
Abstract
This study provides preliminary evidence that Maximizing Energy, an internet-based, self-management intervention, may reduce fatigue impact and severity in people with post–traumatic brain injury fatigue.
Fatigue, a devastating sequela of traumatic brain injury (TBI) with a prevalence of 43% to 73%, persists for years after the injury (Belmont et al., 2006). Fatigue negatively affects a person’s physical, cognitive, social, and emotional functioning (Ezekiel et al., 2021; Mollayeva et al., 2014). People with even mild TBI experience severe fatigue and limitations in daily functioning (Stulemeijer et al., 2006). Fatigue uniquely contributes to disability after controlling for injury severity, executive function, and depression (Juengst et al., 2013). There is an inverse relationship between fatigue and participation and work disability (Cantor et al., 2008). Despite post-TBI fatigue’s interference with community reintegration and quality of life, it is often overlooked in rehabilitation programs (Bay & de-Leon, 2011; Cantor et al., 2012).
Cognitive–behavioral therapy is the most promising treatment for post-TBI fatigue (Cantor et al., 2014; Sullivan et al., 2018). Problem-solving therapy, an application of cognitive–behavioral therapy, emphasizes a positive orientation toward everyday problems and promotes self-directed adaptive coping solutions for their resolution (D’Zurilla & Nezu, 2007). The seven-step framework enhances skills to cope with physical and mental health stressors; is amenable to the individualization of education; and is used for people with depression, TBI, and hypertension (García-Vera et al., 1997; Rath et al., 2003). Research also suggests that TBI rehabilitation must include energy conservation education to facilitate fatigue management (Fellus & Elovic, 2007) and should be individualized to meet clients’ diverse needs (Finlayson & Holberg, 2007).
We developed the Maximizing Energy (MAX) intervention to help clients develop coping and problem-solving skills, combined with individualized energy conservation education to help them manage fatigue-related challenges in daily life (Raina et al., 2016). The MAX intervention is feasible, and people with TBI can independently learn it and apply it to fatigue-related problems.
Given the dearth of evidence-based interventions to address post-TBI fatigue, we examined the preliminary effectiveness of the MAX intervention in comparison with a control health education (HE) intervention. We hypothesized that over the course of 16 wk, people who took part in the MAX intervention would report lower fatigue impact on daily life (primary outcome) and, more specifically, reduced fatigue severity, improved fatigue experience, and increased participation (secondary outcomes) compared with those who received the HE intervention.
Method
Research Design
In this two-group, single-blind, randomized controlled trial (RCT), participants were randomized before baseline assessments by means of a random number generator (1:1 ratio; Figure 1). Assessors, who were masked to group allocation, assessed outcomes at baseline (Time 1), postintervention (Time 2), and 4 (Time 3) and 8 wk (Time 4) postintervention. The institutional review board at the University of Pittsburgh approved the study.
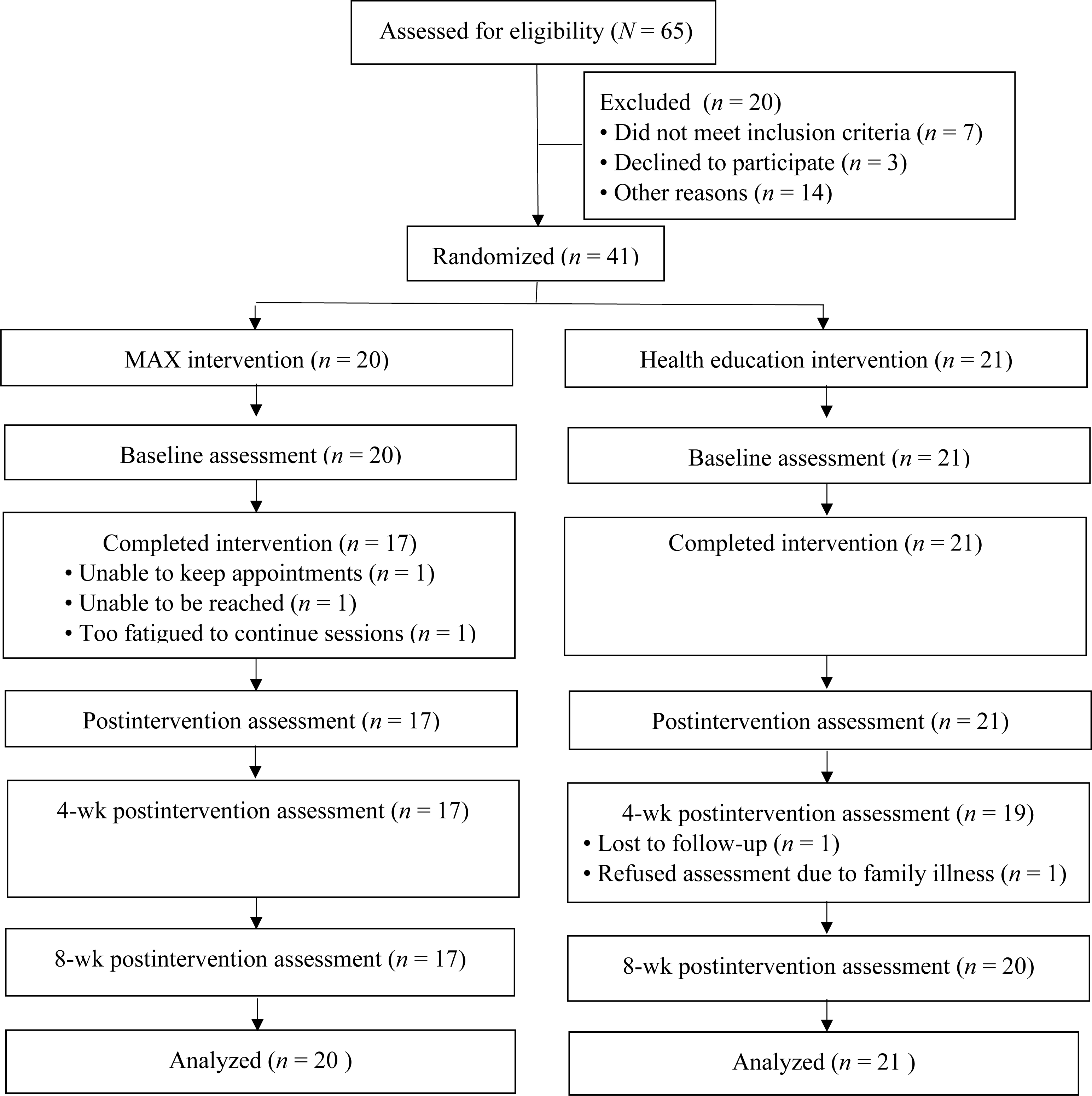
Modified CONSORT 2010 flow diagram.
Participants
Participants, who were recruited from local support groups, research registries, and medical practices, met the following nine criteria: (1) age ≥18 yr; (2) 6 mo after mild to severe TBI, based on a medical chart review of an initial Glasgow Coma Scale score ranging from 3 to 15, accompanied by neuroradiological findings (Teasdale & Jennett, 1974); (3) Fatigue Severity Scale (FSS; Krupp et al., 1989) score ≥4; (4) community dwelling; (5) able to operate a computer and understand English; (6) sufficient cognitive capacity to provide written informed consent; (7) FIM® Motor score >65 (Stineman et al., 1996); 1 (8) no history of psychiatric disorder diagnosed through the Primary Care Evaluation of Mental Disorders and the Mini-International Neuropsychiatric Interview in the past 3 mo, verified by participant interview (Sheehan, 1998; Spitzer et al., 1994); and (9) no disability before the TBI.
Sample Size Calculations
We selected 8 wk postintervention as our primary endpoint because it allows participants to apply the MAX intervention to manage fatigue-related problems independently. A sample size of 20 per group would enable us to detect a large between-groups effect size (Cohen’s d = 0.80) of the Modified Fatigue Impact Scale (mFIS; Learmonth et al., 2013) at 8 wk postintervention with 80% power and an α of .05 (Cohen, 1988).
Instruments
Baseline sociodemographic and clinical characteristics included age, gender, race, education, time since injury, injury severity, and medical burden (measured with the Cumulative Illness Rating Scale; Miller et al., 1992). A cognitive composite T score was derived from six of eight tests from a neuropsychological test battery validated by TBI Model Systems (Hanks et al., 2008). Affective impairments were measured with the Hamilton Depression Rating Scale and the Apathy Evaluation Scale (AES; Hamilton, 1960; Marin et al., 1991).
The mFIS measures the impact of fatigue on daily life; it has 21 items rated on a 5-point scale (0 = never, 4 = almost always), with total scores ranging from 0 to 84 (higher scores indicate greater fatigue impact) and has excellent internal consistency (Cronbach’s α = .97, p < .05; Schiehser et al., 2015), good test– retest reliability (intraclass correlation [ICC] = .85; Larson, 2013), and a minimally important difference (MID) of 4.00 (Rooney et al., 2019).
The FSS measures fatigue symptom severity; it consists of nine items, rated on a 7-point Likert scale (1 = strong disagreement, 7 = strong agreement), averaged for a total score ranging from 0 to 7 (higher scores indicate greater fatigue severity) and has excellent internal consistency (Cronbach’s α > .90) and test–retest reliability (ICC = .93; Nadarajah et al., 2017) and a MID of 0.45 (Rooney et al., 2019).
The Patient-Reported Outcomes Measurement Information System (PROMIS) Fatigue scale is a computer-adaptive test that measures the experience of fatigue (Cella et al., 2016); it has a mean score of 50 (SD = 10; higher scores indicate more fatigue) and a MID of 0.25 to 0.45 (Yost et al., 2011).
Participation Objective, Participation Subjective (POPS) is a 26-item measure of community integration that documents home and community participation frequency (objective) and adequacy (subjective; Brown et al., 2004), yields z scores (objective: range = –3 [no participation] to 3 [higher frequency of participation]; subjective: range = –4 [wants to do less or more of] to 4 [satisfied with participation]), and has moderate test–retest reliability in people with TBI (ICCs = .75 and .80, respectively; Brown et al., 2004).
Procedure
Trained occupational therapists delivered both interventions for 8 wk (two 30-min live internet sessions/wk); intervention fidelity was assessed (Raina et al., 2016).
Maximizing Energy (Experimental) Intervention
The MAX intervention combines energy conservation education and problem solving to promote skill development in defining and solving fatigue-related problems (Raina et al., 2016). It emphasizes skill generalization by applying successful solutions to other fatigue-related problems, gradually eliminating the need for the therapist in the problem-solving process (Table 1).
Example of the MAX Intervention With a Hypothetical Client
Note. MAX = Maximizing Energy; TBI = traumatic brain injury.
Health Education (Control Intervention)
HE focused on energy conservation education and health-related topics (e.g., diet, exercise, strength training; Raina et al., 2016). Participants had knowledge of energy conservation strategies but were not taught to apply them to their fatigue-related problems.
Data Analysis
We compared the groups at baseline and identified covariates for primary analyses using t tests and χ2 tests. We performed an intention-to-treat analysis using linear mixed-effects models, which include all participants, regardless of missingness, so change outcome measures can be examined. We examined model fit for covariance structures (unstructured, compound symmetry, and auto-regressive) using the Akaike information criterion and Bayesian information criterion, with lower values representing better fit. We examined group (MAX or HE) and time (Times 1, 2, 3, 4) as main fixed effects, and the Group × Time interaction and time-invariant grand mean–centered covariates, with a random intercept for participants (p = .05). We performed post hoc tests for significant effects and estimated covariate-adjusted least square means (LSMs) because they are less sensitive to missing data. Primary statistical analyses were conducted with SAS software (Version 9) using PROC MIXED. We computed Cohen’s d between-groups effect sizes (0.20 = small, 0.50 = moderate, 0.80 = large) using change scores over time (Cohen, 1988; Portney & Watkins, 2009). We calculated a fragility index for the dichotomous outcome of mFIS change scores ≥4 (Walsh et al., 2014).
Results
We assessed data from 65 participants; 41 were randomized to a group (Figure 1). The groups did not differ in terms of age (MAX, M = 43.8 yr, SD = 16.2; HE, M = 48.1 yr, SD = 12.5), gender, ethnicity, education, FIM score, depression symptoms, or cognitive impairment (Raina et al., 2016). Participants demonstrated mild to moderate cognitive impairment. Because AES scores were significantly different (MAX, M = 58.4, SD = 4.7; HE, M = 52.8, SD = 7.6; p = .01), we used grand mean–centered baseline scores as covariates in the analysis.
Fatigue Impact
There was a significant Group × Time interaction, F(1, 107) =29.54, p = .01, and post hoc tests revealed significantly lower mFIS scores for MAX participants (LSM = 34.24, SE = 3.50) than HE participants (LSM = 45.21, SE = 3.35) at Time 4 (p = .03), an 11-point difference almost 3 times greater than the MID for the mFIS. There was no relationship between AES and baseline mFIS (p = .11), and baseline differences in AES score did not affect mFIS over time (p = .35). Including AES in the model slightly improved model fit, with lower intercept variance. The effect size for between-groups differences at Time 4 was large (Table 2). The fragility index was 3.
Change Scores From Baseline to Follow-Up
Note. CI = confidence interval.
Experience of Fatigue
There was a significant Group × Time interaction, F(1, 120) = 7.60, p = .01, and post hoc tests showed that MAX participants (LSM = 45.94, SE = 4.05) had significantly lower fatigue than HE participants (LSM = 59.67, SE = 3.94) at Time 2 (p = .02) and Time 4 (MAX group: LSM = 45.35, SE = 4.05; HE group: LSM = 59.80, SE = 3.95; p = .01; see Supplemental Table A.1, available online with this article at https://research.aota.org/ajot). The 15-point difference at Time 4 is 6 times greater than the MID of 2.5. The between-groups effect size at Time 4 was large. There was no relationship between AES and baseline PROMIS–Fatigue; baseline AES did affect PROMIS–Fatigue scores over time, F(1, 120) = 5.58, p = .02.
Fatigue Severity
There was a significant Group × Time interaction, F(1, 109) = 4.57, p = .03, and post hoc tests showed that MAX participants (LSM = 4.37, SE = 0.28) had significantly lower scores than HE participants (LSM = 5.22, SE = 0.26) at Time 2 (p = .03) and Time 4 (MAX: LSM = 4.03, SE = 0.28; HE: LSM = 4.93, SE = 0.26; p = .02; see Supplemental Table A.2). The 0.9-point difference is 2 times greater than the MID. Adding AES did not improve model fit, F(1, 108) = 1.00, p = .32. The between-groups effect size at Time 4 was moderate.
Participation
The main effect of time indicated that objective, F(1, 106) = 38.46, p < .001, and subjective, F(1,147) = 46.99, p < .001, scores changed over time regardless of group; there were no significant interaction or between-groups differences. Adding AES did not improve model fit.
Discussion
Our study provides preliminary evidence that the MAX intervention can reduce the impact, experience, and severity of fatigue. Participants who received the MAX intervention demonstrated significantly lower fatigue impact than those who received HE immediately after intervention completion (moderate effect size), and this finding was magnified at 8 wk postintervention (large effect size). Studies that use education interventions alone have demonstrated no change in fatigue scores 3 mo postintervention (Matuseviciene et al., 2013; Ponsford et al., 2002). People with post-TBI fatigue benefit from the MAX intervention in the short term and up to 2 mo after contact with the therapist is withdrawn. This finding supports the sustainability of the MAX intervention’s effect. Future studies should examine the MAX intervention’s sustainability beyond 8 wk and determine the need, type, and timing of booster sessions.
We observed similar findings for fatigue experience with the PROMIS–Fatigue. Mean scores for the MAX group at 8-wk postintervention were 0.50 SD below the population mean, whereas scores for the HE group were 1.00 SD above the population mean, indicating severe fatigue. We used the PROMIS–Fatigue computerized adaptive test because it demonstrates excellent reliability, precision, and sensitivity to change (Cella et al., 2016). Compared with the ordinal measures we used in this study, the scale may more accurately have captured changes in the participants’ fatigue experiences.
It is interesting that although the MAX intervention demonstrated a reduction in fatigue severity, participants’ mean FSS score was still above 4.0 at 8 wk postintervention, indicating severe fatigue (Krupp et al., 1989). We hypothesize that, rather than alleviating the causes of the fatigue, this intervention teaches participants to use compensatory strategies to manage their energy to participate in meaningful activities.
Last, we did not note a difference between the groups in regard to participation. This lack of a difference could reflect the MAX intervention’s focus on teaching people how to engage in meaningful discrete activities rather than focusing on broad aspects of participation. In addition, our choice of POPS to measure participation may have been problematic given that there are no data to support its responsiveness to change. Future studies need to include a responsive participation measure to determine the MAX intervention’s effect on participation and community integration.
Our findings are consistent with those of studies that have demonstrated that education alone is ineffective in alleviating post-TBI fatigue. In one study, an 8-wk occupational therapist–delivered energy conservation education did not reduce fatigue (Cooper et al., 2009). Vuletic et al. (2016) reported that active duty service members with mild TBI had significantly better sleep quality after engaging in a problem-solving sleep intervention augmented with education than did those who received education alone. Our study diverges from prior studies of cognitive–behavioral therapy– based interventions for post-TBI fatigue, which have focused on improving sleep and thereby fatigue (Cantor et al., 2014). These sleep-focused interventions have not reduced fatigue, likely because sleep and fatigue are independent constructs, and reducing one may not alleviate the other (Arciniegas et al., 2000).
Limitations and Future Studies
The findings from this early-phase RCT are encouraging, but we urge caution in generalizing them. First, the small sample size may have led to inflated effect sizes (Moore et al., 2011). Although a sample size analysis indicated sufficient power to detect a large effect size for mFIS at 8 wk postintervention, we need to replicate this study with a larger sample. Second, the small sample size prevented us from assessing the variable effect of injury severity and cognitive impairment on intervention effectiveness. Third, there was a significant difference in apathy level between the groups at baseline. Although apathy was a covariate in the analyses, there may have been differences in other baseline characteristics that we did not measure. Fourth, we used informed consent to screen participants because we did not want to exclude anyone on the basis of an arbitrary cognitive cutoff score. Instead, we believed that if the participant could provide written informed consent, they could participate in the intervention. Finally, the sample was not ethnically diverse: All of the MAX participants, and 85% of the HE participants, were Caucasian. Future studies need to recruit a diverse sample.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice: The MAX intervention is a top-down, client-centered, occupation-based intervention to help manage post-TBI fatigue. The MAX intervention appears to reduce fatigue impact and severity in post-TBI populations. Occupational therapy practitioners who want to use the MAX intervention should focus on teaching clients problem-solving skills and energy conservation education and promote generalization of solutions to other fatigue-related problems.
Conclusion
This study demonstrated support for a top-down, manualized, internet-based self-management program for reducing the impact and severity of post-TBI fatigue. Future research should replicate the study with larger and more diverse samples, a longer follow-up, and responsive participation measures.
Footnotes
1
FIM® is a trademark of the Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.