
Editorial
Select search scope: search across all journals or within the current journal
Underrepresented minority groups (URMs) in surgery are not significantly increasing despite evidence suggesting that diversity in health care providers leads to excellent patient outcomes and care. Efforts to increase URM representation in surgical residency programs are essential for addressing disparities and improving health care delivery.
This retrospective study outlines a three-phase strategy implemented at a large academic-affiliated hospital to increase URM representation in its general surgery residency program. The strategy encompassed interview selection with a holistic review and implicit bias training for interviewers, modification of the interview scoring rubric, and post-interview recruitment efforts, including a virtual second look event for URM applicants.
Following the implementation of these strategies, the URM match rate improved from 0 to 33.3% in the first year and was sustained at 33.3% in the subsequent year. Consequently, the representation of URMs in the residency program rose from 6.7% before our intervention to 13.3% afterwards.
This structured approach successfully increased URM representation in a surgical residency program, affirming the success of targeted recruitment strategies. By promoting a diverse and inclusive environment, the program better reflects the community it serves, with aims at improved patient care and patient satisfaction.
It has been reported that the oral and gut microbiomes are associated with the prognosis in patients who undergo surgery, chemotherapy, and radiation for colorectal cancer. This study is the first to identify a correlation between the number of healthy teeth, which is an oral health indicator, and the efficacy of preoperative chemotherapy for rectal cancer.
This retrospective single-center study included 30 patients who underwent radical surgery after preoperative chemoradiotherapy (CRT) between December 2013 and June 2021. The relationship between number of teeth before CRT and the efficacy of CRT, CRT-related adverse events, postoperative complications, and long-term postoperative outcomes was examined.
The number of healthy teeth was significantly greater in patients with downstaging of their disease than in those without downstaging (
The number of healthy teeth predicted the response to preoperative CRT, postoperative complications, and the outcome of subsequent surgery in patients with rectal cancer.
Over 50% of hospitalized patients have comorbid psychiatric diagnoses, resulting in increased risk of morbidity such as longer lengths of stay, worse health-related quality of life, and increased mortality. However, data regarding colorectal surgery postoperative outcomes in patients with psychiatric diagnoses (PD) are limited.
We queried a single institution’s National Surgical Quality Improvement Program from 2013-2019 for major colorectal procedures. Postsurgical outcomes for patients with and without PD were compared. Primary outcomes were prolonged length of stay (pLOS) and 30-day readmission.
From a total of 1447 patients, 402 (27.8%) had PD. PD had more smokers (20.9% vs 15%) and higher mean body mass index (29.1 kg/m2 vs 28.2 kg/m2). Bivariate outcomes showed more surgical site infections (SSI) (10.2% vs 6.12%), reoperation (9.45% vs 6.35%), and pLOS (34.8% vs 29.0%) (all
Psychiatric diagnoses are a risk factor for adverse outcomes after colorectal procedures. Further studies are needed to evaluate the benefit of perioperative mental health support services for these patients.
The C-reactive protein (CRP)-albumin-lymphocyte (CALLY) index is a novel immune nutrition scoring system associated with cancer prognosis. This study investigated the association between the CALLY index and the long-term outcomes of patients with gastric cancer.
We included 175 patients with gastric cancer who underwent curative gastrectomies at the Department of Surgery, International University of Health and Welfare Hospital between January 2011 and October 2019. The CALLY index was calculated based on the levels of serum albumin, serum CRP, and peripheral lymphocyte count. Utilizing both univariate and multivariate analyses, the prognostic value of the CALLY index was investigated.
In the multivariate analyses, disease stage (hazard ratio [HR], 7.85; 95% confidence interval [CI], 3.31-18.6;
The CALLY index may be associated with a poor prognosis for gastric cancer, highlighting the utility of a comprehensive assessment using inflammatory, nutritional, and immunological statuses.
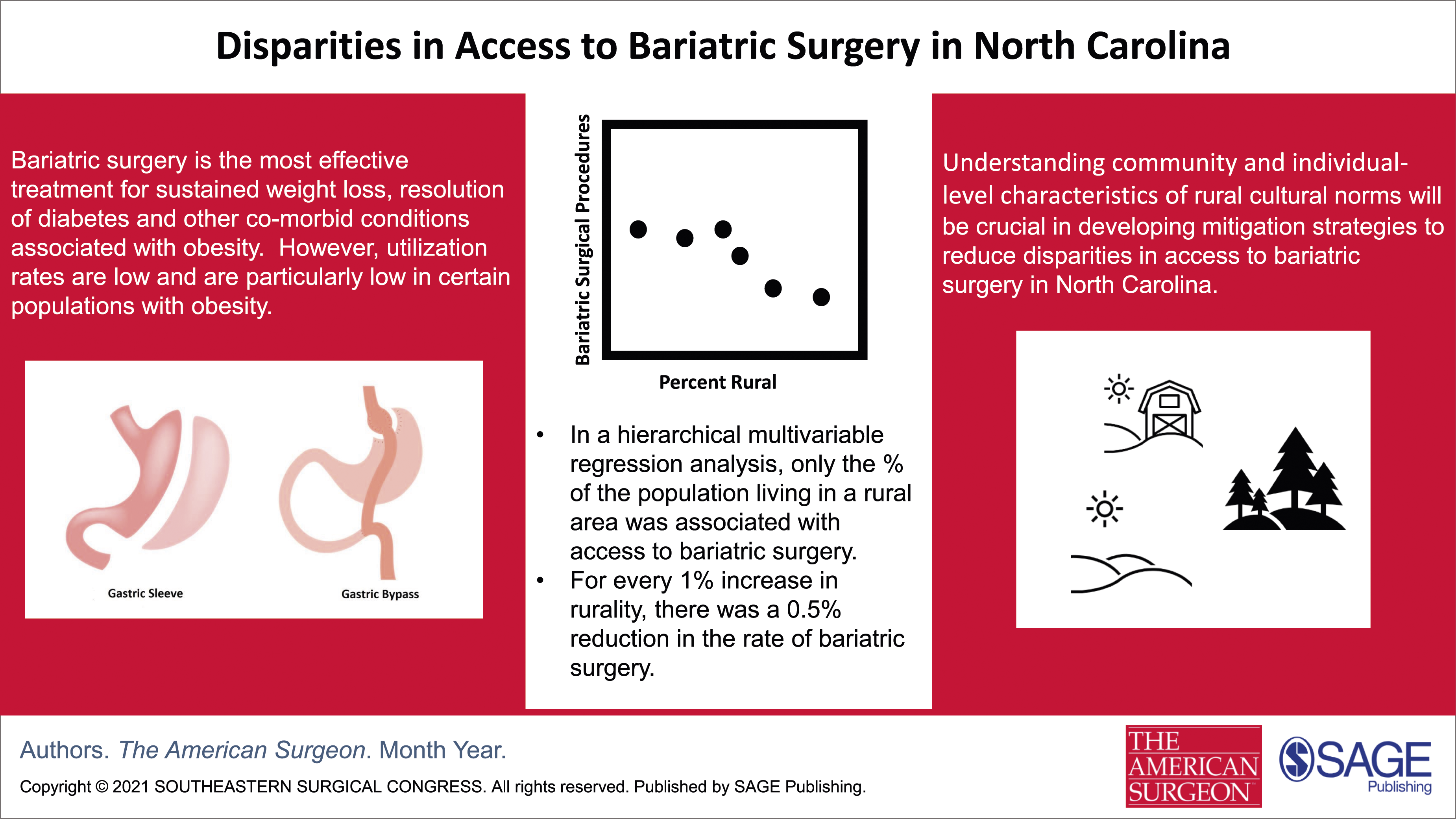
This study sought to identify factors that contribute to disparities in access to bariatric surgery in North Carolina (NC).
Using the rate of bariatric surgery in the county with the best health outcome as the reference, we calculated the Surgical Equity Index (SEI) in the remaining counties in NC.
Approximately 2.95 million individuals (29%) were obese in NC. There were 992 (.5%) bariatric procedures performed on a population of 194 209 individuals with obesity in the Reference County (RC). The mean SEI for bariatric surgery in NC was .47 (SD .17, range .15-.95). A statistically significant difference was observed in 89 counties. Univariable analyses identified the following variables to be significantly associated with the SEI: percent of population living in rural areas (% rural) (relative rate change in SEI [RR] = .994, 95% CI .92-.997; <.0001), median household income (RR = 1.0, 95% CI = 1.0-1.0;
The percent rural is the most significant predictor of disparities in access to bariatric surgery. For every 1% increase in % rural, the rate of surgery decreased by .5%. Understanding the characteristics of rurality that are barriers to access is crucial to mitigate disparities in bariatric surgical access in NC.
Liver failure patients are at increased risk of surgical complications. The decision to perform a colonic anastomosis vs a colostomy in urgent colorectal surgery remains unclear.
The ACS-NSQIP database was queried for patients undergoing nonelective colorectal surgery between 2016 and 2018. MELD score was calculated and stratified into 3 groups. Subgroup analysis of the high-MELD group was performed.
Higher MELD scores were associated with significantly higher mortality. Colostomy formation was consistent between intermediate and high-MELD groups. In high-MELD patients, colonic anastomosis was associated with higher mortality than those receiving colostomy (41.1% vs 28.4%,
High-MELD patients undergoing nonelective colorectal surgery have increased risk of complications such as mortality. Patients in this group receiving an anastomosis have increased complications and mortality, and may benefit from colostomy formation.
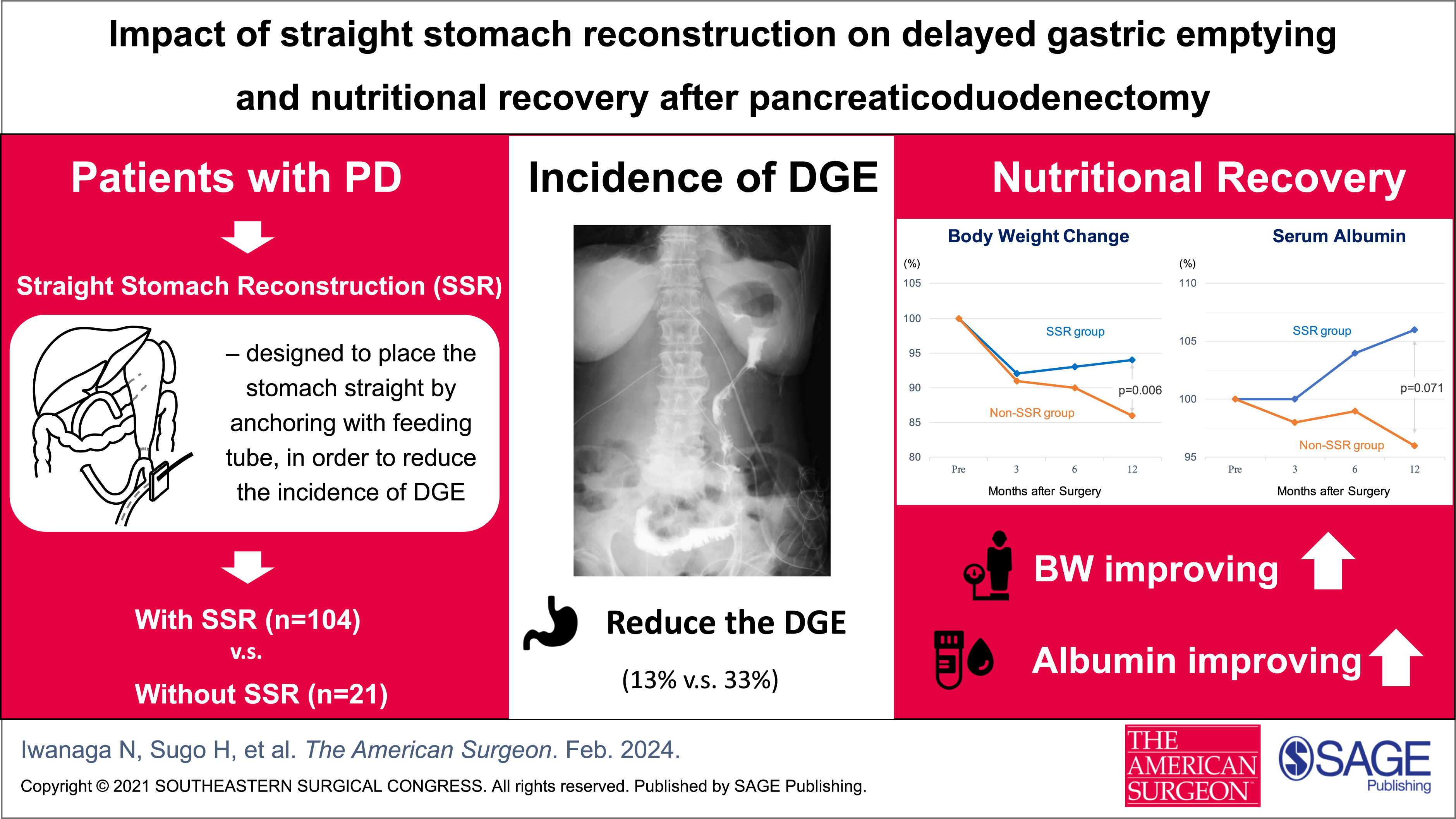
The aim of this study was to evaluate the effectiveness of a modified reconstruction technique—anchored straight stomach reconstruction—in reducing the incidence of delayed gastric emptying (DGE) after pancreaticoduodenectomy (PD) and its impact on postoperative nutritional recovery.
A case series analysis of 125 consecutive PD patients was conducted: 104 of them had undergone anchored straight stomach reconstruction (SSR group) and the remaining 21 without (Non-SSR group). The incidence of DGE and the change in postoperative nutritional status (body weight and serum albumin level during 12 months post-surgery) were compared.
The incidence of DGE in the SSR group (13%) was significantly lower than that in the Non-SSR group (33%) (
Straight stomach reconstruction is able to reduce DGE in patients after PD and also improves their postoperative nutritional recovery.
To determine outcomes after on lay large ventral hernia repair in obese patients.
Large ventral hernia repairs (VHR) in obese patients remain a challenge. Obesity is a risk factor for intraoperative difficulties and postoperative complications. Recurrence rates after VHR in obese patients range between 12-50% versus 10% in nonobese patients. While results of laparoscopic techniques in VHR compare favorably to open, outcomes in correlation with obesity, technique, and defect size are less understood.
A single surgeon’s experience of 329 consecutive VHR between 2013-2022 was retrospectively reviewed. Inclusion criteria were obesity (BMI >30) and large hernia defects (>5 cm). A modified onlay technique was used which included component release and a lightweight monofilament polypropylene mesh. Primary outcome measures were hernia recurrence and wound complications.
A total of 56 patients met inclusion criteria. Patients were majority male (n=30, 54%), with a median age of 58.5 years (inter quartile range (IQR) 33-83), and median BMI of 36 kg/m2 (IQR: 30-72). Median hernia defect size was 8 cm (IQR: 5-15). Twenty patients had undergone prior mesh repairs. Median follow-up was 52 months (IQR: 6 months-9 years). Two patients experienced recurrence (3.6%) and four experienced wound complications (four seromas, one panniculitis, 8.9%). No patients suffered flap ischemia or necrosis.
Obesity is a risk factor for poor outcomes after VHR. We developed a protocol for obese patients with large defects involving a modified onlay technique which demonstrates comparable results to other VHR techniques in obese patients.
The aim of this study was to investigate the demographic and molecular characteristics, overall survival (OS), cancer-specific survival (CSS), and prognostic factors affecting the survival of patients with single primary breast cancer (SPBC) and patients with multiple primary cancers in their life time in which one of them is breast cancer (MPC).
Using data from SEER 17 Research Plus, patients with breast cancer diagnosed between 2010 and 2019 were included in this study. Race, marital status, laterality, tumor size, molecular subtype, grade, stage, radiotherapy-chemotherapy treatment, and surgery data were analyzed in the data obtained after excluding patients with missing values. Kaplan-Meier survival analysis was used for survival analysis, and Cox regression analysis was used to evaluate the prognostic factors.
573175 patients were included in the study. The mean age of MPC patients was significantly higher than SPBC patients (65.99 ± 12.68, 60.33 ± 13.47,
Although patients with SPBC have worse prognostic tumor characteristics, OS and CSS rates are better than patients with MPC.
Oral assessments are essential components of board certification in numerous fields, as they provide insight into problem-solving capacity and clinical reasoning. The development of clinical reasoning often begins in undergraduate medical education and remains a challenge to assess.
We developed a pilot oral assessment to evaluate medical student oral presentations and systematically assess clinical reasoning. This was incorporated into a previously existing cumulative assessment at the conclusion of the third year of medical school, with the intent to demonstrate feasibility and future reliability of this exam format.
This pilot oral assessment was developed using content taught during third year clerkships. A modified Assessment of Reasoning Tool (ART) was used as the evaluation metric. It was conducted virtually to include faculty members from multiple disciplines and accommodate schedules and space limitations.
A total of 152 third year medical students completed the exam, with a total of 15 faculty examiners. 89% of medical students scored as complete in hypothesis directed history, 93% in problem representation, 86% in prioritized differential diagnoses, and 67% in effectively directing management. Most examiners felt an oral assessment is effective to determine a medical student’s clinical reasoning ability.
Virtual oral assessments of clinical reasoning can be incorporated in undergraduate medical education to identify students struggling with components of clinical reasoning, while also allowing maximum flexibility for the clinician educator workforce as examiners. Longitudinal use of these exams would be valuable to track the development of clinical reasoning across the medical school curriculum.
The objective of this study is to analyze the outcomes of patients with resectable/borderline resectable PDAC who receive total neoadjuvant therapy vs upfront surgery.
Patients who were treated at a single institution from 2006 to 2021 were included. The primary outcome was overall survival (OS). Secondary outcomes included disease free survival (DFS), rates of lymph node positivity, and R0 resection. All survival analyses were performed with intention-to-treat.
26 patients received neoadjuvant chemotherapy and radiation (TNT), 28 received neoadjuvant chemotherapy only (NAC), and 168 received upfront surgery. Demographics were comparable across all three groups. Patients who received TNT or NAC had longer OS and DFS compared to the surgery first patients (
Patients with resectable/borderline resectable PDAC who receive neoadjuvant therapy have longer OS and RFS relative to those who receive upfront surgery.
Nipple-sparing mastectomy (NSM) with deep inferior epigastric perforator (DIEP) flap reconstruction is a surgical option for select patients with or at risk of breast cancer. However, post-operative skin flap and nipple-areolar complex (NAC) necrosis remain common complications. This study aimed to identify factors associated with necrosis in patients undergoing NSM with DIEP reconstruction.
A retrospective cohort study was performed from 2015 to 2023. 74 variables were analyzed in patients undergoing NSM with DIEP. Patients were stratified into 3 groups based on post-operative skin/NAC necrosis: none, partial thickness, and full thickness. Comparative and descriptive statistics were performed via t-tests, ANOVA, and chi-squared tests.
34 women with 31 breast cancers met inclusion. 44% experienced necrosis: 15% partial thickness and 29% full thickness. The majority were white (85.3%) with mean age of 50 years (SD = 9.11). In patients with immediate DIEP reconstruction, hypoperfused areas identified by SPY angiography increased risk of necrosis (
In patients receiving NSM with DIEP flap reconstruction, those with hypoperfusion on SPY angiography and longer smoking history had higher necrosis rates. This supports the continued used of SPY angiography and the role of pre-operative counseling in former smokers with increased pack years on their risk of necrosis and the role of preventative measures in the perioperative setting.
Multi-organ metastases represent a substantial life-threatening risk for breast cancer (BC) patients. Nonetheless, the current dearth of assessment tools for patients with multi-organ metastatic BC adversely impacts their evaluation.
We conducted a retrospective analysis of BC patients with multi-organ metastases using data from the SEER database from 2010 to 2019. The patients were randomly allocated into a training cohort and a validation cohort in a 7:3 ratio. Univariate COX regression analysis, the LASSO, and multivariate Cox regression analyses were performed to identify independent prognostic factors in the training set. Based on these factors, a nomogram was constructed to estimate overall survival (OS) probability for BC patients with multi-organ metastases. The performance of the nomogram was evaluated using C-indexes, ROC curves, calibration curves, decision curve analysis (DCA) curves, and the risk classification system for validation.
A total of 3626 BC patients with multi-organ metastases were included in the study, with 2538 patients in the training cohort and 1088 patients in the validation cohort. Age, grade, metastasis location, surgery, chemotherapy, and subtype were identified as significant independent prognostic factors for OS in BC patients with multi-organ metastases. A nomogram for predicting 1-year, 3-year, and 5-year OS was constructed. The evaluation metrics, including C-indexes, ROC curves, calibration curves, and DCA curves, demonstrated the excellent predictive performance of the nomogram. Additionally, the risk grouping system effectively stratified BC patients with multi-organ metastases into distinct prognostic categories.
The developed nomogram showed high accuracy in predicting the survival probability of BC patients with multi-organ metastases, providing valuable information for patient counseling and treatment decision making.
The timely identification of both malignant and nonmalignant pancreatic lesions has the potential to significantly enhance prognosis and implement risk management strategies across various levels. microRNAs (miRs) and their corresponding targets play a crucial role in the development of pancreatic lesions and can serve as valuable diagnostic and therapeutic targets. The objective of our study was to investigate potential diagnostic markers that can effectively differentiate between malignant and nonmalignant pancreatic lesions.
Gene Expression Omnibus (GEO) database with GSE24279 dataset was utilized to screen differentially expressed miRNAs (DEMs). We utilized the TargetScanHuman database to predict the target genes associated with hsa-miR-150-3p, hsa-miR-150-5p, and hsa-miR-214-3p. Furthermore, a cohort comprising healthy individuals (n = 52), chronic pancreatitis (CP; n = 34), and pancreatic adenocarcinoma (PAAD; n = 53) patients was recruited to ascertain the levels of plasma markers.
We identified 3 miRNAs (hsa-miR-150-3p, hsa-miR-150-5p, and hsa-miR-214-3p) and 2 proteins (PCDH1 and AMN) as potential diagnostic markers for distinguishing between CP and PAAD. The area under the curve (AUC) values for all markers exceeded .800. Notably, a combination of plasma PCDH1 and AMN demonstrated excellent diagnostic performance (AUC = .921; 95% CI: .866-.977; sensitivity = .792; specificity = .941) in discriminating between CP and PAAD. In addition, the model of hsa-miR-150-3p, hsa-miR-150-5p, and hsa-miR-214-3p yielded an AUC of .928, sensitivity of .830, and specificity of .912, respectively.
Plasma levels of miRNAs (hsa-miR-150-3p, hsa-miR-150-5p, and hsa-miR-214-3p) and their corresponding targets (PCDH1 and AMN) hold promise as potential biomarkers for predicting PAAD in patients with CP.
Gallstone pancreatitis (GSP) is common in elderly patients and carries worse outcomes. Laparoscopic cholecystectomy (LC) is recommended for prevention of recurrent GSP. In frail populations, an endoscopic retrograde cholangiopancreatography with sphincterotomy (ERCP-s) is an alternative. Management guidelines of GSP in the elderly are lacking. This study aimed to investigate and compare management strategies for GSP in the elderly.
A retrospective comparison of outcome of patients aged ≥65 years with first presentation of GSP treated either with (1) LC only, (2) ERCP-s, (3) ERCP-S followed by LC, or (4) no intervention.
216 patients were included. Median age was 76 years (interquartile range 70-83). Most (80%, n = 172) had mild pancreatitis, whilst 12% (n = 26) had severe disease. 24% (n = 55) were treated with ERCP-s; 40% (n = 87) underwent LC alone; 11% (n = 23) had ERCP-s followed by LC; and 25% (n = 55) received no intervention. Patients without intervention were older (
Laparoscopic cholecystectomy represents the gold standard for elderly patients with GSP.
Optimization of antibiotic stewardship requires determining appropriate antibiotic treatment and duration of use. Our current method of identifying infectious complications alone does not attempt to measure the resources actually utilized to treat infections in patients. We sought to develop a method accounting for treatment of infections and length of antibiotic administration to allow benchmarking of trauma hospitals with regard to days of antibiotic use.
Using trauma quality collaborative data from 35 American College of Surgeons (ACS)-verified level I and level II trauma centers between November 1, 2020, and January 31, 2023, a two-part model was created to account for (1) the odds of any antibiotic use, using logistic regression; and (2) the duration of usage, using negative binomial distribution. We adjusted for injury severity, presence/type of infection (eg, ventilator-acquired pneumonia), infectious complications, and comorbid conditions. We performed observed-to-expected adjustments to calculate each center’s risk-adjusted antibiotic days, bootstrapped Observed/Expected (O/E) ratios to create confidence intervals, and flagged potential high or low outliers as hospitals whose confidence intervals lay above or below the overall mean.
The mean antibiotic treatment days was 1.98°days with a total of 88,403 treatment days. A wide variation existed in risk-adjusted antibiotic treatment days (.76°days to 2.69°days). Several hospitals were identified as low (9 centers) or high (6 centers) outliers.
There exists a wide variation in the duration of risk-adjusted antibiotic use amongst trauma centers. Further study is needed to address the underlying cause of variation and for improved antibiotic stewardship.
Congenital heart disease (CHD) is one the most common congenital anomalies, with a prevalence of 8-10 cases per 1000 live births in the United States. Congenital heart disease has been recognized as a risk factor for poor perioperative and postoperative outcomes in non-cardiac surgery. We aimed to determine if documentation of CHD-related diagnosis codes was associated with similar risks for trauma surgery.
Data were acquired from the 2010-2019 American College of Surgeons’ Trauma Quality Programs Participant Use Files. This study included trauma patients of all ages with one or more surgical procedures and at least one documented non-trauma (comorbidity) International Classification of Diseases code. Patients were stratified based on presence of CHD-related comorbidity codes vs any other comorbidity. Outcomes included mortality, hospital length of stay (LOS), discharge disposition, and in-hospital complications.
Using 1:1 propensity score matching, we matched 215 cases with CHD-related comorbid diagnoses to non-CHD controls. Compared to patients with other comorbidities, patients with CHD-related comorbidites were less likely to be discharged home to self-care (odds ratio: 0.44, 95% confidence interval [CI]: 0.25, 078
We present the first quantitative multicenter analysis correlating documentation of comorbid CHD-related diagnoses with higher risk of adverse outcomes after trauma surgery. These results support the need to routinely acknowledge and document CHD as comorbidity in trauma admissions that could lead to surgical intervention and for trauma centers to prepare for patients with a possible CHD comorbidity.
The abdominal seat belt sign (SBS) is associated with an increased risk of hollow viscus injury (HVI). Older age is associated with worse outcomes in trauma patients. Thus, older trauma patients ≥65 years of age (OTPs) may be at an increased risk of HVI with abdominal SBS. Therefore, we hypothesized an increased incidence of HVI and mortality for OTPs vs younger trauma patients (YTPs) with abdominal SBS.
This post hoc analysis of a multi-institutional, prospective, observational study (8/2020-10/2021) included patients
Of the 754 patients included in this study from nine level-1 trauma centers, there were 110 (14.6%) OTPs and 644 (85.4%) YTPs. Older trauma patients were older (mean 75.3 vs 35.8 years old,
Despite a similar rate of HVI, OTPs with an abdominal SBS had an increased rate of mortality and LOS. This suggests the need for heightened vigilance when caring for OTPs with abdominal SBS.
Level-I and level-II trauma centers are required to offer equivalent resources since “The Orange Book.” This study evaluates differences between level-I and level-II management of solid organ injury (SOI) with traumatic brain injury (TBI).
We conducted a retrospective review of the National Trauma Data Banks from 2013 to 2021 of adult (≥18 years), blunt trauma patients with both TBI and SOI treated at level-I or level-II trauma centers.
48,479 TBI and SOI patients were identified, 32,611 (67.3%) at level-I centers. Unadjusted incidence of laparotomy was higher at level I (14.5% vs 11.7%,
Nonoperative management was seen more at level-II centers with laparotomy at level I. Subgroup analysis showed no difference in mortality in trauma levels. Matched patients for level I and II showed no statistical difference in management. Patients were treated similarly at both levels with similar outcomes and mortality.
Inflammatory bowel diseases (IBDs) pose an increased risk of gastrointestinal cancer with especially worse prognosis. Cytoreductive surgery and heated intraperitoneal chemotherapy (CRS/HIPEC) improves outcomes in selected patients with colorectal peritoneal metastases. Little published data describes the outcomes of CRS/HIPEC in IBD patients.
We performed a retrospective review of a prospectively maintained CRS/HIPEC database. Outcomes in patients with and without IBD were compared for short-term outcomes such as hospital/intensive care unit stay, blood loss/transfusions, complications, and reoperations. We also examined oncological outcomes including recurrence, overall (OS), and disease-free survival (DFS).
We identified 232 patients that underwent CRS/HIPEC for colorectal or small bowel adenocarcinoma, of which 10 were with IBD. Patients with IBD had lower ASA (
Cytoreductive surgery and heated intraperitoneal chemotherapy in patients with IBD has similar complication profile and trended towards poorer oncological outcomes as CRS/HIPEC in non-IBD patients.
The impact of socioeconomic inequalities on cancer care and outcomes has been well recognized and the underlying causes are likely multifactorial. Income is regarded as a cornerstone of socioeconomic status and has been assumed to correlate with access to care. We therefore sought to investigate whether income and changes in income would affect the rate of patients undergoing surgical resection for early-stage pancreatic cancer.
Inflation-adjusted income data were obtained from the United States Census Bureau from 2010 to 2019. The cancer data were obtained from the SEER database. Counties present in both data sets were included in the analysis. Patients with stage I or II pancreatic cancer who underwent formal resection were deemed to have undergone appropriate surgical management. Patients were grouped into an early (2010-2014) and late (2015-2019) time period.
The final analysis included 23968 patients from 173 counties across 11 states. The resection rate was 45.1% for the entire study and rose from 42.8% to 47.4% from the early to late time periods (
Our surgical care of pancreatic cancer is improving with more patients undergoing resection. In addition, there are now fewer disparities between patients of lower-income and higher-income groups with respect to receiving surgical intervention. This implies that our access to care has improved over the past decade. This is an encouraging finding with regards to reducing health care disparities.
Despite the increasing number of female surgeons in general surgery programs, women are still inadequately represented in leadership positions. This study aims to investigate the magnitude of gender bias in university-based trauma surgery fellowship programs and leadership positions in the United States of America.
FRIEDA was used to identify trauma surgery programs. A thorough website review of each program obtained further information on faculty members, including their name, age, gender, and faculty rank. Trauma surgeons with an MD or DO qualification and a faculty rank of Professor, Associate Professor, or Assistant Professor were selected for inclusion in this study. SCOPUS was used to assess the H-index and the number of publications and citations of surgeons.
The total number of programs included was 136, consisting of 715 faculty members. Less than a quarter (n = 166; 23.2%) comprised females and less than one-fifth (n = 30; 19%) of female surgeons were Professors. The difference in the research productivity of male and female trauma surgeons was statistically significant (
Gender disparity exists in the field of trauma surgery, as noted in senior faculty ranks and leadership positions. Female-inclusive state policies, appropriate mentorship, and supportive institutions can help to bridge this gap.
The Affordable Care Act (ACA) aimed to expand Medicaid, enhance health care quality and efficiency, and address health disparities. These goals have potentially influenced medical care, notably revascularization rates in patients presenting with chronic limb-threatening ischemia (CLTI). This study examines the effect of the ACA on revascularization vs amputation rates in patients presenting with CTLI in Maryland.
This was a retrospective analysis of the Maryland State Inpatient Database comparing the rate of revascularization to rate of major amputation in patients presenting with CLTI over 2 periods: pre-ACA (2007-2009) and post-ACA (2018-2020). In this study, we included patients presenting with CLTI and underwent a major amputation or revascularization during that same admission. Using regression analysis, we estimated the odds of revascularization vs amputation pre- and post-ACA implementation, adjusting for pertinent variables.
During the study period, 12,131 CLTI patients were treated. Post-ACA, revascularization rate increased from 43.9% to 77.4% among patients presenting with CLTI. This was associated with a concomitant decrease in the proportion of CLTI patients undergoing major amputation from 56.1% to 22.6%. In the multivariate analysis, there was a 4-fold odds of revascularization among patients with CLTI compared to amputation (OR = 4.73, 95% CI 4.34-5.16) post-ACA. This pattern was seen across all insurance groups.
The post-ACA period in Maryland was associated with an increased revascularization rate for patients presenting with CLTI with overall benefits across all insurance types.
Abdominal pain continues to be a common chief complaint in the emergency setting. While this presentation can be non-specific, there are certain findings that warrant immediate surgical intervention. Portal venous gas on imaging in the setting of peritonitis and sepsis is one such finding. Thyrotoxicosis on the other hand is an uncommon diagnosis that is associated with non-specific symptoms resulting in delayed diagnosis, a clinical scenario that can lead to significant morbidity and mortality. Here, we present a rare case of a patient who presented with signs and symptoms of peritonitis and portal venous gas on CT scan that was taken emergently to the operating room. No intraabdominal pathology was identified. The patient was later diagnosed with thyrotoxicosis, the presumed cause of the acute abdomen presentation.
This study’s aim was to show the feasibility and safety of robotic liver resection (RLR) even without extensive experience in major laparoscopic liver resection (LLR).
A single center, retrospective analysis was performed for consecutive liver resections for solid liver tumors from 2014 to 2022.
The analysis included 226 liver resections, comprising 127 (56.2%) open surgeries, 28 (12.4%) LLR, and 71 (31.4%) RLR. The rate of RLR increased and that of LLR decreased over time. In a comparison between propensity score matching-selected open liver resection and RLR (41:41), RLR had significantly less blood loss (384 ± 413 vs 649 ± 646 mL,
The findings suggest that RLR is a feasible, safe, and acceptable platform for liver resection, and that the safe implementation and dissemination of RLR can be achieved without solid experience of LLR.
Acute substance intoxication is associated with traumatic injury and worse hospital outcomes. The objective of this study was to evaluate the association between simultaneous opioids and benzodiazepines (OB) use and hospital outcomes in elderly trauma patients.
We performed a retrospective analysis using the American College of Surgeons Trauma Quality Improvement Program (ACS-TQIP) 2017 database. We included trauma patients (age ≥ 65 years) examined by urine toxicology within 24 hours of presentation. The primary outcome was in-hospital mortality. Secondary outcomes included hospital and ICU lengths of stay (HLOS AND ICULOS), in-hospital complications (eg, ventilator-associated pneumonia), unplanned intubation, and duration of mechanical ventilation. Patients were stratified being both positive for opioids and benzodiazepines (OB+) or not (OB−) based on having positive or negative drug screen for both drugs, respectively. A 1:1 propensity score matching was performed controlling for demographics (eg, age and sex), comorbidities (eg, alcoholism), and injury characteristics.
Of 77,311 tested patients, 849 OB+ were matched to OB− patients. Compared to OB− group, OB+ patients were more likely to have unplanned intubation (26 [3.1%] vs 8 [0.9%],
The OB intake is associated with higher incidence of unplanned intubation and longer HLOS in elderly trauma patients. Early identification of elderly trauma patient with OB+ can help provide necessary pharmacologic and behavioral interventions to treat their substance use and potentially improve outcomes.
Trauma is a leading cause of global death, with 200 000 deaths and over 3 million non-fatal injuries/year in the United States. We aim to assess trauma care value for patients who underwent urgent laparotomies (LAP) and thoracotomies (THO) in our Health Network System.
Clinical variables (v = 84) from trauma patients (>18 yo) were retrieved retrospectively (Jan-2010 to July-2016) and prospectively (Aug-2016 to Sept-2021) from a Health System warehouse under IRB-approved protocols. Patients were divided according to their Injury Severity Score (ISS) into mild/moderate cases (ISS <15) and severe cases (ISS >15). Value was assessed using quality and cost domains. Quality surrogates included graded postoperative complications (PCs), length of stay (LOS), 30-day readmission (RA), patient satisfaction (PS), and textbook (TB) cases. Total charges (TCs) and reimbursement index (
41,927 trauma evaluations were performed, leading to 16 044 admissions, with 528 (3.2%) patients requiring urgent surgical procedures (LAP = 413 and THO = 115). Although the M:F ratio (7:3) was similar in LAP vs THO groups, age and BMI were significantly different (41.8 ± 19.1 vs 51.8 ± 19.9 years, 28.6 ± 9.9 vs 27.4 ± 7 Kg/m2, respectively,
The Trauma Program holds high value in our Health Network System. Protocols for decreasing LOS are being implemented.
This study aimed to investigate the characteristics of patients with colorectal mucinous adenocarcinoma (MAC) who benefit from postoperative chemotherapy (POCT) and to develop effective postoperative survival nomograms for predicting overall survival (OS) in colorectal MAC patients.
Data of colorectal MAC patients who underwent surgery from the Surveillance, Epidemiology, and End Results (SEER) database between 2010 and 2020 were collected. Patients were grouped based on POCT, and intergroup analysis was performed using 1:1 propensity score matching (PSM). Kaplan-Meier (K-M) curves were used to compare the prognosis between the 2 groups. Cox analysis was employed to identify factors associated with OS in patients with colorectal MAC who underwent POCT. The variance inflation factor (VIF) and bilateral stepwise regression were used to determine factors included in the model. Additionally, a nomogram was constructed to predict postoperative survival outcomes for patients. The discriminative ability of the nomograms was evaluated using the C-index and calibration curve analysis, the decision curve analysis (DCA) assessed the clinical utility of the nomogram, and the receiver operating characteristic (ROC) curve evaluated the nomograms’ performance.
This study encompassed 6829 patients with colorectal MAC, among whom 2258 received POCT, and 4571 did not. Whether pre or post PSM, patients in the POCT group consistently exhibited a superior median OS compared to those in the postoperative non-chemotherapy group (
This study revealed the characteristics of colorectal MAC patients who benefit from POCT and established effective prognostic nomograms, which can aid clinicians in designing personalized treatment plans for individual patients and promote precision medicine.
The Boston naming test (BNT), as a simple, fast, and easily administered neuropsychological test, was demonstrated to be useful in detecting language function. In this study, BNT was investigated whether it could be a screening tool for early postoperative cognitive dysfunction (POCD).
This prospective observational cohort study included 132 major noncardiac surgery patients and 81 nonsurgical controls. All participants underwent a mini-mental state examination (MMSE) and BNT 1 day before and 7 days after surgery. Early POCD was assessed by reliable change index and control group results.
Seven days after surgery, among 132 patients, POCD was detected in 30 (22.7%) patients (95% CI, 15.5%-30.0%) based on MMSE, and 45 (34.1%) patients (95% CI, 26.3%-41.9%) were found with postoperative language function decline based on BNT and MMSE. Agreement between the BNT spontaneous naming and MMSE total scoring was moderate (Kappa .523), and the sensitivity of BNT spontaneous naming for detecting early POCD was .767. Further analysis showed that areas under receiver operating characteristics curves (AUC) did not show statistically significant differences when BNT spontaneous naming (AUC .862) was compared with MMSE language functional subtests (AUC .889), or non-language functional subtests (AUC .933).
This study indicates the feasibility of implementing the BNT spontaneous naming test to screen early POCD in elderly patients after major noncardiac surgery.
Imposter phenomenon can occur in highly competitive fields causing internal feelings of fraud and self-doubt. Significant imposterism has been recently reported amongst general surgery residents.
We hypothesized that attending surgeons, navigating the transition into independent practice, would report a similar experience. We surveyed and collected Clance Imposter Phenomenon Scale (CIPS) scores from 24 Army general surgeons within 4 years of graduation.
Nearly all exhibited at least moderate imposterism, and over half reported significant or intense imposterism. Women reported statistically higher scores than men. Surgeons who engaged in off-duty employment or participated in mentorship were less likely to have significant or intense imposterism.
Transition to practice is a challenging and highly variable time for new surgeons. Identifying factors that attenuate these feelings could help with early career advancement.
This study aims to compare the efficacy of cephalosporin and non-cephalosporin antibiotics in preventing surgical site infections (SSIs) in patients undergoing colorectal surgery, providing a scientific basis for the selection of perioperative antibiotics through systematic review and meta-analysis.
Adhering to the PRISMA guidelines, this research employed an extensive literature search strategy across multiple databases to identify relevant studies, including randomized controlled trials (RCTs) and observational studies. Inclusion criteria were studies on adults undergoing colorectal surgery who received preoperative prophylaxis with either cephalosporin or non-cephalosporin antibiotics. Exclusion criteria included preoperative diagnosis of infectious diseases and preoperative use of antimicrobial agents. Meta-analysis was conducted using RevMan 5.3 software to assess the effectiveness of both antibiotic classes in preventing SSIs, including subgroup analyses.
Eight studies met the inclusion criteria, comprising 872 patients. Meta-analysis revealed that the incidence of SSI in the cephalosporin group was lower than in the non-cephalosporin group (14.8% vs 25.1%), with statistical significance (OR = 1.94, 95% CI: 1.38-2.74,
This study suggests that cephalosporin antibiotics may be superior to non-cephalosporins in preventing SSIs following colorectal surgery, especially in the short term. However, their long-term efficacy in SSI prevention may be similar. The selection of perioperative antibiotics should consider factors such as the antimicrobial spectrum, pharmacokinetic properties, and bacterial resistance.
Many complex abdominal hernias are referred to tertiary academic institutions for evaluation and treatment. The purpose of this study was to compare clinical outcomes from complex abdominal hernia repairs and abdominal wall reconstructions at a community hospital vs high volume academic centers participating in Abdominal Core Health Quality Collaborative (ACHQC).
Patients undergoing elective complex abdominal hernia repair were identified in our community setting and treated between 2016 and 2019. These results were then compared to Academic centers in the ACHQC database. Complex hernia definition was limited to those who have undergone any myofascial advancement procedure for homogeneity. Informed consent was obtained, and study was IRB approved. All data was de-identified.
A total of 180 patients underwent complex abdominal hernia repair at our community hospital. The ACHQC database identified 6299 patients meeting criteria at participating academic centers. Demographics were similar between the two groups including hernia grade, size and wound class. Academic centers tended to have patients with previous component separations (25.7% vs 10.6%) and immunosuppressed (7.2% vs 2.8%), while the community hospital patients included more patients with tobacco use (18.9% vs 12.1%) and hypertension (65% vs 54.9%). Operative times were significantly less at the community hospital, patients requiring >240 minutes of time for repair at academic centers (39.6% vs 5%). Postoperatively length of stay was significantly shorter at the community hospital group averaging 3.7 days vs academic centers of 6 days (
Community hospitals can provide comparable care and surgical expertise as major academic centers in regard to complex hernias in a large majority of cases. There is a need for dedicated care coordination and continuous review of supporting staff and outcomes is necessary to assure quality care. There is still a need to identify which patients would benefit from treatment at an academic center as opposed to a community hospital in order to maximize patient access and outcomes at both types of hospital setting. Further investigation needs to be performed regarding criteria for which patients should be transferred to academic centers for their complex hernia care. Identifying patients who would benefit from treatment at Academic Centers as opposed to Community hospitals should continue to be investigated.
Proximal gastrectomy (PG) is one of function‐preserving gastrectomy (FPG). In this study, we compared the long-term results of proximal gastric cancer (PGC) patients undergoing proximal gastrectomy and total gastrectomy (TG).
Patients diagnosed with PGC and receiving PG or TG between 2004 and 2020 were selected from the Surveillance, Epidemiology, and End Results (SEER) database. Propensity score matching (PSM) was applied to minimize confounding factors. Kaplan-Meier analysis and log-rank test were used to compare overall survival (OS) and cancer-specific survival (CSS) between the PG and TG groups. Univariate and multivariate Cox regression analyses were performed to identify independent risk factors affecting OS.
A total of 3916 patients were recruited according to the inclusion and exclusion criteria, with 2614 undergoing PG and 1302 undergoing TG. After 1:1 PSM matching, 912 pairs of data were included for analysis. Before PSM matching, PG group tended to have better OS and CSS outcomes. However, after PSM matching, both surgical approaches showed similar long-term results.
PG for PGC yields comparable long-term outcomes to TG and demonstrates safety in terms of oncologic outcomes.
Patients with low socioeconomic status (SES) are disadvantaged in terms of access to health care. A novel metric for SES is the Distressed Communities Index (DCI). This study evaluates the effect of DCI on hospital choice and distance traveled for surgery.
A Florida database was queried for patients with symptomatic cholelithiasis or chronic cholecystitis who underwent an outpatient cholecystectomy between 2016 and 2019. Patients’ DCI was compared with hospital ratings, comorbidities, Charlson Comorbidity Index, and distance traveled for surgery. Stepwise logistic regression was used to determine which factors most influenced distance traveled for surgery.
There were 54,649 cases—81 open, 52,488 laparoscopic, and 2,080 robotic. There was no difference between surgical approach and patient’s DCI group (p = 0.12). Rural patients traveled the farthest for surgery (avg 21.29 miles); urban patients traveled the least (avg 5.84 miles). Patients from distressed areas more often had surgery at one- or two-star hospitals than prosperous patients (61% vs 36.3%). Regression indicated distressed or at-risk areas predicted further travel for rural/small-town patients, while higher hospital ratings predicted further travel for suburban/urban patients.
Compared to prosperous areas, patients from distressed areas have surgery at lower-rated hospitals, travel further if they live in rural/small-town areas, but travel less if they live in suburban areas. We postulate that farther travel in rural areas may be explained by a lack of health care resources in poor, rural areas, while traveling less in suburban areas may be explained by personal lack of resources for patients with low SES.
The aim of this study was to investigate the prognostic value of systematic inflammatory response in patients with lymph node-negative colorectal cancer.
We retrospectively investigated 245 patients with lymph node-negative colorectal cancer who underwent curative resection and evaluated the prognostic impact of systematic inflammatory response, which was represented by neutrophil-to-lymphocyte ratio (NLR), prognostic nutritional index (PNI), and C-reactive protein-to-albumin ratio (CAR). Then, the prognostic significance of the systematic inflammatory response on survival was analyzed using the Kaplan-Meier method in patients selected by propensity score matching (PSM) analysis.
In the multivariate analysis, CAR ≥ .081 (
C-reactive protein-to-albumin ratio may be a significant indicator of poor long-term outcomes in patients with lymph node-negative colorectal cancer.
Ileus is a common complication of major abdominal surgery, including colorectal resection. The present study aimed to assess the predictors of ileus after laparoscopic right colectomy for colon cancer.
This study was a retrospective case-control analysis of a prospective IRB-approved database of patients who underwent laparoscopic right colectomy at the Department of Colorectal Surgery, Cleveland Clinic Florida. Patients who developed ileus after right colectomy were compared to patients without ileus to determine the risk factors of ileus.
The present study included 270 patients with a mean age of 68.7 years. Thirty-six patients (13.3%) experienced ileus after laparoscopic right colectomy. The median duration of ileus was 6 days. Factors associated with ileus were age (71.6 vs 68.2 years,
Increased age, emergency surgery, green GIA cartridge, and longer operative times were associated with ileus, yet the only independent predictor of ileus was extended right hemicolectomy.
Pancreatic adenocarcinoma, increasingly diagnosed in the United States, has a disheartening initial resection rate of 15%. Neoadjuvant therapy, particularly FOLFIRINOX and gemcitabine-based regimens, is gaining favor for its potential to improve resectability rates and achieving microscopically negative margins (R0) in borderline resectable cases, marked by intricate arterial or venous involvement. Despite surgery being the sole curative approach, actual benefit of neoadjuvant therapy remains debatable. This study scrutinizes current literature on oncological outcomes post-resection of borderline resectable pancreatic cancer. A MEDLINE/PubMed search was conducted to systematically compare oncological outcomes of patients treated with either neoadjuvant therapy with intent of curative resection or an “upfront resection” approach. A total of 1293 studies were initially screened and 30 were included (n = 1714) in this analysis. All studies included data on outcomes of patients with borderline resectable pancreatic adenocarcinoma being treated with neoadjuvant therapy (n = 1387) or a resection-first approach (n = 356). Patients treated with neoadjuvant therapy underwent resection 52% of the time, achieving negative margins of 43% (n = 601). Approximately 77% of patients who received an upfront resection underwent a successful resection, with 39% achieving negative margins. Neoadjuvant therapy remains marginally efficacious in treatment of borderline resectable pancreatic adenocarcinoma, as patients undergo an operation and successful resection less often when treated with neoadjuvant therapy. Rates of curative resection are comparable, despite neoadjuvant therapy being a primary recommendation in borderline resectable cases and employed more often than upfront resection. Upfront resection may offer improved resection rates by intention-to-treat, which can provide more patients with paths to curative resection.
Adhesions are a feared complication of abdominal surgery. There have been many new adhesion barriers developed and tested; however, there is no recent systematic review analyzing all the published literature. To address this, we aimed to analyze the different types of adhesion barriers, and determine their effects on postoperative outcomes in patients.
A total of 14,038 articles utilizing adhesion barriers in abdominal surgery were retrieved from the PubMed, EMBASE, and Scopus databases. Inclusion criteria were: patients undergoing abdominal surgery, patients receiving an adhesion barrier, and reported postoperative outcomes. Two reviewers independently screened titles/abstracts and full-text articles using Covidence. The ROBINS-I tool was used to assess the quality of the included studies. Study protocol: Prospero CRD42023458230.
A total of 20 studies, with no overall high risk of bias, with 171,792 patients were included. Most studies showed an equivocal benefit for adhesion barriers, with no singular adhesion barrier type that had definitive superior outcomes compared to the others. Bioresorbable barriers emerged as the most extensively researched adhesion barrier type, exhibiting promising results in colorectal surgery. Starch-based adhesion barriers also exhibited a reduction in overall postoperative bowel obstructions and may be beneficial for stoma sites and port closures. On the other hand, many studies raised concerns regarding complications, including risk of abscess formation, fistula development, peritonitis, and anastomotic leakage.
Adhesion barriers should be considered on a case-by-case basis, however, they should not be utilized prophylactically in all abdominal surgeries due to their risk of complications.
In evidence-based medicine, systematic review continues to carry the highest weight in terms of quality and reliability, synthesizing robust information from previously published cohort studies to provide a comprehensive overview of a topic. Meta-analysis provides further depth by allowing for comparative analysis between the studied intervention and the control group, providing the most up-to-date evidence on their characteristics and efficacy. We discuss the principles and methodology of meta-analysis, and its applicability to the field of surgical research. The clinical question is defined using PICO framework (Problem, Intervention, Comparison, Outcome). Then a systematic article search is performed across multiple medical databases using relevant search terms, which are then filtered out based on appropriate screening tools. Pertinent data from the selected articles are collected and undergo critical appraisal by at least two independent reviewers. Additional statistical tests may be performed to identify the presence of any significant bias. The data are then synthesized to perform comparative analysis between the intervention and comparison groups. In this article, we discuss specifically the usage of R software (R Foundation for Statistical Computing, Vienna, Austria) for data analysis and visualization. Meta-analysis results of the pooled data are presented using forest plots. Concerns for potential bias may be addressed through the creation of funnel plots. Meta-analysis is a powerful tool to provide highly reliable medical evidence. It may be readily performed by independent researchers with minimal need for funding or institutional approval. The ability to conduct such studies is an asset to budding medical scholars.
This study aimed to evaluate the effectiveness and safety of 2D laparoscopy vs 3D laparoscopy for the treatment of colorectal cancer.
A literature search was conducted through PubMed, Web of Science, and Embase from their inception to January 2024. Studies investigating different outcomes of colorectal surgery were included. Results are presented as odds ratios (ORs) or mean differences (MDs) with 95% confidence intervals (CIs). The protocol for this review has been registered on PROSPERO (CRD42024504902).
A total of 10 publications were retrieved in this article. The 3D group is associated with a significant improvement in intraoperative blood loss (MD = −8.04, 95% CI = −14.18 to −1.89,
This meta-analysis demonstrates that 3D laparoscopy could reduce the amount of blood loss, accelerate postoperative pass flatus, and shorten the operation time and postoperative hospital stay over 2D for radical rectal cancer surgery, without obvious advantage for radical colon cancer surgery. Moreover, 3D laparoscopy increases the number of dissected lymph nodes for radical colon cancer surgery but may not be observed in rectal cancer surgery.
The walking blood bank (WBB) is a system for emergency blood acquisition from nearby donors if a patient’s blood needs exceed the immediate supply. USCENTCOM medical units will perform a walking blood bank if immediate blood requirements exceed the local supply. A benchmark WBB performance time was needed to provide a training goal for military WBB exercises. An expeditionary WBB performance time benchmark was created from prospective measurements of USCENTCOM medical unit performance times over 9 months. The mean total time, and new performance benchmark, for a WBB in USCENTCOM was 41.4 min +/− 13.2 min. USCENTCOM time from donor arrival to a transfusable unit mean time was 34.4 +/− 12.1 min. Expeditionary medical units conducting a WBB should expect to meet or exceed the provided benchmark.


A 40-year-old woman admitted for hyponatremia and anasarca due to decompensated cirrhosis after a recent steroid taper developed extremely painful cutaneous breast lesions clinically mimicking cellulitis and inflammatory breast cancer and was biopsy-diagnosed instead with diffuse dermal angiomatosis (DDA) of the breasts, a rare and painful disease that can be a diagnostic chameleon. This case highlights the importance of early surgical consultation and tissue biopsy to correctly diagnose the etiology of severely painful mastitis and prevent prolonged symptomology and repeated administrations of ineffective treatments. Diffuse dermal angiomatosis should be considered when suspected breast cellulitis is refractory to treatment or there is concern for inflammatory breast cancer, especially in pendulous-breasted women with comorbidities that increase susceptibility to local tissue hypoxia.

At Cleveland clinic, an incorrect surgical count triggers Code Rust; a protocol that mandates an intraoperative patient X-ray, staff radiology read, and discussion with the surgeon before the incision is closed. Code Rust calls from November 2014 to December 2022 were retrospectively reviewed. Realtime workflow and operative details of Code Rust cases were analyzed.1277 Code Rusts were identified. Average time from ordering the X-ray to final radiology report was 50 minutes, totalling $2,362,450.00 spent on operating room time. Code Rust was called twice as frequently during urgent or emergent cases, compared to elective. There were more staff in Code Rust rooms compared to non-Code Rust rooms. A foreign body on X-ray was identified in 42/1277 (3.3%) cases. Code Rust is a resource intensive process that is more common in emergent cases that involve multiple staff. While retained foreign bodies are identified in a small percentage of cases, the current system should be revisited to reduce operating time and expense.
Intracholecystic papillary neoplasm (ICPN) of the gallbladder is a rare tumor described as a mucosal exophytic neoplastic lesion that projects into the gallbladder lumen. In regards to the size, lesions that did not make the arbitrary 1cm cutoff are described as “incipient” ICPN. Not much is known about these incipient ICPNs, as they are often excluded in ICPN studies, given the attempted adherence to the traditional 1cm cutoff. We present the youngest reported case of incipient, non-mucinous gastric-pylorus type ICPN who underwent cholecystectomy. Resection with negative margin for ICPN appears to be sufficient treatment and post resection imaging surveillance could be of value but further studies are required.
Traumatic abdominal wall hernias are a rare complication of high energy blunt trauma. There exist several studies evaluating and outlining potential management options but still no generalized consensus on management. This series was meant to evaluate the diagnosis and management of traumatic abdominal wall hernias. A prospectively maintained database was used to identify patients with TAWH from 2021 to 2022. The primary outcome was operative management. Secondary outcomes included: time to diagnosis and post-operative outcomes. Of the 19 patients in this case series, 100% (n = 19/19) were secondary to blunt trauma with a mean ISS of 21. Exploratory laparotomy was performed in 17 cases. 14 cases had concomitant traumatic injuries to visceral structures. Complications were found in nearly half of the patients with 3 experiencing wound dehiscence. Future studies should be aimed at standardizing management approach taking into account nature of the mechanism and concomitant injuries.
Recognition of patients at high risk (HR) for breast cancer allows earlier screening and opportunities for risk reduction. We compare patients referred to our breast clinic as HR vs referrals for other reason (ROR) and found to be HR. We evaluate under-recognized factors and treatment differences. A retrospective chart review of patients found to be HR but referred for any reason to our breast clinic from July 2012 to December 2022 was performed. Referral reason, demographics, hormonal history, family history, and other risk factors were evaluated and compared (HR vs ROR). While other risk models were used for screening, Gail and Tyrer-Cuzick version 7 (TCv7) were used for comparison. Breast imaging received, hormonal therapy, and genetics referral evaluations were compared. 195 patients were referred to our breast team, 113 (58%) were referred as HR while 82 (42%) were ROR. Average age was 47 years old. 175 (91%) were Caucasian. 74 (65.5%) were referred for genetic testing, and 32 (26%) tested positive for a genetic mutation (n = 10, 12% ROR). 67 (35%) were recommended chemoprevention (n = 32, 16.4% took chemoprevention). 6 (3.1%) underwent prophylactic mastectomies and 163 (85%) had supplemental breast imaging. Comparison of HR vs ROR did not show significant differences in hormonal factors or treatments received; however, TCv7 was higher in the group referred as HR (
Achalasia is a neurodegenerative disorder affecting esophageal sphincter function. Treatment options include non-surgical and surgical approaches, such as Heller myotomy (HM). Combining Dor fundoplication with HM is controversial but may prevent gastroesophageal reflux disease (GERD). This retrospective cohort study aimed to assess whether HM with Dor fundoplication reduces GERD rates and increases dysphagia rates. Eighty patients who underwent HM between January 2018 and August 2023 were included. Sixty-four patients had Dor fundoplication and were matched 4:1 to 16 patients without fundoplication. Records were reviewed for GERD and achalasia symptoms at various postoperative time points. No significant differences in GERD or dysphagia symptoms were found between the two groups at any time point. Similarly, there were no significant differences in chest pain or dysphagia treatment. In conclusion, this study suggests that the addition of Dor fundoplication to HM does not significantly impact postoperative GERD or achalasia-related symptoms.
The aim was to determine whether on-call case volumes differ amongst colorectal surgeons, and what cases are performed on-call in an academic colorectal surgery practice. The on-call schedule for the year 2021 of a colorectal surgery practice was analyzed. Details of the case origin and operative details were collected. Average cases performed per call per surgeon were compared. Ten surgeons were included, and average cases per call ranged from .5 to 1.4 with 1.0 the overall average (
Peritoneal adhesion is a common cause of small bowel obstruction (SBO). In this study, we included 40 adult patients who had SBO, or partial obstructive symptoms. In the abdominal instillation of crystalloid fluid (AICF) cohort, 16 patients underwent lysis of adhesions and abdominal crystalloid fluid instillation at the end of the procedure. In the control (CO) group, 24 patients received lysis of adhesions without fluid instillation. AICF was achieved by the abdominal instillation of 1864 ± 97.5 mL of crystalloid fluid. We analyzed the recurrence of peritoneal adhesions resulting in reoperation for SBO within the 64.3 ± 9.15 months of follow-up time for the CO and the 70.5 ± 13.16-month follow-up for the AICF group. The AICF group had a lower SBO recurrence rate of 12.5% compared to the CO group’s 41.6% rate (

Throughout history, animal hair and human hair have been used as suture materials in surgery and retain sporadic interest today. This systematic literature review examines 42 primary sources to uncover insights into the use of hair sutures. Several notable figures documented their experiences across specialties, highlighting horsehair’s longevity and patient comfort. Despite waning popularity owing to synthetic alternatives, recent interest in autologous hair filaments for facial wounds signals a resurgence. The time-tested hair sutures offer a cost-effective, eco-friendly option, particularly in resource-limited settings.

Before the 20th century, peripheral artery disease (PAD) manifested as extreme pain, chronic wounds, and, eventually, gangrene requiring amputation. Despite this, it was rarely diagnosed. However, at the turn of the century, Western medicine shifted focus from infectious to chronic illnesses, and with this change, physicians’ engagement with PAD transformed. Aiming to mitigate long-term injury, physicians now worked to identify and treat vessel disease to restore meaningful blood circulation. This article explores the development and deployment of a new device resulting from this refocus, the PAssive VAscular EXerciser (PAVAEX) Boot, and its role as a creative response to a previously intractable clinical problem. The PAVAEX Boot, designed in 1933 by vascular surgeons Louis G. Herrmann and Mont R. Reid, was one of the few interventions for PAD at the time. Based on the observation that continuous negative pressure results in vasoconstriction, while short bursts transiently increase blood flow, the PAVAEX Boot utilized intermittent negative pressure to enhance peripheral vascular perfusion. Well-marketed and praised throughout the 1930s, it vanished from public writing and academic literature just 20 years later. However, negative pressure wound therapy resurged in the late 20th century, and though its inventors failed to recognize the precedent of the PAVAEX Boot, many of these devices and therapies are rooted in identical theories. We examine why the PAVAEX Boot faded from use and argue that the device remains a crucial advancement in negative pressure therapy.

Historically, surgery has been considered an inherently “masculine” profession. This persistent stereotype has led to gender inequality in currently practicing surgeons, despite gender parity of newly admitted medical students in North America. Since women began practising medicine in the 19th century, these norms began to be challenged in tandem with the suffragette movement. In the United States, United Kingdom and Canada, pioneering female physicians and surgeons worked together to establish spaces where women would be welcomed and mentored the next generation of female surgeons. In this essay, I highlight prominent women physicians and surgeons that have contributed to the presence of women in the operating room through mentorship.
Musicians with physical disabilities who achieved stardom are part of the lore of popular music. Guitarist Django Reinhardt contrived alternate fingering patterns necessitated by burn contractures of his left hand. Les Paul, a legend in the development of the solid body electric guitar and multitrack recording, mangled his right arm in a car wreck so severely that his elbow was set permanently at 90° so he could continue to play guitar. Michel Petrucciani suffered from osteogenesis imperfecta, a condition that stunted his growth to the point where he used a special attachment to reach the sustaining pedals of his piano. Their stories show the force of human genius in music.