate-level coursework and by conducting prior interviews with people with disabilities. Bathje provided feedback to Stasell about the interviews throughout the process. The interview guide was developed on the basis of a literature review and discussions with members of a disability advocacy organization. Two faculty members with experience working with the disability community and conducting qualitative research reviewed the guide. The interview guide questions are listed in Figure 1.
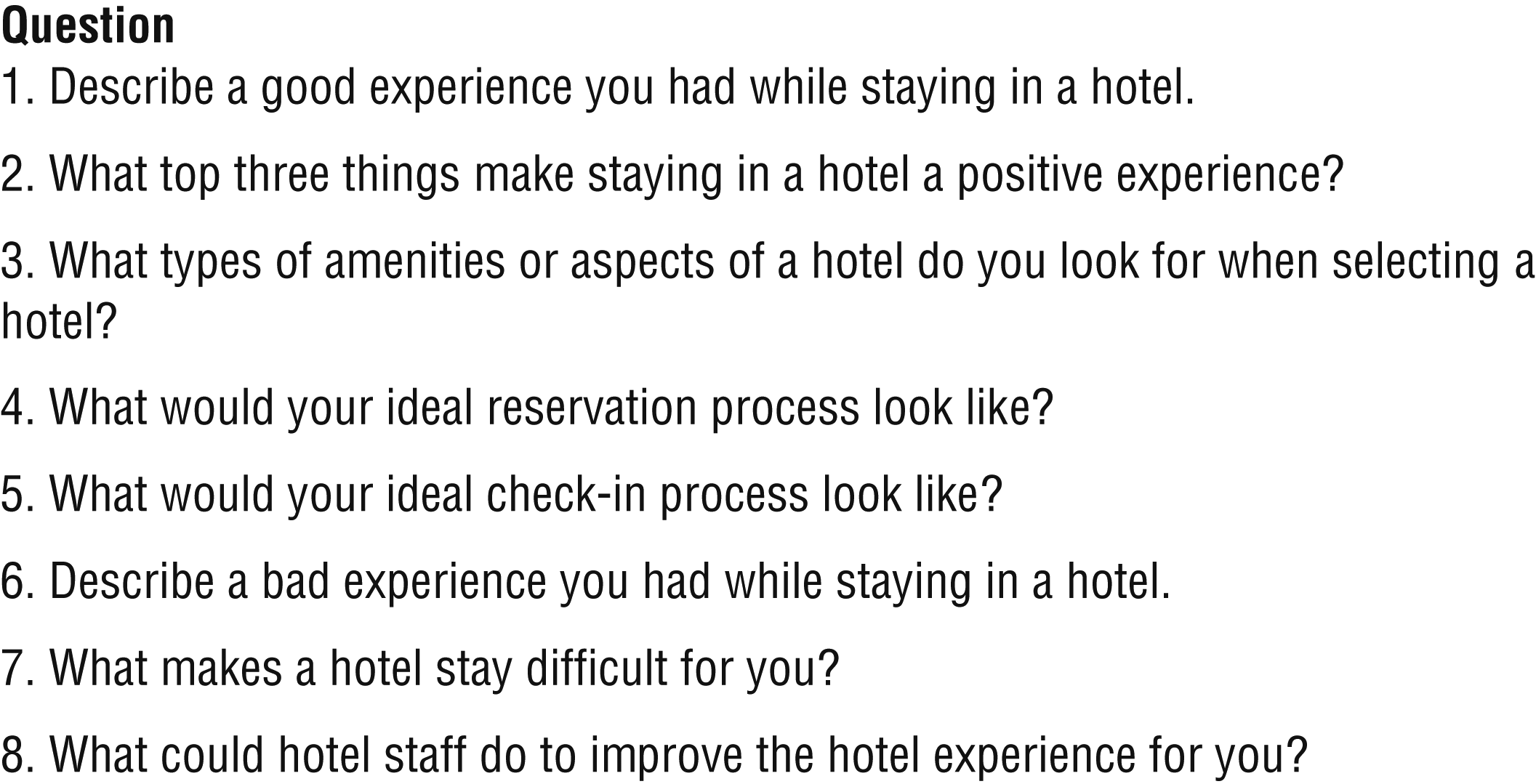
Semistructured interview guide.
The interviews, which lasted 50 min on average, occurred via secure video conferencing software, except interviews that required an American Sign Language interpreter, which occurred in person. Participants received the questions before the interview to encourage more robust answers. The study protocol was approved by the institutional review board of Rush University.
Participants
Participants with a variety of physical and sensory disabilities were recruited through a registry of people with disabilities at a local government organization, the authors’ personal connections, and contact with advocacy organizations. Eight participants completed interviews. One participant was known to the research staff from involvement in advocacy work. Participants were contacted via email, and the informed consent process was completed over the phone. To be eligible for the study, participants needed to (1) self-identify as a person with a physical or sensory disability, (2) have stayed in a hotel in the United States at least twice in the past year, (3) be at least age 18 yr, and (4) be their own legal guardian. For the purposes of this study, physical disabilities included any illness or bodily condition that affected physical functioning, and sensory disabilities encompassed anyone deaf, hard of hearing, blind, or with low vision.
Data Analysis
The data analysis involved the following six steps: (1) exploring researchers’ personal experiences with and biases toward the hospitality industry and people with disabilities, to increase reflexivity; (2) developing a list of statements in the verbatim transcripts that represented how the participants experienced hotel stays; (3) grouping significant statements into themes; (4) writing a textual description of what the participants had experienced; (5) writing a structural description of how the participants’ experiences occurred; and (6) writing a description of the essence of the participants’ experience in hotels that included both the what and the how of the experience (Creswell, 2013). Data analysis began after the first four participant interviews, using Dedoose software (Version 8.0.35; https://app.dedoose.com/App/?Version=8.0.35).
We reviewed the verbatim interview transcripts separately to identify significant statements. Next, we met to review the significant statements and, through discussion, developed agreement about which statements were significant. Over several subsequent meetings, we collaborated to combine the significant statements into themes. As Interviews 5 through 8 occurred, we followed the same iterative process for identifying significant statements separately, then meeting to discuss and agree on which statements should be included and grouping statements into existing or new themes. After reviewing the transcript of Interview 8, we agreed that no new themes were emerging and that data saturation had been achieved. Themes were further refined and considered across all transcripts. Stasell reviewed each theme and, for each, created a statement of essence, all of which were reviewed and agreed on by both authors.
Results
The 8 participants had a variety of disabilities; 5 had acquired disabilities and 3 had congenital disabilities. Four participants identified as male, and 4 identified as female. Their ages ranged from 37 to 72 yr. Table 1 contains a comprehensive list of participant demographic characteristics. Six themes arose from the data analysis process: (1) customer service, (2) reservation process, (3) built environment challenges, (4) traits and skills, (5) use of technology, and (6) safety and emergency preparedness. The sections that follow describe each theme.
Participant Demographics (N = 8)
Note. Pseudonyms were randomly assigned to participants.
Customer Service
Participants indicated that positive hotel experiences involved positive interactions with hotel staff. When asked what made a hotel stay successful, Susan explained, “[Hotel staff] don’t get shocked or look ‘off put’ if I come up to the desk or have a request, they seem knowledgeable when I ask them questions about a room, space, or need.” Participants revealed that hotel staff offering personalized service is important. Carl remarked, “We’re not all the same. . . . My disability is going to need something different than someone else’s disability.”
Several participants indicated that negative experiences resulted from poor communication and coordination between hotel departments. For example, participants discussed how, although the front desk was aware that someone with a disability was staying in the room, this was not communicated to housekeeping staff. Carl shared his experience of housekeeping staff rearranging personal care items after he set them up in certain locations to enable his independence:
Oftentimes, my work trips are one night, so it’s not an issue, but where I am on longer stays, multiple days for work or even, you know, for vacation purposes . . . cleaning staff [are] coming in and they want to put things in a certain way. They see the shampoo, and they’ll remove it from the shower area, put it back on the shelf, or put a new bottle out, which can be problematic.
Reservation Process
Participants’ preferences for making room reservations included using the phone, the hotel website, or third-party websites. Barriers to booking reservations through websites included incompatibility with screen readers and limited opportunity to explain individualized accessibility needs. Participants also reported encountering websites that lacked information on accessibility features, such as presence of a roll-in shower for guests in wheelchairs. Joe stated, “I like details. I like having more, you know, details [on] what the amenities are for accessible rooms.”
Participants reported that reserving a room over the phone can sometimes be problematic. Margaret shared that she is often quoted a higher price booking over the phone instead of online:
I tend to call. When I call, I know the price [from viewing the rates online] and how much it will cost me. And I ask them, “How much will you charge me for this room?” And they will tell me a different price. And I say, “Well, I have this price.”
Despite efforts to reserve accessible rooms in advance, participants stated they often did not receive them, likely because of hotels overbooking. Michael shared this experience:
This was an event where there are a number of wheelchair users for this conference, a program focused . . . on disability. So, of course, they didn’t have enough rooms and a friend of mine got the last accessible room.
Susan also highlighted the overbooking issue: “I think a good experience for me . . . is knowing that when I’ve requested a wheelchair-accessible room, I show up, and I actually get a wheelchair-accessible room.”
Built Environment Challenges
Some participants reported that accessible rooms often contain nonaccessible features. Michael questioned, “Why are they putting super-high beds into so-called ‘accessible rooms’ when the average wheelchair seat is somewhere between 16 and 20 inches off the ground?” Participants also described bathroom inaccessibility, such as a built-in shower bench placed on the side opposite the shower controls, flimsy shower benches, and showers that leaked. Joe spoke of this negative experience on the route to his accessible room: “We were going to this one particular section . . . and we found out that, ‘Oh, that there’s a problem. There are actually stairs in this section of the hotel.’”
Participants also mentioned that accessible rooms often lack desirable views and other attractive features. Susan stated, “I’ve had [accessible rooms] in beautiful places that are looking out at the air conditioner.” Some reported that hotels often offer only one type or class of accessible room. Michael pondered, “Why do some establishments only have a king bed in an accessible room, or why do others only offer a double bed? For my attendant? For my caretaker? I don’t have one yet.”
Traits and Skills
Participants described skills they used to manage their disability in hotels. They indicated that these skills developed naturally over time in response to their disability and experiences in the hotel environment. They said they preferred to act independently and engaged hotel staff for disability-related support as a secondary option or only for an initial orientation to the hotel. Cheryl stated, “I like to learn how to [navigate the hotel], so I can be more independent.”
All participants discussed using problem-solving skills to manage challenges. Those with sensory disabilities used lip reading, created “mental maps,” and used mobile technologies to navigate hotels. Joe discussed how he navigated around a “tight” accessible room he was sharing with multiple people in wheelchairs by coordinating maneuvers such as backing into and out of the room. Michael used problem-solving skills when the shower bench he requested was not provided:
So I noticed that the desk chair was of a plasticized and metal variety . . . and I lifted that up into the shower and then I transferred from my wheelchair onto that and precariously jumped back in my chair and lived life to the fullest.
Participants described how uncertainty and risk accompanied a hotel stay as a disabled person; however, they also described the various cognitive and psychological skills they used to anticipate, adapt to, and accept those risks. Joe mentioned how
I have to do a little bit more research . . . mostly calling but also like looking and seeing if I can find photos of like different rooms or even just asking the hotel, hotel management about the different [accessible] amenities.
Margaret shared that she now brings her own vibrating alarm clock instead of requesting one from the hotel because hotels have required her to leave her driver’s license with the front desk while borrowing the alarm clock:
[The hotel staff] had asked us to provide our driver’s license when we picked up the [deaf] equipment. That’s one disadvantage. I couldn’t drive, because they took [the license]. So now, we don’t bother asking anymore. We always bring our own alarm.
Participants described taking the perspective that sometimes a negative experience had more to do with external factors (e.g., noisy neighbors, a built environment determined by corporate brand) rather than the hotel’s staff. Shawn took the perspective that there are “both positive and negatives” involved in hotel experiences (e.g., the TV had captioning, but the captions were too small).
All participants discussed self-advocacy skills they used, including asking for help and seeking out hotel managers to discuss shortcomings and provide suggestions for improvement. Participants were knowledgeable about the ADA and its application to lodging facilities, enabling them to be self-advocates. Carl recalled asking for assistance at the breakfast buffet and noted that it is their “obligation under the ADA to provide assistance.”
Use of Technology
Participants emphasized technology, including websites and mobile apps, as an important part of their hotel experience. Carl stated,
I, as someone that uses assistive technology . . . use a screen reader on my phone, I should have that same ability and ease, you know, to make a room reservation or just to simply check rates and find out the different amenities that are available in a hotel.
Participants emphasized the need for a strong internet connection for web-based accessibility applications that increase independence. Shawn revealed, “They need to have good WiFi as well, [if I want to talk] to my friends or family on FaceTime.” Low-tech options for communication were valued as well. Margaret stated, “One of the nicest things they could have is a whiteboard and a marker, so that [I] can use it over and over again [to communicate].”
Safety and Emergency Preparedness
Participants with sensory disabilities shared the most experiences and thoughts about safety. Referring to guests with visual impairment and the need for emergency evacuation, Carl stated that “[guests] should know where the stairwell is; that that should just be basic [instruction].” Shawn also reported, “If I’m on the first floor, it’s more comfortable, because it’s easier to get out if there’s a fire.” Margaret emphasized the importance of a functioning visual smoke alarm for guests who are deaf. Shawn discussed hotel staff entering her room without her knowledge: “They could just enter any time they want. I didn’t like that. And that’s happened to a few deaf people at a conference. They just went in without letting me know.” Participants also suggested that hotel staff could better include guests with disabilities in their safety and emergency preparedness plans.
Discussion
The results of this study support previous reports indicating that people with disabilities experience challenges in hotels. Participants’ responses focused mainly on the challenges encountered in the environment (physical, social, and virtual), indicating the considerable role the environment plays. Participants in this study had long-term chronic conditions and would be considered part of the healthy population with disabilities, that is, people who have a stable, predictable future and do not require ongoing medical treatment (Goering, 2015). This population often finds that the disadvantages they face do not have anything to do with their body or condition; instead, they stem from environmental inaccessibility and negative societal attitudes (Goering, 2015). Participants in this study held this view and provided multiple suggestions for changes to the environment that would enable greater independence within hotels.
Our results also indicate that personal factors play a role in successful hotel stays. The participants described specific personal factors, including cognitive, psychological, and self-advocacy skills, that helped them respond to barriers and increase their occupational performance during hotel stays. The psychological skills they described enabled them to manage the stressors they encountered during hotel stays by placing the negative experiences within the larger context. Cognitive and self-advocacy skills helped participants make changes in their environment that supported their occupational participation. For example, when Michael did not have a shower bench, he adapted the desk chair to enable his participation. Cheryl asked hotel staff to provide way-finding assistance, thus using her skills to enhance her social environment to provide the support she needed to act independently. The PEOP model indicates that the performance of an occupation—in this case, staying in a hotel—enables participation in everyday living and contributes to a sense of well-being (Baum et al., 2014). It is clear that occupational performance and participation in hotel stays can be influenced, and potentially enhanced, by both personal and environmental factors (e.g., people with disabilities acquiring self-advocacy skills or hotel staff completing disability training).
The results of this study suggest that there are many opportunities for hotels to modify environmental factors that influence the hotel stays of people with disabilities. Training hotel staff in disability awareness and etiquette may help the staff create a welcoming and informed environment. Physical environment barriers may be reduced by involving people with disabilities in the design of spaces and selection of furnishings. Likewise, the virtual environment, such as the hotel’s website and app, can be improved by following online accessibility guidelines and eliciting feedback from users with disabilities.
Modifications to the environment may improve hotel stays, but such changes may be slow to occur and will likely vary among hotel chains. Therefore, focusing on personal factors is important. Participants’ descriptions of the skills they used to improve their hotel stays offer valuable information to other people with disabilities who want or need to stay in hotels. People with disabilities can learn these skills from peer mentors in the disability community who have traveled or from rehabilitation professionals who incorporate these skills into treatment plans.
Limitations
Limitations of this study include that the sample did not represent all disability groups and included only a narrow age range of participants, who were recruited from the Chicago metropolitan area. The scope of the study focused on hotel stays only in the United States, also limiting generalizability. Despite her training, Stasell may not have been successful in fully exploring the participants’ experiences or the participants may have felt uncomfortable fully disclosing experiences and emotions related to this topic.
Future Research
The results of this study, and the extant literature, indicate that further research on hotel stays for people with disabilities is warranted. This study is the first in the occupational therapy literature to explore this topic. Future research could include explorations of the capability of a disability training program for hotels to inform the industry on the needs of guests with disabilities, occupational therapy interventions on the development of skills required for hotel stays, and peer mentoring programs that link newly disabled clients to seasoned travelers with disabilities to facilitate skill and knowledge transfer. In addition, research focused on occupational therapy advocacy efforts to improve accessible lodging would be a valuable contribution to the literature.
Implications for Occupational Therapy Practice
Occupational therapy practitioners should support the participation of their clients with disabilities in hotel stays through addressing both personal and environmental factors by doing one or more of the following:
Advocating for accessible lodging and practices through legislative action (e.g., the ADA National Network; https://adata.org/)
Consulting with hotels on how to improve their customer service and accommodations for guests with disabilities
Providing interventions that focus on skills for successful hotel stays (e.g., knowledge of self-advocacy skills, navigating a hotel’s website using a screen reader).
Conclusion
Travel is an occupation in which recipients of occupational therapy services engage and on which they may want to focus in treatment. To effectively support their clients, occupational therapy practitioners must be informed about how personal and environmental factors affect hotel stays as well as how those factors interact throughout the hotel experience. This study provides the first information of its kind to inform occupational therapy practitioners about the hotel experience of people with disabilities. The results can guide practitioners in addressing the challenges related to hotel stays for people with disabilities by means of interventions that target both personal and environmental factors, including advocacy for accessible lodging and the integration of people with disabilities into the community, consultation with hotels on the needs of guests with disabilities, and direct intervention with clients who wish to travel.
Footnotes
Acknowledgments
Morgan R. Stasell acknowledges and thanks the Rush University Department of Occupational Therapy faculty, especially Evguenia S. Popova, Paula J. Costello, and Linda M. Olson, for their support and contributions to this research.