
Abstract
Purpose
To provide an assessment by meta-analysis of the relationship between the expression variations of 5-fluorouracil metabolic enzymes and clinical outcomes in patients with gastric cancer treated with S-1.
Method
Databases were searched electronically from inception to April 19th, 2015. Studies in gastric cancer patients treated with S-1 investigating the expression variations of 5-fluorouracil metabolic enzymes were included after having been identified systematically. Pooled odds ratios (OR) for the objective response rate (ORR) and median survival ratio were calculated using the Review Manager 5.3 and Stata 12.0 software separately.
Results
A total of 555 patients in 10 studies met our inclusion criteria. There was a significant difference in ORR between patients with high/+ and low/- expression of orotate phosphoribosyl transferase (OPRT) (OR = 8.06; 95% CI, 4.06-16.02; p<0.001) and dihydropyrimidine dehydrogenase (DPD) (OR = 1.95; 95% CI, 1.21-3.13; p = 0.006). There was no significant difference in ORR between different expression levels of thymidylate synthase (TS) and thymidine phosphorylase (TP). Although patients with low/- TS expression, low/- TP expression and high/+ DPD expression showed a trend towards longer survival, no statistical significance was found. The median OS was significantly longer in patients with high/+ expression of OPRT (p = 0.076).
Conclusions
OPRT and DPD expression can be treated as a potential predictive biomarker for S-1 response in gastric cancer patients. Further investigation is warranted.
Introduction
Gastric cancer (GC) is one of the most common malignant tumors. A total of 989,600 new GC cases and 738,000 deaths are estimated to have occurred in 2008, accounting for 8% of the total cases and 10% of total deaths (1). Although the incidence rate of GC is falling globally, the World Cancer Report 2014 showed that GC is still the third leading cause of cancer-related deaths and has a higher incidence in Asia (2).
Commonly used chemotherapy regimens for GC patients contain both cytotoxic drugs and drugs inhibiting DNA synthesis. 5-Fluorouracil (5-FU) and its derivatives have played a key role in the treatment regimens for GC. S-1 is an oral anticancer compound capsule composed of tegafur (FT), gimeracil (CDHP) and potassium oxonate (Oxo) in a molar ratio of 1:0.4:1. FT is a prodrug of 5-FU that shows good oral bioavailability and sustained release. When administered orally, FT is absorbed stably in the small intestine and slowly converted to 5-FU by drug-metabolizing enzymes in the liver. CDHP is a reversible competitive inhibitor which can inhibit the key enzyme during the degrading process of 5-FU, and thereby it can keep longer at higher concentrations of 5-FU in the bloodstream (3). Oxo administered orally can selectively function in OPRT to block phosphorylation of 5-FU in the gastrointestinal tract, and thus can reduce the main side effects of gastrointestinal disturbance. Several enzymes have key roles in the metabolic pathway of 5-FU (Fig. 1) (4). Thymidylate synthase (TS) is a target enzyme of 5-FU. 5-FU is converted into fluorodeoxyuridine monophosphate (FdUMP) in the tumor cells to exert an anticancer effect by forming a ternary complex of TS. Thymidine phosphorylase (TP) exerts its function by promoting transfer of FT to 5-FU. DPD is a rate-limiting enzyme which translates 5-FU into metabolites without cytotoxicity during the degrading process (5). OPRT is a critical metabolic enzyme in the activation of 5-FU (6).
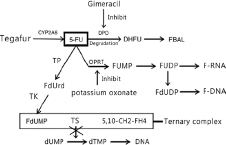
S-1 metabolic pathways. 5-FU = 5-fluorouracil; CYP = hepatic cytochrome P450; TS = thymidylate synthase; TP = thymidine phosphorylase; DPD = dihydropyrimidine dehydrogenase; OPRT = orotate phosphoribosyl transferase; TK = thymidine kinase; DHFU = dihydrofluorouracil; FdUMP = fluorodeoxyuridine monophosphate; FdUDP = fluorodeoxyuridine diphosphate; FUDP = fluorouridine diphosphate; FUMP = fluorouridine monophosphate; F-DNA = fluorinated DNA; F-RNA = fluorinated RNA; dUMP = fluorodeoxyuridine monophosphate; dTMP = deoxythymidine monophosphate.
S-1-based chemotherapy has yielded excellent results in adjuvant chemotherapy, neoadjuvant chemotherapy and palliative chemotherapy of GC (4). S-1 in combination with cisplatin has been a recommended first-line treatment regimen for GC in Japan based on the phase III clinical trial results of SPIRITS (7) and JCOG9912 (8). In addition, S-1 has proven to be efficacious and better tolerated than 5-FU across a variety of clinical settings for GC, leading to its widespread use in Asia (9).
However, there are individual differences among the treatment effects of S-1. Meanwhile, toxicities of S-1-based chemotherapy including myelosuppression, liver damage, gastrointestinal and skin toxicities are common. This has created a great need for biomarkers that can predict clinical outcomes such as response and survival in GC. 5-FU metabolic enzymes may be a major determinant of the sensitivity to S-1-based chemotherapy and survival in GC. A number of studies have investigated the association between 5-FU metabolic enzyme expression and chemotherapy response in GC patients treated with S-1-based chemotherapy (10-11-12). However, some of the presented results were controversial and there has been no comprehensive assessment. So we reviewed the published studies and carried out this meta-analysis, further exploring the possibility of considering 5-FU metabolic enzymes as biomarkers to predict the efficacy of S-1 treatment.
Materials and methods
Search Strategy
A comprehensive literature search was performed by searching the electronic databases PubMed, Embase, CBM, CNKI and VIP for all relevant studies from inception to April 19th, 2015. Search strategies were carried out using both medical subject headings and free terms. Publications were retrieved using a combination of the following terms and their synonyms: “thymidylate synthase”, “orotate phosphoribosyl transferase”, “thymidine phosphorylase” OR “dihydropyrimidine dehydrogenase” AND “stomach neoplasms” AND “tegafur-gimeracil-oteracil”. There were no language restrictions. The references of retrieved articles and important meeting materials were also screened for relevant articles.
Selection Criteria
Studies meeting the following eligibility criteria set before screening were selected: 1) all patients included in the analysis had pathologically confirmed GC and at least 1 measurable lesion; 2) all patients received S-1-based chemotherapy; 3) the expression of 5-FU metabolic enzymes was detected with immunohistochemistry (IHC) or reverse-transcription polymerase chain reaction (RT-PCR) in tumor tissues; 4) the study presented sufficient data on objective response rate (ORR) or overall survival (OS) according to 5-FU metabolic enzyme status; 5) only the largest or the most recent article was included if there were multiple articles based on similar clinical trial data.
The exclusion criteria were the following: 1) research using animals or cell lines; 2) letters, reviews and case reports; 3) studies researching other tumors; 4) studies detecting the expression of 5-FU metabolic enzymes in peripheral blood; 5) studies where the primary outcomes were not ORR or OS; 6) studies without qualified data.
Data Extraction
Two independent reviewers (D Wang and XW Wang) extracted the relevant data from all eligible studies. Discrepancies were resolved by discussion and consultation of the contents of the articles. The following characteristics and data were retrieved from each study if available: first author name, publication year, patient number, ethnicity, age distribution, gender, clinical features, specimen type, detection method, cutoff value, expression status of 5-FU metabolic enzymes, and the expression-related ORR or OS data.
Informed Consent
We did not carry out trials directly on patients but all trials included in the meta-analysis had obtained permission and consent from patients before providing the therapy.
Statistical Analysis
We extracted the number of patients with available data of ORR or OS and the number of total GC patients with each 5-FU metabolic enzyme from the included studies. OS was defined as the time from random assignment to death from any cause and ORR was the sum of the partial response rate (PR) and complete response rate (CR). The odds ratios (OR) with corresponding 95% confidence intervals (CI) were calculated to quantitatively determine the association between 5-FU metabolic enzyme expression and ORR of GC, while median survival ratio analysis was used for quantitatively evaluating the association of 5-FU metabolic enzyme expression with survival. All the data on ORR and OS were entered into the Review Manager v.5.3 and Stata v.12.0 software to make statistical analyses. The chi-square-based Q test and inconsistency index (I2) test were used to assess heterogeneity in studies. For the heterogeneity tests, a p value less than 0.10 was considered to indicate significance and the total variation among studies was estimated by I2. If there was significant heterogeneity among studies (p<0.10 and of I2 >50%), the pooled estimate was calculated based on the random-effects model. Otherwise, a fixed-effects model was selected with homogeneity present. A funnel plot was visually inspected to estimate potential publication bias by examining the relationship between the treatment effects and the standard error of the estimate. The degree of asymmetry was tested using Egger's test (p<0.1 was considered a significant publication bias). In addition, sensitivity analysis was performed by excluding the small-size sample studies to dissect the heterogeneity. All statistical analyses were performed using Stata v.12.0 and Review Manager v.5.3.
Results
Selection of Literature
The search strategy identified 76 potentially relevant articles; the selection process is illustrated in Figure 2. All identified studies were carefully screened and 47 of the potentially relevant articles were excluded after review of the titles. A total of 29 studies were included for abstract review after the first exclusion. Of these 29 studies, 3 were not relevant to S-1-based chemotherapy and 2 did not evaluate ORR or OS. Two of them used peripheral blood as samples. There were also 4 review articles and 3 experiments in vitro. Fourteen articles were excluded and 15 studies were extracted for full text review after careful abstract review. One article lacking independent data of S-1-based chemotherapy and 4 articles without ORR or OS data according to 5-FU metabolic enzyme status (only illustrating 5-FU metabolic enzyme expression and its correlation with the clinical characteristics of GC) were excluded. Ten studies involving 555 cases were ultimately included in the present meta-analysis after completion of the selection process. All of them studied the association between 5-FU metabolic enzyme expression and response to S-1-based chemotherapy with sufficient ORR and OS data (13-14-15-16-17-18-19-20-21-22).
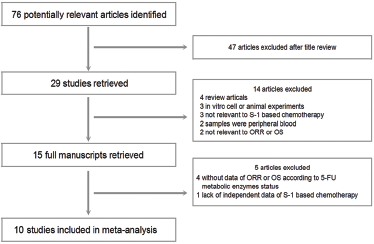
Flow diagram of the literature search process.
The characteristics of the patients included in the studies are presented in Table I. The 10 eligible studies were all performed in Asian populations including 8 from Japan and 2 from Korea. All studies sampled the tumor tissue before chemotherapy by surgical resection or biopsy. We obtained data on chemotherapy schemes, male/female proportions, clinical diagnosis, median age and ECOG performance status.
Characteristics of studies included in the meta-analysis
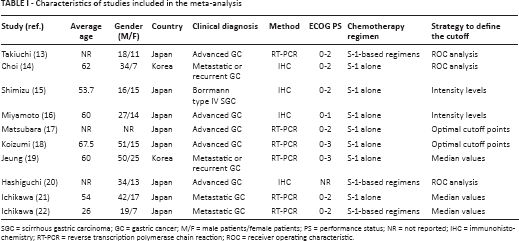
SGC = scirrhous gastric carcinoma; GC = gastric cancer; M/F = male patients/female patients; PS = performance status; NR = not reported; IHC = immunohistochemistry; RT-PCR = reverse transcription polymerase chain reaction; ROC = receiver operating characteristic.
Objective Response Rate
Nine studies reported data on tumor ORR according to 5-FU metabolic enzyme status (Tab. II) (13-14-15-16-17, 19-20-21-22), which included complete and partial tumor responses. High/+ expression of TS was found in 159 patients and low/- expression of TS in 186 patients. High/+ expression of TP was found in 116 patients and low/- expression of TP in 125 patients. High/+ expression of DPD was found in 155 patients and low/- expression of DPD in 186 patients. High/+ expression of OPRT was found in 179 patients and low/- expression of OPRT in 106 patients.
Data of objective response rate
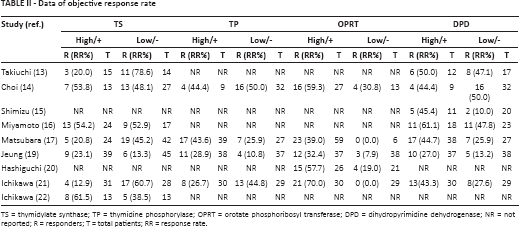
TS = thymidylate synthase; TP = thymidine phosphorylase; OPRT = orotate phosphoribosyl transferase; DPD = dihydropyrimidine dehydrogenase; NR = not reported; R = responders; T = total patients; RR = response rate.
ORR According to TS Expression
Since heterogeneity was found across the 7 studies (Fig. 3A) (χ2 = 1.36, p = 0.0006, I2 = 75%), the random-effects model was used. Pooled data from these 7 studies showed an overall ORR of 30.8% for high/+ TS expression (49/159) and 43.0% for low/- TS expression (80/186). The pooled OR of the 7 studies was 0.56 (95% CI, 0.21-1.54; p = 0.26). These results indicate no statistically significant difference in outcomes between patients with high/+ and low/- expression of TS. Bias assessment was done by funnel plot analysis as shown in Figure 4A and the heterogeneity in the 7 studies was not significant (p = 0.227).

Objective response rate in GC patients. (
ORR According to TP Expression
Heterogeneity was also found across these 4 studies (Fig. 3B) (χ2 = 7.23, p = 0.06, I2 = 59%), so the random-effects model was used. Pooled data from the 4 studies showed an overall ORR of 34.5% for high/+ TP expression (40/116) and 32% for low/- TP expression (40/125). The pooled OR of the 4 studies was 1.28 (95% CI, 0.50-3.28; p = 0.6). These results indicate no statistically significant difference in outcomes between high/+ and low/- expression of TP either. Bias assessment was done by funnel plot analysis as shown in Figure 4B and the heterogeneity in the 4 studies was not significant (p = 0.847).

Funnel plot for the detection of publication bias. (
ORR According to DPD Expression
The fixed-effects model was applied since no heterogeneity was found across the 7 studies (Fig. 3C) (χ2 = 4.16, p = 0.66, I2 = 0). Pooled data from these 7 studies showed an overall ORR of 42.6% for high/+ DPD expression (66/155) and 30.6% for low/- DPD expression (57/186). The pooled OR of the 7 studies was 1.95 (95% CI, 1.21-3.13; p = 0.006). These results indicate a statistically significant favorable clinical outcome for patients with high/+ expression of DPD. Bias assessment was done by funnel plot analysis as shown in Figure 4C and the heterogeneity in the 7 studies was not significant (p = 0.819).
ORR According to OPRT Expression
Because no heterogeneity was found across the 5 studies (Fig. 3D) (χ2 = 5.69, p = 0.22, I2 = 30%), the fixed-effects model was used. Pooled data from these 5 studies showed an overall ORR of 48.6% for high/+ OPRT expression (87/179) and 10.3% for low/- OPRT expression (11/107). The pooled OR of the 5 studies was 8.06 (95% CI, 4.06-16.02; p<0.001). These results indicate a statistically significant favorable clinical outcome for patients with high/+ expression of OPRT. Bias assessment was done by funnel plot analysis as shown in Figure 4D and the heterogeneity in the 5 studies was not significant (p = 0.97).
Median Overall Survival
OS data were available in 4 of 10 studies on the association between 5-FU metabolic enzyme expression and response to S-1-based chemotherapy (Tab. III) (14-15-16, 18). High/+ TS expression was found in 50 patients and low/- TS expression in 97 patients. High/+ TP expression was found in 51 patients and low/- TP expression in 56 patients. High/+ DPD expression was found in 47 patients and low/- DPD expression in 131 patients. High/+ OPRT expression was found in 81 patients and low/- OPRT expression in 23 patients. Although patients with low/- expression of TP, low/- expression of TS and high/+ expression of DPD showed a trend towards longer survival, no statistical significance was found. The median OS was significantly longer in patients with high/+ expression of OPRT (Tab. III).
Overall survival data

TS = thymidylate synthase; TP = thymidine phosphorylase; OPRT = orotate phosphoribosyl transferase; DPD = dihydropyrimidine dehydrogenase; OS = overall survival; NR = not reported; CI = confidence interval.
Subgroup Analysis of Detection Method
We also carried out a subgroup analysis based on the detection method used. As there was insufficient IHC-based data, all specimens were detected by RT-PCR in this subgroup analysis. Overall ORR was 23.7% for high/+ TS expression (29/122), 40.8% for low/- TS expression (58/142), 33.6% for high/+ TP expression (36/107), 25.8% for low/- TP expression (24/93), 44.4% for high/+ OPRT expression (56/126), 4.1% for low/- OPRT expression (3/73), 39.3% for high/+ DPD expression (46/117), and 25.2% for low/- OPRT expression (28/111). These results indicate no statistically significant difference in outcomes between high/+ and low/- expression of TP (OR = 1.46; 95% CI, 0.44-4.88; p = 0.54) and TS (OR = 0.41; 95% CI, 0.10-1.67; p = 0.22). There was, however, a significant difference in ORR between patients with high/+ and low/- expression of OPRT (OR = 14.17; 95% CI, 2.08-96.76; p = 0.007) and DPD (OR = 2.01; 95% CI, 1.12-3.61; p = 0.02).
Discussion
In this meta-analysis, we evaluated the effects of 5-FU metabolic enzyme expression status on ORR and OS in GC patients treated with S-1-based chemotherapy. By analyzing the data from 10 studies (for a total of 555 cases), we found a significantly higher ORR to S-1 chemotherapy in patients with high/+ DPD expression and high/+ OPRT expression. The median OS was significantly longer in patients with high/+ expression of OPRT.
TS is the crucial target enzyme of fluorouracil drugs (23). High expression of TS in the tumor tissue may indicate resistance and poor sensitivity to chemotherapy. Previous studies have documented that the expression level of the TS gene was significantly correlated with sensitivity to 5-FU chemotherapy (24, 25). However, in our meta-analysis the available data indicated that there was no statistically significant favorable clinical outcome between high/+ and low/- TS expression (OR = 0.56; 95% CI, 0.21-1.54; p = 0.26). It seems that TS cannot be the biomarker to predict the efficacy of S-1 treatment.
The results of the meta-analysis also indicated no statistically significant beneficial clinical outcome between high/+ and low/- expression of TP (OR = 1.28; 95% CI, 0.50-3.28; p = 0.6). TP catalyzes the conversion process of 5-FU and FdUMP, during which the efficacy and sensitivity of chemotherapy are promoted. It plays a vital part in promoting angiogenesis, similar to the structure and function of angiogenic platelet-derived endothelial cell growth factor (PD-ECGF), and plays an important role in tumor progression and metastasis (26-27-28). Therefore, the relationship between the expression variations of TP and clinical outcomes is affected by those 2 factors.
The expression of DPD has a significant impact on the antitumor activity of 5-FU. Its expression level determines the quantity of 5-FU entering into the anabolic pathway, which ultimately influences the quantity of nucleotide analogues. A study using human tumor xenografts in nude mice by Ishikawa et al (29) found that high intratumoral DPD activity and a high DPD mRNA level resulted in low sensitivity to 5-FU, and the authors therefore considered high expression of DPD in the tumor cells as the indicator of non-response and resistance to 5-FU. A controlled study by Fujiwara et al (30) showed that S-1 had higher antitumor activity than UFT and 5-FU. The difference in antitumor activity between fluorouracil drugs may be affected by CDHP and Oxo included in S-1. CDHP, a potent DPD inhibitor, might circumvent the resistance to 5-FU that occurs at high levels of DPD activity, in addition to bringing a pharmacokinetic benefit resulting from the inhibition of 5-FU degradation. In patients with low expression of DPD, there was no increase in cytotoxicity, although CDHP can further reduce the level of DPD. Overall, with high expression of DPD, the maximum increase in the antitumor activity of 5-FU may be the reason for higher clinical response during S-1 chemotherapy. This meta-analysis revealed a statistically significant favorable ORR for patients with high/+ expression of DPD (OR = 1.95; 95% CI, 1.21-3.13; p = 0.006), which is in agreement with the studies mentioned above.
Direct conversion to fluorouridine monophosphate (FUMP) by OPRT is the predominant pathway of 5-FU phosphorylation in tumor tissues. FUMP is subsequently metabolized to fluorouridine diphosphate (FUDP), which mediates apoptosis by interfering with RNA and DNA synthesis. This means that OPRT is the major rate-limiting enzyme in the activation of 5-FU (31). Previous studies have shown that the expression level of OPRT is connected with individual gene polymorphisms, tumor site, invasiveness, venous invasion and lymph node metastasis (32, 33). In our meta-analysis, these results also indicate a statistically significant favorable ORR (OR = 8.06; 95% CI, 4.06-16.02; p<0.001) and OS for patients with high/+ OPRT expression.
Despite our efforts to perform a comprehensive analysis, the study has many limitations, such as the inclusion of different types of GC in the analysis; the differences in the estimation criteria of ORR and OS between trials (WHO or RECIST); the wide CIs of the combined ORs; the different drug dosages that may affect ORR and OS; the significant heterogeneity observed in some analyses. Different bio-methods used in different studies were also possible limitations: IHC detects 5-FU metabolic enzyme expression at the protein level, while RT-PCR assays do so at the mRNA level.
Several studies have reported some discrepancy between mRNA expression and protein expression (34). Research has indicated that the expression of 5-FU metabolic enzymes is a dynamic process and there may be different regulation mechanisms between tumor tissues and tumor-free tissues (35). Transcription, posttranscriptional regulation, translation and posttranslation processing of the protein may contribute to the difference between IHC and RT-PCR results. The subgroup analysis of this meta-analysis indicated that there were no differences between bio-methods. Publication bias is also a possible limitation because studies that report negative results are published less frequently than those reporting positive results or those consistent with the prevailing theories. However, we did not find that publication bias significantly influenced the results of our meta-analysis. Only 10 studies were eligible for our meta-analysis as the available published literature was rather limited and the sample size analyzed in each study was relatively small. However, this is the first and initial meta-analysis assessing whether expression variations of 5-FU metabolic enzymes are associated with clinical outcomes in patients with GC treated with S-1. In spite of the small number of included trials, it is important to point out that the search criteria were broad and there were no other trials fitting the inclusion criteria.
Conclusion
Our meta-analysis indicated that high/+ expression levels of OPRT and DPD were associated with higher ORRs in GC patients treated with S-1 chemotherapy. Meanwhile, high/+ expression of OPRT was associated with longer median OS. OPRT and DPD expression in GC tissues may be suitable predictors for S-1 chemotherapy in patients with GC. Future prospective studies with large sample sizes and better study designs will be helpful in clarifying whether this is a true association.
Footnotes
Acknowledgment
We extend our thanks to Yao Chen, Senior Medical Science Liaison of Shanghai Roche Pharmaceuticals Ltd., for assisting in the preparation of this manuscript.
Conflict of interest: None of the authors has any financial interests related to this study to disclose.
Financial support: No grants or funding have been received for this study.