Editorial
Select search scope: search across all journals or within the current journal
Background: Although arthroscopic repairs of the rotator cuff are becoming increasingly popular, security of fixation remains a concern. Two-row repairs have been described, but clinical outcome reports have primarily involved open techniques.
Hypothesis: An arthroscopic repair technique that uses 2 rows of fixation produces satisfactory outcome and structural integrity by ultrasonography.
Study Design: Case series; Level of evidence, 4.
Methods: Forty-eight patients (52 shoulders) with a full-thickness, but fully reducible, rotator cuff tear who met the inclusion criteria were treated with an arthroscopic rotator cuff repair using 2 rows of suture anchors. The mean tear size was 2.47 cm (range, 1-4 cm). Patients were evaluated by subjective functional assessment (L'Insalata Shoulder Rating Questionnaire), clinical examination, including measured strength testing, and ultrasonography.
Results: At a mean follow-up of 30 months (minimum of 2 years), functional scores improved from a mean of 42 preoperatively to 93 postoperatively (P < .001). Active range of motion was increased in all measured planes (P < .001). Strength was also increased in elevation (P < .001), external rotation (P < .001), and internal rotation (P = .033). Nine of the 52 shoulders (17%) had evidence of retear or persistent defect on postoperative ultrasonography. There were no differences detected in functional scores between those with an intact repair and those with a defect, but those with an intact repair were stronger in elevation (P = .006) and external rotation (P = .001).
Conclusion: An arthroscopic 2-row rotator cuff repair produces excellent functional outcome and repair integrity comparable with previously reported open repairs. Presence of a defect after repair did not appear to affect patient-reported function and return to preinjury activity but did affect measured strength.
Background: Short-term to midterm data are available on arthroscopic shoulder stabilization using bioabsorbable tacks or suture anchors. It remains unknown whether these techniques can equal the success of open Bankart repair in the long term.
Purpose: To assess the long-term outcome of arthroscopic Bankart repair using bioabsorbable tacks in patients with traumatic anterior shoulder instability with a minimum follow-up of 7 years.
Study Design: Case series; Level of evidence, 4.
Methods: Treatment outcomes were determined prospectively according to the Rowe score and retrospectively according to the Constant and American Shoulder and Elbow Surgeons scores. Included in this study were 18 consecutive patients with a mean age of 26.8 years (range, 16-62 years) who underwent arthroscopic Bankart repair using bioabsorbable tacks for traumatic anterior shoulder instability. The study group consisted of 14 male and 4 female patients. The mean follow-up was 8.7 years (range, 7.0-9.8 years).
Results: One patient had recurrent dislocations requiring further surgery, for an overall failure rate of 5.6%. An additional patient had 1 traumatic subluxation episode within the first postoperative year that did not recur. According to the Rowe score, which increased to 90.3 (17.8) from 32.8 (8.3) points preoperatively, 15 patients (83.3%) achieved a good or excellent result. The mean Constant score was 91.3 (SD, 6.9) points, and the mean American Shoulder and Elbow Surgeons score was 92.1 (SD, 6.9) points postoperatively. A return to the preinjury level of sports competition was reported by 64% of patients. No signs of synovitis occurred in any patient postoperatively.
Conclusion: Arthroscopic Bankart repair for the treatment of recurrent traumatic anterior shoulder instability repair using bioabsorbable tacks offers reliable results with respect to failure rate, range of motion, and shoulder function during a minimum follow- up of 7.0 years. In contrast to previous reports on arthroscopic Bankart repair, results did not deteriorate during follow-up.
Background: Anterior cruciate ligament injuries are common in professional football players, and their career impact is unclear.
Purpose: To quantify the affect of anterior cruciate ligament injuries on professional football player performance.
Study Design: Cohort study (prognosis); Level of evidence, 2.
Methods: Anterior cruciate ligament injury data from the National Football League were collected during a 5-year period (1998-2002) for running backs and wide receivers. Recorded variables included player age, experience, position, time to return to competition, and yearly total yards and touchdowns. Power ratings (total yards divided by 10 plus touchdowns multiplied by 6) were calculated for the injury season as well as for the 3 seasons before and after injury. A control group consisted of all running backs and wide receivers without an identified anterior cruciate ligament injury who competed in the 2000 season.
Results: Data were analyzed for 31 running backs and wide receivers with 33 anterior cruciate ligament injuries. More than one fifth of players never returned to a National Football League game. Returning players first competed in a game 55.8 ± 5.4 weeks (mean ± standard error) after injury. For the 24 anterior cruciate ligament–injured players with a minimum total power rating (sum of all 7 seasons) of 200 points, power rating per game played decreased from 9.9 ± 1.1 preinjury to 6.5 ± 0.9 postinjury. This decline in power rating per game played was statistically significant (P = .002) when compared with the change for the 146 control players.
Conclusion: Nearly four fifths of National Football League running backs and wide receivers who sustain an anterior cruciate ligament injury return to play in a game. On return to competition, player performance of injured players is reduced by one third.
Background: Vascular endothelial growth factor (VEGF) is a potent mediator of angiogenesis.
Hypothesis: An application of VEGF may enhance angiogenesis in the grafted tendon in anterior cruciate ligament (ACL) reconstruction, and the application may affect mechanical characteristics of the ACL graft.
Study Design: Controlled laboratory study.
Methods: Eighteen sheep were divided into groups I and II. In group I, the harvested semitendinosus tendon was soaked in VEGF solution, and the right knee then underwent ACL reconstruction using this tendon. In group II, the right knee underwent identical procedures to those of group I except that the harvested tendon was soaked in phosphate-buffered saline. All animals were sacrificed 12 weeks after ACL reconstruction.
Results: Histologic findings showed that newly formed vessels and infiltrative fibroblasts were more abundant in group I than in group II. The anterior-posterior translation of the knee during an anterior-posterior force of ±100 N was significantly larger in group I than in group II by 2.58 mm (95% confidence interval, -1.76 mm to 1.76 mm) (P = .002). The linear stiffness of the femur-graft-tibia complex in group I was significantly lower than that in group II by 41.5 N/mm (95% confidence interval, -32.2 N/mm to 32.2 N/mm) (P= .017).
Conclusion: This study has revealed that VEGF as administered in this study promotes angiogenesis in the ACL graft and significantly reduces the stiffness of the ACL graft with increased knee laxity at 12 weeks after ACL reconstruction.
Clinical Relevance: Exogenous VEGF application for ACL reconstruction can induce an increase in knee laxity and a decrease in the stiffness of the grafted tendon at least temporarily after ACL reconstruction. These potentially negative mechanical effects need to be taken into account when considering clinical use of VEGF.
Background: Medial ulnar collateral ligament insufficiency of the elbow can be a devastating injury in the throwing athlete. Reconstruction of the medial ulnar collateral ligament was initially described by Jobe and associates; good clinical results have been described after this procedure. The authors' experience with this technique raised several concerns, and thus the “docking” procedure was developed as an alternative method for medial ulnar collateral ligament reconstruction of the elbow. The early results of the docking technique were good. The authors wish to investigate the intermediate-term clinical results of this method in a large group of athletes.
Hypothesis: The docking technique can return overhead-throwing athletes to sport with minimal perioperative morbidity.
Study Design: Case series; Level of evidence, 4.
Methods: During a 3-year period, 100 consecutive overhead-throwing athletes were treated with surgical reconstruction using the docking technique. The inclusion criteria were as follows: (1) a history of medial elbow pain that prevented throwing, (2) a preoperative standard noncontrast magnetic resonance image demonstrating medial ulnar collateral ligament injury, (3) clinically apparent medial ulnar collateral ligament insufficiency, and (4) an overhead-throwing athlete. At the time of surgery, all patients underwent routine arthroscopic assessment. The ulnar nerve was transposed in 22 cases. The mean follow-up was 36 months (range, 24-60 months).
Results: Ninety of 100 (90%) patients were able to compete at the same or a higher level than before medial ulnar collateral ligament injury for more than 12 months as noted at the follow-up interval; 7 patients were able to compete at a lower level. Only 3 patients suffered postoperative complications.
Conclusion: The docking technique reliably returns athletes to competitive throwing with a low perioperative morbidity.
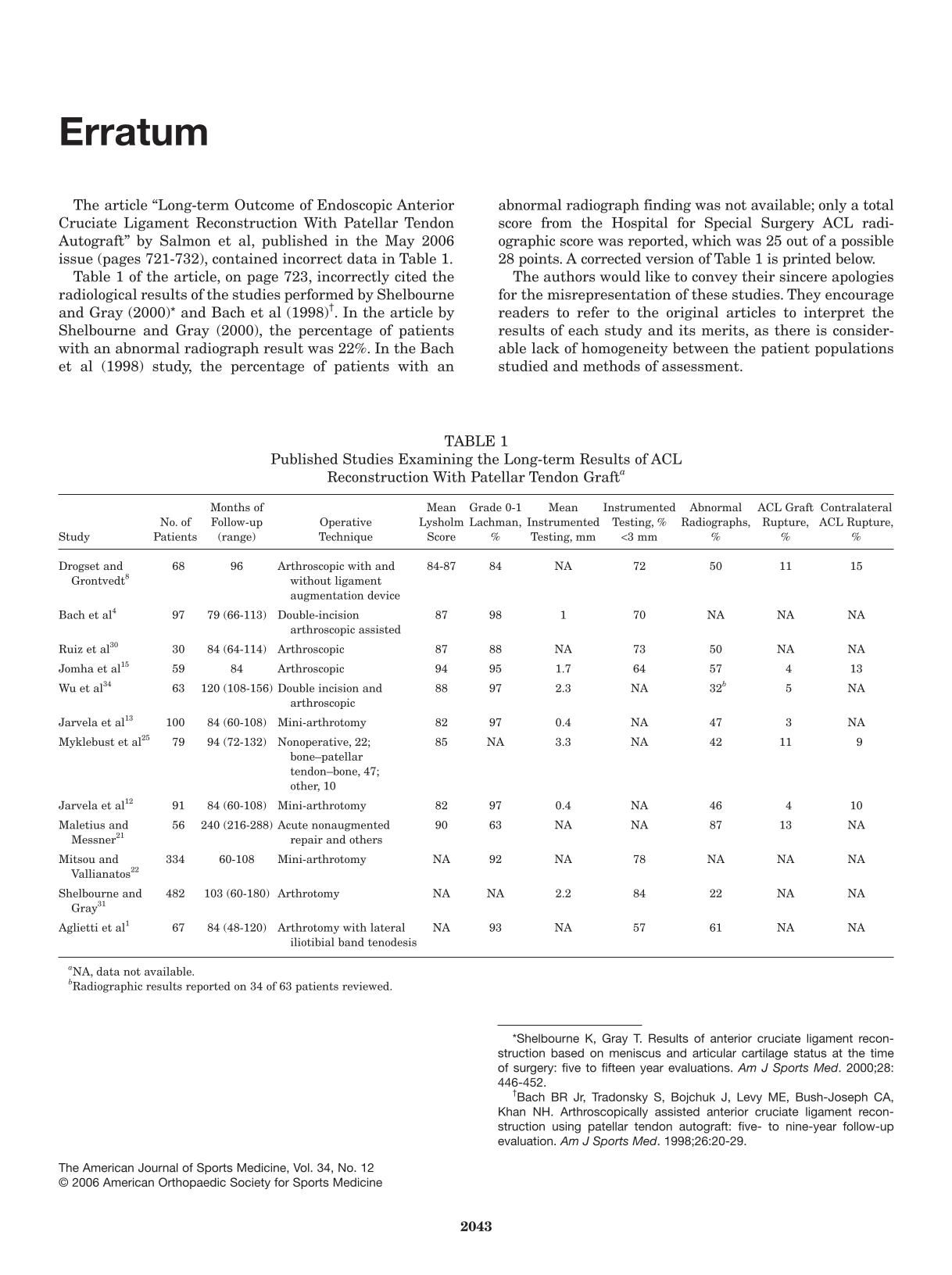
Background: There are still controversies about graft selection for primary anterior cruciate ligament reconstruction. Prospective randomized long-term studies are needed to determine the differences between the materials.
Hypothesis: Five years after anterior cruciate ligament reconstruction, there is a difference between hamstring and patellar tendon grafts in development of degenerative knee joint disease.
Study Design: Randomized controlled trial; Level of evidence, 1.
Methods: From June 1999 to March 2000, 64 patients were included in this prospective study. A single surgeon performed primary arthroscopically assisted anterior cruciate ligament reconstruction in an alternating sequence. In 32 patients, anterior cruciate ligament reconstruction was performed with hamstring tendon autograft, whereas in the other 32 patients, anterior cruciate ligament reconstruction was performed with patellar tendon autograft.
Results: At the 5-year follow-up, no statistically significant differences were seen with respect to the Lysholm score, clinical and KT-2000 arthrometer laxity testing, anterior knee pain, single-legged hop test, or International Knee Documentation Committee classification results; 23 patients (82%) in the hamstring tendon group and 23 patients (88%) in the patellar tendon group returned to their preinjury activity levels. Graft rupture occurred in 2 patients from the hamstring tendon group (7%) and in 2 patients from the patellar tendon group (8%). Grade B abnormal radiographic findings were seen in 50% (13/26) of patients in the patellar tendon group and in 17% (5/28) of patients in the hamstring tendon group (P = .012).
Conclusion: Both hamstring and patellar tendon grafts provided good subjective outcomes and objective stability at 5 years. No significant differences in the rate of graft failure were identified. Patients with patellar tendon grafts had a greater prevalence of osteoarthritis at 5 years after surgery.
Background: Numerous studies have investigated the biomechanical properties of meniscal repair techniques. One of the most commonly discussed parameters is the failure load in the axis of insertion, although little is known about the distraction forces actually occurring at repaired bucket-handle lesions.
Hypothesis: There are clinically relevant distraction forces on repaired meniscus bucket-handle lesions.
Study Design: Controlled laboratory study.
Methods: Meniscus bucket-handle lesions were created and repaired in human cadaveric knees with a vertical suture made from a braided steel wire. A small-sized load sensor was connected to the wire at the periphery of the meniscus. The distraction forces acting on the lesion were measured at different knee joint angles (0°-120° of flexion) with internal and external rotation and with and without weight loading. Forces in excess of 10 N were considered to have clinical relevance.
Results: Mean forces on the meniscus repair ranged from 1.64 to 4.72 N. Irrespective of the modalities (ie, different flexion angles, weight load, direction of rotation), it was found that the forces were well below the cutoff value of 10 N (P < .01). Increasing flexion angles generally did not cause an increase in distraction forces.
Conclusion: The data suggest that distraction forces are not the primary factor in the mechanical stability of meniscal repair. It must therefore be assumed that other factors such as shear forces are of greater significance.
Clinical Relevance: The results may help to validate the biomechanical properties of different meniscal repair techniques.
Background: Female athletes have a higher incidence of anterior cruciate ligament injuries than do male athletes in similar sports. Hormones, particularly estrogen, have been indicated by some studies to be correlated with the disproportionate number of anterior cruciate ligament injuries in female athletes.
Hypothesis: Estrogen does not affect the mechanical or material properties of primate anterior cruciate ligaments or patellar tendons.
Study Design: Controlled laboratory study.
Methods: Twenty-six cynomolgus monkeys (Macaca fascicularis) were divided into 2 groups: sham operated (estrogen maintained, n = 12) and ovariectomized (estrogen deficient, n = 14). After 2 years, the animals were sacrificed, and various properties of ligaments were tested. Two different ligaments were studied, the anterior cruciate ligament and patellar tendon.
Results: No differences were found between the sham-operated (sham) and ovariectomized group for failure load (anterior cruciate ligament: sham, 394 ± 67 N; ovariectomized, 392 ± 96 N; P > .74), stiffness, elongation at failure, ultimate stress (anterior cruciate ligament: sham, 115 ± 30 MPa; ovariectomized, 128 ± 36 MPa; P > .58), ultimate strain, modulus, failure sites, or energy to failure.
Conclusion: Endogenous estrogen does not directly affect the mechanical or material properties of the anterior cruciate ligament or the patellar tendon of cynomolgus macaques.
Clinical Relevance: This study supports the idea that knee ligament injury in female athletes is not a direct result of estrogen's effect on ligament properties.
Background: Cryotherapy and compression have been shown to decrease pain and improve function. The dosage and timing of these options remain unclear.
Purpose: To examine the effects of a standardized compression and cryotherapy device (Cryo/Cuff) on midportion Achilles tendon microcirculation during intermittent administration.
Study Design: Descriptive laboratory study.
Methods: Twenty-six subjects were included (13 men and 13 women; age, 32.3 ± 12 years; body mass index, 25.4 ± 5 kg/m2). Each underwent three 10-minute applications of the device, followed by a 10-minute recovery period. A continuous real-time assessment of parameters of Achilles tendon midportion microcirculation was performed with a laser Doppler spectrophotometry system.
Results: Superficial tendon oxygen saturation dropped significantly from 35.9 ± 21 arbitrary units (AU) to 13.5 ± 15, 15.9 ± 16, and 11.1 ± 11 AU (P = .0001) during each period of cryo-compression, respectively. There was significant increase during the recovery period (55.4 ± 29, 65.2 ± 26, and 65.7 ± 27 AU; P = .003), up to +83% of the baseline level. At 8-mm tendon depth, cryo-compression preserved local oxygen with -4% (P = .001) of the baseline level and small but significant increased oxygen saturation of up to +13% (P = .0001). Relative postcapillary venous tendon filling pressures were favorably reduced both superficially (57% ± 34%, 67% ± 27%, and 64% ± 38%, respectively; P = .0004) and deep (76% ± 13%, 79% ± 11%, and 78% ± 18%, respectively; P = .0002). Superficial capillary blood flow was reduced from 48.4 ± 48 to 5 ± 7, 4 ± 5, and 3 ± 4 AU at each period, respectively (–94%, P = .0003), with increased flow during recovery periods of up to 58 ± 64, 58 ± 79, and 47 ± 71 AU, respectively (+20%, P = .265). Deep flow was reduced from 197 ± 147 to 66.7 ± 64, 55 ± 46, and 43 ± 39 AU, respectively (–78%, P = .0002) without increase during recovery periods.
Conclusion: Cryo/Cuff exerts beneficial effects on the microcirculatory level of the midportion Achilles tendon with decreased capillary blood flow, preserved deep tendon oxygen saturation, and facilitated venous capillary outflow.
Background: Hockey is one of the top sports for participation in youth in Canada. There are limited data on the epidemiology of injury in youth hockey.
Purpose: Through implementation and validation of an injury surveillance system, youth ice hockey injury rates, risk factors, and mechanisms of injury will be examined.
Study Design: Descriptive epidemiology study.
Methods: During the 2004-2005 season in minor hockey in Calgary, Alberta, Canada, 71 hockey teams (N = 986) were studied, including teams from each age group (Atom, 9/10 years; Pee Wee, 11/12 years; Bantam, 13/14 years; Midget, 15/16 years) and division of play (7-10 divisions per age group). A certified athletic therapist or candidate did weekly assessments of any identified hockey injury. Injury definition included any injury occurring during the regular hockey season that required medical attention, removal from a session, or missing a subsequent session.
Results: Of the 986 participating players, 216 players sustained a total of 296 injuries in the 2004-2005 season. The overall injury rate was 30.02 injuries per 100 players per season (95% confidence interval, 27.17-32.99) or 4.13 injuries per 1000 player hours (95% confidence interval, 3.67-4.62). Forty-five percent of all injuries occurred during body checking. Compared with the youngest age group, Atom, the risk of injury was greater in Pee Wee (relative risk, 2.97; 95% confidence interval, 1.63-5.8), Bantam (relative risk, 3.72; 95% confidence interval, 2.08-7.14), and Midget (relative risk, 5.43; 95% confidence interval, 3.14-10.17) leagues. The risk of injury in Pee Wee was greatest in the most elite divisions (relative risk, 2.45; 95% confidence interval, 1.15-5.81). Concussion, shoulder sprain/dislocation, and knee sprain were the most common injuries.
Conclusion: Significant differences in injury rates were found by age and division of play. The public health significance of body checking injury in minor hockey is great. Future research will include expansion of surveillance to further examine body checking injuries and prevention strategies in minor hockey.
Background: The ankle joint requires very precise neuromuscular control during the transition from terminal swing to the early stance phase of the gait cycle. Altered ankle joint arthrokinematics and muscular activity have been cited as potential factors that may lead to an inversion sprain during the aforementioned time periods. However, to date, no study has investigated patterns of muscle activity and 3D joint kinematics simultaneously in a group of subjects with functional instability compared with a noninjured control group during these phases of the gait cycle.
Purpose: To compare the patterns of lower limb 3D joint kinematics and electromyographic activity during treadmill walking in a group of subjects with functional instability with those observed in a control group.
Study Design: Controlled laboratory study.
Methods: Three-dimensional angular velocities and displacements of the hip, knee, and ankle joints, as well as surface electromyography of the rectus femoris, peroneus longus, tibialis anterior, and soleus muscles, were recorded simultaneously while subjects walked on a treadmill at a velocity of 4 km/h.
Results: Before heel strike, subjects with functional instability exhibited a decrease in vertical foot-floor clearance (12.62 vs 22.84 mm; P < .05), as well as exhibiting a more inverted position of the ankle joint before, at, and immediately after heel strike (1.69°, 2.10°, and -0.09° vs -1.43°, -1.43°, and -2.78°, respectively [minus value = eversion]; P < .05) compared with controls. Subjects with functional instability were also observed to have an increase in peroneus longus integral electromyography during the post–heel strike time period (107.91%[.dotmath]millisecond vs 64.53%[.dotmath]millisecond; P < .01).
Conclusion: The altered kinematics observed in this study could explain the reason subjects with functional instability experience repeated episodes of ankle inversion injury in situations with only slight or no external provocation. It is hypothesized that the observed increase in peroneus longus activity may be the result of a change in preprogrammed feed-forward motor control.
Background: Inappropriately sized tennis racket grip is often cited in the popular media as a risk factor for overuse injuries about the forearm and elbow. Currently, a hand measurement technique developed by Nirschl is commonly used by tennis racket manufacturing companies as the method for determining a player's “recommended” grip size.
Hypothesis: Quarter-inch changes from that recommended by Nirschl in tennis racket grip size will have no significant effect on forearm muscle firing patterns.
Study Design: Controlled laboratory study.
Methods: Sixteen asymptomatic Division I and II collegiate tennis players performed single-handed backhand ground strokes with rackets of 3 different grip sizes (recommended measurement, undersized 1/4 in, and oversized 1/4 in). Fine-wire electromyography was used to measure muscle activity in extensor carpi radialis longus and brevis, extensor digitorum communis, flexor carpi radialis, and pronator teres. Repeated-measure analysis of variance was used for within-group comparisons, comparing different grips in specified phases for backhand ground strokes (P [.lessequal] .05).
Results: There were no significant differences in muscle activity between small, recommended, or big grips in any muscle tested.
Conclusion: Based on these findings, tennis racket grip size 1/4 in above or below Nirschl's recommended measurement does not significantly affect forearm muscle firing patterns.
Clinical Relevance: Alterations in tennis racket grip size within 1/4 in of Nirschl's recommended sizing do not have a significant effect on forearm muscle activity and therefore may not represent a significant risk factor for upper extremity cumulative trauma, such as lateral epicondylitis.
Background: After trauma, internal knee lesions are found in approximately two thirds of patients. However, magnetic resonance imaging abnormalities have also been described in asymptomatic volunteers.
Hypothesis: Not all visualized lesions in symptomatic posttraumatic knees are the result of recent trauma; there are subgroups of lesions that may be preexistent.
Study Design: Cross-sectional study (prevalence); Level of evidence, 2.
Methods: Patients visiting their general practitioners after knee trauma were invited for magnetic resonance imaging of both knees. Prevalence of knee abnormalities was compared between symptomatic and asymptomatic knees. Multivariable analysis was performed to investigate the association between lesions that were seen in symptomatic and asymptomatic knees (ie, effusion and meniscal tears) and recent trauma, history of old trauma, age, and osteoarthritis.
Results: In 134 participants, ligament lesions were found almost exclusively in symptomatic knees. Meniscal lesions and effusion were almost equally found in symptomatic and asymptomatic knees. Effusion was related to recent trauma (odds ratio, 14.0; 95% confidence interval, 5.0-39.6) and osteoarthritis (odds ratio, 4.7; 95% confidence interval, 1.4-15.5) but not to history of old trauma and age. Meniscal tears were more common in older patients (odds ratio, 1.09; 95% confidence interval, 1.05-1.12) but were not related to osteoarthritis. History of old trauma was more strongly related to the group of radial, longitudinal, and complex meniscal tears (odds ratio, 8.6; 95% confidence interval, 3.3-22.5) than to horizontal tears (odds ratio, 2.3; 95% confidence interval, 0.9-5.6). Recent trauma was not related to horizontal meniscal tears but was strongly related to other types of meniscal tears (odds ratio, 3.2; 95% confidence interval, 1.4-6.9).
Conclusion: Ligament knee lesions are most probably the result of recent trauma. Radial, longitudinal, and complex meniscal tears are strongly related to trauma, whereas horizontal meniscal tears and effusion may be preexistent in many cases.
Background: Overuse tendon injuries are frequent. Corticosteroid injections are commonly used as treatment, although their direct effects on the material properties of the tendon are poorly understood.
Purpose: To examine the influence of corticosteroids on the tensile strength of isolated collagen fascicles.
Study Design: Controlled laboratory study.
Methods: Single strands (300-500 [.mu]m) of rat-tail collagen fascicles were incubated in either high (1 mL of 40 mgmL-1 mixed with 0.5 mL saline 9%) or low (1 mL of 40 mgmL-1 mixed with 2 mL saline 9%) concentration of methylprednisolone acetate (Depomedrol) for 3 or 7 days, while the control segment from the same fascicle was kept in saline (N = 64). After the incubation period, the fascicles underwent displacement to failure in a mechanical test rig at 0.13 mm/s, and thereafter hydroxylysyl pyridinoline and lysyl pyridinoline cross-link content was evaluated in a high-performance liquid chromatography system. Data for each group were analyzed with a 2-way analysis of variance (time × incubation) for ultimate stress (mean ± standard deviation).
Results: In the high-concentration groups, strength was reduced after 3 (16.6 ± 4.6 MPa) and 7 (8.6 ± 1.7 MPa) days compared to the controls (30.2 ± 5.0 MPa and 25.6 ± 4.6 MPa, respectively; P < .05). In the low-concentration groups, strength was reduced after 3 (12.0 ± 3.1 MPa) and 7 days (10.9 ± 2.5 MPa) compared to the controls (31.5 ± 5.0 MPa and 32.4 ± 5.6 MPa, respectively; P < .05). The amount of cross-linking was unaffected by the intervention.
Conclusion: Data show that the tensile strength of isolated fascicles is markedly reduced after 3-and 7-day incubation in both high and low concentration of corticosteroids, although the observed effect on whole tendon remains unknown.
Clinical Relevance: Corticosteroids may weaken specific regions of the injected tendon and leave it more prone to rupture. This weakening effect is manifested in the individual collagen fascicles that constitute the tendon.
Background: Running shoes are designed to accommodate various arch types to reduce the risk of lower extremity injuries sustained during running. Yet little is known about the biomechanical changes of running in the recommended footwear that may allow for a reduction in injuries.
Purpose: To evaluate the effects of motion control and cushion trainer shoes on running mechanics in low-and high-arched runners.
Study Design: Controlled laboratory study.
Methods: Twenty high-arched and 20 low-arched recreational runners (>10 miles per week) were recruited for the study. Three-dimensional kinematic and kinetics were collected as subjects ran at 3.5 ms-1 ± 5% along a 25-m runway. The motion control shoe evaluated was the New Balance 1122, and the cushioning shoe evaluated was the New Balance 1022. Repeated-measures analyses of variance were used to determine if low- and high-arched runners responded differently to motion control and cushion trainer shoes.
Results: A significant interaction was observed in the instantaneous loading rate such that the low-arched runners had a lower instantaneous loading rate in the motion control condition, and the high-arched runners had a lower instantaneous loading rate in the cushion trainer condition. Significant main effects for shoe were observed for peak positive tibial acceleration, peak-to-peak tibial acceleration, mean loading rate, peak eversion, and eversion excursion.
Conclusion: These results suggest that motion control shoes control rearfoot motion better than do cushion trainer shoes. In addition, cushion trainer shoes attenuate shock better than motion control shoes do. However, with the exception of instantaneous loading rate, these benefits do not differ between arch type.
Clinical Relevance: Running footwear recommendations should be based on an individual's running mechanics. If a mechanical analysis is not available, footwear recommendations can be based empirically on the individual's arch type.
Background: Recent follow-up studies have reported a high incidence of joint degeneration in patients with anterior cruciate ligament reconstruction. Abnormal kinematics after anterior cruciate ligament reconstruction have been thought to contribute to the degeneration.
Hypothesis: Anterior cruciate ligament reconstruction, which was designed to restore anterior knee laxity under anterior tibial loads, does not reproduce knee kinematics under in vivo physiological loading conditions.
Study Design: Controlled laboratory study.
Methods: Both knees of 7 patients with complete unilateral rupture of the anterior cruciate ligament were magnetic resonance imaged, and 3D models were constructed from these images. The anterior cruciate ligament of the injured knee was arthroscopically reconstructed using a bone–patellar tendon–bone autograft. Three months after surgery, the kinematics of the intact contralateral and reconstructed knees were measured using a dual-orthogonal fluoroscopic system while the subjects performed a single-legged weightbearing lunge. The anterior laxity of both knees was measured using a KT-1000 arthrometer.
Results: The anterior laxity of the reconstructed knee as measured with the arthrometer was similar to that of the intact contralateral knee. However, under weightbearing conditions, there was a statistically significant increase in anterior translation of the reconstructed knee compared with the intact knee at full extension (approximately 2.9 mm) and 15° (approximately 2.2 mm) of flexion. In addition, there was a mean increase in external tibial rotation of the anterior cruciate ligament–reconstructed knee beyond 30° of flexion (approximately 2° at 30° of flexion), although no statistical significance was detected.
Conclusion: The data demonstrate that although anterior laxity was restored during KT-1000 arthrometer testing, anterior cruciate ligament reconstruction did not restore normal knee kinematics under weightbearing loading conditions.
Clinical Relevance: Future reconstruction techniques should aim to restore function of the knee under physiological loading conditions.
Background: The most frequent injuries in badminton players are in the lower extremities, especially in the Achilles tendon.
Hypothesis: The game of badminton may be related to abnormal intratendinous flow in the Achilles tendon as detected by color Doppler ultrasound. To a certain extent, this blood flow might be physiological, especially when examined after match.
Study Design: Cohort study (prevalence); Level of evidence, 3.
Methods: Seventy-two elite badminton players were interviewed regarding Achilles tendon pain (achillodynia) in the preceding 3 years. Color Doppler was used to examine the tendons of 64 players before their matches and 46 players after their matches. Intratendinous color Doppler flow was graded from 0 to 4. The Achilles tendon was divided into dominant (eg, right side for right-handed players and vice versa) and nondominant side and classified as midtendon, preinsertional, and calcaneal areas.
Results: Of 72 players, 26 had experienced achillodynia in 34 tendons, 18 on the dominant side and 16 on the nondominant side. In 62% of the players with achillodynia, the problems had begun slowly, and the median duration of symptoms was 4 months (range, 0-36 months). Thirty-five percent had ongoing pain in their tendons for a median duration of 12 months (range, 0-12 months). Achillodynia was not associated with the self-reported training load or with sex, age, weight, singles or doubles players, or racket side. Forty-six players were scanned before and after match. At baseline, color Doppler flow was present in the majority of players, and only 7 (16%) players had no color Doppler flow in either tendon. After match, all players had some color Doppler flow in 1 or both tendons. Achillodynia and color Doppler flow were related in the nondominant Achilles tendon (chi-square, P = .008). The grades of Doppler flow also increased significantly after match in the preinsertional area in both the nondominant (P = .0002) and dominant (P = .005) side tendons.
Conclusion: A large proportion of the players had experienced achillodynia and habitually played with a degree of pain that demanded medication. The self-reported pain was associated with increased intratendinous color Doppler flow in the nondominant Achilles tendon. Doppler flow was found in most players before and in all players after the match and therefore may in part be a physiological response to activity.
Failed anterior cruciate ligament (ACL) reconstruction presents a difficult clinical challenge. Successful revision ACL reconstruction depends on identifying the causes of failure and correcting technical or diagnostic errors. Failed ACL reconstruction may be either traumatic or atraumatic. Atraumatic failures may be attributable to technical errors, diagnostic errors, or failure of graft incorporation. Published outcomes of revision ACL reconstruction have been worse than for primary ACL reconstruction. The preoperative evaluation, surgical techniques, and clinical outcomes of revision ACL reconstruction are reviewed.