
Abstract
Occupational therapy practitioners can address barriers to expression of sexuality among adults with IDD as part of client-centered practice and support sexuality as part of the full human experience.
Sexuality is an important part of the human experience (World Health Organization [WHO], n.d.). Sexuality includes the physical encounter of sex and is also a form of expression, intimacy, and exploration (WHO, n.d.). It is expressed through relationships, roles, and actions (WHO, n.d.) and is linked to well-being (Diamond & Huebner, 2012). The relationship between sexuality and well-being holds true for people with and without disabilities (Lee et al., 2020).
Society lacks recognition of the importance of sexuality to the well-being of people with disabilities (McGrath & Sakellariou, 2016). There is a long history of legal, social, and cultural restriction of sexuality of people with intellectual and developmental disabilities (IDD), which are defined as limitations in mental functioning or adaptive behavior with a developmental onset (American Association on Intellectual and Developmental Disabilities, 2020). Throughout the 19th and 20th centuries in the United States, people with IDD were often institutionalized, resulting in isolation and restriction of their rights, including sexuality. In these settings, sexual expression was often misinterpreted and punished (Kempton & Kahn, 1991), with no acknowledgment or education about sexuality and lack of privacy.
During the deinstitutionalization period (1960s–1990s), people with IDD transitioned into community living with the goal of increasing community integration. Some of the first laws protecting the inclusion of people with disabilities were initiated. For example, the Education for All Handicapped Children Act of 1975 (Pub. L. 94-142), which later became the Individuals With Disabilities Education Act of 1990 (Pub. L. 101-476), and the Rehabilitation Act of 1973 (Pub. L. 93-112) required equal access to health care and education for people with disabilities (Wade, 2002). During this time, the disability rights movement emerged, advocating for equal and fair treatment of people with disabilities.
Despite legislative changes and advocacy work, sexuality and the sexual rights of people with disabilities were largely ignored or overtly restricted in legislation and policies. For example, some state laws prohibited people with IDD to marry and permitted involuntary sterilization of people with disabilities (Wade, 2002). Negative societal attitudes about people with disabilities and sexuality also continued to pervade policy and even health professions’ support of sexuality in people with disabilities, and these attitudes and their effects continue today (McGrath & Sakellariou, 2016).
Advocates have pushed for recognition of sexuality as part of well-being among adults with IDD. In a joint statement, the American Association on Intellectual and Developmental Disabilities and The Arc of the United States indicated that “Every person has the right to exercise choices regarding sexual expression and social relationships. The presence of IDD, regardless of severity, does not, in itself, justify loss of rights related to sexuality” (American Association on Intellectual and Developmental Disabilities, 2013, para. 3).
Despite limited access to comprehensive information regarding sexuality and lack of opportunity for sexual expression (Lafferty et al., 2012), studies have shown that up to 70% of people with IDD have engaged in sexual encounters (Siebelink et al., 2006). Research has also indicated that people with IDD are at risk for contracting sexually transmitted diseases and experiencing unwanted pregnancies (Sullivan et al., 2013). This risk demonstrates the need to improve access to information and opportunities to explore sexuality to improve safety. Despite calls to recognize adults with IDD as sexual beings, health care practices do not always bear out these principles (Eglseder et al., 2018; Hyland & McGrath, 2013; Schmidt et al., 2019).
Occupational therapy practitioners should conceptualize sexuality as part of a holistic approach to treatment (Sakellariou & Algado, 2006), but research has indicated that practitioners often do not address sexuality in practice (Hyland & McGrath, 2013; Young et al., 2020). Sexual activity and health maintenance are included in the Occupational Therapy Practice Framework: Domain and Process (4th ed.; American Occupational Therapy Association, 2020), supporting a focus on this aspect of well-being. Understanding the experience of sexuality among adults with IDD is crucial to effectively addressing sexuality in practice.
Little is known about the experience of sexuality from the perspective of adults with IDD to inform health care practices. The voice of people with disabilities, in general, is not included in the literature about sexuality (Lee et al., 2020). Literature specific to sexuality in people with IDD has focused on the barriers to sexuality and sexual knowledge (Lafferty et al., 2012) or has explored the impact of sex education curriculums to overcome these barriers (Blanchett & Wolfe, 2002; Schaafsma et al., 2015). These curriculums are often developed without input from people in the IDD community, and feedback from participants indicates that the content is too broad and does not focus on topics that they are most interested in, such as relationship building and mechanics of sex (Swango-Wilson, 2009).
Additionally, topics of biology and safety are of greater focus than the experience of sexuality as a whole (Sala et al., 2019). The inclusion of perspectives of people with IDD in research that informs practice is essential to its quality (Goering, 2015; Kitchin, 2000; Stone & Priestley, 1996). Calls are increasing for the incorporation of lived experience of disability in the occupational therapy literature (Kielhofner, 2005). The purpose of this scoping review was to summarize what is known about the lived experience of sexuality among adults with IDD from their perspective to inform occupational therapy practice and research.
Method
Study Design
We chose scoping review methodology because it facilitates the review of a broad topic area and helps identify gaps in the literature. In this review, we followed Arksey and O’Malley’s (2005) methodology, which includes the following stages: Stage 1, identifying the research question; Stage 2, identifying relevant studies; Stage 3, study selection; Stage 4, charting the data; and Stage 5, collating, summarizing, and reporting results. The process was also guided by the checklist from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR; Peters et al., 2015).
Data Selection and Analysis
Articles were included if they were published in English, were peer reviewed, and described either the experience of sexuality from the perspective of adults with IDD or observations of expressed sexuality from caregivers. Caregiver reports were included to allow for people with limited verbal skills to share their experiences. Attitudes toward sexuality are culturally based; therefore, we limited the search to articles published after 2008 and initially limited the search to articles published in the United States. Initial results of the literature search did not identify enough articles published in the United States (n = 6) to substantiate a scoping review. Therefore, we expanded the inclusion criteria to articles published in Canada, Ireland, and the United Kingdom on the basis of the cultural attributes of these countries being most similar to the United States. Articles focused on criminal sexual behavior or sexual violence were not included because they emphasize culturally deviant behaviors.
A research librarian completed the data search in February 2019 using CINAHL, Scopus, PubMed, and PsycINFO. The search terms included three concepts: intellectual disability, sexual activity, and feelings/opinions. Search results were imported into Rayyan (http://rayyan.qcri.org) data search software (Ouzzani et al., 2016) for review.
After reviewing initial search results (N = 1,365), we excluded articles if they were duplicates, were published before 2008, were not peer reviewed, or were not in English. The remaining articles (n = 868) were divided into two groups, on the basis of year of publication, and two teams of two researchers (each including a faculty member and graduate student) completed title and abstract reviews to determine eligibility. Both members of the research teams voted to include or exclude articles. Fewer than one-tenth of articles were voted in disagreement, which was resolved by discussion to reach unanimous agreement by all researchers.
Next, remaining articles were divided into two groups alphabetically by the last name of the first author, and each research team completed full-text reviews on half of the 93 articles remaining. Each member of the research team voted to include or exclude. Disagreements were resolved by discussion and unanimous agreement by all researchers. During full-text reviews, articles not published in the United States were excluded, resulting in 6 articles for full-text review. Researchers then expanded inclusion criteria to include Canada, Ireland, and the United Kingdom, resulting in 17 final articles for data extraction (Figure 1).
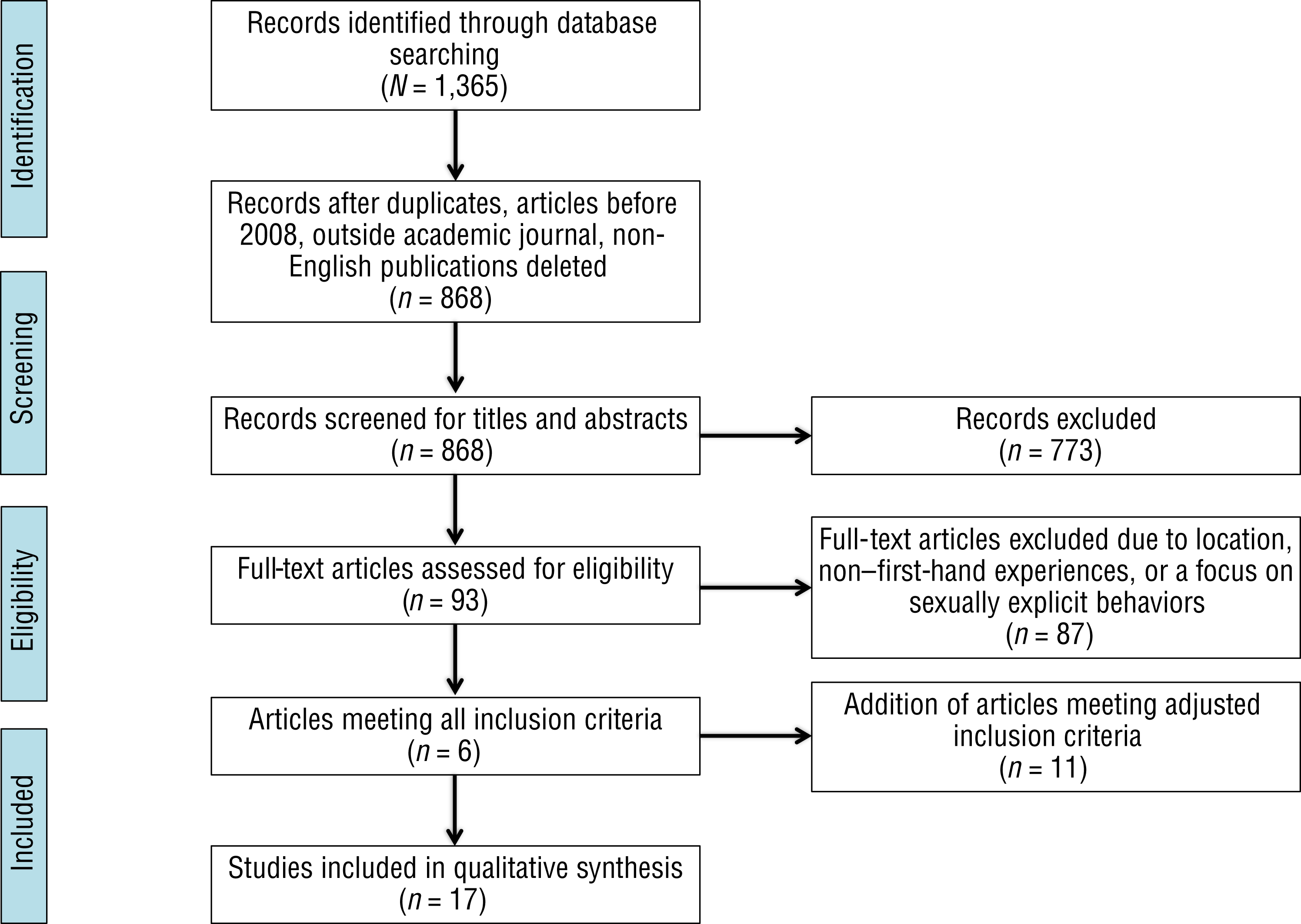
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Researchers extracted data that included author(s), location, author discipline, study title, study design, research question(s), sample, outcome, and recommendations. Each team member completed the data extraction individually and then collaborated with their teammate to complete the final data extraction worksheet (see Table A.1 in the Appendix). Each researcher compiled a list of themes from reviews of the data extraction worksheet. Researchers met as a group three times to discuss and agree on themes. Each researcher wrote a theme description, and the research team reviewed and revised the theme descriptions collaboratively.
Results
The primary country of origin for the included articles was the United Kingdom (9), followed by the United States (6), Ireland (2), and Canada (0). The articles were primarily qualitative studies (n = 14), including thematic analysis (6), interpretive phenomenological analysis (4), ethnography (2), descriptive inquiry (1), and critical discourse analysis (1). Two articles used a quantitative design, and 1 article used a mixed-methods design with the nominal group technique. Participants in qualitative studies were categorized as having mild to moderate IDD. No articles included caregivers who reported on behalf of people with IDD. The academic disciplines of authors varied widely, but of note, none of the articles were published by occupational therapy practitioners. Through our review of articles, four themes emerged: intimate relationships, oppressed sexual activity, identity, and knowledge.
Intimate Relationships
Responses of participants in the included studies indicated that they valued intimate relationships but considered intimacy as more than sexual relationships. Rogers and Tuckwell (2016) found that people wanted close friendships, someone they could talk to about “sex, having babies and relationships” (p. 631). Sullivan et al. (2013) reported that when participants in their study were asked about the importance of intimate relationships, they did not necessarily equate this topic with sexual relationships. Many participants talked about the importance of being close physically (i.e., touch) and emotionally and the resulting contribution to feelings of security. Participants in another study stated that being in an intimate relationship increased their self-esteem and made them feel normal (Wilkinson et al., 2015). However, Kelly et al. (2009) found that ambivalence, limited social knowledge, fear, and embarrassment caused participants to avoid intimate relationships, resulting in reported increased loneliness and isolation.
Oppressed Sexual Activity
Participants in these studies identified barriers related to sexual activity and intimate relationships that provide space for sexual activity. Internalized barriers included beliefs that sexual activity is wrong and punishable (Kelly et al., 2009; Sullivan et al., 2013) and that sexual activity should only occur between married people (Bernert & Ogletree, 2013; Wilkinson et al., 2015). External barriers included residential agencies or families prohibiting intimate relationships and sexual activities (Fish, 2016; Grace et al., 2020; Sullivan et al., 2013; Turner & Crane, 2016a). Participants in a study by Healy et al. (2009) stated that they wanted to get married but believed they were not allowed to do so. Many participants in the studies were aware of these barriers and expressed concerns that they were not able to talk about their sexual behavior for fear that others would see it as unacceptable.
Similarly, women in another study reported being discouraged from talking about their sexuality (Fitzgerald & Withers, 2011). An extreme example of this oppression was a participant who hid being raped and hospitalized because she was concerned that her parents would be mad at her for having had sexual intercourse (Sullivan et al., 2013). In general, participants in the reviewed studies wanted control and choice over their sexuality and ability to engage in relationships, but they faced barriers.
Identity
Many studies found that participants wanted to be in intimate relationships; however, not all participants perceived themselves as sexual beings (Fitzgerald & Withers, 2011; Wilkinson et al., 2015). Although most studies found that opportunities to develop a sexual identity were lacking, evidence showed that some participants were successful in developing positive identities (Fitzgerald & Withers, 2011; Turner & Crane, 2016a; Wilkinson et al., 2015). Some study participants expressed the belief that sex is equated with bad behavior and experienced self-shame, whereas others felt a sense of pride about being in a sexual relationship and saw sex as positive. Being in a sexual relationship provided participants the assurance that they could be sexual beings and seen as a “normal” adult. Participants acknowledged the need for others to respect their sexual identity and to provide opportunities for developing this identity because it is part of adult development (Fitzgerald & Withers, 2011; Friedman et al., 2014; Turner & Crane, 2016a; Wilkinson et al., 2015).
Sexual orientation added to this struggle for participants in the reviewed studies who identified as lesbian, gay, bisexual, or transgender (LGBT). Participants in one study faced discrimination related to both their IDD and their sexual orientation and, in some cases, their gender identity (Dinwoodie et al., 2020). These people felt unsupported and often experienced abuse by caregivers, the general public, and law enforcement. This treatment also led to problems with self-acceptance and affirmed the belief that something was wrong with them on the basis of their sexual orientation or gender identity (Dinwoodie et al., 2020). In addition, studies found that education focused primarily on heteronormative standards, which may lead to negative perceptions about LGBT identity (Burns & Davies, 2011; Fitzgerald & Withers, 2011).
Knowledge
The knowledge theme includes basic sexual knowledge, relationship knowledge, and lack of formal sex education. Basic sexual knowledge consisted of topics such as pregnancy, intercourse, masturbation, and safe sex. Participants in one study had little knowledge of how women become pregnant, stating that pregnancy occurs “in hospitals” and “in tummies” (Kelly et al., 2009, p. 311). When asked what to do if a partner was pregnant, participants displayed limited knowledge (Swango-Wilson, 2011). Healy et al. (2009) found that participants often thought that masturbation and intercourse were the same, believing they could get pregnant through masturbation. Moreover, participants from several studies indicated limited knowledge of safe sex, condom use, and “how to do it” (Bernert & Ogletree, 2013; Healy et al., 2009; Swango-Wilson, 2011).
Five studies explored relationship knowledge. Participants in these studies expressed limited knowledge of how to make friends and develop long-term relationships (Baines et al., 2018; Rogers & Tuckwell, 2016; Rushbrooke et al., 2014; Swango-Wilson, 2011; Turner & Crane, 2016b). Participants in 2 studies indicated they did not know how to ask someone on a date or whether they wanted to have sex (Rushbrooke et al., 2014; Swango-Wilson, 2011).
Three studies indicated that opportunities to engage in formal sex education were limited (Kelly et al., 2009; Swango-Wilson, 2011; Turner & Crane, 2016b). The results of these studies indicated that although some participants learned about sex at school, the majority stated that they learned from their parents, agency staff located where they live, social media, and movies and television.
Discussion
Findings of this scoping review are consistent with past research indicating that sexuality is a part of the lives of many adults with IDD, regardless of engaging in sexual activity (Borawska-Charko et al., 2016). Results of this study are supported by previous research indicating that beyond sexual activity, adults with IDD desire intimacy (Rogers & Tuckwell, 2016; Sullivan et al., 2013; Wilkinson et al., 2015). Although intimacy is related to sexual activity, it also includes developing relationships that are based on feelings of trust, safety, and friendship (Council on Quality and Leadership, 2017), which, in turn, have been found to be the foundation for developing a sexual identity (Friedman, 2019). Findings of this review and other studies have found that people with IDD do not have the same opportunities, knowledge, and skills to develop these relationships as those without IDD (Pottie & Sumarah, 2004).
An important finding in this study is that adults with IDD experience oppression related to their sexuality because of barriers at family, organization, and societal levels. Results of a study by Friedman (2019) support this finding, indicating that context has a considerable impact on the development of intimate relationships among people with IDD. Those people living with family, in group homes, or in institutions had a lower probability of developing intimate relationships compared with those who lived independently. This outcome may be because of caregivers’ beliefs that people with IDD are incapable of self-determination, especially in the area of intimate and sexual relationships (Wilkinson et al., 2015). Caregivers may fear that people are more vulnerable to sexual exploitation or violence. However, this belief can limit the person’s access to education related to sex and intimacy and may limit their ability to form relationships, which also puts them at greater risk for unsafe sex practices or sexually transmitted diseases (Sullivan et al., 2013).
At a national level, oppression may be attributed to policies informed by cultural beliefs and attitudes (Hyland & McGrath, 2013). Cultural influences on policy in the United States include religiously based views of sexuality and sexual behaviors, historical stigma, and low expectations and protective attitudes toward adults with IDD (McGrath & Sakellariou, 2016). Policy discussions and decisions typically exclude people with IDD (Friedman et al., 2014) and focus on the risks related to people in this population having sex versus the importance of relationships to health and well-being. When people with IDD have been included in policy-making, they report feeling like “tokens” and not being fully included in the decision-making process (Beckwith et al., 2016).
Results of this study demonstrate the known lack of inclusion of people with IDD in research about sexuality. Our initial literature search revealed several hundred articles about this topic, but many were excluded because they did not include the voice of people with IDD. This finding is a known issue to advocates in the disability community who have been working toward more inclusive research designs (Alexander & Gomez, 2017). When studying adults with IDD, research designs need to be flexible enough to address pragmatic challenges, such as recruitment and consent, and incorporate these people as partners in the research process (Beckwith et al., 2016; Rogers & Tuckwell, 2016). Bigby et al.’s (2014) framework for inclusive designs for research with people with IDD can be applied to studies about sexuality to increase the knowledge base.
Even within occupational therapy, a profession that embraces a client-centered approach, there is a dearth of information on this topic. In this review, no articles came from the occupational therapy literature. Previous research has shown that although occupational therapy practitioners view sexuality and sexual activity as an important part of daily functioning, the practice of occupational therapy does not reflect this assessment (McGrath & Sakellariou, 2016). This tendency to exclude sexuality, combined with a lack of the voice of people with disabilities in literature, contributes to the lack of knowledge and guidance for intervention. Guidance about addressing sexuality originating in the occupational therapy literature focuses mainly on sexuality after acquired disabilities, such as spinal cord injury, stroke, and so forth (Fritz et al., 2015; Thomas, 2016), and not on IDD (Lynch & Fortune, 2019; McGrath & Sakellariou, 2016).
Limitations
This study has several limitations. Definitions of IDD vary between professions and geographically. Search terms may have not accounted for all the variability in language. Another limitation is that all articles focused on people with mild to moderate impairments, leaving out the perspectives of those with more severe intellectual or communication impairments.
Implications for Occupational Therapy Practice and Research
Given occupational therapy’s scope of practice and the expression of sexuality as a meaningful occupation, practitioners should include sexuality as part of person-centered holistic care for adults with IDD by
Developing and providing interventions focused on sexuality-related skills, including self-advocacy, decision making, relationship building, self-expression, and health knowledge;
Developing and providing interventions focused on social skills training for developing intimacy and sexual relationships;
Including sexuality in transition plans and making referrals to programs that address sexuality and sex education in adulthood;
Including people with IDD as partners in research and ensuring that their voice is included in the literature; and
Engaging in scholarship that explores sexuality among adults with IDD as a part of client-centered care.
Conclusion
The results of this scoping review provide support for addressing sexuality among adults with IDD in occupational therapy. Engaging in intimate relationships can contribute to overall well-being and developing sexual identity. Opportunities for adults with IDD to express sexuality and to engage in relationships that provide a space for sexual expression are often limited by several internal and external factors, including limited self-awareness or awareness of their own rights related to sexuality, societal attitudes, and policies. Occupational therapy practitioners can address barriers as part of client-centered practice and support sexuality as part of the full human experience.
Footnotes
Acknowledgments
We thank Jennifer Westrick (library research information specialist at Rush University Medical Center) for assisting with the literature search.
Appendix
*
Indicates studies included in the scoping review.