Editorial
Select search scope: search across all journals or within the current journal
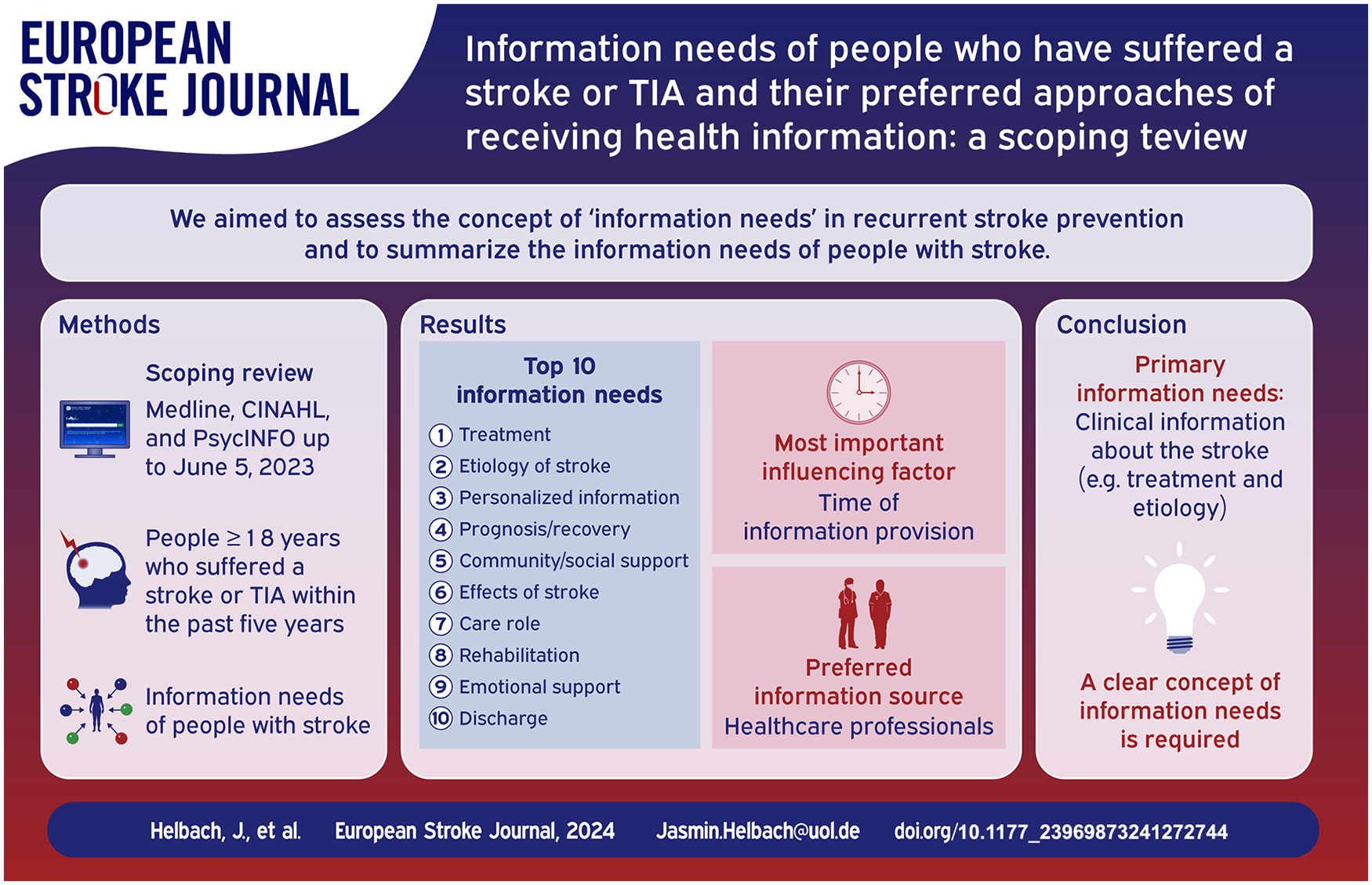
We aimed to synthesize the information needs of people with stroke (PwS) in recurrent stroke prevention.
In this scoping review we searched Medline (via PubMed), CINAHL, and PsycINFO from inception to June 5, 2023, to identify all studies describing the information needs of people 18 years and older who have suffered a stroke or transient ischemic attack within the past 5 years. We included qualitative and quantitative studies from developed countries published in German or English. Data analysis was performed following Arksey and O’Malley’s methodological framework for scoping reviews.
We screened 5822 records for eligibility and included 36 articles published between 1993 and 2023. None of the included studies used a comprehensive framework or defined information needs. Based on statements from PwS and their caregivers, PwS needed information on treatment, etiology, effects of stroke, prognosis, rehabilitation, discharge, life changes, care role, support options, information sources, and hospital procedures. The most frequently expressed needs were information on the treatment (77.8%) and stroke etiology (63.9%). The primary information source was healthcare professionals (85.7%), followed by written information (71.4%), family and friends (42.6%), and the internet (35.7%), with information provided directly by healthcare professionals being preferred. The timing of information transfer is often described as too early.
PwS are primarily interested in clinical information about stroke, for example, treatment and etiology, and less often in information about daily life, for example, rehabilitation, the role of care, or lifestyle changes. PwS prefer to receive information directly from healthcare professionals. Developing a shared understanding of PwS’s information needs is crucial to implement suitable strategies and programs for dealing with these needs in clinical practice.
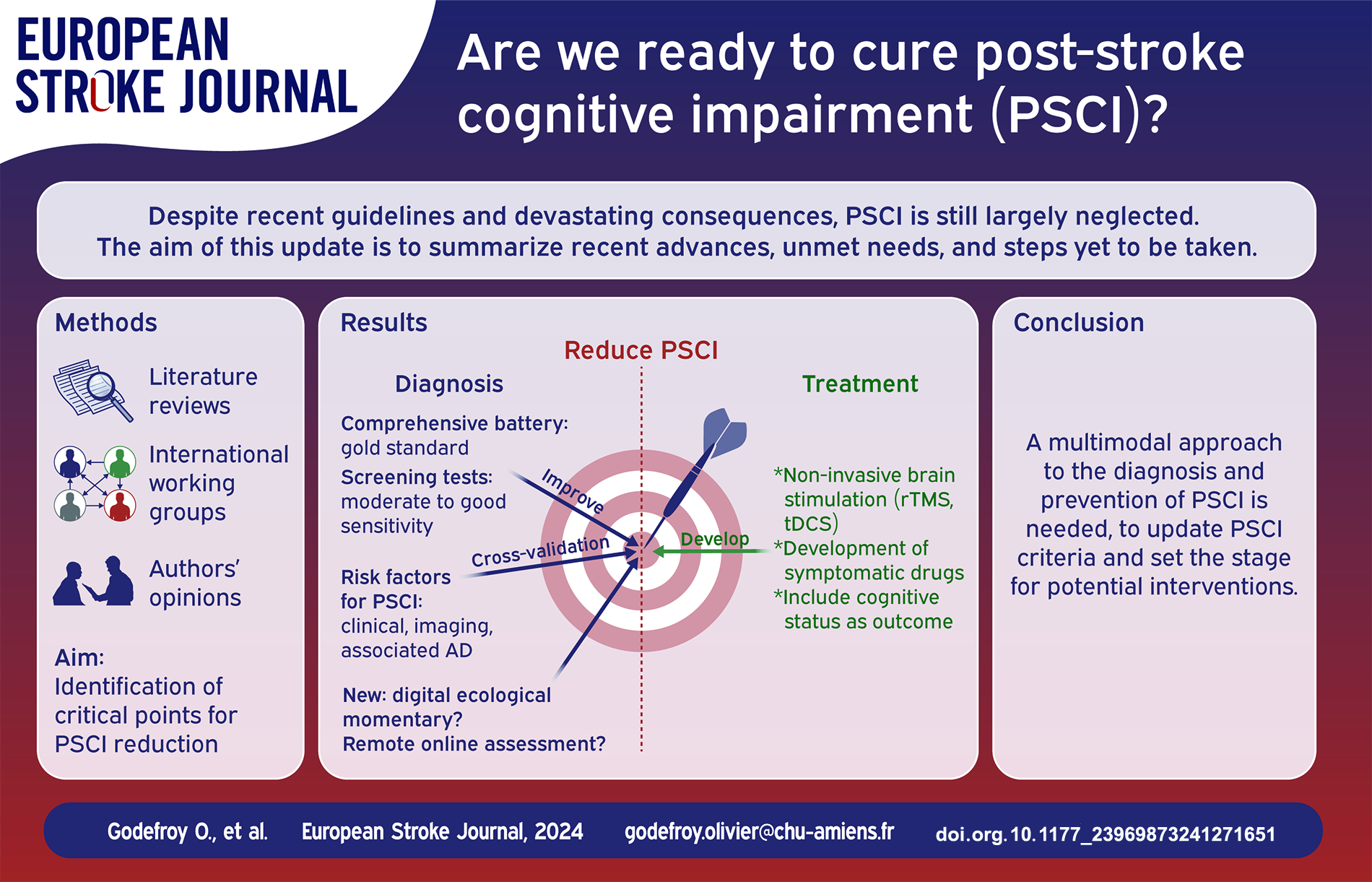
Post-stroke (PS) cognitive impairment (CI) is frequent and its devastating functional and vital consequences are well known. Despite recent guidelines, they are still largely neglected. A large number of recent studies have re-examined the epidemiology, diagnosis, imaging determinants and management of PSCI. The aim of this update is to determine whether these new data answer the questions that are essential to reducing PSCI, the unmet needs, and steps still to be taken.
Literature review of stroke unit-era studies examining key steps in the management of PSCI: epidemiology and risk factors, diagnosis (cognitive profile and assessments), imaging determinants (quantitative measures, voxelwise localization, the disconnectome and associated Alzheimer’s disease [AD]) and treatment (secondary prevention, symptomatic drugs, rehabilitation and noninvasive brain stimulation) of PSCI.
(1) the prevalence of PSCI of approximately 50% is probably underestimated; (2) the sensitivity of screening tests should be improved to detect mild PSCI; (3) comprehensive assessment is now well-defined and should include apathy; (4) easily available factors can identify patients at high risk of PSCI; (5) key imaging determinants are the location and volume of the lesion and the resulting disconnection, associated AD and brain atrophy; WMH, ePVS, microhemorrhages, hemosiderosis, and cortical microinfarcts may contribute to cognitive impairment but are more likely to be markers of brain vulnerability or associated AD that reduce PS recovery; (6) remote and online assessment is a promising approach for selected patients; (7) secondary stroke prevention has not been proven to prevent PSCI; (8) symptomatic drugs are ineffective in treating PSCI and apathy; (9) in addition to cognitive rehabilitation, the benefits of training platforms and computerized training are yet to be documented; (10) the results and the magnitude of improvement of noninvasive brain stimulation, while very promising, need to be substantiated by large, high-quality, sham-controlled RCTs.
These major advances pave the way for the reduction of PSCI. They include (1) the development of more sensitive screening tests applicable to all patients and (2) online remote assessment; crossvalidation of (3) clinical and (4) imaging factors to (5) identify patients at risk, as well as (6) factors that prompt a search for associated AD; (7) the inclusion of cognitive outcome as a secondary endpoint in acute and secondary stroke prevention trials; and (8) the validation of the benefit of noninvasive brain stimulation through high-quality, randomized, sham-controlled trials. Many of these objectives can be rapidly and easily attained.
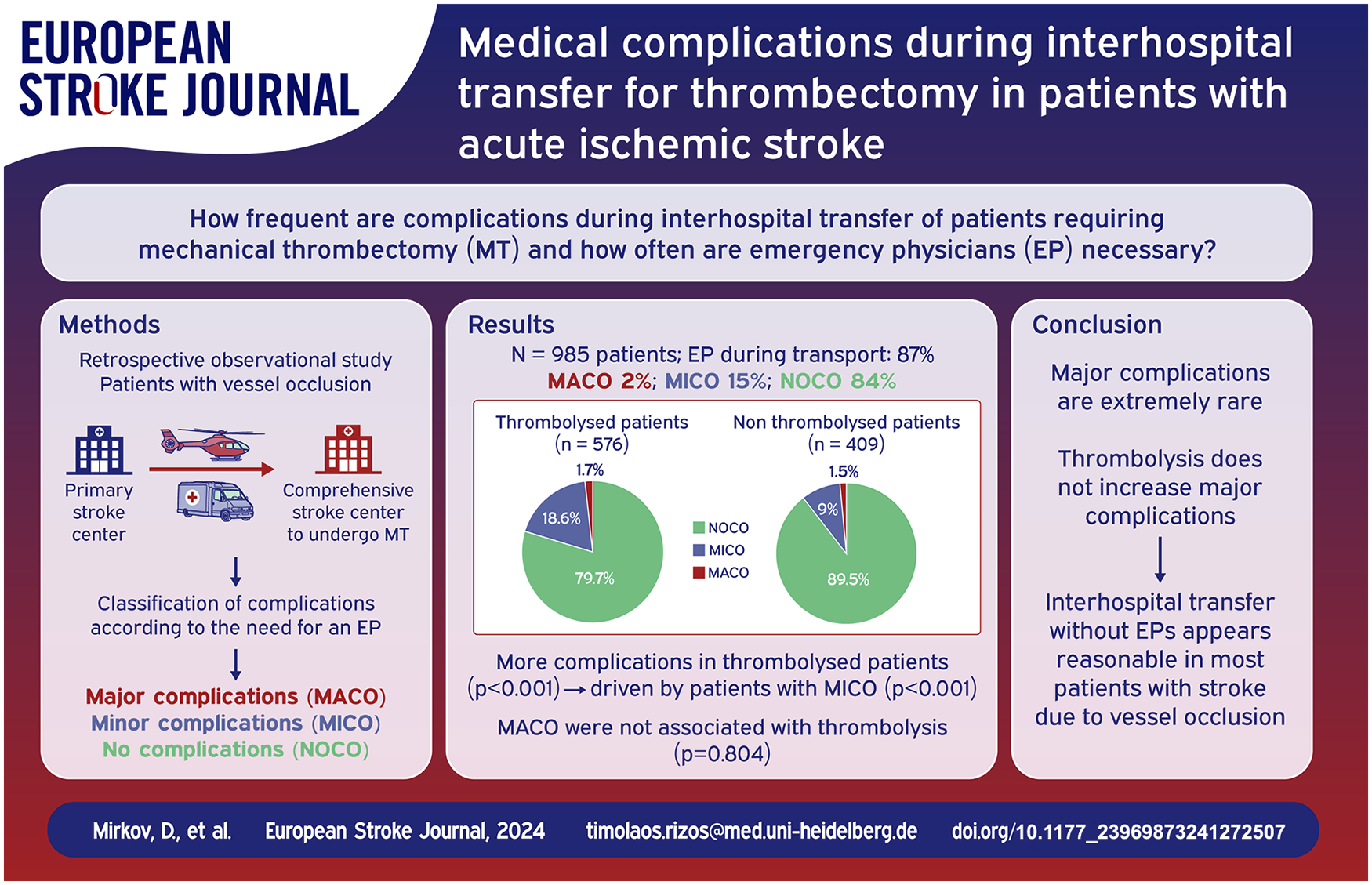
Patients with acute ischemic stroke (AIS) and large-vessel occlusion are frequently transferred by emergency physicians (EPs) from primary to comprehensive stroke centers (CSC) for thrombectomy, particular when thrombolysed. Data on complications during such transfers are highly limited.
Consecutive AIS patients transferred between 01/2015 and 10/2021 to our CSC were included. Associations of major (MACO) and minor (MICO) complications with clinical and imaging data were assessed.
In total, 985 patients were included in the analysis (58.5% thrombolysed). MACO developed in 1.6%, MICO in 14.6%. Compared to patients without complications (NOCO), patients with MACO did not differ in terms of demographics, cerebrovascular risk factors, or site of vessel occlusion. They had more severe strokes (
In this large cohort, no patient-specific factor increasing the risk of complications during interhospital transfer was identified. Specifically, our results do not indicate that thrombolysis increases MACO. Hence, interhospital transfer without EPs appears reasonable in most patients.
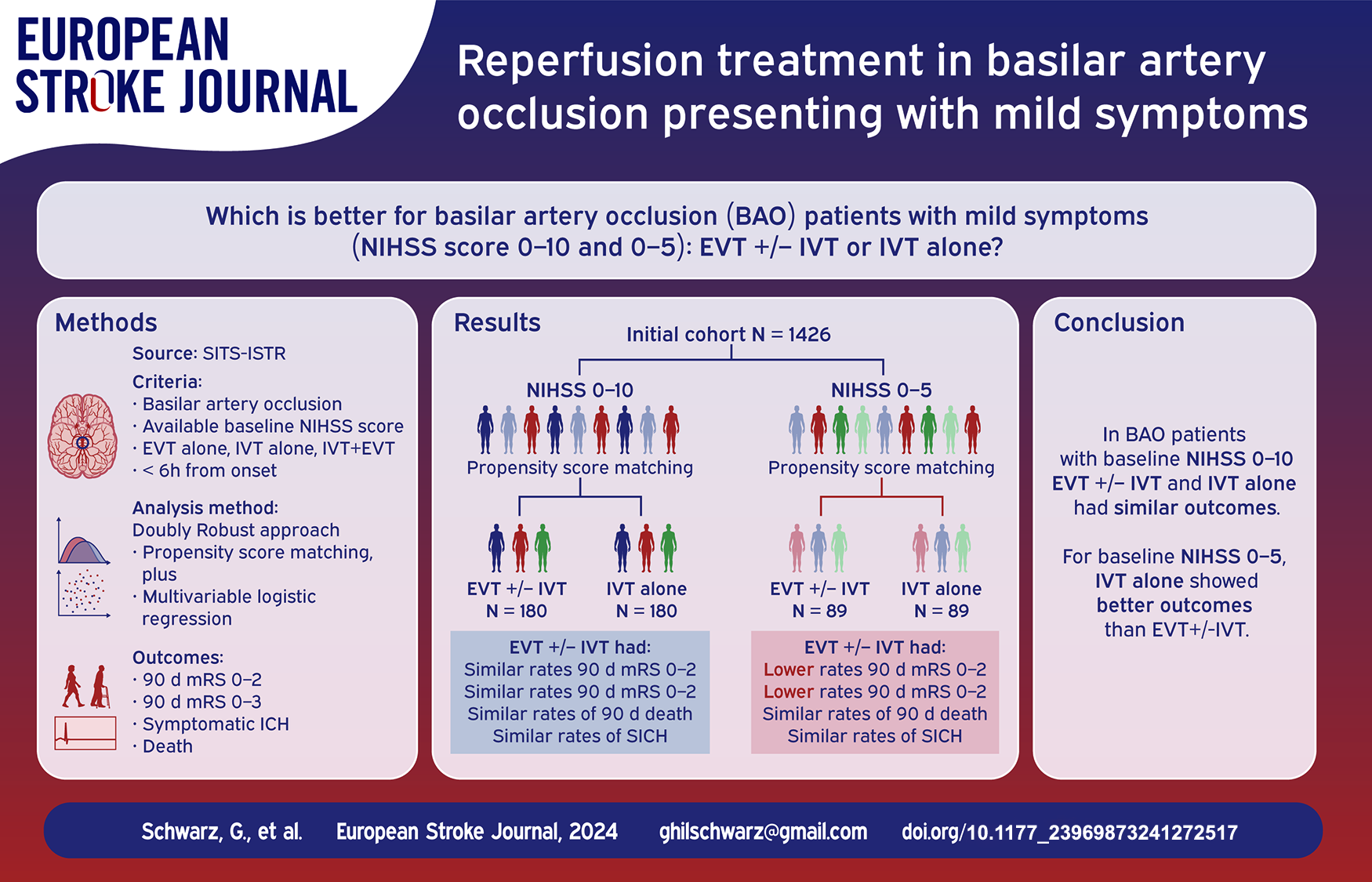
Endovascular treatment (EVT) improves outcomes for basilar artery occlusion (BAO) with moderate-to-severe symptoms. However, the best treatment for mild symptoms (NIHSS score 0–10 and 0–5) remains unclear. This study compared EVT ± IVT to IVT alone in BAO patients with mild symptoms.
From the SITS-International Stroke Treatment Register, we included BAO patients with available baseline NIHSS score, treated by EVT, IVT, or both within 6 h of symptom onset from 2013 to 2021. Using the Doubly Robust approach (propensity score matching plus multivariable logistic regression), we analyzed efficacy (3-month mRS) and safety (SICH and 3-month death) outcomes for EVT ± IVT versus IVT alone in BAO patients with NIHSS scores 0–10 and 0–5.
1426 patients were included. For NIHSS scores 0–10 (180 matched, 1:1 ratio), outcomes were similar between EVT ± IVT and IVT alone groups. For NIHSS scores 0–5 (89 matched, 1:1 ratio), EVT ± IVT was associated with worse outcomes compared to IVT alone (mRS 0–2, aOR 0.20 [95% CI 0.06–0.61];
In early-treated BAO patients with mild symptoms, defined as NIHSS 0–10, there were no significant differences in outcomes between EVT ± IVT and IVT alone. However, for very mild symptoms, defined as NIHSS 0–5, IVT alone was associated with better outcomes compared to EVT ± IVT.
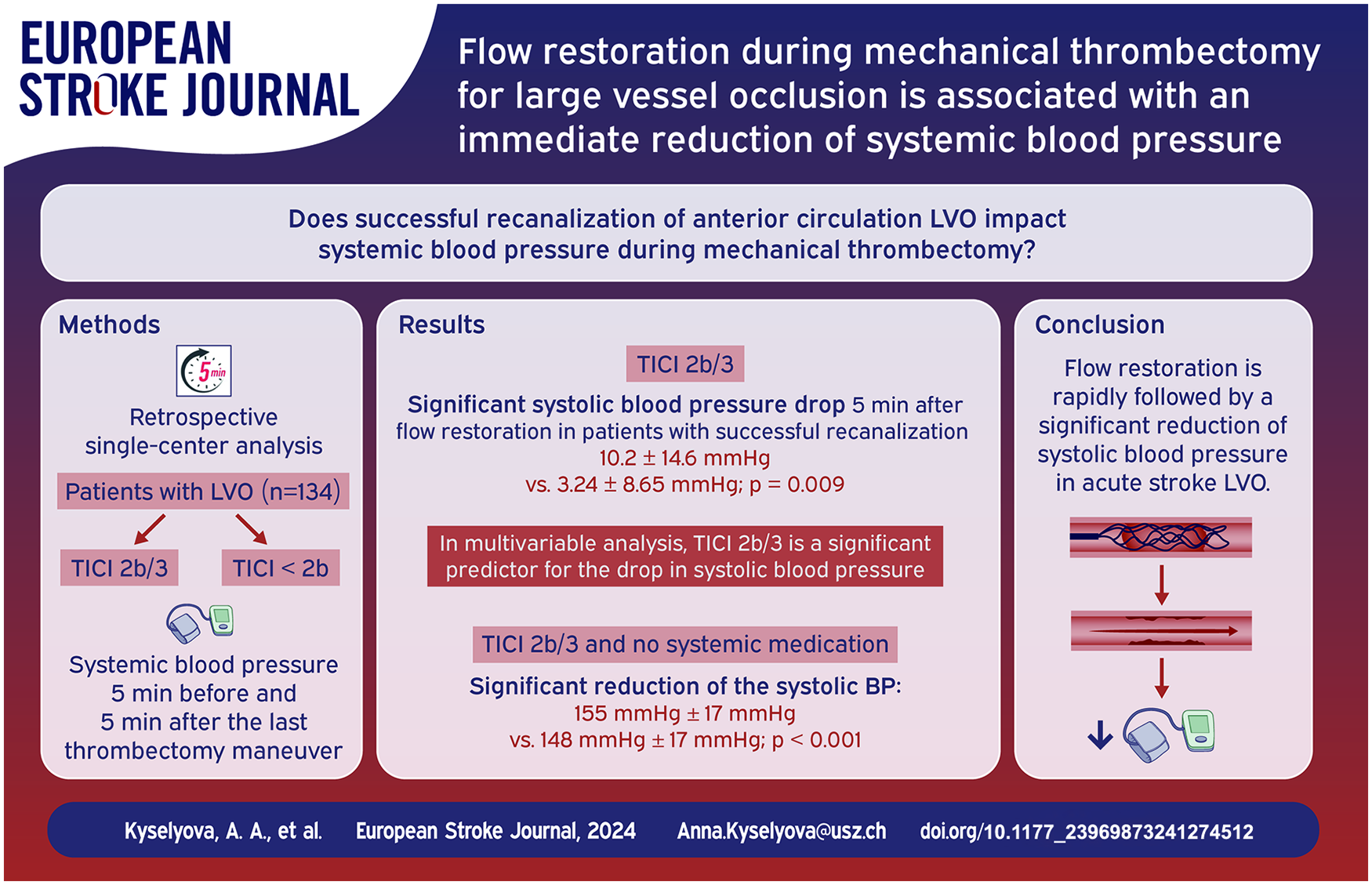
Managing blood pressure in patients with large vessel occlusion affects infarct size and clinical outcomes. We examined how restoring blood flow impacts systemic blood pressure during mechanical thrombectomy.
Patients with large vessel occlusion in the anterior circulation undergoing mechanical thrombectomy between June 2016 and January 2018 were screened. We included those treated under local anesthesia or conscious sedation and analyzed standardized anesthesia protocols to assess systolic and diastolic blood pressure levels throughout the procedure. The primary outcome was the change of blood pressure, compared 5 min before versus 5 min after the last recanalization attempt. Successful reperfusion was defined as Thrombolysis in Cerebral Infarction score ⩾ 2b.
Of 134 patients, 117 (87%) achieved successful angiographic reperfusion, showing a notable systolic blood pressure drop 5 min after flow restoration (10.2 ± 14.6 vs 3.24 ± 8.65 mm Hg,
Flow restoration was associated with an immediate reduction of systolic blood pressure values in patients undergoing mechanical recanalization under local anesthesia or conscious sedation. This suggests a complex interplay between endovascular stroke therapy and cardiovascular hemodynamics.
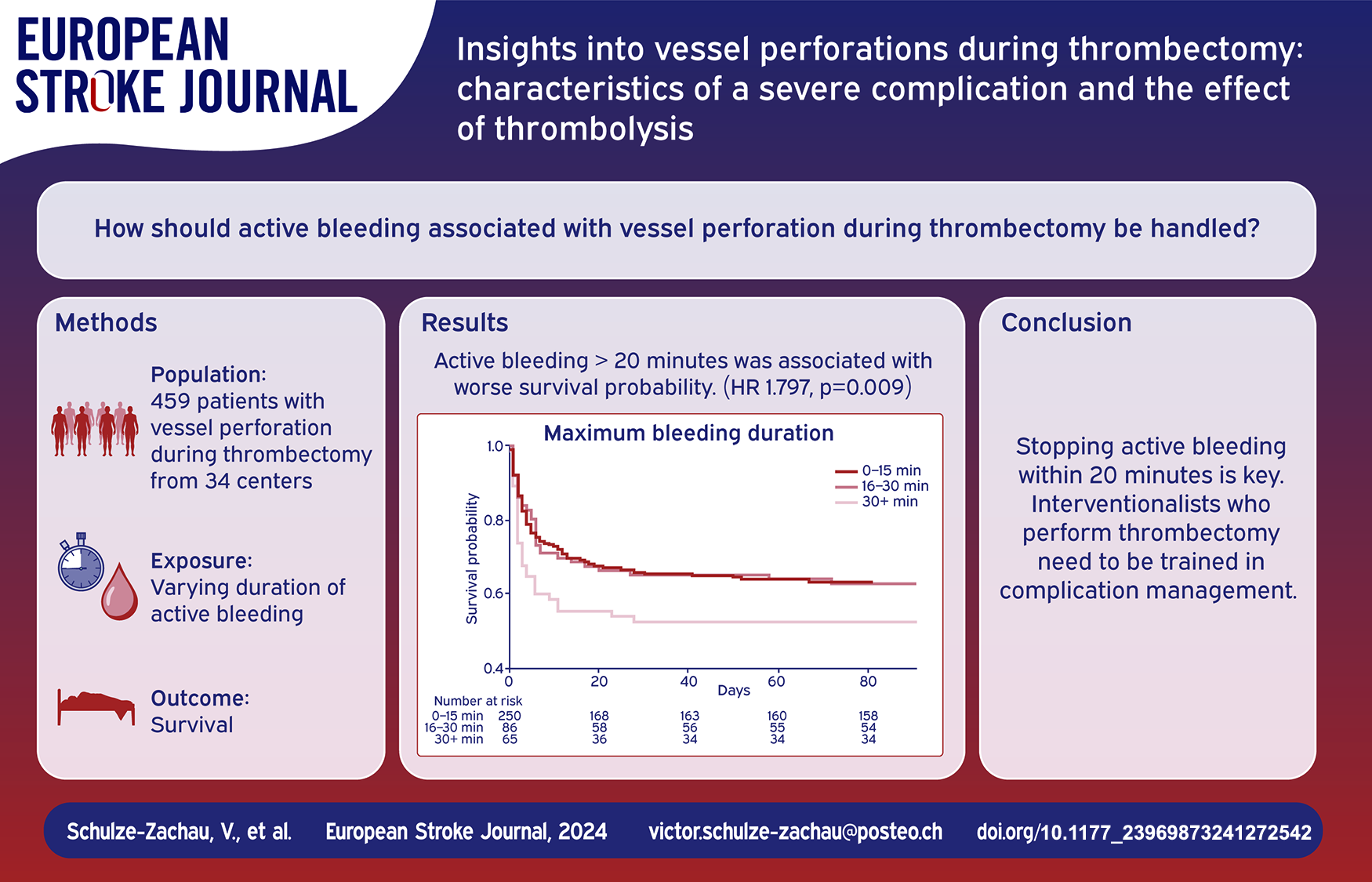
Thrombectomy complications remain poorly explored. This study aims to characterize periprocedural intracranial vessel perforation including the effect of thrombolysis on patient outcomes.
In this multicenter retrospective cohort study, consecutive patients with vessel perforation during thrombectomy between January 2015 and April 2023 were included. Vessel perforation was defined as active extravasation on digital subtraction angiography. The primary outcome was modified Rankin Scale (mRS) at 90 days. Factors associated with the primary outcome were assessed using proportional odds models.
459 patients with vessel perforation were included (mean age 72.5 ± 13.6 years, 59% female, 41% received thrombolysis). Mortality at 90 days was 51.9% and 16.3% of patients reached mRS 0–2 at 90 days. Thrombolysis was not associated with worse outcome at 90 days. Perforation of a large vessel (LV) as opposed to medium/distal vessel perforation was independently associated with worse outcome at 90 days (aOR 1.709,
Vessel perforation during thrombectomy is a severe and frequently fatal complication. This study does not suggest that thrombolysis significantly attributes to worse prognosis. Prompt cessation of active bleeding within 20 min is critical, emphasizing the need for interventionalists to be trained in complication management.
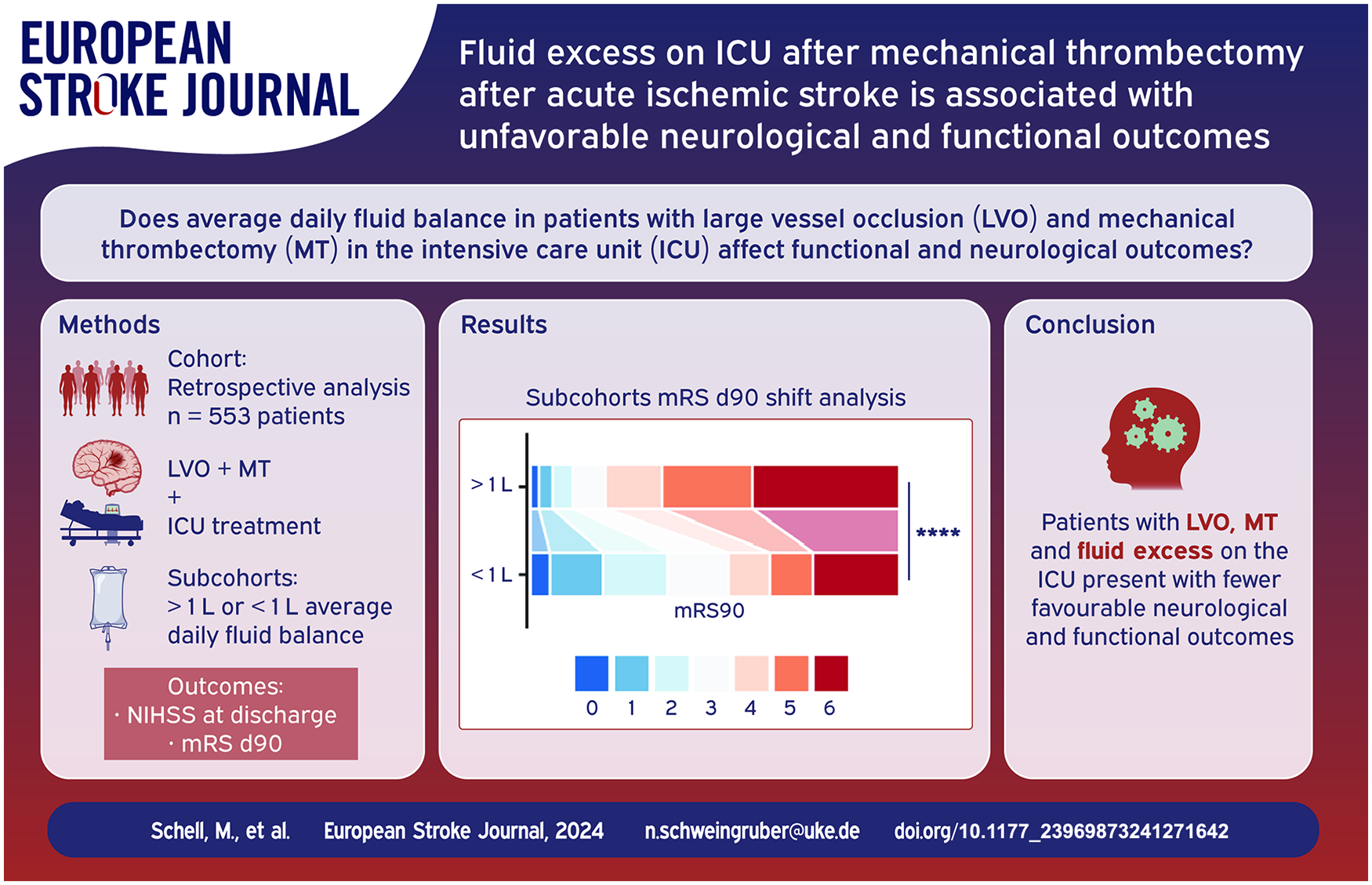
Endovascular thrombectomy stands as a pivotal component in the standard care for patients experiencing acute ischemic stroke with large vessel occlusion. Subsequent care for patients often extends to a neurological intensive care unit. While fluid management is integral to intensive care, the association between early fluid balance and neurological and functional outcomes post-thrombectomy has not yet been thoroughly investigated.
In a retrospective analysis of an observational, single-center study spanning from 2015 to 2021 at the University Medical Center Hamburg-Eppendorf, Germany, we enrolled stroke patients who underwent thrombectomy and received subsequent treatment in the ICU. Unfavorable functional and neurological outcome was defined as a mRS > 2 on day 90 after admission (mRS d90) or NIHSS > 5 at discharge, respectively. A multivariate regression model, adjusting for confounders, utilized the average fluid balance in the first 5 days to predict outcomes. Patients were dichotomized by their average fluid balance (>1 L vs <1 L) within the first 5 days, and a multivariate mRS d90 shift analysis was conducted after adjusting for covariates.
Between 2015 and 2021, 1252 patients underwent thrombectomy, and 553 patients met the inclusion criteria (299 women [54%]). Unfavorable functional outcome was significantly associated with a higher daily average fluid balance in the first 5 days in the ICU (mRS d90 ⩽ 2: 0.3 ± 0.5 L, mRS d90 > 2: 0.7 ± 0.7 L,
Fluid retention in post-thrombectomy stroke patients in the ICU is associated with poorer functional and neurological outcomes. Consequently, fluid retention emerges as an additional potential predictor for post-intervention stroke outcomes. Our findings provide an initial indication that preventing excessive fluid retention in stroke patients after endovascular thrombectomy could be beneficial for both functional and neurological recovery. Therefore, fluid retention might be an element to consider in optimizing fluid management for stroke patients.
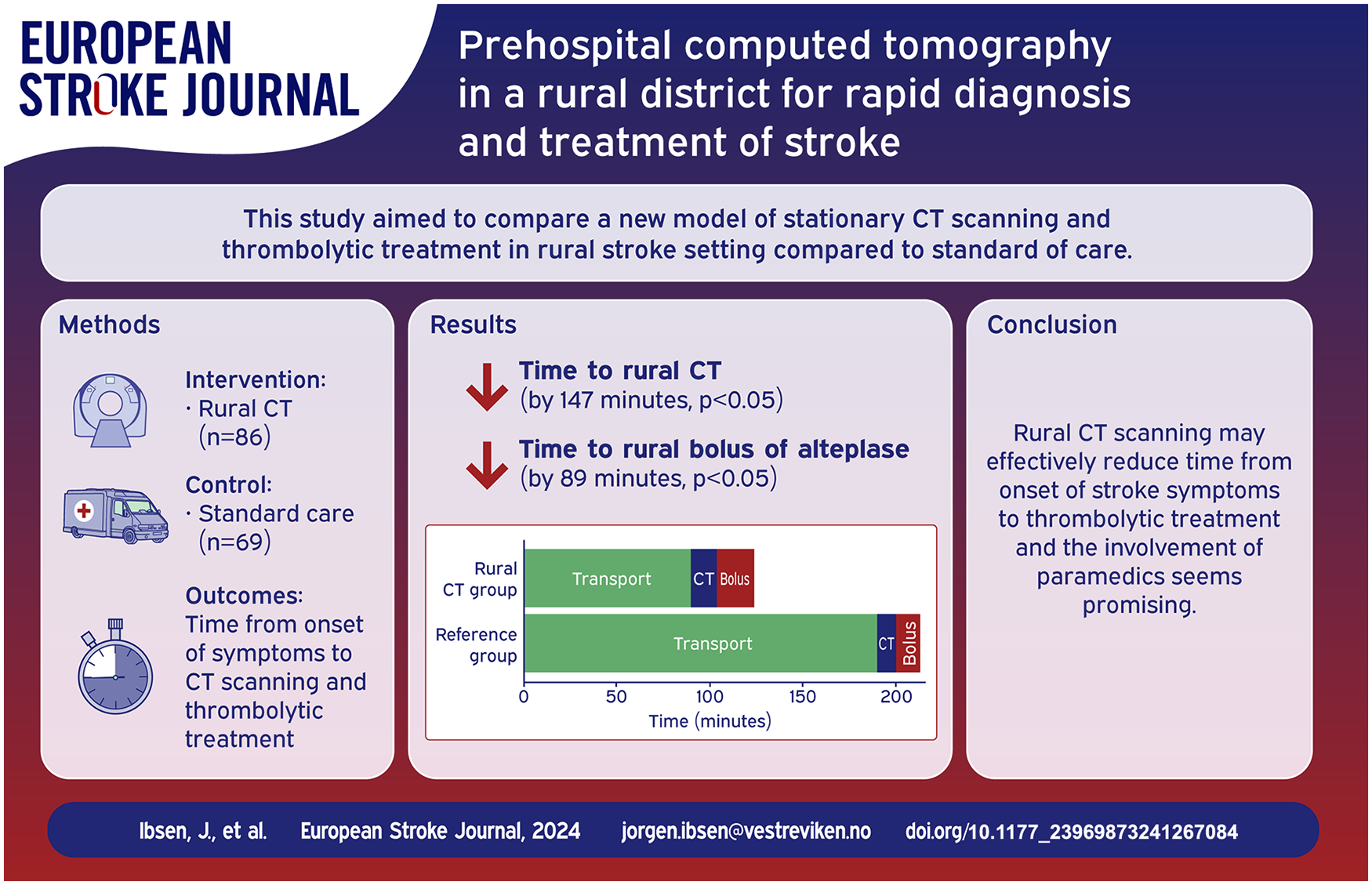
Early diagnosis and triage of patients with ischemic stroke is essential for rapid reperfusion therapy. The prehospital delay may be substantial and patients from rural districts often arrive at their local hospital too late for disability-preventing thrombolytic therapy due to prolonged transport times.
Hallingdal District Medical Centre (HDMC) is located in a rural area of Norway and is equipped with a computed tomography (CT) scanner. We established emergency pathways of CT imaging and thrombolytic treatment of patients with acute ischemic stroke at HDMC. During office hours these pathways were managed by a radiographer and a general physician supported by videoconference from the Primary Stroke Centre. Outside office hours we remotely controlled the CT exam and supported telestroke guided paramedics handling and examining the patients. With a primary aim of demonstrating the feasibility of this de novo concept we enrolled patients in the period 2017–2021 into a comparative cohort observational study. We compared patients treated at HDMC (the Rural CT group) to patients from two other rural regions in Norway with similar distances to their local hospital but without access to a rural CT scanner (the Reference group).
A total of 86 patients were included in the Rural CT group (mean age 74, 52% male, 43% stroke mimics), and 69 patients were included in the Reference group (mean age 70, 42% male, 28% stroke mimics). Median time from onset of symptoms to completed CT examination was 93 min in the Rural CT group as compared to 240 min in the Reference group (
Combining prehospital rural CT examination with telestroke guided diagnosis and thrombolytic treatment by paramedics may facilitate earlier initiation of thrombolysis for patients with ischemic stroke.
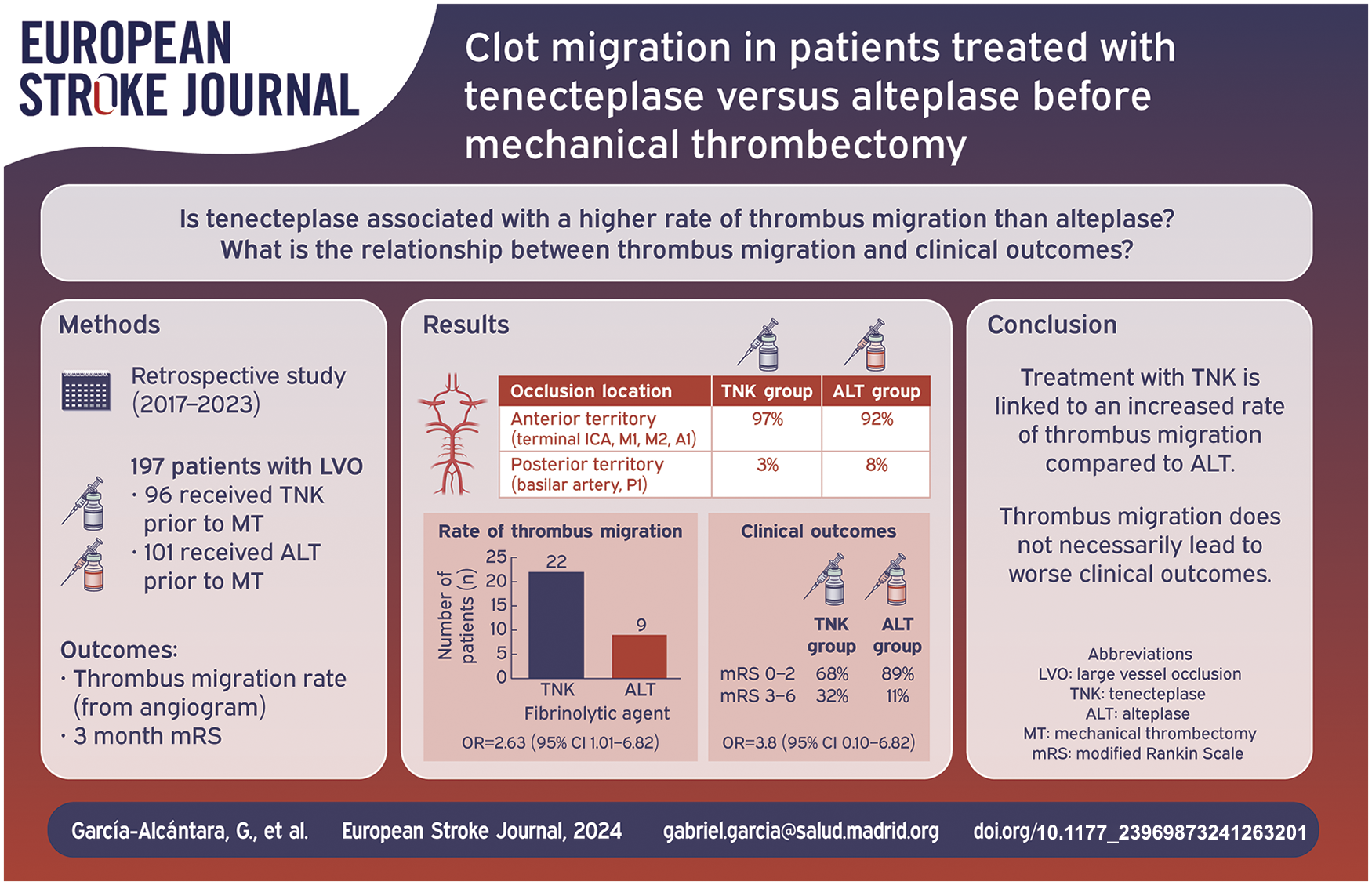
This study aimed to describe and analyze the rate of clot migration of vessel thrombosis to distal segments in patients with acute ischemic stroke (AIS) who received intravenous thrombolysis (IVT) with tenecteplase (TNK) and alteplase (ALT) before mechanical thrombectomy (MT). In addition, we aimed to determine the relationship between thrombus migration and functional prognosis.
This study followed the STROBE reporting guidelines. We performed a retrospective analysis of a series of patients from November 2017 to April 2023 with an AIS with thrombosis on CT imaging, treated with IVT (TNK or ALT, split into two distinct groups) prior to mechanical thrombectomy.
Two hundred and fifty-six patients with large vessel occlusion (LVO) were included. Ninety-six had received TNK. One hundred and sixty had received ALT. Of the 96 TNK patients, 25 experienced either complete recanalization (
The use of TNK over ALT as a fibrinolytic agent is associated with a higher thrombus migration rate. The migration of thrombi to distal segments, which are theoretically less accessible for mechanical thrombectomy, did not result in worse clinical outcomes.
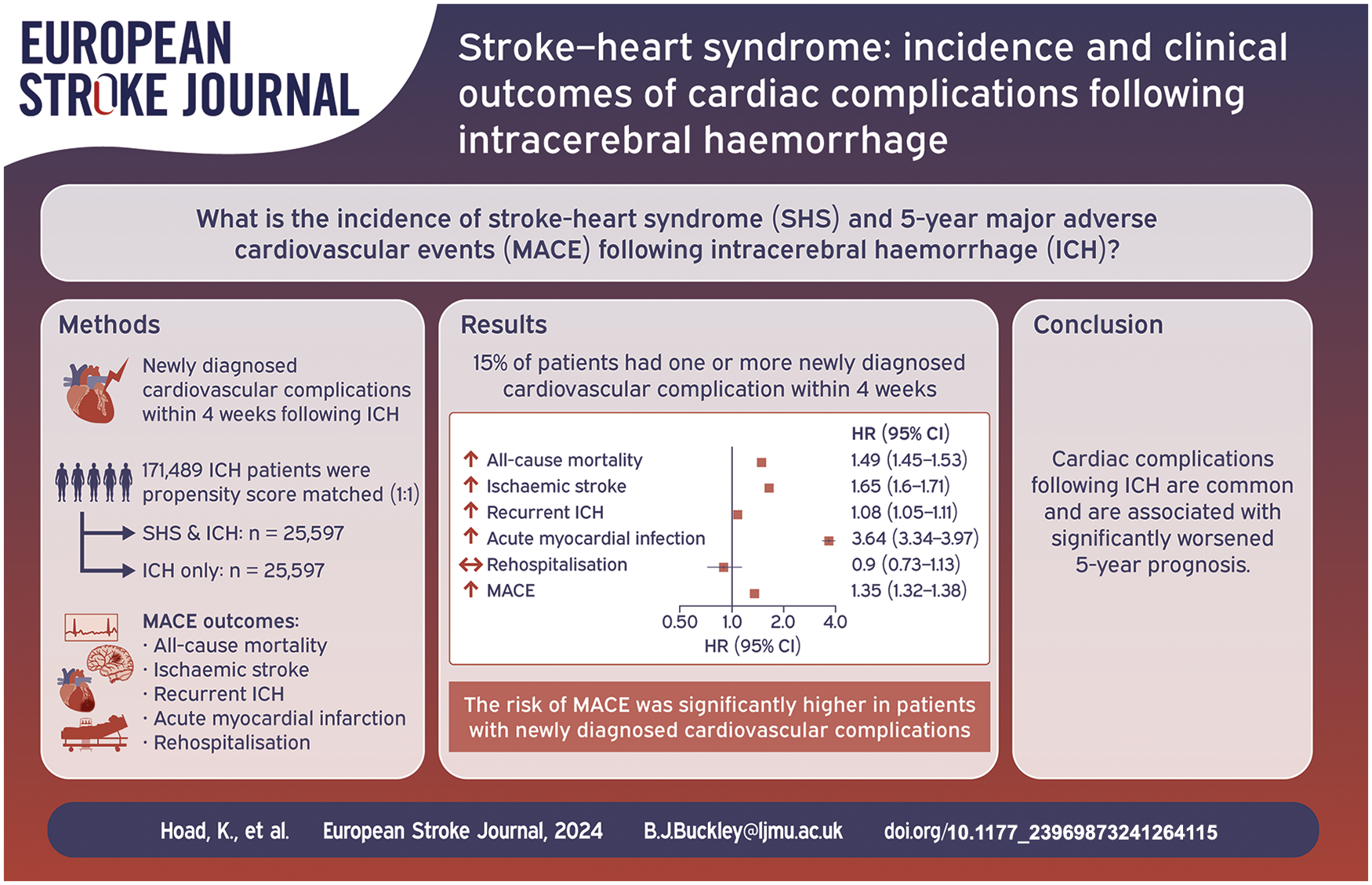
Newly diagnosed cardiovascular complications following an ischaemic stroke, termed stroke-heart syndrome, are common and associated with worse outcomes. Little is known regarding stroke-heart syndrome in relation to intracerebral haemorrhage (ICH). This study aimed to investigate the incidence and 5-year major adverse cardiovascular events (MACE; acute myocardial infarction, ischaemic stroke, all-cause mortality and recurrent ICH) of newly diagnosed cardiovascular complications following incident ICH, using a global federated database.
A retrospective cohort study was conducted using anonymised electronic medical records. Patients aged ⩾ 18 years with non-traumatic ICH and 5-year follow-up were included. Patients with newly diagnosed cardiovascular complications
Before propensity score matching, 171,489 patients with non-traumatic ICH, 15% (
Newly diagnosed cardiovascular complications following ICH (i.e. stroke-heart syndrome) were common and associated with a significantly worsened 5-year prognosis.
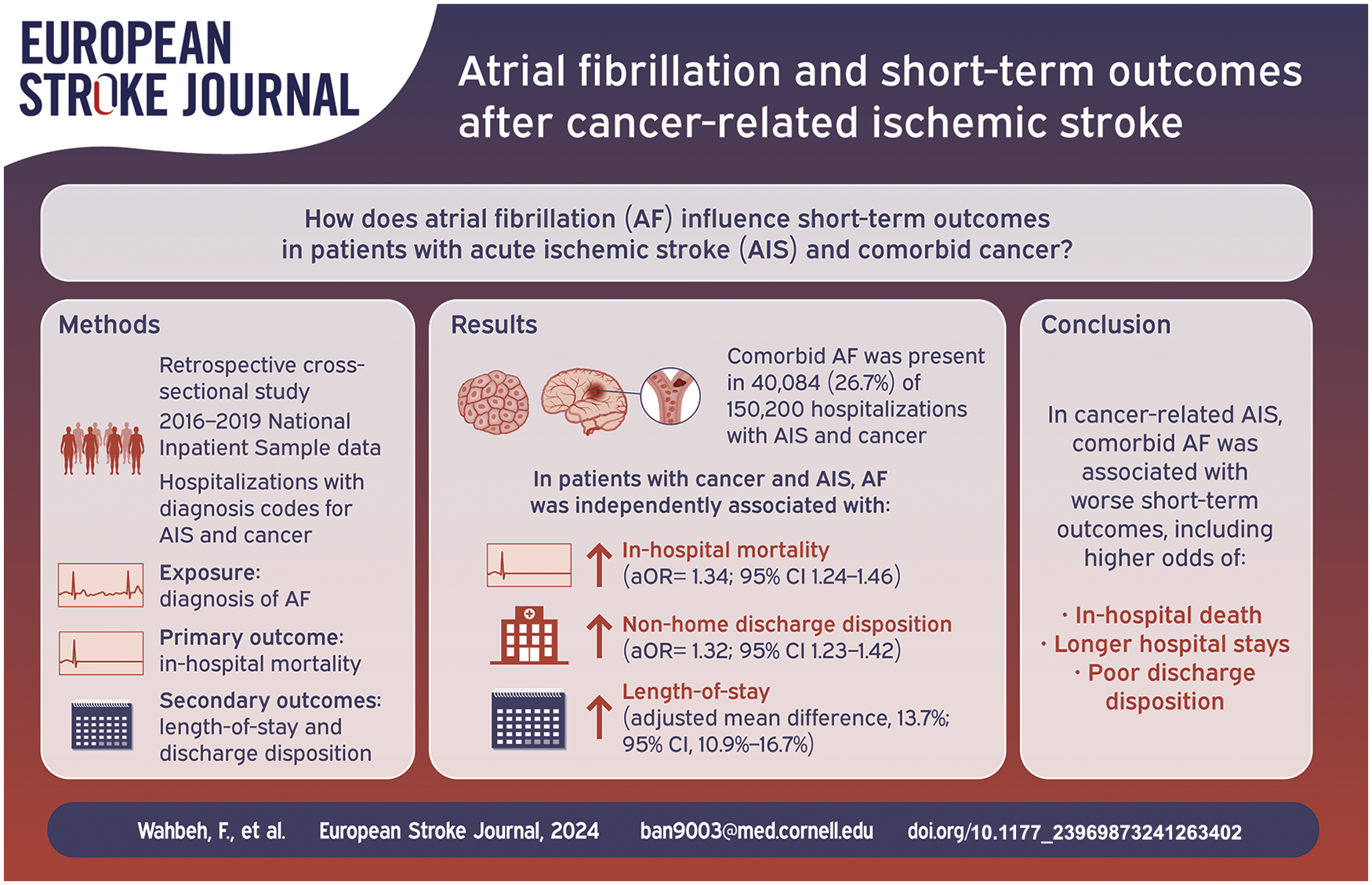
Atrial fibrillation (AF) and cancer are each associated with worse outcomes in patients with acute ischemic stroke (AIS). Few studies have evaluated the impact of AF on outcomes of cancer-related stroke.
We conducted a retrospective cross-sectional study using the 2016–2019 National Inpatient Sample, identifying all hospitalizations with diagnosis codes for cancer and AIS. The primary exposure was a diagnosis of AF. The primary outcome was in-hospital mortality. The secondary outcomes were length-of-stay and discharge to non-home locations. We used multiple logistic and linear regression models, adjusted for age, gender, race-ethnicity, and the Charlson Comorbidity Index, to examine the association between AF and study outcomes.
Among 150,200 hospitalizations with diagnoses of cancer and AIS (mean age 72 years, 53% male), 40,084 (26.7%) included comorbid AF. Compared to hospitalizations without AF, hospitalizations with AF had higher rates of in-hospital mortality (14.8% [95% CI, 14.0%−15.6%] vs 12.1% [95% CI, 11.6%−12.5%]) and non-home discharge disposition (83.5% [95% CI, 82.7%−84.3%] vs 75.1% [95% CI, 74.5%−75.7%]) as well as longer mean length-of-stay (8.4 days [95% CI, 8.2–8.6 days] vs 8.2 days [95% CI, 8.0–8.3 days]). In multivariable analyses, AF remained independently associated with higher odds of in-hospital mortality (adjusted odds ratio [aOR], 1.34; 95% CI, 1.24–1.46), non-home discharge disposition (aOR, 1.32; 95% CI, 1.23–1.42), and longer length-of-stay (adjusted mean difference, 13.7%; 95% CI, 10.9%−16.7%).
In cancer-related AIS, comorbid AF is associated with worse short-term outcomes, including higher odds for in-hospital mortality, poor discharge disposition, and longer hospital stays.
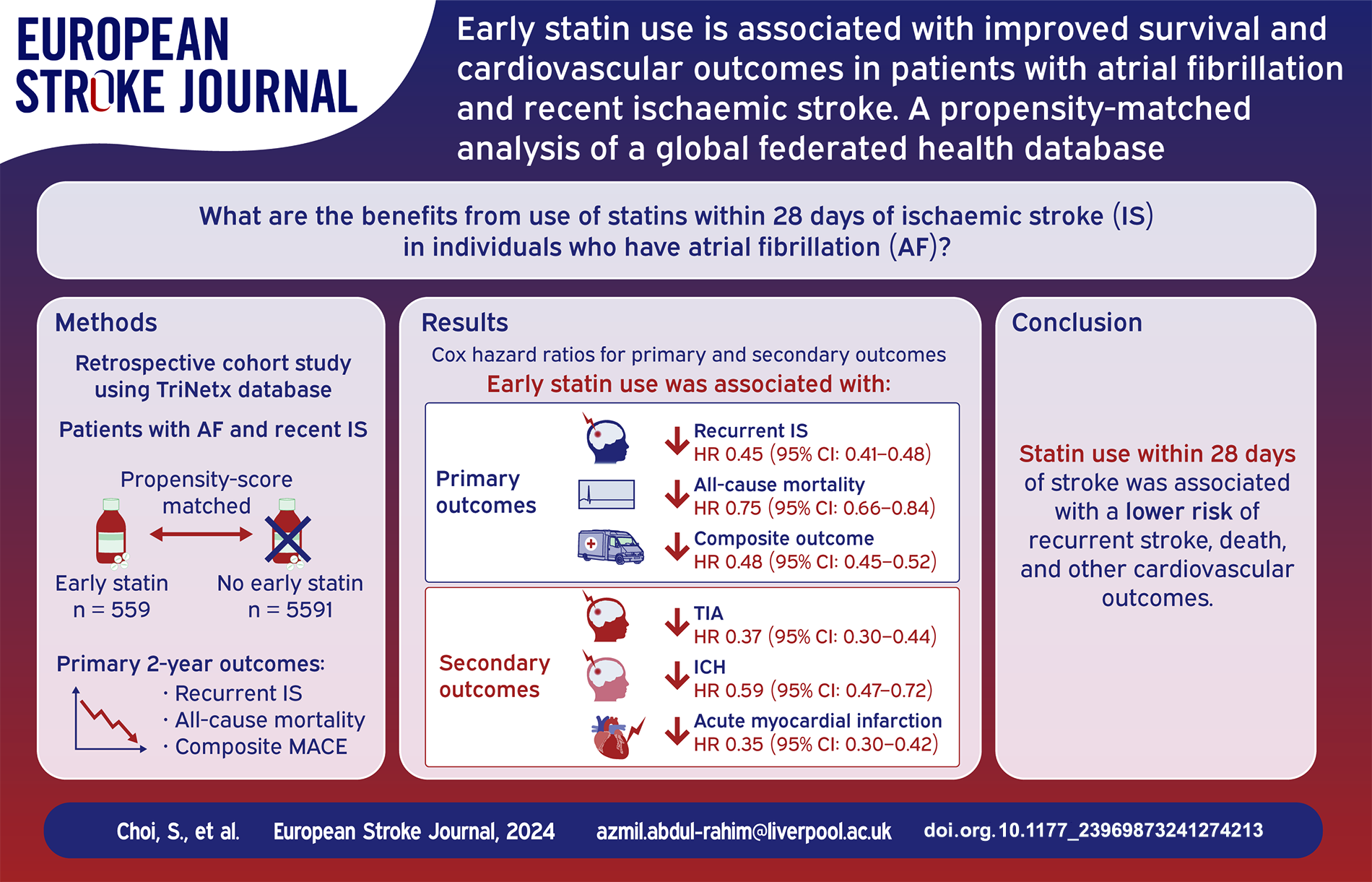
Statins reduce recurrent stroke and cardiovascular events in patients with non-cardioembolic stroke. The benefits of statins in patients with AF and recent IS remain unclear. We aimed to investigate the benefits of statins in patients with AF and recent IS.
This retrospective, cohort study was conducted using deidentified electronic medical records within TriNetX platform. Patients with AF and recent IS, who received statins within 28 days of their index stroke were propensity score-matched with those who did not. Patients were followed up for up to 2 years. Primary outcomes were the 2-year risk of recurrent IS, all-cause mortality and the composite outcome of all-cause mortality, recurrent IS, transient ischaemic attack (TIA), and acute myocardial infarction (MI). Secondary outcomes were the 2-year risk of TIA, intracranial haemorrhage (ICH), acute MI, and hospital readmission. Cox regression analyses were used to calculate hazard ratios (HRs) with 95% confidence intervals (95%CI).
Of 20,902 patients with AF and recent IS, 7500 (35.9%) received statins within 28 days of their stroke and 13,402 (64.1%) did not. 11,182 patients (mean age 73.7 ± 11.5; 5277 (47.2%) female) remained after propensity score matching. Patients who received early statins had significantly lower risk of recurrent IS (HR: 0.45, 95%CI: 0.41–0.48,
Patients with AF and recent IS, who received early statins, had a lower risk of recurrent stroke, death, and other cardiovascular outcomes including ICH, compared to those who did not.
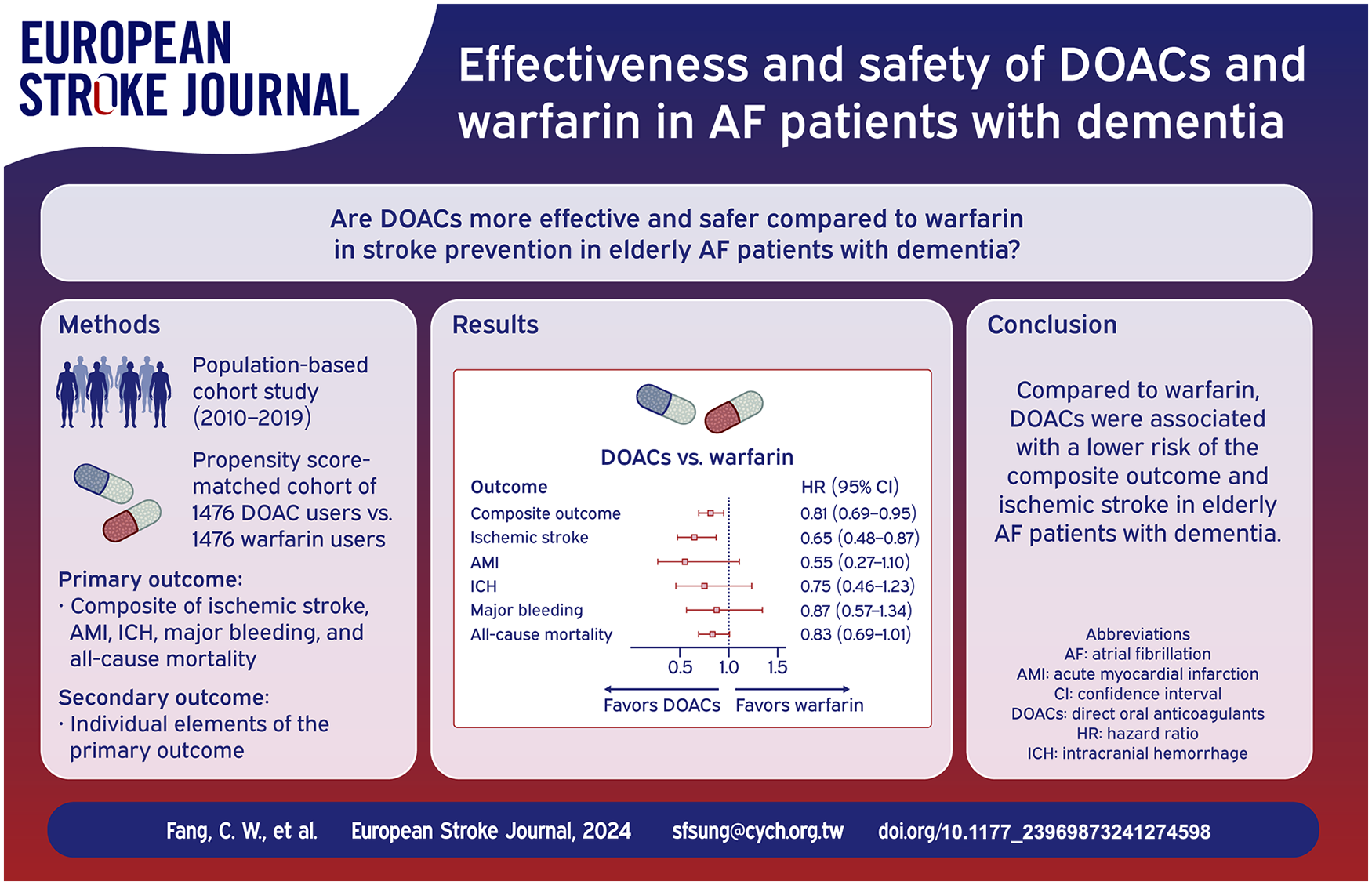
Developing an effective stroke prevention strategy is crucial for elderly atrial fibrillation (AF) patients with dementia. This is due to the limited and inconsistent evidence available on this topic. In this nationwide, population-based cohort study, we aim to compare the effectiveness and safety of direct oral anticoagulants (DOACs) and warfarin in AF patients with dementia.
We identified AF patients with dementia, aged 50 years or older, from Taiwan’s National Health Insurance Research Database between 2010 and 2019. The primary outcome was a composite of hospitalizations due to ischemic stroke, acute myocardial infarction, intracranial hemorrhage, or major bleeding, as well as all-cause mortality. We used 1:1 propensity score matching and Cox proportional hazard models to adjust for confounding factors when comparing outcomes between warfarin and DOAC (apixaban, dabigatran, edoxaban, or rivaroxaban) users or warfarin and each individual DOAC.
There were 2952 patients in the DOAC-warfarin matched cohort. The apixaban-, dabigatran-, edoxaban-, and rivaroxaban-warfarin matched cohorts had 2346, 2554, 1684, and 2938 patients, respectively. The DOAC group, when compared to warfarin, was associated with a lower risk of both the composite outcome (hazard ratio (HR), 0.81; 95% confidence interval (CI) 0.69–0.95) and ischemic stroke (HR 0.65; 95% CI 0.48–0.87). Apixaban (HR 0.79; 95% CI 0.66–0.94), dabigatran (HR 0.64; 95% CI 0.53–0.77), and rivaroxaban (HR 0.82; 95% CI 0.70–0.97) were also associated with a lower risk of the composite outcome.
Compared to warfarin, DOACs, whether as a group or apixaban, dabigatran, or rivaroxaban individually, were associated with a reduced risk of the composite outcome in elderly patients with concurrent AF and dementia.
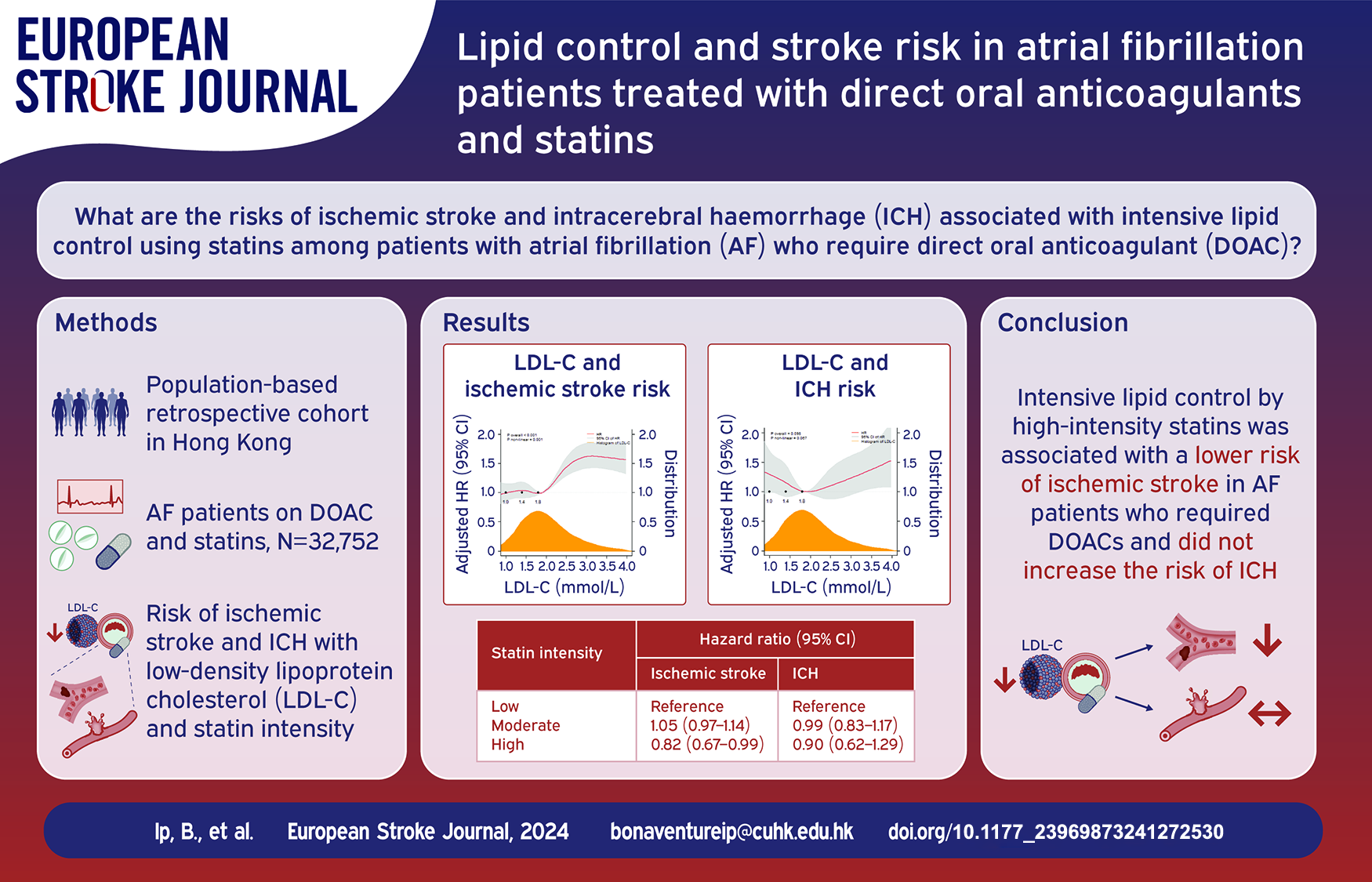
The risk of ischemic stroke and intracerebral hemorrhage (ICH) with intensive lipid control by statins among patients with atrial fibrillation (AF) who require direct oral anticoagulants (DOAC) is unclear. We aimed to determine the risks of ischemic stroke and ICH in AF patients treated with DOAC and statins.
In a population-based retrospective cohort study, we identified AF patients concurrently on DOAC and statins from 2015 to 2021 in Hong Kong. Primary outcome was ischemic stroke. Secondary outcomes were ICH and death. We correlated study outcomes with low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) as time-varying, continuous variables with restricted cubic spline. In secondary analyses, the risks of study outcomes with statin intensity (low, moderate, high) were determined by multivariable time-dependent marginal structural Cox models.
We identified 32,752 AF patients co-prescribed with DOAC and statins. Lower LDL-C (
Intensive lipid control by high-intensity statins was associated with a lower risk of ischemic stroke in AF patients who required DOACs and did not appear to increase the risk of ICH.
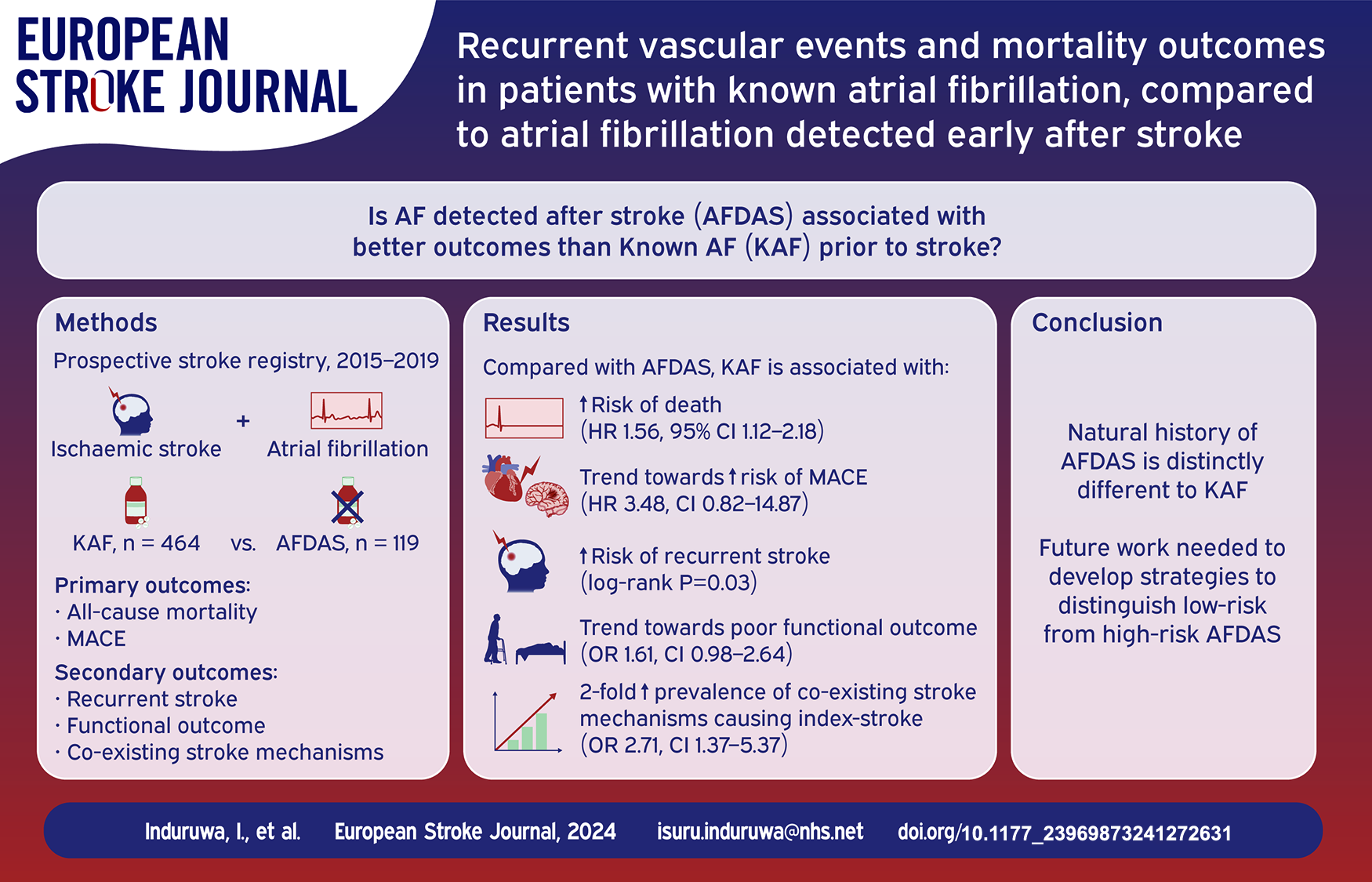
Atrial fibrillation (AF) detected after stroke (AFDAS) may represent a distinct clinical entity to that of known AF (KAF). However, there is limited long-term outcome data available for patients with AFDAS. More information regarding prognosis in AFDAS is required to inform future trial design in these patients.
We used data (2015–2019) from a national prospective stroke registry of consecutive patients with acute ischaemic stroke and AF. AFDAS was defined as a new diagnosis of AF after stroke detected on electrocardiograph or cardiac monitoring. The co-primary endpoints were: (1) all-cause mortality; (2) recurrent major adverse cardiovascular events (MACE) at 3 years. Secondary endpoints were: (1) recurrent stroke; (2) functional outcome at discharge; (3) presence of co-existing stroke mechanisms.
583 patients were included. After a median follow-up of 2.65 years (cumulative 1064 person-years) 309 patients died and 23 had recurrent MACE. Compared with AFDAS, KAF was associated with a higher risk of all-cause mortality (adjusted Hazard Ratio (aHR) 1.56, 95% CI 1.12–2.18), a higher prevalence of co-existing stroke mechanisms (adjusted odds ratio (aOR) 2.28, 95% CI 1.14–4.59), but not poor functional outcome (aOR 1.61, 95% CI 0.98–2.64). A trend towards a higher risk of MACE was observed in patients with KAF, but this was limited by statistical power (aHR 2.90, 95% CI 0.67–12.51). All 14 recurrent strokes occurred in the KAF group (Log-rank
These data provide further evidence that AFDAS differs to KAF with respect to risk of recurrent stroke, MACE, and all-cause mortality.
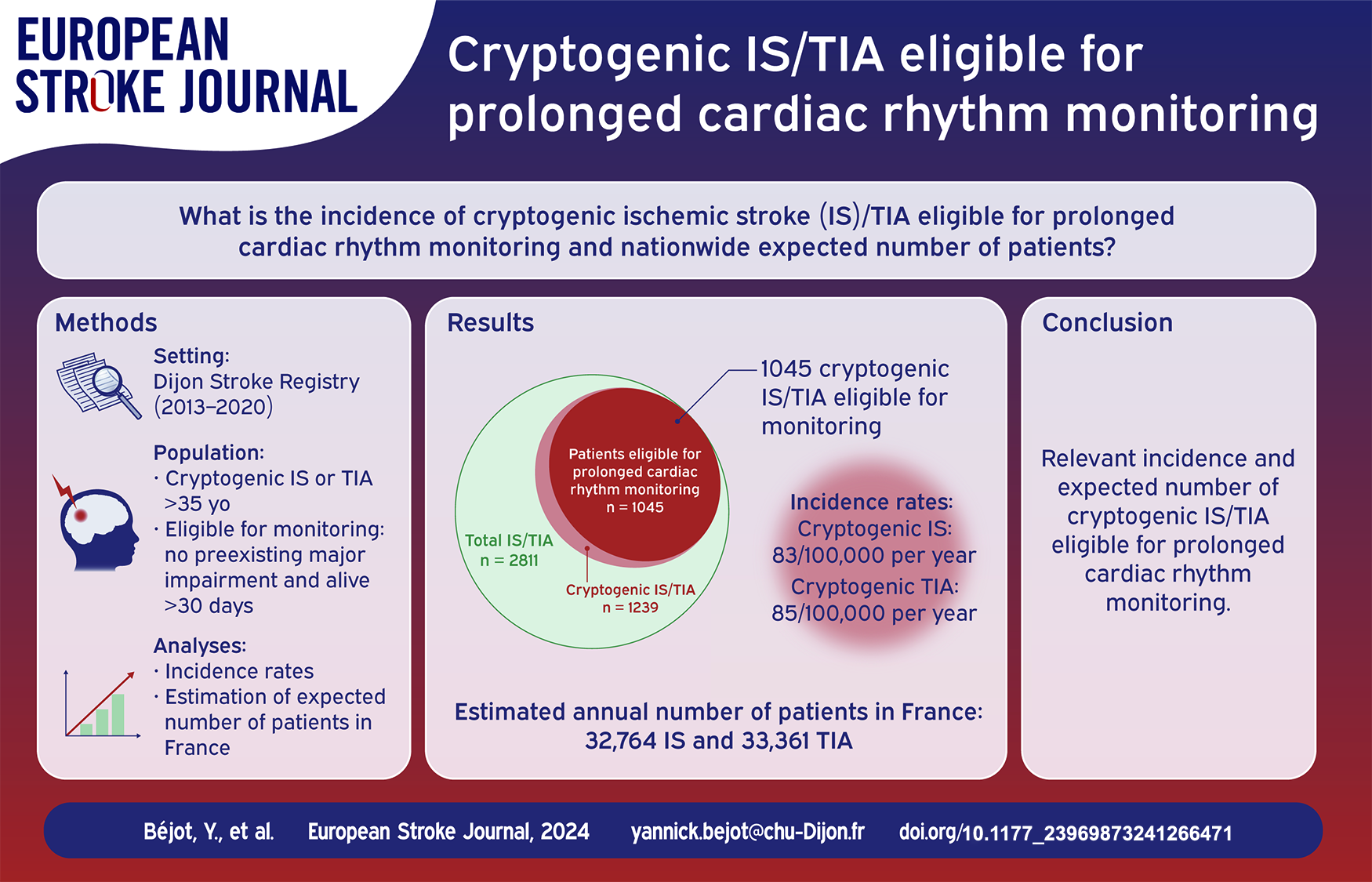
Current guidelines indicate prolonged cardiac rhythm monitoring for atrial fibrillation screening in patients with cryptogenic ischemic stroke (IS) or transient ischemic attack (TIA). This study aimed to assess the incidence of cryptogenic IS/TIA eligible for such investigation, and to estimate the number of patients potentially concerned in whole France annually.
All cryptogenic acute IS/TIA cases ⩾35 years old were retrieved from the population-based Dijon Stroke Registry, France (2013–2020). Patients eligible for prolonged cardiac rhythm monitoring were defined after excluding those who died in-hospital or within the first 30 days, or with preexisting major impairment. Annual incidence rates of eligible cryptogenic IS/TIA were calculated by age groups and sex. The total number of eligible patients in France was estimated by standardization to age- and sex-specific incidence.
Among 2811 IS/TIA patients recorded in the Dijon Stroke Registry, 1239 had cryptogenic IS/TIA of whom 1045 were eligible for prolonged cardiac rhythm monitoring (517 IS and 528 TIA, mean age 73.6 ± 14.6 years old, 55.4% women). Crude incidence rates of eligible cryptogenic IS/TIA were 169/100,000 per year (95% CI: 159–179) in overall sexes, 83/100,000 per year (95% CI: 76–91) for IS, and 85/100,000 per year (95% CI: 78–93) for TIA. The total number of patients with cryptogenic IS/TIA eligible for prolonged cardiac rhythm monitoring in France was estimated to be 66,125 (95% CI: 65,622–66,630) for the calendar year 2022, including 32,764 (95% CI: 32,410–33,120) with IS and 33,361 (95% CI: 33,004–33,721) with TIA.
This study demonstrated a high incidence of cryptogenic IS/TIA eligible for prolonged cardiac rhythm monitoring. Estimates at a national level pointed out the large number of patients who may require access to such atrial fibrillation screening, with attention to be paid on regarding organization of care networks and related costs.
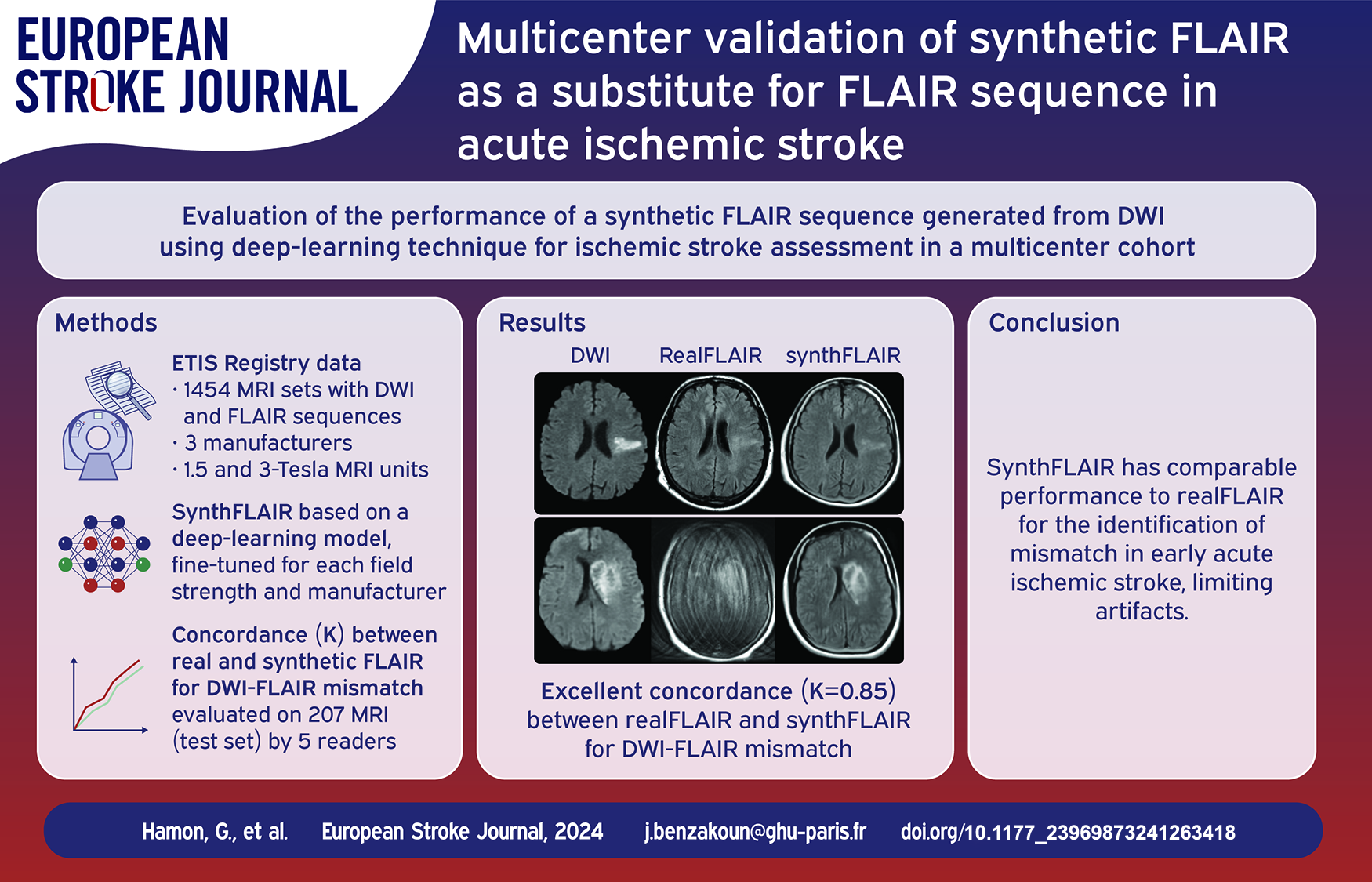
To evaluate performance of synthetic and real FLAIR for identifying early stroke in a multicenter cohort.
This retrospective study was conducted using DWI and FLAIR extracted from the Endovascular Treatment in Ischemic Stroke image registry (2017–2021). The database was partitioned into subsets according to MRI field strength and manufacturer, and randomly divided into training set (70%) used for model fine-tuning, validation set (15%), and test set (15%). In test set, five readers, blinded to FLAIR sequence type, assessed DWI-FLAIR mismatch using real and synthetic FLAIR. Interobserver agreement for DWI-FLAIR rating and concordance between synthetic and real FLAIR were evaluated with kappa statistics. Sensitivity and specificity for identification of ⩽4.5 h AIS were compared in patients with known onset-to-MRI delay using McNemar’s test.
1454 complete MRI sets (1172 patients, median (IQR) age: 73 years (62–82); 762 women) acquired on 125 MRI units were analyzed. In test set (207 MRI), interobserver reproducibility for DWI-FLAIR mismatch labeling was substantial for real and synthetic FLAIR (Fleiss κ = 0.79 (95%CI: 0.73–0.84) and 0.77 (95%CI: 0.71–0.82), respectively). After consensus, concordance between real and synthetic FLAIR was excellent (κ = 0.85 (95%CI: 0.78–0.92)). In 141 MRI sets with known onset-to-MRI delay, diagnostic performances for ⩽4.5 h AIS identification did not differ between real and synthetic FLAIR (sensitivity: 60/71 (85%) vs 59/71 (83%),
A deep-learning-based FLAIR fine-tuned on multicenter data can provide comparable performances to real FLAIR for early AIS identification. This approach may help reducing MR protocol duration and motion artifacts.
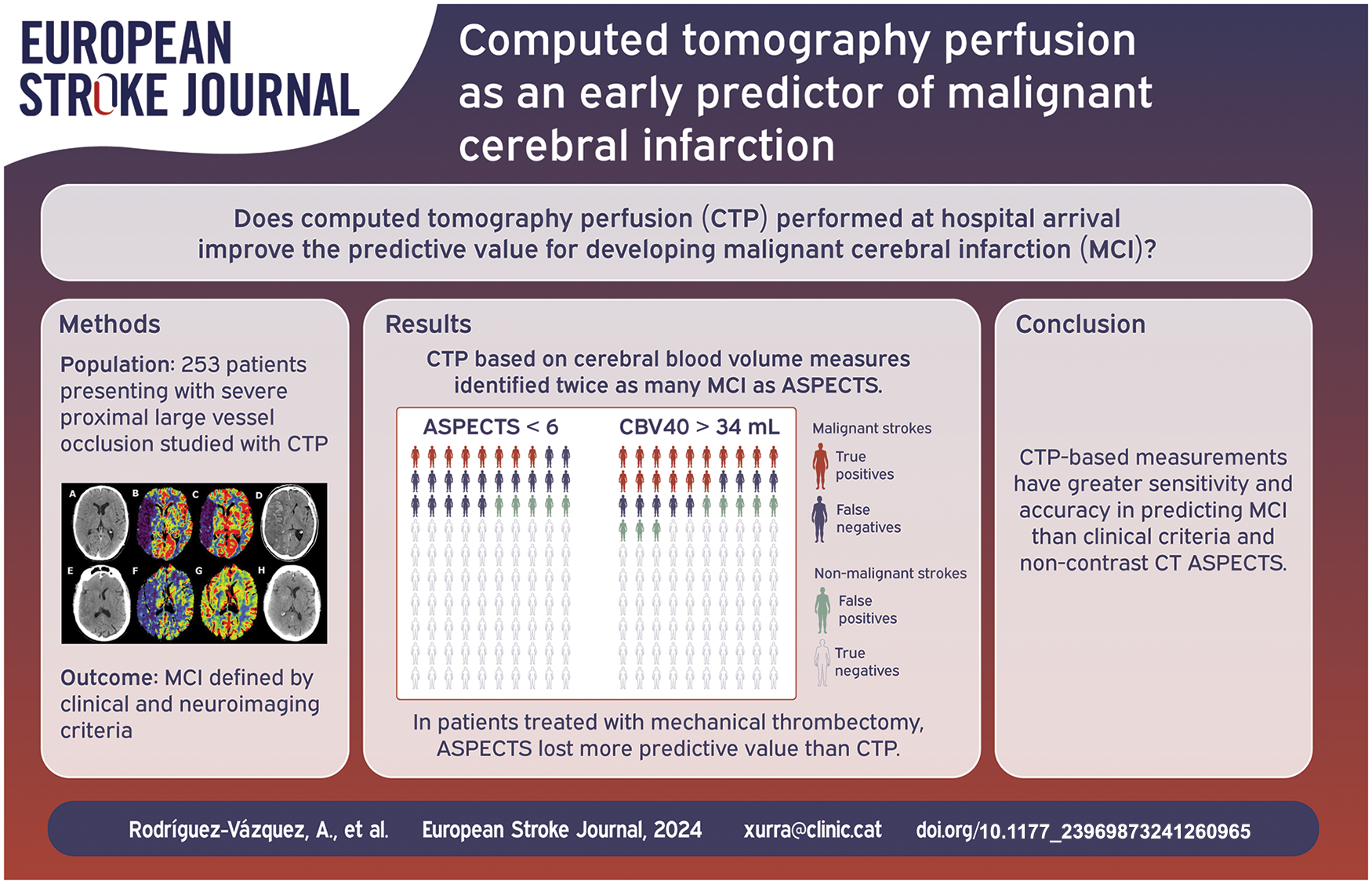
Malignant middle cerebral artery infarction (MCI) needs rapid intervention. This study aimed to enhance the prediction of MCI using computed tomography perfusion (CTP) with varied quantitative benchmarks.
We retrospectively analyzed 253 patients from a single-center registry presenting with acute, severe, proximal large vessel occlusion studied with whole-brain CTP imaging at hospital arrival within the first 24 h of symptoms-onset. MCI was defined by clinical and imaging criteria, including decreased level of consciousness, anisocoria, death due to cerebral edema, or need for decompressive craniectomy, together with midline shift ⩾6 mm, or infarction of more than 50% of the MCA territory. The predictive accuracy of baseline ASPECTS and CTP quantifications for MCI was assessed by receiver operating characteristic (ROC) area under the curve (AUC) while
Sixty-three out of 253 patients (25%) fulfilled MCI criteria and had worse clinical and imaging results than the non-MCI group. The capacity to predict MCI was lower for baseline ASPECTS (AUC 0.83,
CTP-based quantifications may offer enhanced predictive capabilities for MCI compared to non-contrast baseline CT ASPECTS, potentially improving the monitoring of severe ischemic stroke patients at risk of life-threatening edema and its treatment.
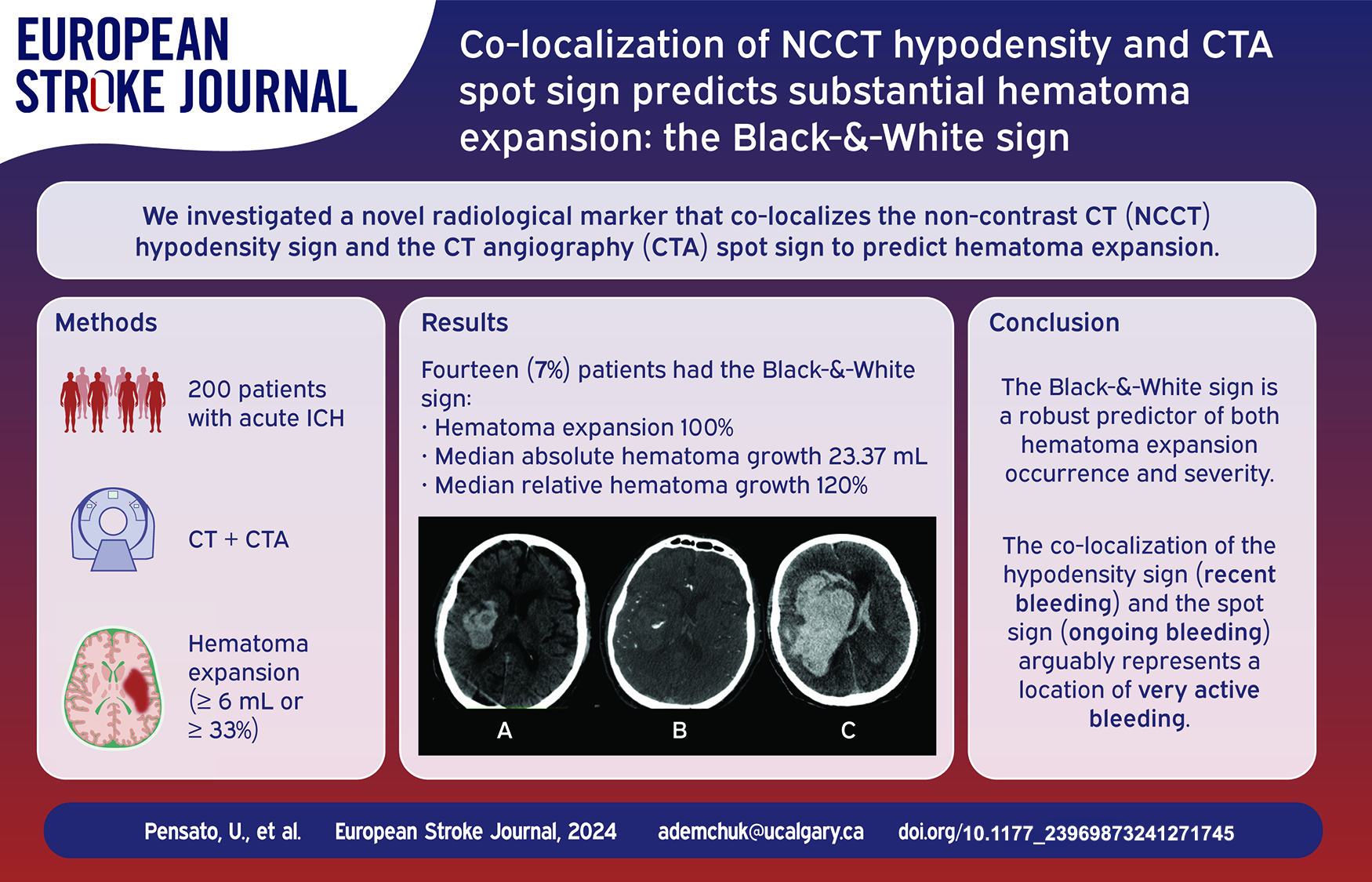
Existing radiological markers of hematoma expansion (HE) show modest predictive accuracy. We aim to investigate a novel radiological marker that co-localizes findings from non-contrast CT (NCCT) and CT angiography (CTA) to predict HE.
Consecutive acute intracerebral hemorrhage patients admitted at Foothills Medical Centre in Calgary, Canada, were included. The Black-&-White sign was defined as any visually identified spot sign on CTA co-localized with a hypodensity sign on the corresponding NCCT. The primary outcome was hematoma expansion (⩾6 mL or ⩾33%). Secondary outcomes included absolute (<3, 3–6, 6–12, ⩾12 mL) and relative (0%, <25%, 25%–50%, 50%–75%, or >75%) hematoma growth scales.
Two-hundred patients were included, with 50 (25%) experiencing HE. Forty-four (22%) showed the spot sign, 69 (34.5%) the hypodensity sign, and 14 (7%) co-localized both as the Black-&-White sign. Those with the Black-&-White sign had higher proportions of HE (100% vs 19.4%,
The Black-&-White sign is a robust predictor of hematoma expansion occurrence and severity, yet further validation is needed to confirm these compelling findings.
The prognosis for stroke patients with type 2 diabetes mellitus (T2DM) remains poorly understood. We examined the risk of mortality and stroke recurrence in stroke patients with T2DM and stroke patients without diabetes.
We conducted a population-based cohort study including all patients diagnosed with a first-time ischemic stroke (
Following ischemic stroke, the 5-year standardized mortality was 46.1% for patients with T2DM and 35.4% for patients without diabetes (standardized risk difference: 10.7% [95% CI 9.9–11.6]; risk ratio: 1.3 [95% CI 1.3–1.3]). The 5-year risk of recurrence following ischemic stroke was 12.7% for patients with T2DM and 11.3% for those without diabetes (risk difference: 1.4% [95% CI 0.9–2.0]; risk ratio: 1.1 [95% CI 1.1–1.2]). Following ICH, the 5-year mortality was 62.8% for patients with T2DM and 53.0% for patients without diabetes (risk difference: 9.8% [95% CI 7.2–12.4)]; risk ratio: 1.2 [95% CI 1.1–1.2]). The 5-year risk of recurrence after ICH was 9.1% for patients with T2DM and 9.7% for patients without diabetes.
Stroke patients with T2DM were at increased risk of mortality. The risk of stroke recurrence was slightly higher for ischemic stroke patients with T2DM than patients without diabetes, while no difference was observed among ICH patients.

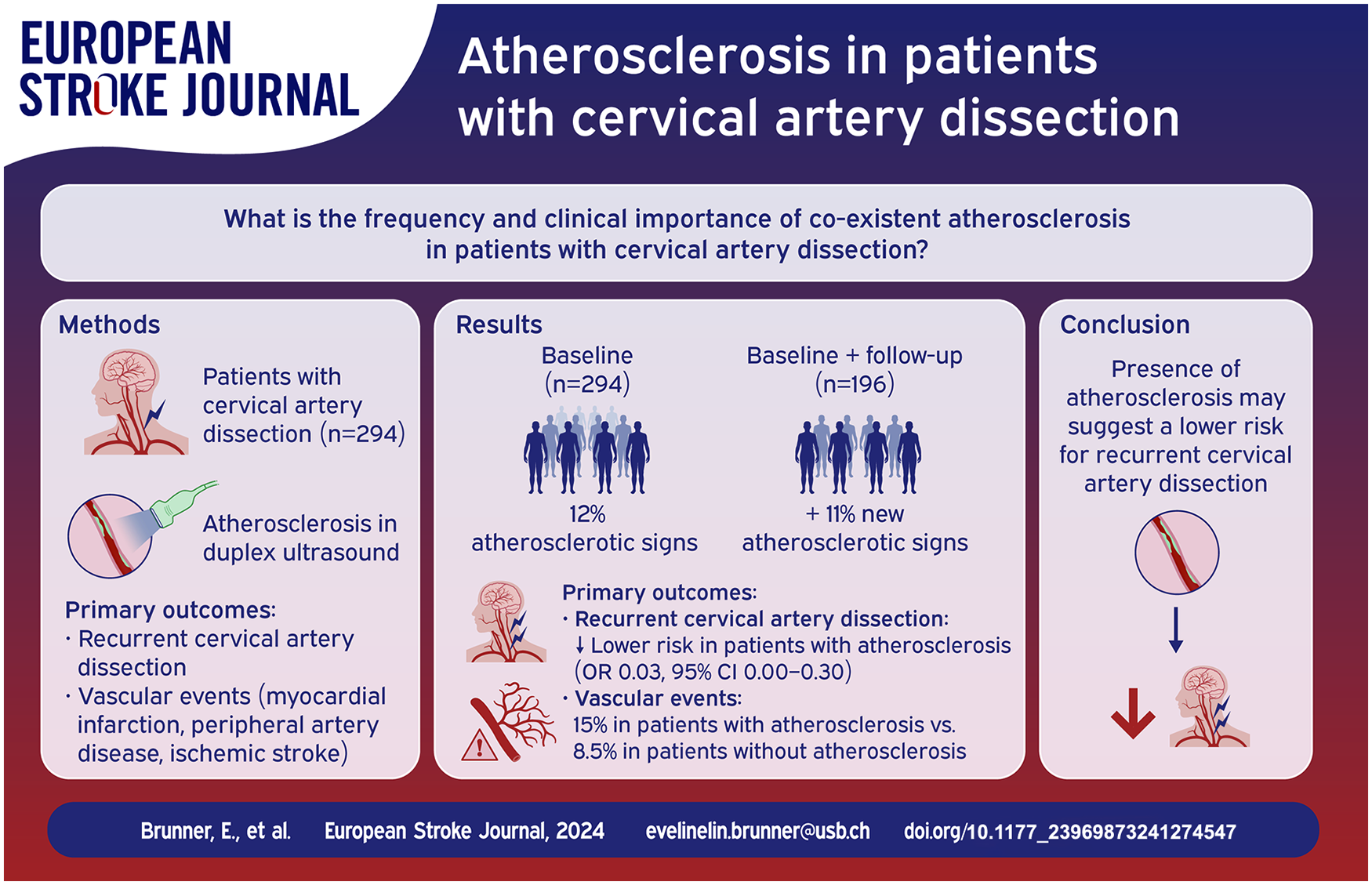
Cervical artery dissection (CeAD) is considered a non-atherosclerotic arteriopathy, but atherosclerosis of the cervical arteries may co-exist. We explored the frequency and clinical importance of co-existent atherosclerosis in patients with CeAD.
Single-center exploratory study from the Stroke Center Basel, Switzerland. We re-reviewed duplex ultrasound images at (i) baseline and (ii) last follow-up visit for the presence versus absence of the following atherosclerotic manifestations in the carotid arteries: (i) abnormal carotid intima-media thickness, (ii) plaques, and (iii) atherosclerotic stenosis. We investigated whether CeAD patients with versus without co-existing atherosclerosis differ regarding (a) recurrence of CeAD and (b) occurrence of vascular events (myocardial infarction, peripheral artery disease, or ischemic stroke) using logistic regression with adjustment for age and follow-up time.
Among 294 CeAD patients (median age 46 [IQR 37–53], 41.8% women), 35 (12%) had any atherosclerotic signs at baseline. Among 196 patients with available follow-up, another 21/196 (11%) patients developed atherosclerosis during a median follow-up of 55.7 months. Patients with atherosclerosis had decreased odds of recurrent CeADs when compared to patients without atherosclerosis (OR 0.03, 95% CI = 0.00-0.30). During follow-up, 6 (15%) vascular events occurred among 40 CeAD patients with atherosclerosis and 13 (8.5%) among 153 patients without atherosclerosis (OR 1.38, 95% CI = 0.39-4.55, data for 3 patients were missing).
Signs of atherosclerosis in the carotid artery were detectable in 12% of CeAD patient at baseline. Additionally, 11% of CeAD patients developed new signs of atherosclerosis within the following 5 years. The presence of atherosclerosis may suggest a lower risk for recurrent CeAD. Whether it might indicate an increased risk for late clinical vascular events deserves further studies.
The Tranexamic acid for IntraCerebral Haemorrhage-2 (TICH-2) trial reported no significant improvement in death and dependency at day 90 despite reductions in haematoma expansion, early neurological deterioration and early death. However, significant recovery after stroke, particularly intracerebral haemorrhage (ICH), may take more than 3 months. Here we report the participant outcomes at 1 year after stroke.
TICH-2 was a prospective randomised controlled trial that tested the efficacy and safety of tranexamic acid in spontaneous ICH when given within 8 h of onset. Patients with ICH on anticoagulation were excluded. Centralised blinded telephone follow up was performed for patients from the United Kingdom at 1 year. The primary outcome was modified Rankin Scale at 1 year. Secondary outcomes included Barthel index, Telephone Interview Cognitive Status-modified, EuroQoL-5D and Zung Depression Scale. This was a prespecified secondary analysis of the TICH-2 trial.
About 2325 patients were recruited into the trial (age 68.9 ± 13.8 years; 1301 male, 56%). About 1910 participants (82.2%) were eligible for day 365 follow up. 57 patients (3.0%) were lost to follow up. Tranexamic acid did not reduce the risk of poor functional outcome at 1 year (adjusted OR 0.91 95% CI 0.77–1.09;
There was no difference in functional outcome at 1 year after ICH. Tranexamic acid may reduce mortality at 1 year without an increase in severely dependent survivors. But this should be interpreted with caution as this is a result of secondary analysis in a neutral trial.
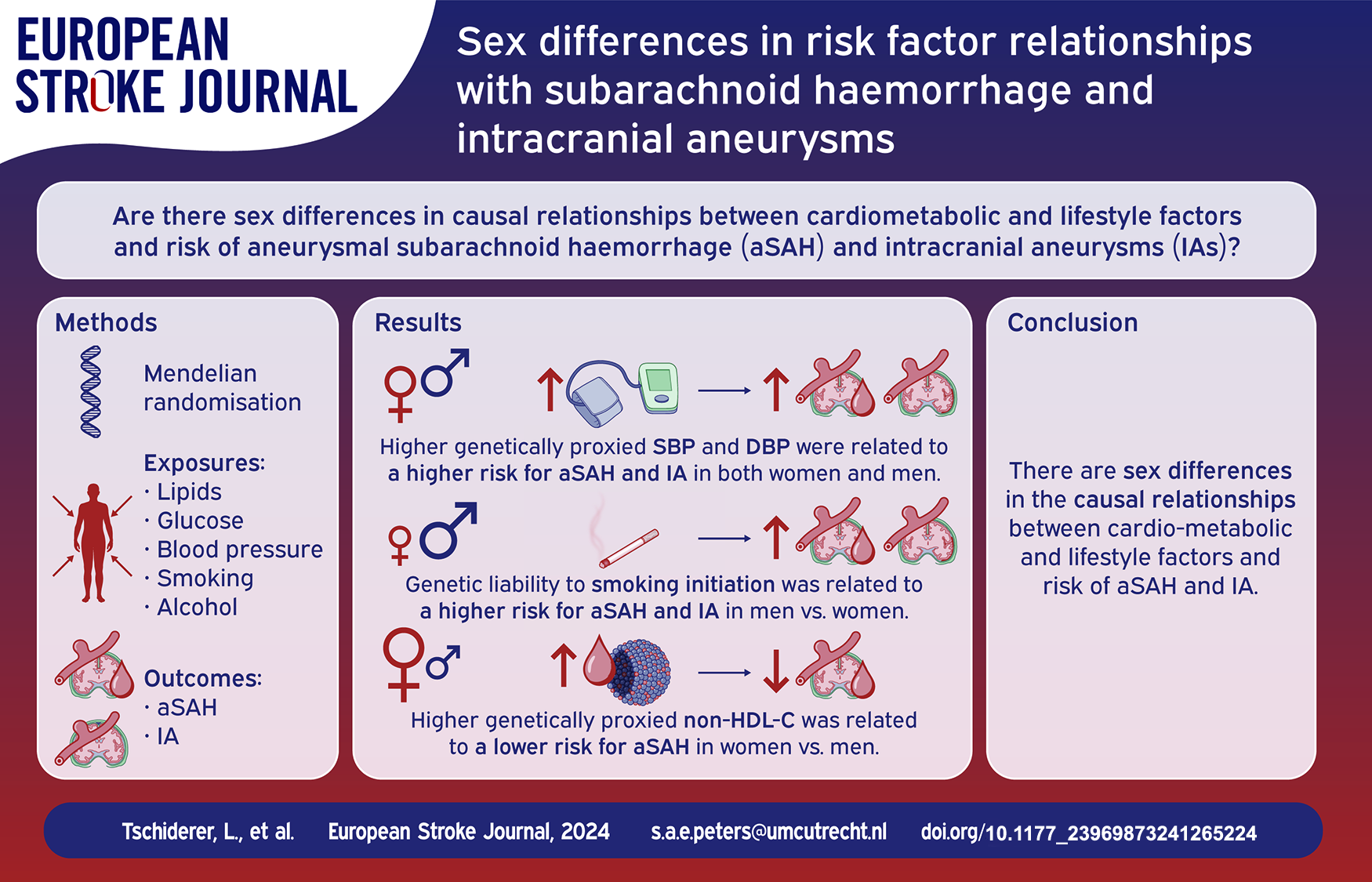
The prevalence of intracranial aneurysms (IAs) and incidence of aneurysmal subarachnoid haemorrhage (aSAH) is higher in women than in men. Although several cardiometabolic and lifestyle factors have been related to the risk of IAs or aSAH, it is unclear whether there are sex differences in causal relationships of these risk factors.
The aim of this study was to determine sex differences in causal relationships between cardiometabolic and lifestyle factors and risk of aSAH and IA.
We conducted a sex-specific two-sample Mendelian randomization study using summary-level data from genome-wide association studies. We analysed low-density lipoprotein cholesterol, high-density lipoprotein cholesterol [HDL-C], triglycerides, non-HDL-C, total cholesterol, fasting glucose, systolic and diastolic blood pressure, smoking initiation, and alcohol use as exposures, and aSAH and IA (i.e. aSAH and unruptured IA combined) as outcomes.
We found statistically significant sex differences in the relationship between genetically proxied non-HDL-C and aSAH risk, with odds ratios (ORs) of 0.72 (95% confidence interval 0.58, 0.88) in women and 1.01 (0.77, 1.31) in men (
Higher genetically proxied non-HDL-C was related to a lower risk of aSAH in women compared to men. Moreover, genetic liability to smoking initiation was associated with a higher risk for aSAH and IA in men compared to women. These findings may help improve understanding of sex differences in the development of aSAH and IA.
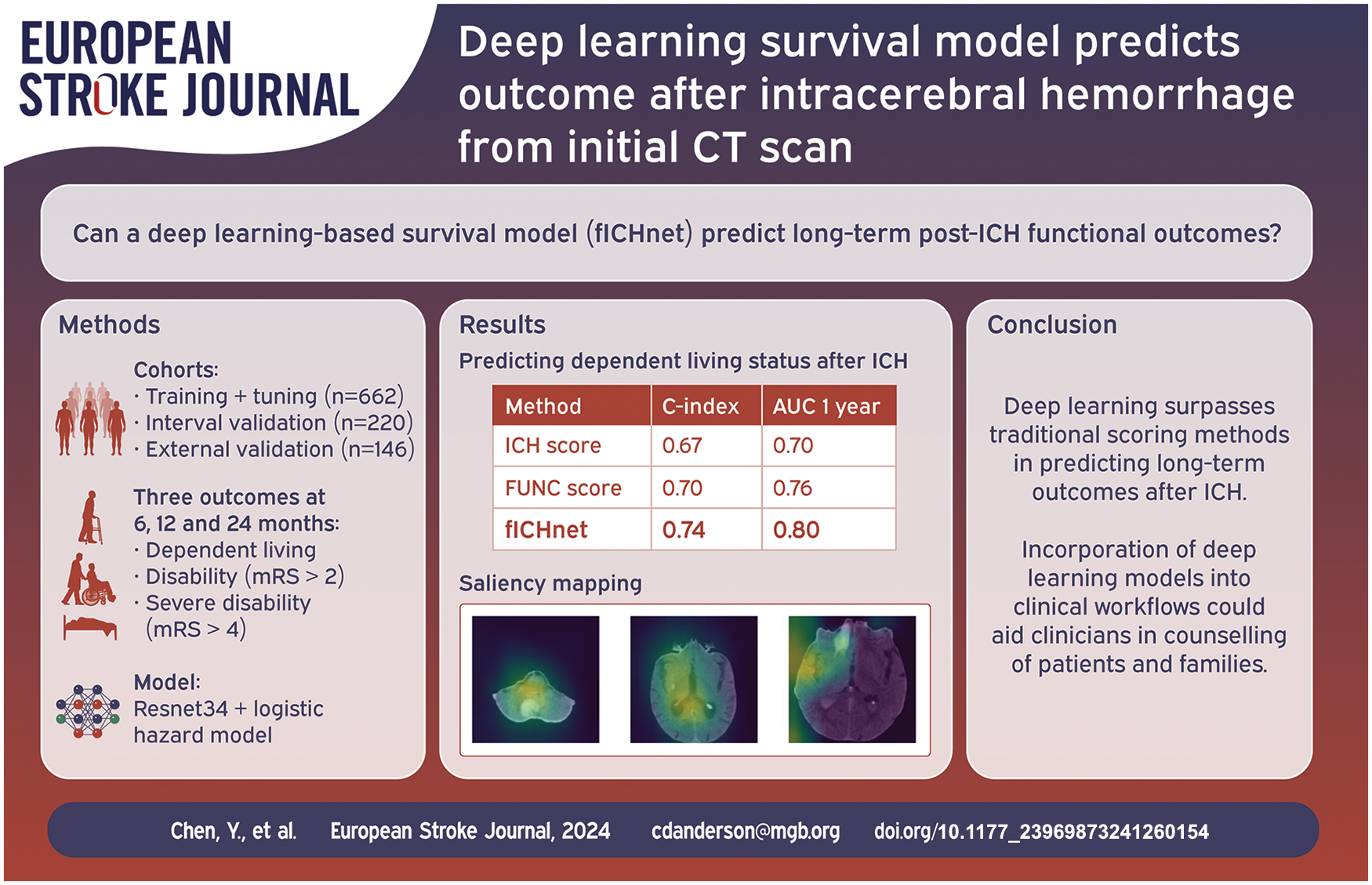
Predicting functional impairment after intracerebral hemorrhage (ICH) provides valuable information for planning of patient care and rehabilitation strategies. Current prognostic tools are limited in making long term predictions and require multiple expert-defined inputs and interpretation that make their clinical implementation challenging. This study aimed to predict long term functional impairment of ICH patients from admission non-contrast CT scans, leveraging deep learning models in a survival analysis framework.
We used the admission non-contrast CT scans from 882 patients from the Massachusetts General Hospital ICH Study for training, hyperparameter optimization, and model selection, and 146 patients from the Yale New Haven ICH Study for external validation of a deep learning model predicting functional outcome. Disability (modified Rankin scale [mRS] > 2), severe disability (mRS > 4), and dependent living status were assessed via telephone interviews after 6, 12, and 24 months. The prediction methods were evaluated by the c-index and compared with ICH score and FUNC score.
Using non-contrast CT, our deep learning model achieved higher prediction accuracy of post-ICH dependent living, disability, and severe disability by 6, 12, and 24 months (c-index 0.742 [95% CI –0.700 to 0.778], 0.712 [95% CI –0.674 to 0.752], 0.779 [95% CI –0.733 to 0.832] respectively) compared with the ICH score (c-index 0.673 [95% CI –0.662 to 0.688], 0.647 [95% CI –0.637 to 0.661] and 0.697 [95% CI –0.675 to 0.717]) and FUNC score (c-index 0.701 [95% CI– 0.698 to 0.723], 0.668 [95% CI –0.657 to 0.680] and 0.727 [95% CI –0.708 to 0.753]). In the external independent Yale-ICH cohort, similar performance metrics were obtained for disability and severe disability (c-index 0.725 [95% CI –0.673 to 0.781] and 0.747 [95% CI –0.676 to 0.807], respectively). Similar AUC of predicting each outcome at 6 months, 1 and 2 years after ICH was achieved compared with ICH score and FUNC score.
We developed a generalizable deep learning model to predict onset of dependent living and disability after ICH, which could help to guide treatment decisions, advise relatives in the acute setting, optimize rehabilitation strategies, and anticipate long-term care needs.
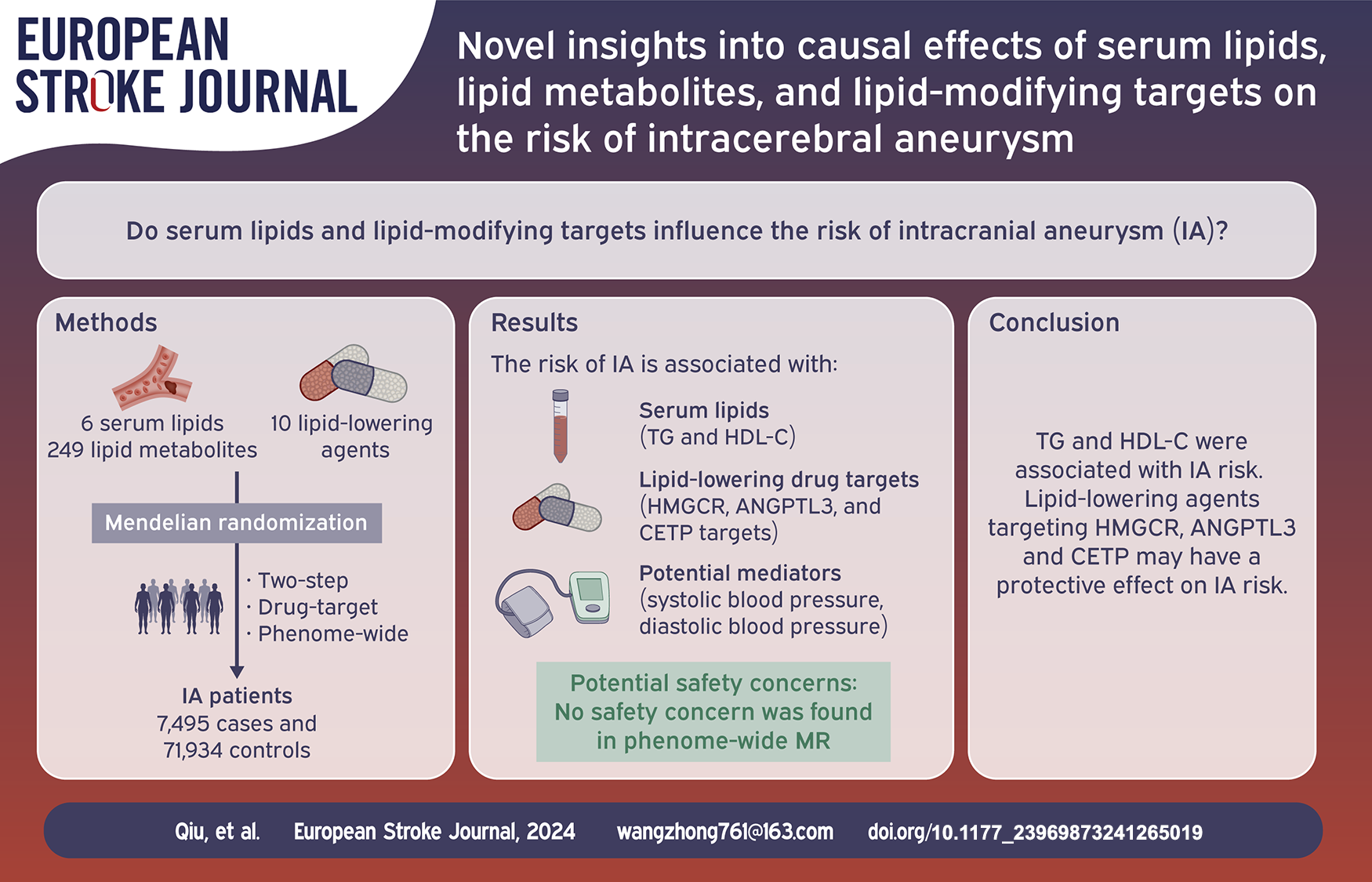
Different serum lipid and lipid-lowering agents are reported to be related to the occurrence of intracerebral aneurysm (IA). However, the causal relationship between them requires further investigation.
Mendelian randomization (MR) analysis was performed on IA and its subtypes by using instrumental variants associated with six serum lipids, 249 lipid metabolic traits, and 10 lipid-lowering agents that were extracted from the largest genome-wide association study. Phenome-wide MR analyses were conducted to identify potential phenotypes associated with significant lipid-lowering agents.
After multiple comparison adjustments (
This study not only supports that serum lipids (TG and HDL-C) are associated with IA but also confirms the positive effect and absence of safety concerns of intervening
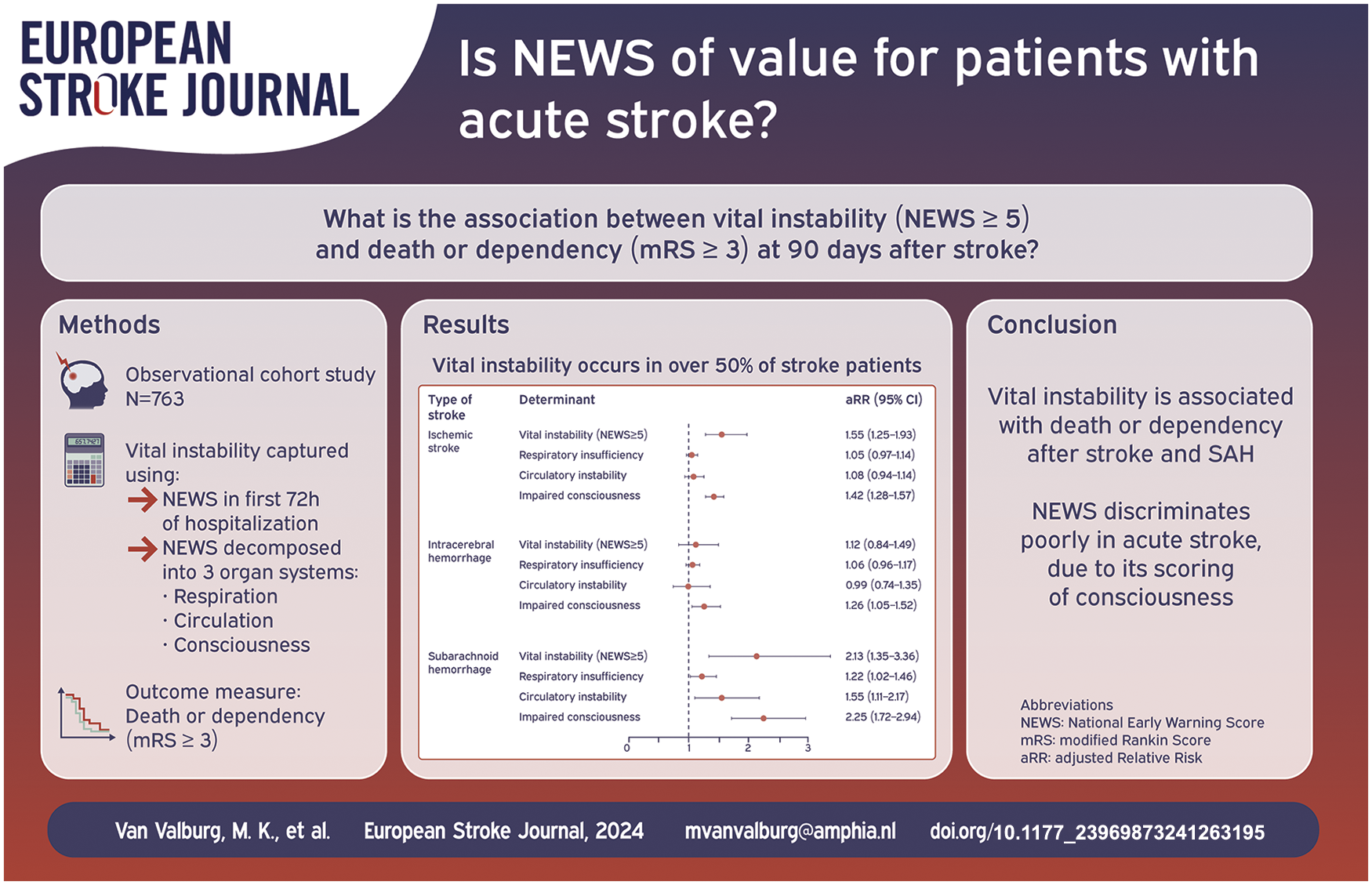
Patients with acute stroke are at risk of respiratory or circulatory compromise resulting in vital instability, which can be captured through the widely used aggregated National Early Warning Score (NEWS). We aimed to assess the relation between vital instability (defined as NEWS of five or higher) and death or dependency at 90 days after stroke.
In this observational cohort study we studied 763 patients with ischaemic stroke (
Two hundred and twenty-seven (58%) patients with ischaemic stroke, 101 (69%) with ICH and 142 (65%) with SAH had at least one episode of vital instability. In patients with ischaemic stroke or SAH, vital instability was associated after adjustment for confounders with death or dependency (adjusted relative risk 1.55 ((95% CI) 1.25–1.93 and 2.13 (1.35–3.36), respectively)). This was mainly driven by impaired consciousness, which was associated with death or dependency in all types of stroke. Respiratory insufficiency and circulatory instability were associated with death or dependency only in SAH.
Vital instability in the first 72 h of hospitalization for ischaemic stroke or SAH is associated with death or dependency at 90 days. Impaired consciousness was the main driver of this relationship. NEWS may not be appropriate for patients with acute stroke, mainly due to the dichotomous manner in which the level of consciousness is classified, and modification of NEWS should be considered for these patients
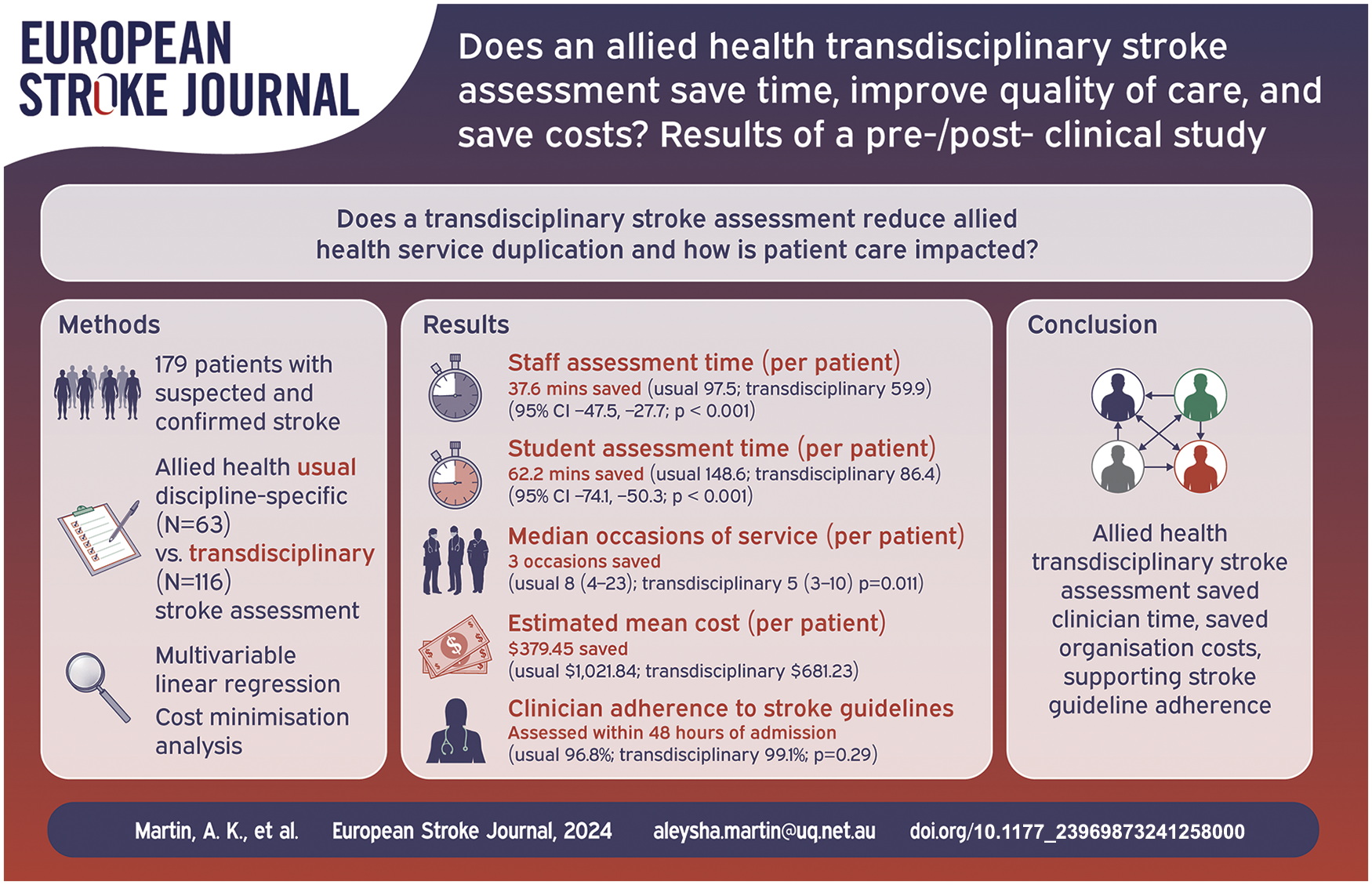
Demand for stroke services is increasing. To save time and costs, stroke care could be reorganised using a transdisciplinary assessment model embracing overlapping allied health professional skills. The study compares transdisciplinary assessment to discipline-specific allied health assessment on an acute stroke unit, by evaluating assessment time, quality of care, and cost implications.
The pre-/post- clinical study used non-randomised groups and 3-month follow-up after hospital admission. Patients with confirmed/suspected stroke received usual discipline-specific allied health assessment (pre-implementation phase) or the novel transdisciplinary assessment (post-implementation phase). Staff/student assessment times (primary outcome) and medical record data (secondary outcomes) were collected. Time differences were estimated using multivariable linear regression controlling for confounding factors. Cost minimisation and sensitivity analyses estimated change in hospital resource use.
When the transdisciplinary assessment was used (
Transdisciplinary stroke assessment has potential for reorganising allied health services to save assessment time and reduce healthcare costs. The transdisciplinary stroke assessment could be considered for implementation in other stroke services.
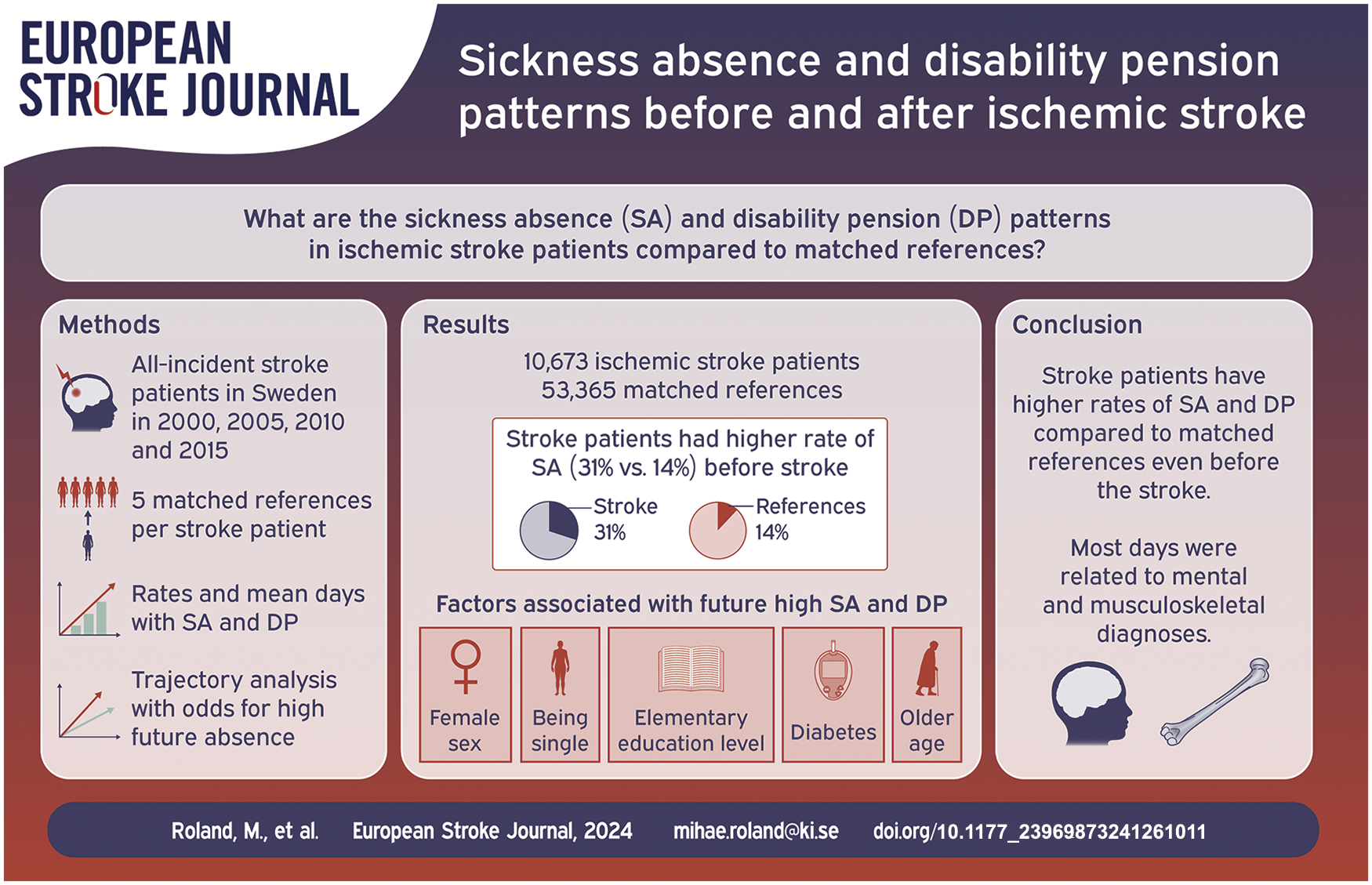
The aim was to determine ischemic stroke patients’ sickness absence and disability pension before and after stroke, and compare these to that of matched references.
All working-aged individuals (aged 18–61) in Sweden with incident ischemic stroke in year 2000, 2005, 2010, or 2015, respectively, and five population-based matched references to each stroke patient. Each cohort was followed 1 year prior stroke and 3 years after. We calculated rates and mean days of sickness absence and disability pension among stroke patients and references and computed trajectories of absence days with predictors of high sickness absence and disability pension.
Number of patients with incident ischemic stroke in 2000 (
Ischemic stroke patients have more absence days compared to matched references even before the stroke, mainly related to mental and musculoskeletal diagnoses. Future research should address the impact of efficient stroke treatment on sickness absence and disability pension.
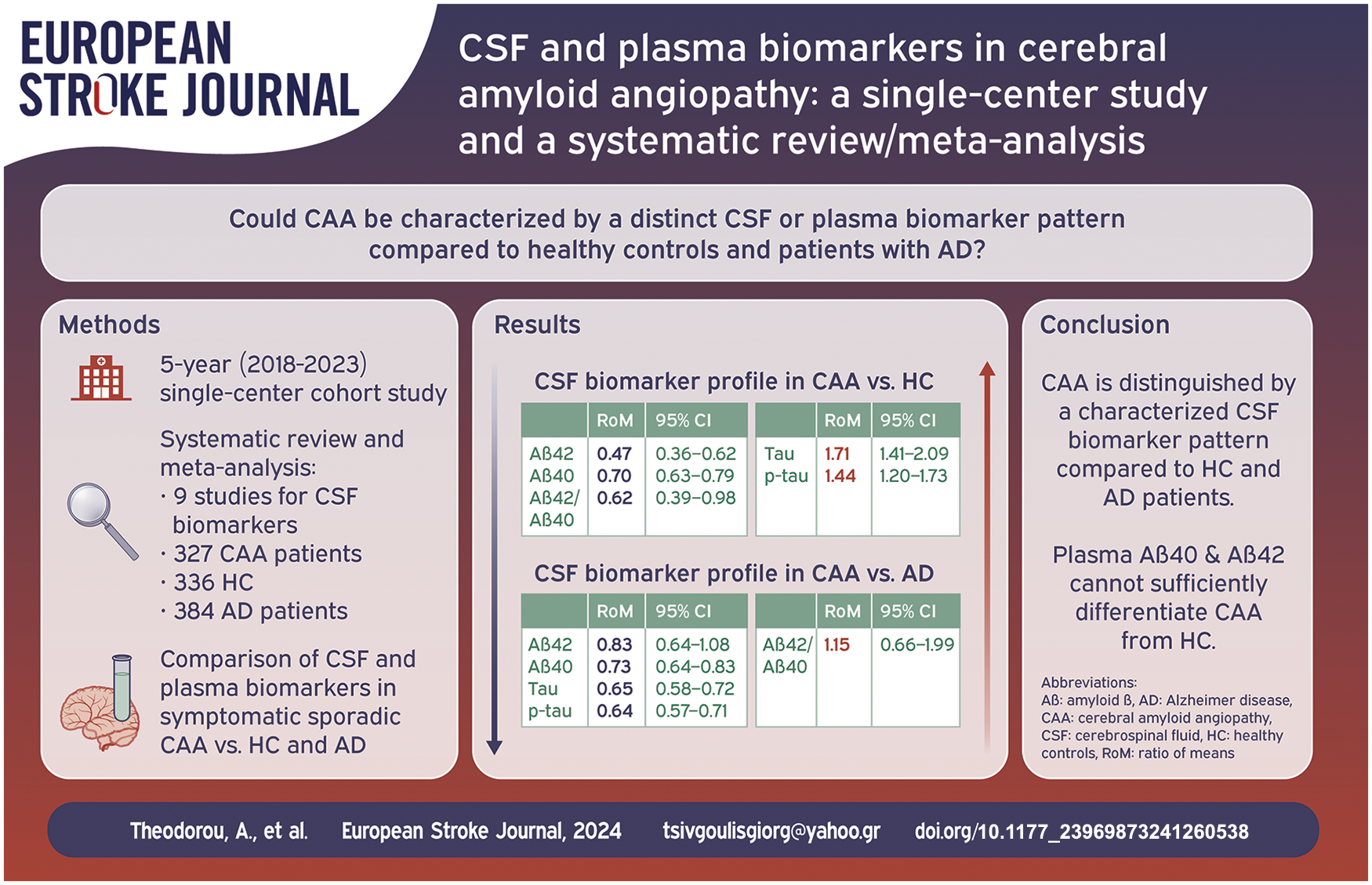
There are limited data regarding cerebrospinal fluid (CSF) and plasma biomarkers among patients with Cerebral Amyloid Angiopathy (CAA). We sought to investigate the levels of four biomarkers [β-amyloids (Aβ42 and Aβ40), total tau (tau) and phosphorylated tau (p-tau)] in CAA patients compared to healthy controls (HC) and patients with Alzheimer Disease (AD).
A systematic review and meta-analysis of published studies, including also a 5 year single-center cohort study, with available data on CSF and plasma biomarkers in symptomatic sporadic CAA versus HC and AD was conducted. Biomarkers’ comparisons were investigated using random-effects models based on the ratio of mean (RoM) biomarker concentrations. RoM < 1 and RoM > 1 indicate lower and higher biomarker concentration in CAA compared to another population, respectively.
We identified nine cohorts, comprising 327 CAA patients (mean age: 71 ± 5 years; women: 45%) versus 336 HC (mean age: 65 ± 5 years; women: 45%) and 384 AD patients (mean age: 68 ± 3 years; women: 53%) with available data on CSF biomarkers. CSF Aβ42 levels [RoM: 0.47; 95% CI: 0.36–0.62;
CAA is characterized by a distinct CSF biomarker pattern compared to HC and AD. CSF Aβ40 levels are lower in CAA compared to HC and AD, while tau and p-tau levels are higher in CAA compared to HC, but lower in comparison to AD patients.
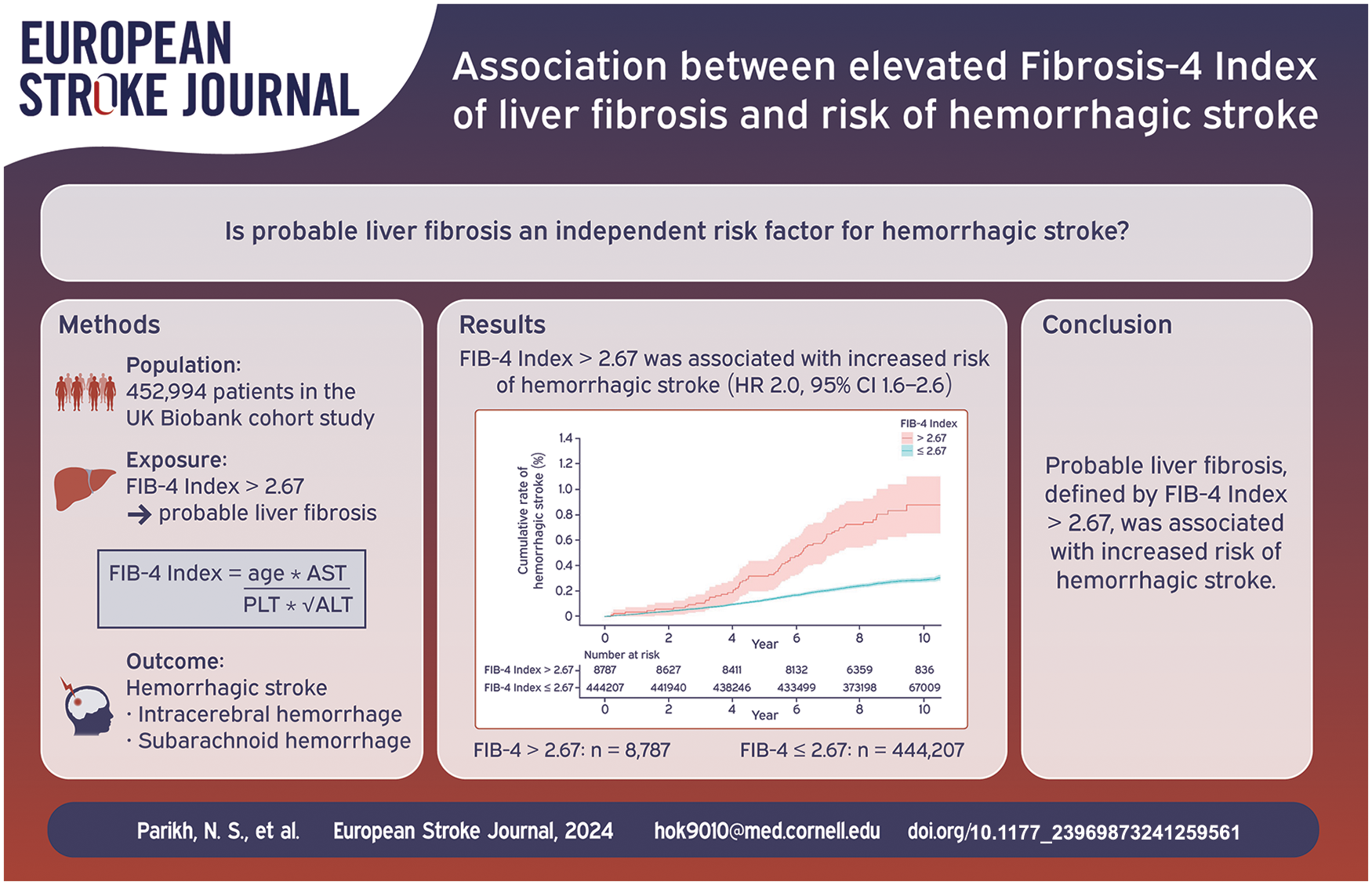
Cirrhosis is associated with an increased risk of hemorrhagic stroke. Liver fibrosis, typically a silent condition, is antecedent to cirrhosis. The objective of this study was to test the hypothesis that elevated Fibrosis-4 (FIB-4) index, indicating a high probability of liver fibrosis, is associated with an increased risk of hemorrhagic stroke.
We performed a cohort analysis of the prospective United Kingdom Biobank cohort study. Participants 40–69 years old were enrolled between 2007 and 2010 and had available follow-up data until March 1, 2018. We excluded participants with prevalent hemorrhagic stroke or thrombocytopenia. High probability of liver fibrosis was defined as having a value >2.67 of the validated FIB-4 index. The primary outcome was hemorrhagic stroke (intracerebral or subarachnoid hemorrhage), defined based on hospitalization and death registry data. Secondary outcomes were intracerebral and subarachnoid hemorrhage, separately. We used Cox proportional hazards models to evaluate the association of FIB-4 index >2.67 with hemorrhagic stroke while adjusting for potential confounders including hypertension, alcohol use, and antithrombotic use.
Among 452,994 participants (mean age, 57 years; 54% women), approximately 2% had FIB-4 index >2.67, and 1241 developed hemorrhagic stroke. In adjusted models, FIB-4 index >2.67 was associated with an increased risk of hemorrhagic stroke (HR, 2.0; 95% CI, 1.6–2.6). Results were similar for intracerebral hemorrhage (HR, 2.0; 95% CI, 1.5–2.7) and subarachnoid hemorrhage (HR, 2.2; 95% CI, 1.5–3.5) individually.
Elevated FIB-4 index was associated with an increased risk of hemorrhagic stroke.