Editorial
Select search scope: search across all journals or within the current journal
Promoting the highest quality, evidence-based research across Europe is a priority of the European Stroke Organisation (ESO). The ESO Guideline Board communicate and promote evidence-based recommendations for clinical practice through their Guidelines. However, there are many aspects of stroke care where robust scientific evidence may be unavailable or difficult to obtain. Thus, there is a need for practical, consensus guidance, produced following robust, consistent, and transparent methods, that is suitable for high-priority clinical scenarios where evidence is currently lacking. The ESO Guideline Board developed methods for producing practical clinical guidance based on expert consensus in response to this need. These ESO’ White Papers’ are intended to complement standard ESO Guidelines. Here, we outline the ESO White Papers’ standard operating procedure (SOP). We will describe the motivation for creating White Papers, the preferred composition of writing groups and expert consensus panellists, the methods for achieving consensus, and how results will be communicated. To ensure that all voting members have an equal voice, our methods are based upon the Delphi process of repeated rounds of anonymous voting, feedback and review. We hope that the White Papers will add further value to the clinical practice guidance that is offered by ESO. We look forward to receiving suggestions for White Paper topics from the stroke community.
National stroke clinical quality registries/audits support improvements in stroke care. In a 2016 systematic review, 28 registries were identified. Since 2016 there have been important advances in stroke care, including the development of thrombectomy services. Therefore, we sought to understand whether registries have evolved with these advances in care. The aim of this systematic review was to identify current, hospital-based national stroke registries/audits and describe variables (processes, outcome), methods, funding and governance).
We searched four databases (21st May 2015 to 1st February 2024), grey literature and stroke organisations’ websites. Initially two reviewers screened each citation; when agreement was satisfactory, one of four reviewers screened each citation. The same process was applied to full texts. If there were no new publications from registries identified in the original 2016 review, we contacted the registry leads. We extracted data using predefined categories on country (including income level), clinical/process variables, methods, funding and governance.
We found 37 registries from 31 countries (28 high income, four upper-middle income, five lower-middle income) of which 16 had been identified in 2016 and 21 were new. Twenty-two of the same variables were collected by >50% of registries/audits (mostly acute care, including thrombectomy, and secondary prevention), compared with only four variables in 2016. Descriptions of funding, management, methods of consent and data privacy, follow-up, feedback to hospitals, linkage to other datasets and alignment of variables with guidelines were variably reported. Reasons for apparent termination of some registries was unclear.
The total number of stroke registries has increased since 2016, and the number of variables collected has increased, reflecting advances in stroke care. However, some registries appeared to have ceased; the reasons are unclear.

Evidence on endovascular therapy (EVT) for symptomatic intracranial stenosis (sICAS) from randomized-controlled clinical trials (RCTs) is conflicting. While prior RCTs on percutaneous transluminal angioplasty and stenting (PTAS) demonstrated harm or no benefit over best medical treatment (BMT), recent data suggest that submaximal balloon angioplasty with BMT may be superior to BMT alone.
A systematic review and meta-analysis of RCTs was conducted to evaluate the safety and efficacy of elective EVT plus BMT compared to BMT alone for sICAS.
Six RCTs (5 on PTAS and 1 on balloon-angioplasty) comprising 1606 patients were included. EVT increased the risk of any stroke or death (RR = 2.68; 95% CI: 1.72–4.19;
EVT is associated with adverse early outcomes, without reducing the risk of long-term stroke recurrence or mortality compared to BMT. Further research is warranted to identify high-risk subgroups who may benefit from EVT for sICAS and refine interventions to minimize periprocedural risks.

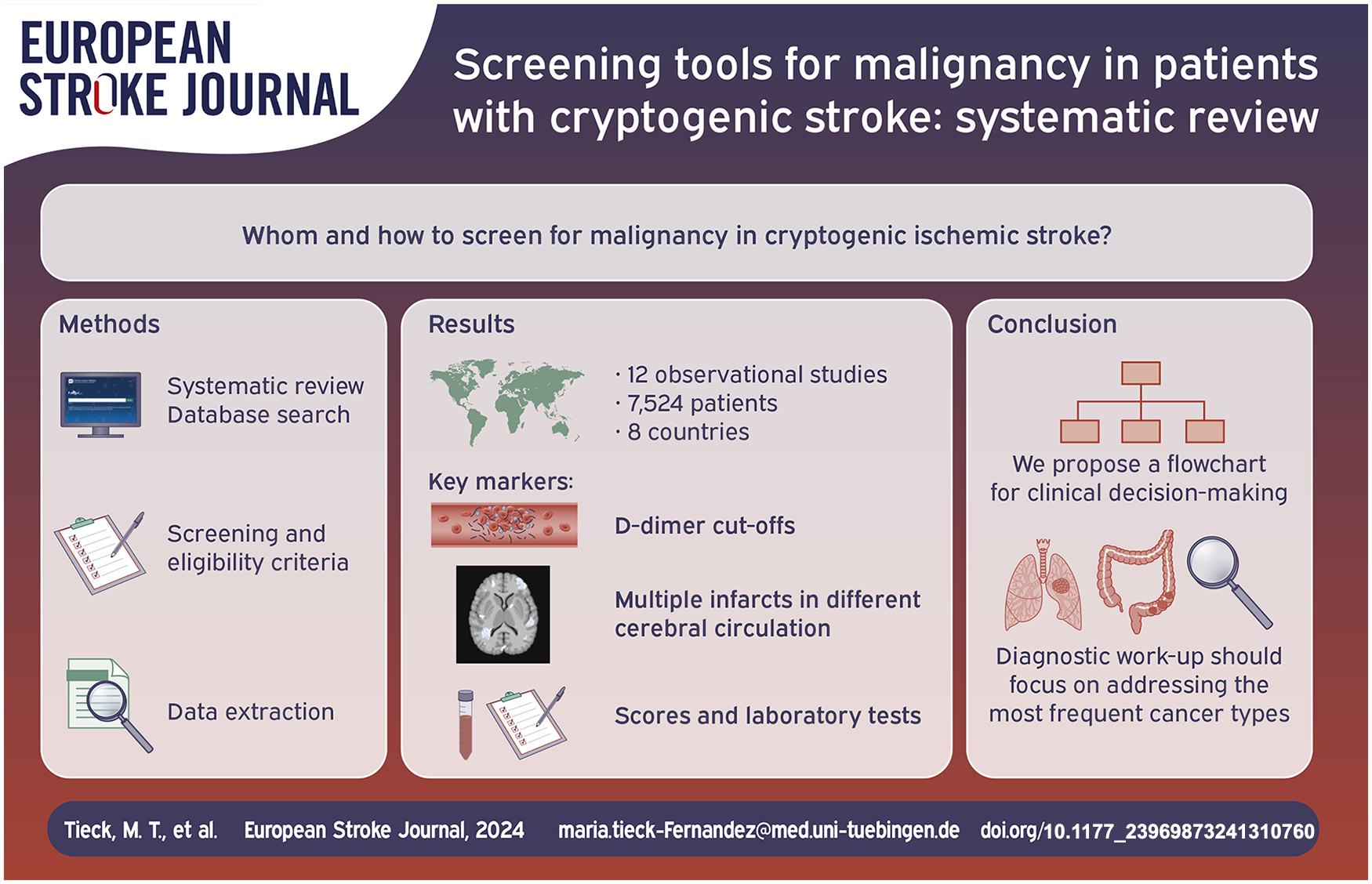
Up to 20% of patients with cryptogenic ischemic stroke have an occult malignancy at the time of stroke presentation, providing an opportunity for early cancer detection. Despite this significant association, there is currently no consensus in international guidelines on how to systematically screen for malignancy in ischemic stroke patients. This review aims to summarize recent evidence on clinical features and scores, and predictive laboratory tests, that can guide malignancy screening in ischemic stroke patients. Our systemic search included PubMed, MEDLINE and Cochrane databases and yielded a total of 12 studies meeting the inclusion criteria for review. Elevated D-dimer levels and multiple infarcts in different cerebral circulations emerged as key markers. Based on the summarized data, we propose a flowchart for clinical decision-making regarding malignancy screening in patients with ischemic stroke. As the initial steps, we recommend using D-dimers cut-offs and stroke pattern on brain imaging to classify patients according to their risk profile. Based on the identified risk, we recommend a subsequent diagnostic workup addressing the most prevalent cancer types, including gastrointestinal tract, lung adenocarcinoma and gender-related cancer. The clinical implications of early malignancy screening and the need for evidence-based guidelines in cryptogenic stroke are discussed.
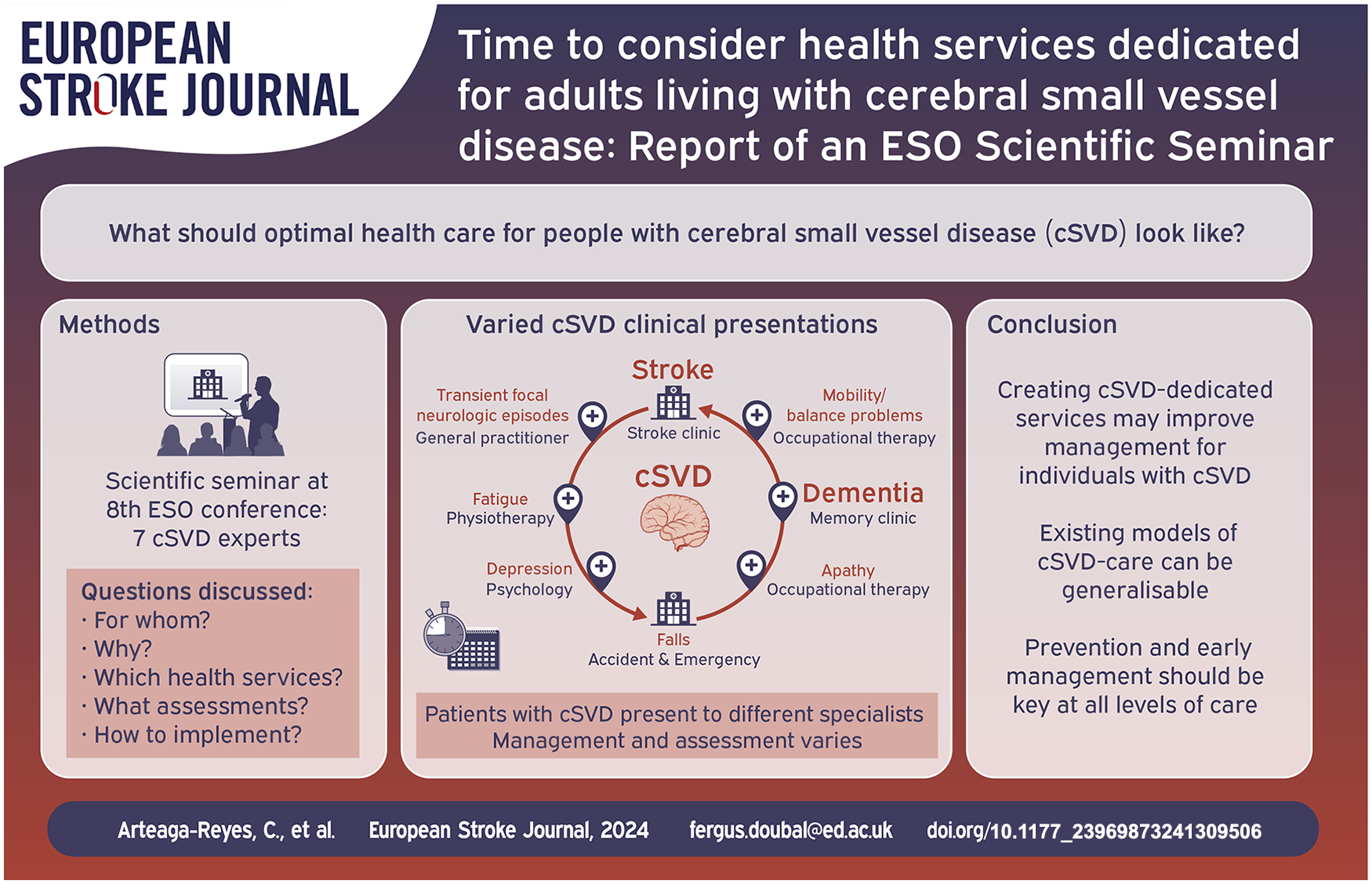
Cerebral small vessel disease (cSVD) is a highly prevalent disorder leading to physical, cognitive and functional decline. We report key barriers in the management of individuals with cSVD, the potential benefit of cSVD-dedicated health services, and evidence from existing models of care for adults with cSVD.
We examined information from a scientific seminar developed between seven experts in cSVD during the eighth European Stroke Organisation Conference that discussed the optimal health care for adults with cSVD and what health services dedicated to cSVD should include.
Barriers in cSVD care include unrecognised symptoms and modifiable risk factors, heterogeneity of clinical presentations, inefficient inter/intra-clinical services communication/organisation, and uncertainties regarding what assessments/treatments should be routinely done, when and by whom. However, existing health services and research studies suggest models of care in cSVD. Multi-step approaches can be used for identification and aetiological workup in individuals with cSVD, including basic and selected advanced evaluations, for example, monogenic cSVD testing. Although current guidelines for management of cSVD illlustrate limitations, there are recommendations on risk factors and lifestyle considerations, as well as pharmacological and non-pharmacological interventions for people with cSVD.
Existing healthcare models do not provide optimal care for individuals with cSVD. Lack of awareness of heterogeneous clinical presentations and uncertainty in threshold of cSVD ‘burden’ for referral to specialist multidisciplinary services, are key challenges for health services to overcome. Creating cSVD-dedicated services may prevent underdiagnosing and achieve standardised holistic management to improve outcomes in people with cSVD. However, adequate prevention and early management should be offered at all levels of care.
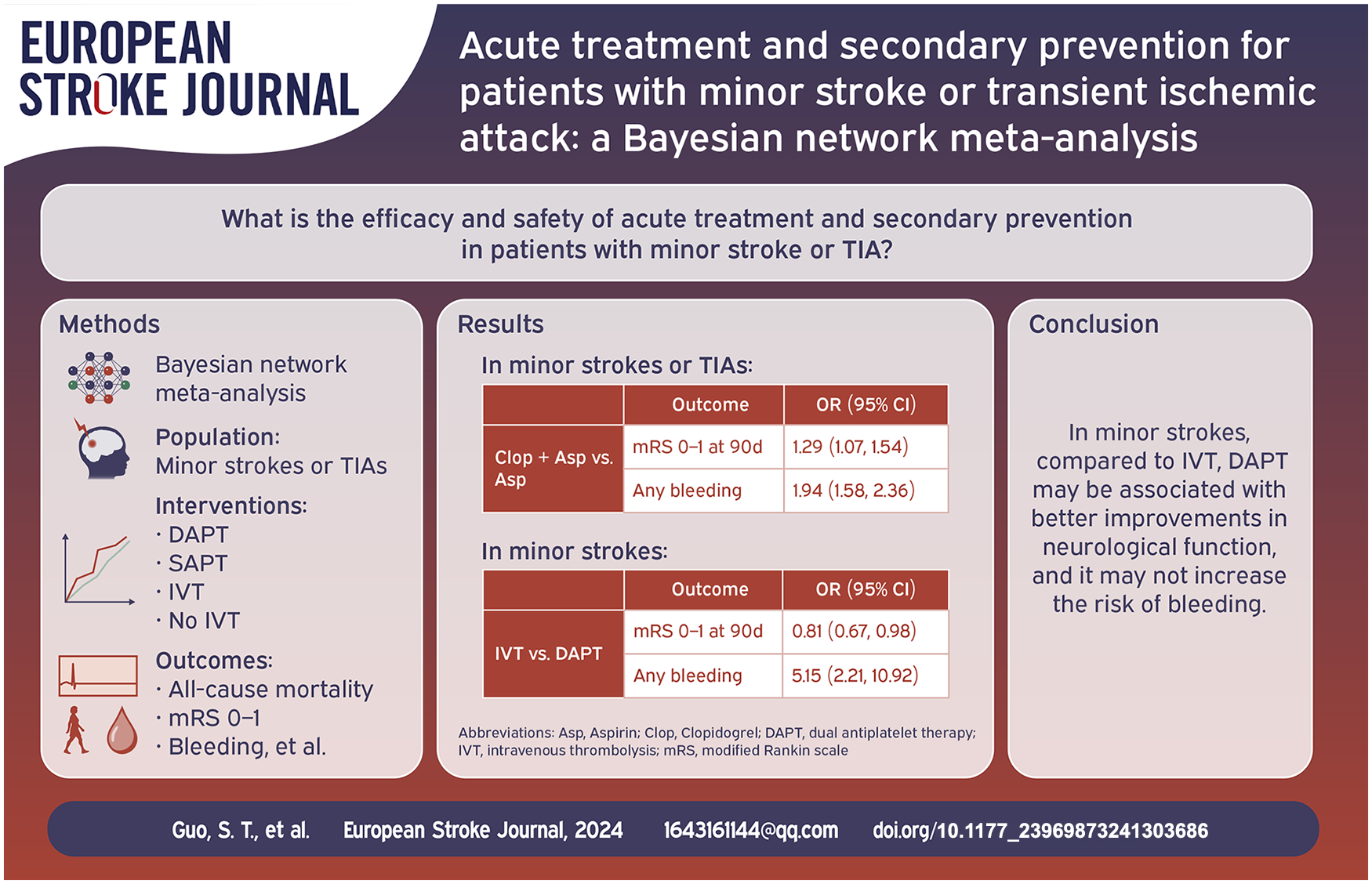
The efficacy of different antiplatelet treatment in minor strokes (MSs) or transient ischemic attacks (TIAs) and that of antiplatelet and intravenous thrombolysis (IVT) in MSs remain controversial.
We searched PubMed, Embase, Web of Science and the Cochrane Library to identify all eligible articles until April 12, 2024. Efficacy outcomes were all-cause mortality, excellent outcome, functional independence and recurrent stroke. Safety outcomes were any types of bleeding and intracerebral hemorrhage (ICH). The associations were calculated for the overall data by using odds ratios (ORs).
Twenty three high-quality studies with 10 RCTs and 13 non-RCTs were included, involving 47,135 patients with MSs or TIAs. In MSs or TIAs, dual antiplatelet therapies (DAPTs) significantly improved the modified Rankin Scale (mRS) scores for patients with recurrent stroke, major vascular events and ischemic stroke although it was associated with an increased risk of ICH and bleeding when compared to aspirin. In MSs, compared to IVT, DAPT had a significant advantage in improving the mRMS scores and SAPT and DAPT significantly reduced the risk of any bleeding or sICH. IVT significantly reduced all-cause mortality, although it also increased the risk of sICH and ICH compared to no IVT.
In MSs or TIAs, compared to aspirin, DAPTs can effectively prevent the recurrence of post-stroke neurological dysfunction and ischemic events, but it may increase the risk of ICH together with moderate or severe bleeding. Dipyridamole + aspirin resulted in the lowest risk of bleeding. In MSs, compared to IVT, DAPT may be associated with better improvements in neurological function, and it may not increase the risk of bleeding.
Evidence regarding the benefit of endovascular therapy (EVT) in patients with acute ischemic stroke (AIS) due to isolated cervical internal carotid artery occlusion (c-ICA-O) is lacking. We assessed the outcomes and safety of EVT in patients with isolated c-ICA-O.
Retrospective multicenter cohort study of patients with an AIS due to isolated c-ICA-O, within 24-h since last-seen-well. Comparisons were made between EVT and best medical therapy (BMT). The primary outcome was 3-months modified Rankin Scale (mRS) ordinal shift. Secondary outcomes included 3-month favorable outcome (mRS 0–2, or return to pre-stroke mRS), symptomatic intracranial hemorrhage (sICH) and any parenchymal hemorrhage. Outcomes were compared combining inverse probability of treatment weighting with regression models and propensity score matching (PSM) as sensitivity analysis.
We analyzed 998 patients (66.2% male, mean age 71.1 ± 13.2 years). 487 (48.8%) patients received EVT and 511 (51.2%) received BMT. Patients receiving EVT had a higher admission NIHSS [13 (7–18) vs 5 (2–13)] compared to BMT. There was no difference between EVT and BMT groups in 3-month mRS shift (adjusted common odds ratio [OR], 1.01 [95% CI 0.76–1.34]) and favorable outcome (adjusted OR [aOR] 1.16 [95% CI 0.84–1.60]). No patient (0%) in the BMT group had sICH versus 1.6% in the EVT group. Parenchymal hemorrhage was numerically higher in EVT patients (2.7% vs 0.6%; aOR 3.85 [95% CI 0.98–15.23]). PSM analysis revealed similar results.
In patients with isolated c-ICA-O, EVT was associated with similar odds of disability and intracranial bleeding compared to BMT. Randomized-controlled clinical trials in patients with isolated c-ICA-O are warranted.

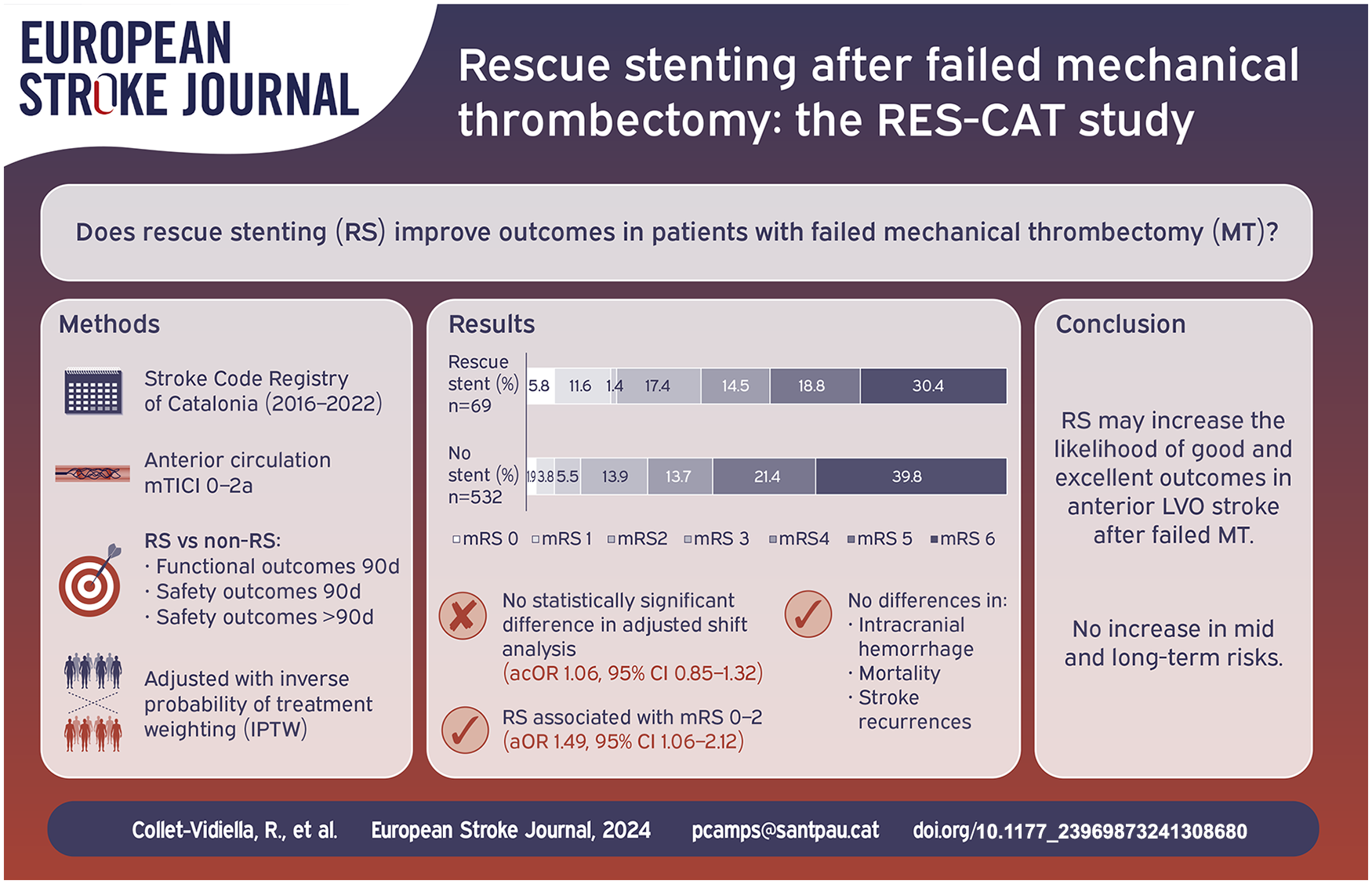
The efficacy of intracranial rescue stenting (RS) following failed mechanical thrombectomy (MT) in large-vessel occlusion (LVO) stroke remains uncertain. We aimed to evaluate clinical outcomes of RS in patients with anterior circulation LVO stroke following unsuccessful MT.
We conducted a retrospective analysis using the Stroke Code Registry of Catalonia (January 2016–March 2022), a prospective, population-based registry including patients treated at 10 comprehensive stroke centers. We compared outcomes between patients who received RS and those who did not after failed MT. The primary outcome was the shift in 90-day functional status, assessed by the modified Rankin Scale (mRS), adjusted for confounders using inverse probability of treatment weighting (IPTW). Secondary outcomes included good (mRS ⩽ 2 or 3 if baseline mRS was 3) and excellent (mRS ⩽ 1) outcomes, ischemic recurrences, hemorrhagic transformation, and 90-day mortality.
Of 601 patients, 69 underwent RS. RS did not significantly impact the 90-day mRS shift (adjusted common odds ratio [acOR] 1.06, [95% CI 0.85–1.32];
RS may increase the likelihood of good and excellent outcomes in anterior LVO stroke after failed MT, without increasing long-term risks. Further randomized trials are warranted for comprehensive validation.
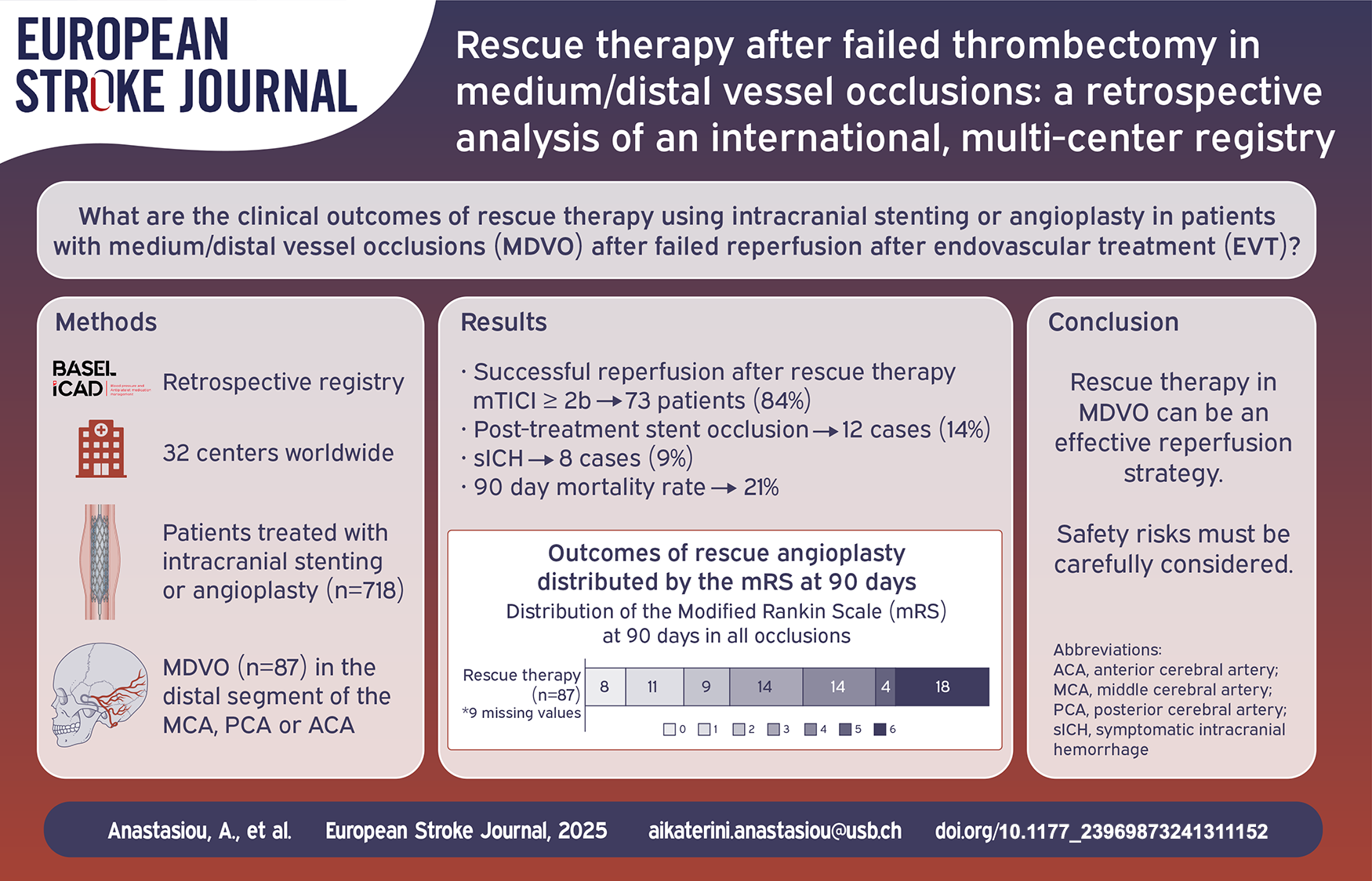
There are limited therapeutic options in cases of failed reperfusion (modified thrombolysis in cerebral infarction [mTICI] score < 2b) after stent-retriever and/or aspiration based endovascular treatment (EVT) for acute ischemic stroke. Despite the absence of data supporting its use, rescue therapy (balloon angioplasty and/or stent implantation) is often utilized in such cases. Studies are limited to large vessel occlusions, while the outcomes and complications after rescue therapy in medium/distal vessel occlusions (MDVOs) have not been reported. This study aims to report the outcomes of rescue therapy in MDVO stroke patients.
We performed an analysis of the “Blood pressure and Antiplatelet medication management after reScue angioplasty after failed Endovascular treatment in Large and distal vessel occlusions with probable IntraCranial Atherosclerotic Disease” (BASEL ICAD) retrospective registry. All MDVO stroke patients were included in the analysis.
Out of the 718 registry patients, 87 (12.1%) presented with an MDVO. Fifty-six patients (64.4%) showed an occlusion of the M2 segment of the middle cerebral artery. Rescue stenting was performed in 78 patients (89.7%) while balloon angioplasty alone was performed in 9 patients (10.3%). Successful reperfusion (mTICI score ⩾ 2b) was achieved in 73 (83.9%) patients after rescue therapy. Symptomatic intracranial hemorrhage (sICH) occurred in 8 patients (9.2%) and post-treatment stent occlusion in 12 patients (13.8%). Ninety days mortality was 20.7%. Twenty-eight patients (32.2%) achieved functional independence at 90 days (modified Rankin Scale 0–2).
Rescue therapy with stenting and/or balloon angioplasty in patients undergoing EVT for isolated MDVO with suspected underlying intracranial atherosclerotic disease is an effective reperfusion strategy but is associated with complications and poor functional outcomes.
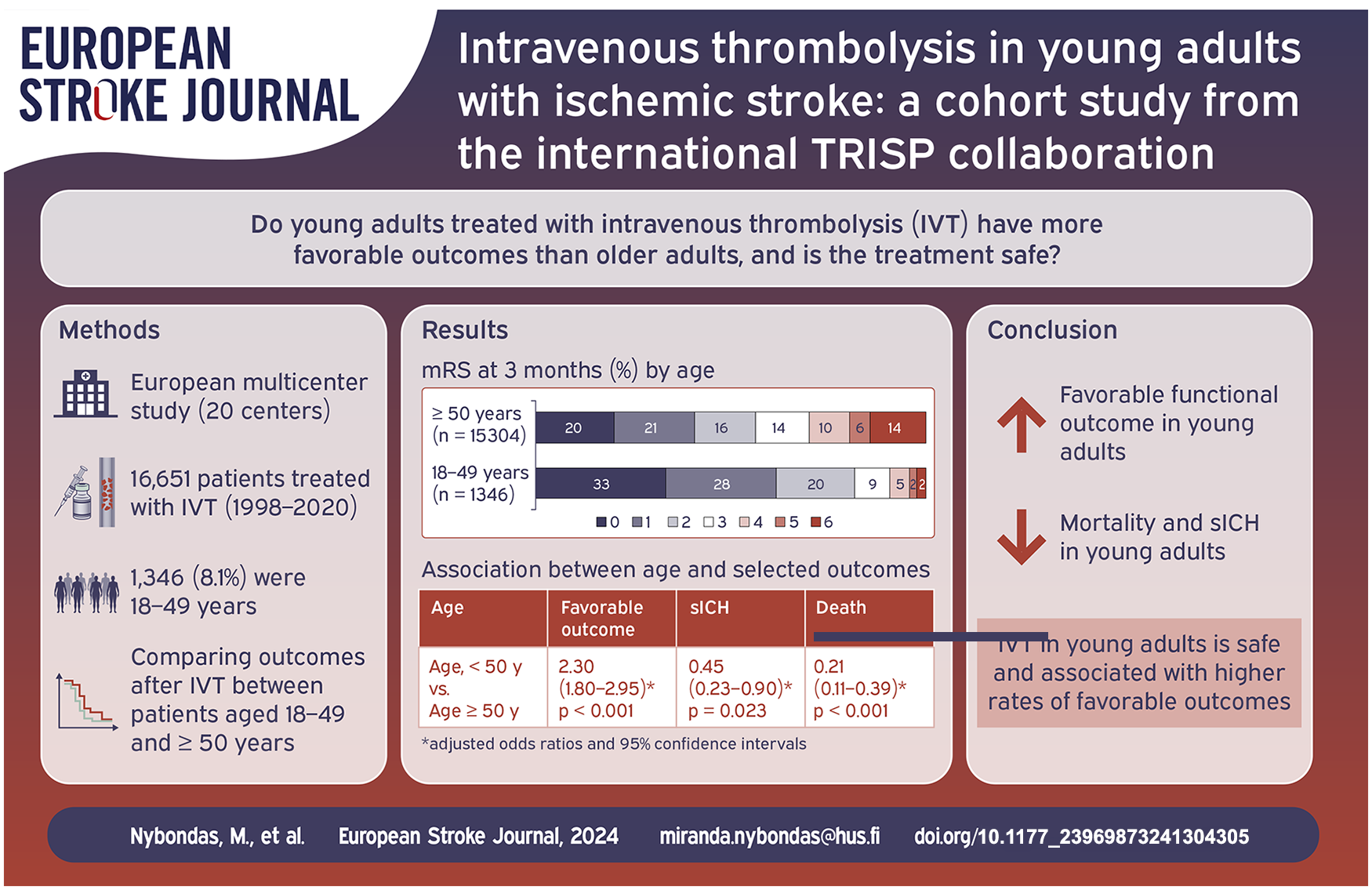
Previous observational data indicate that young adults treated with intravenous thrombolysis (IVT) for acute ischemic stroke have more favorable outcomes and less complications when compared to older adults. Given the limited data on this topic, we aimed to provide more evidence on clinical outcomes and safety in such patients, using a large international thrombolysis registry.
In this prospective multicenter study, we used data from the Thrombolysis in Ischemic Stroke Patients (TRISP) registry from 1998 to 2020. Patients who received endovascular treatment (EVT), as only treatment or in addition to IVT, were not included in this cohort. Using multivariable regression models, we compared thrombolysed young patients aged 18–49 years with those aged ⩾50 years with regards to the following outcomes: favorable outcome in stroke survivors (modified Rankin Scale ⩽2), symptomatic intracranial hemorrhage (sICH) according to European Cooperative Acute Stroke Study II (ECASS II) criteria, and three-months all-cause death.
Of the 16,651 IVT treated patients, 1346 (8.1%) were 18–49 years. Young adults in TRISP were more often male (59.6% vs 54.0%), had a lower median NIHSS score on admission, 7 (4–13) versus 8 (5–15), and had less cardiovascular risk factors except for smoking (42.0% vs 19.0%) when compared to older patients. When compared to thrombolysed patients aged ⩾50 years, a favorable functional outcome was more likely in young adults: 81.9% versus 56.4%, aOR 2.30 (1.80–2.95), whilst sICH 1.6% versus 4.6%, aOR 0.45 (0.23–0.90) and death 2.3% versus 14.2%, aOR 0.21 (0.11–0.39) were less likely.
Intravenous thrombolysis in young adults is independently associated with higher rates of favorable outcomes and lower rates of complications.
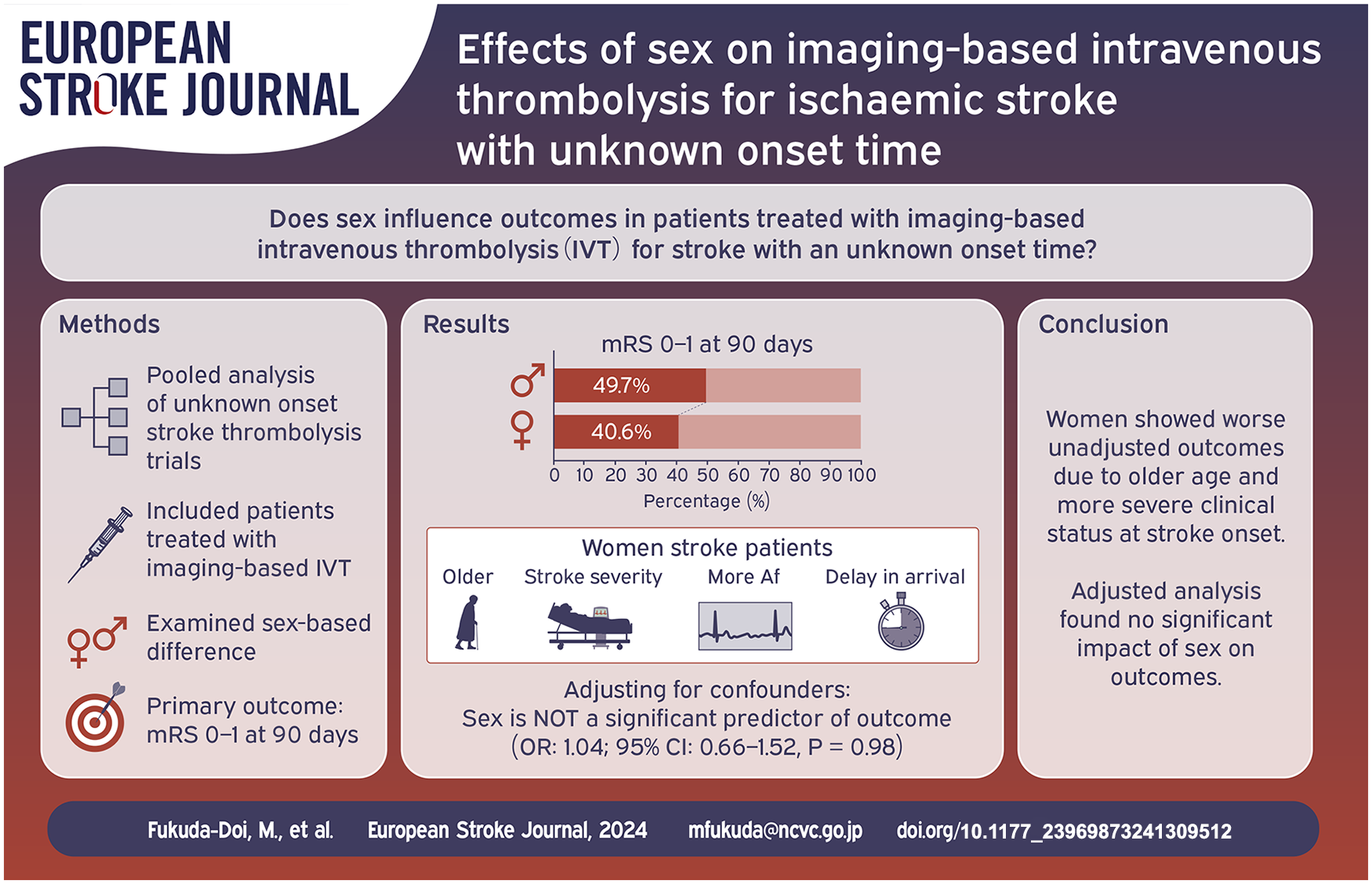
The effects of imaging-based intravenous thrombolysis on outcomes based on patient sex remain unclear. We aimed to investigate whether outcomes among patients with stroke with an unknown onset time and treated with imaging-based intravenous thrombolysis are influenced by their sex.
This study was a pooled analysis of individual patient-level data acquired from the Evaluation of unknown Onset Stroke thrombolysis trials. Patients treated with imaging-based intravenous thrombolysis for stroke with an unknown onset time were included. The primary outcome was a favourable outcome (modified Rankin Scale score 0–1) at 90 days. The sex-based difference in outcomes was studied using mixed-effect logistic or ordinal regression models, considering potential heterogeneity across trials.
Out of 509 patients in total, 204 (40.1%) were women. Compared with men, women were older and more likely to have atrial fibrillation. Baseline National Institutes of Health Stroke Scale score was higher and hours from last-known-well to treatment were longer for women than for men. Favourable outcomes occurred less often among women than among men. However, multivariate adjustment revealed a non-significant association between female sex and favourable outcome (adjusted odds ratio: 1.04 [95% confidence interval: 0.66–1.52],
Pooled data from the included clinical trials showed that women with ischaemic stroke with an unknown onset time had worse functional outcomes following imaging-based intravenous thrombolysis than did men. However, this sex-based difference can be explained by the higher age and more severe clinical status at onset among women.
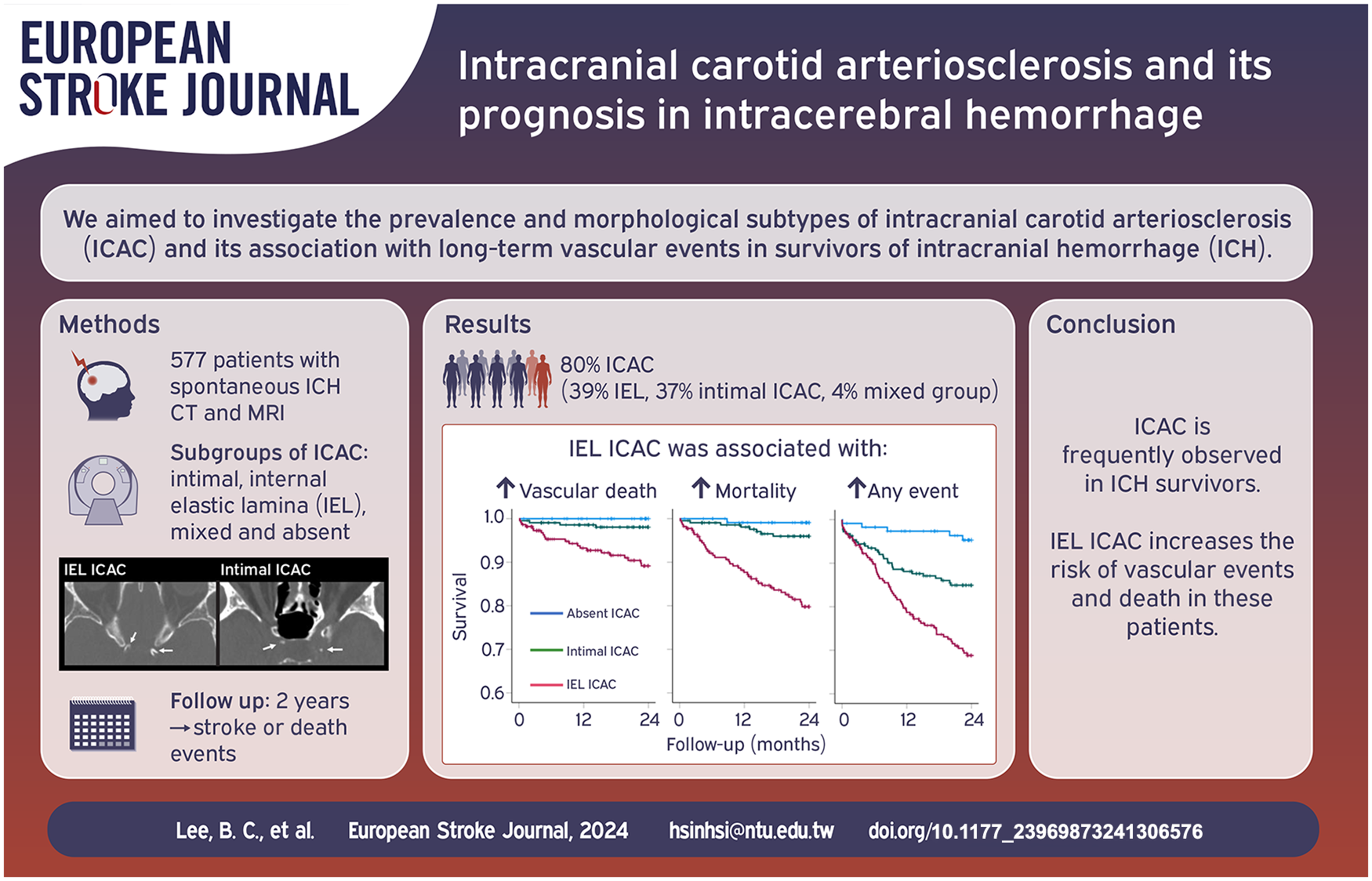
Intracerebral hemorrhage (ICH) is a manifestations of sporadic cerebral small vessel disease, and the survivors are predisposed to higher long-term risks of vascular events. Intracranial carotid artery calcification (ICAC), a potential marker for arteriosclerosis, is a risk factor for stroke but their roles in ICH is unknown. We aimed to investigate the prevalence and morphological subtypes of ICAC and their associations with long-term vascular events in ICH survivors.
Survivors of spontaneous ICH treated at a single center in Taiwan were included. ICAC was assessed by non-contrast CT; morphology was evaluated and categorized as intimal, internal elastic lamina (IEL), or mixed subtype. Patients were followed up for two years. Associations between calcification subtypes and follow-up events (stroke, cardiovascular event, death) were explored using multivariable Cox regression models.
Overall, 462 (80.1%) survivors of ICH had ICAC—223 (38.6%) were categorized as IEL calcification, 216 (37.4%) as intimal calcification, and 23 (4.0%) as mixed type calcification—and 115 patients (19.9%) had no calcification. Patients with IEL calcification were older than patients with intimal or no calcification (
ICAC is common among ICH survivors and the subtype of IEL calcification may potentially have prognostic value for long-term vascular events.
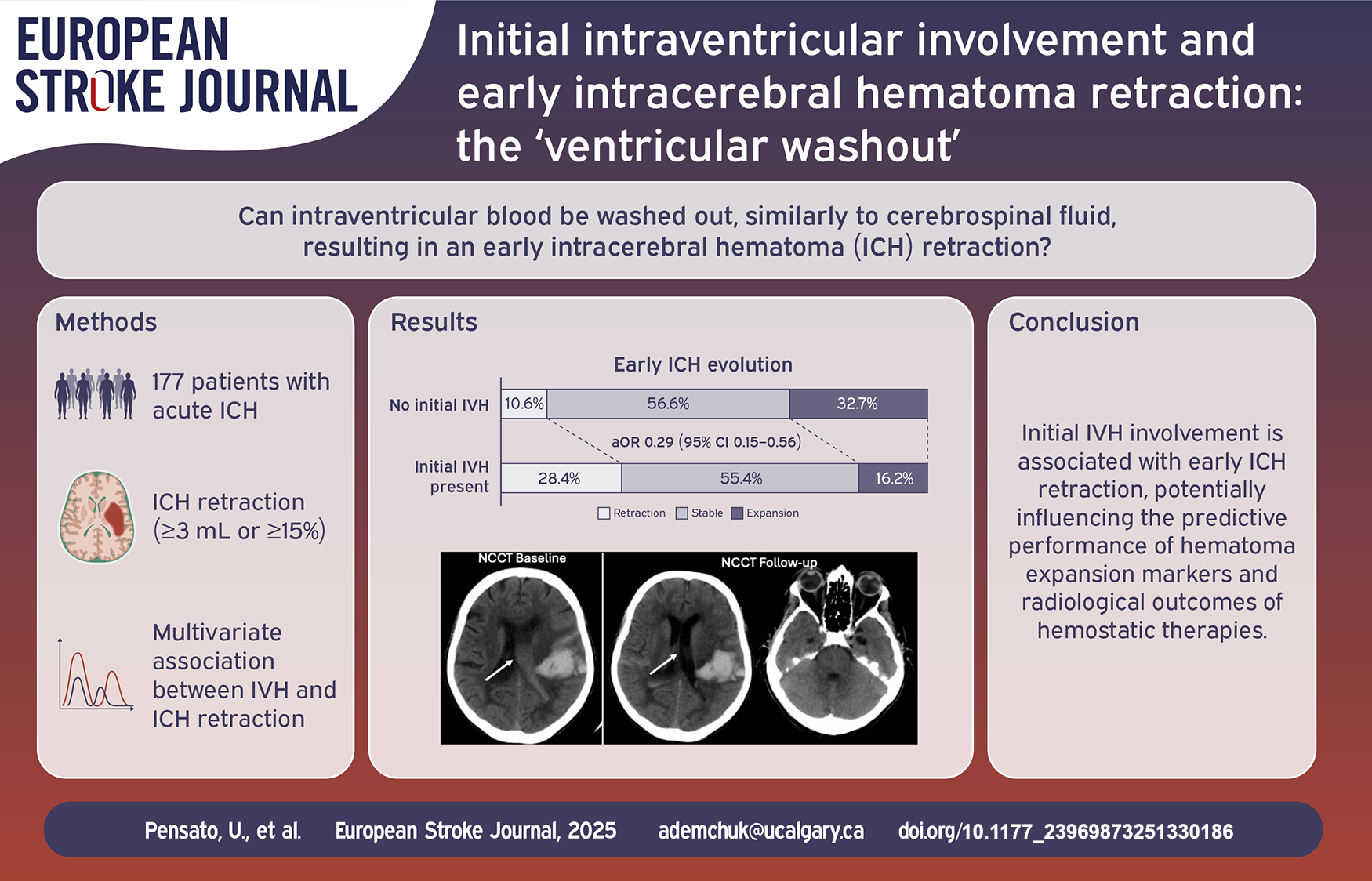
Intraventricular hematoma (IVH) occurs in approximately 40% of acute intracerebral hemorrhage (ICH) patients and is significantly associated with worse clinical outcomes. According to cerebrospinal fluid dynamics, some blood within the ventricles may circulate through the subarachnoid spaces, leading to its apparent “disappearance” on follow-up imaging. We aim to investigate the association between initial IVH involvement and significant early ICH retraction at follow-up imaging.
Data are from the MCAHP (Multiphase CT Angiography Hematoma Prediction) Study, which included consecutive patients with acute ICH investigated with multimodal CT imaging. Patients who underwent surgery before follow-up imaging were excluded. IVH severity was assessed using the IVH score. The primary outcome was significant early ICH retraction, defined as volume decrease (⩾3 ml or ⩾15%) between the initial and follow-up scans. Secondary outcomes included early absolute and relative ICH decrease. Associations between outcomes and initial IVH involvement or IVH score were assessed with logistic regression adjusted for age, baseline NIHSS, initial ICH volume, and onset-to-CT time.
Overall, 177 ICH patients were included. The median age was 71 years (IQR = 59–80), 71 (40.1%) patients were female, and 64 (36.2%) presented with initial IVH involvement. Patients with initial IVH, compared to those without, had a larger initial ICH volume (28.5 ml [IQR = 12.7–52.5] vs. 18.9 ml [IQR = 8.1–30.6],
Initial IVH involvement is associated with early ICH retraction – “intraventricular washout.” This might result in an underestimation of hematoma expansion occurrence and severity in these patients, with potential implications when evaluating the predictive performance of hematoma expansion markers/scores and the radiological efficacy of hemostatic treatments.
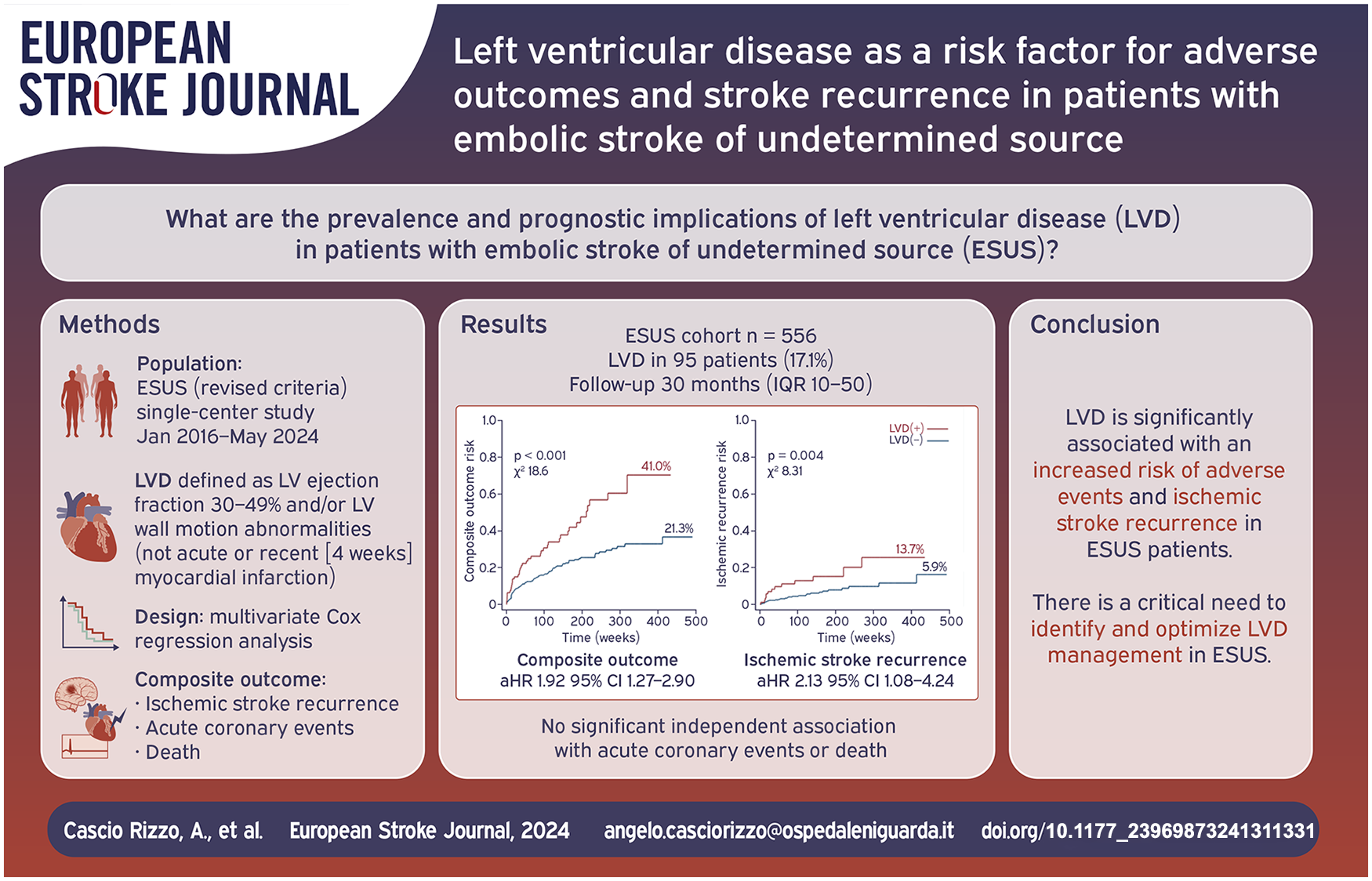
Severe left ventricular (LV) systolic dysfunction (ejection fraction [EF] < 30%) is a known cardiovascular risk factor and a major cause of cardioembolism. However, less severe forms of LV disease (LVD), such as mild-to-moderate LV dysfunction and LV wall motion abnormalities (LVWMAs), are considered potential minor cardiac sources in Embolic Stroke of Undetermined Source (ESUS), but their role is underexplored. This study aims to evaluate the prevalence of LVD in ESUS and its association with adverse vascular events and mortality.
Retrospective, single-center study including consecutive ESUS patients admitted from January 2016 to May 2024. LVD was defined as either global systolic dysfunction (LV ejection fraction 30%–49%) or regional LVWMAs, unrelated to acute or recent (within 4 weeks) myocardial infarction. Univariate and multivariate Cox regression analyses evaluated the association of LVD with a primary composite outcome (including ischemic stroke recurrence, acute coronary events, and all-cause mortality), and its components separately.
Among the 556 ESUS patients (median age 71 years [IQR 60–80], 44.6% female), 95 (17.1%) had LVD, including 51 (53.7%) with reduced LVEF (30%–49%), and 81 (85.3%) presenting LVWMAs. During follow-up (median 30 months), LVD(+) patients had significantly higher rates of the composite outcome (41.0% vs 21.3%,
LVD is significantly associated with an increased risk of ischemic stroke recurrence and adverse outcomes in ESUS patients. These findings highlight the clinical importance of identifying and optimizing LVD management among ESUS to improve long-term outcomes in this population.
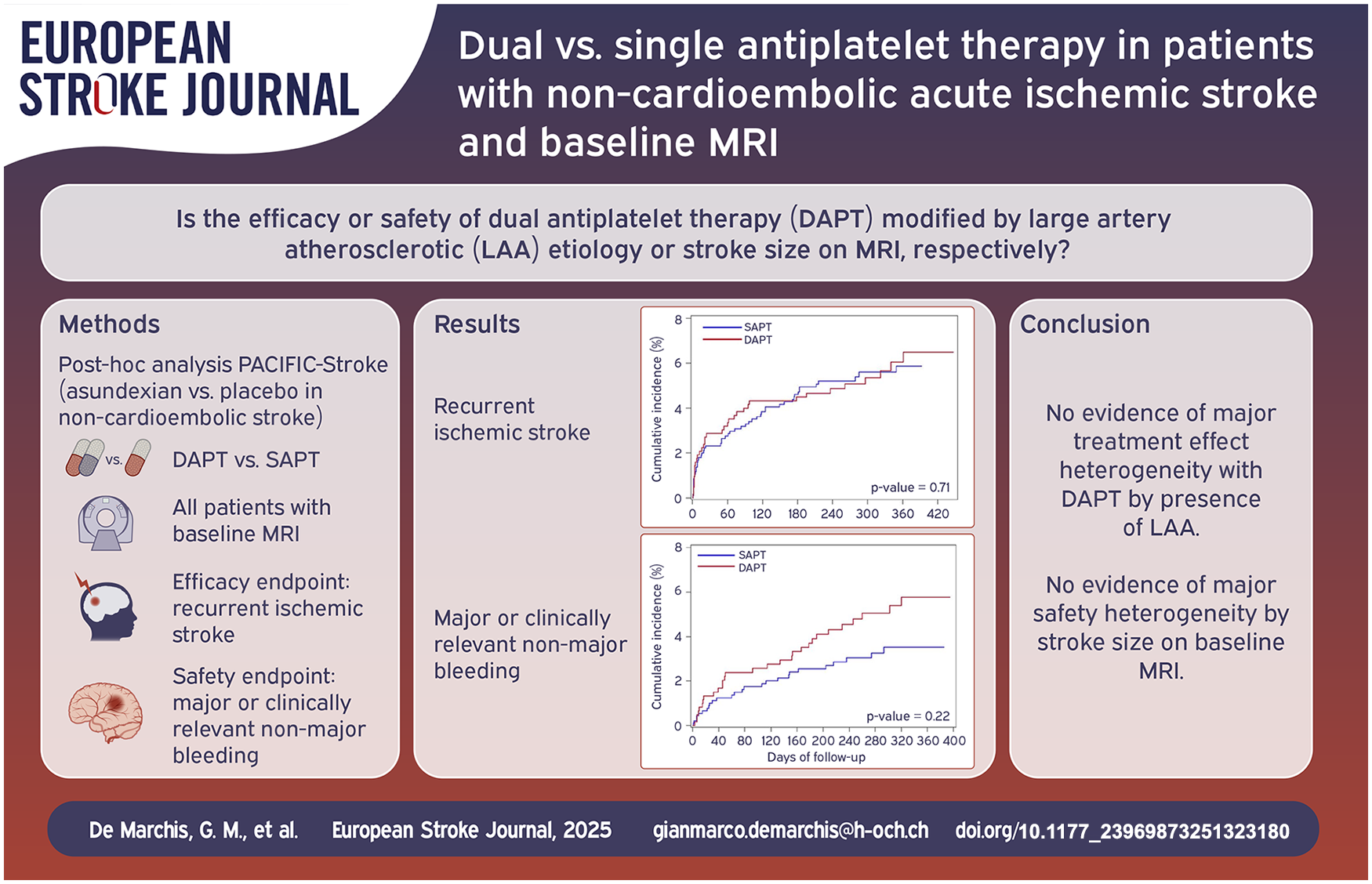
Dual antiplatelet therapy (DAPT) is superior to single antiplatelet therapy (SAPT) for secondary prevention after minor, non-cardioembolic stroke. We aimed to assess whether DAPT efficacy is modified by large artery atherosclerotic (LAA) etiology, and DAPT safety by stroke size on MRI.
Post hoc analysis of the Phase 2 PACIFIC-STROKE randomized clinical trial, which enrolled patients with non-cardioembolic stroke, all with baseline MRI and compared the Factor XIa inhibitor asundexian with placebo on a background of DAPT or SAPT. We compared patients treated with DAPT versus SAPT. The efficacy endpoint was the rate of recurrent ischemic stroke, the safety endpoint was major or clinically relevant non-major bleeding during follow-up.
1590 patients were included, median NIHSS was 2 (interquartile range [IQR] 1–4), 40% received DAPT. Median follow-up was 11.5 months. The efficacy endpoint occurred in 4.4% and 4.8% in the DAPT group and SAPT group, respectively, with the strongest numerical benefit of DAPT over SAPT among patients with NIHSS ⩽ 3 not treated by intravenous thrombolysis. LAA index stroke etiology did not modify DAPT treatment effect. The safety endpoint occurred more often in the DAPT than in the SAPT group (4.6% vs 2.7%), with the numerically lowest risk among patients with NIHSS ⩽ 3 not treated by intravenous thrombolysis. Stroke size did not modify the effect of DAPT on the safety endpoint.
We found no evidence of major treatment effect heterogeneity with DAPT compared with SAPT in patients with and without LAA or by stroke size on MR-DWI.
The efficacy and safety of statins for secondary prevention in patients who have experienced a cardioembolic stroke are not well-defined. However, previous observational data reported hyperlipidemia as a risk factor for both ischemic and bleeding complications in patients with AF and previous stroke. Based on these premises, we conducted a sub-analysis of the RAF and RAF-NOAC studies to evaluate the efficacy and safety of statins in secondary prevention in patients with acute ischemic stroke and AF.
We combined patient data from the RAF and RAF-NOAC studies, prospective observational studies conducted across Stroke Units in Europe, the United States, and Asia from January 2012 to June 2016. We included consecutive patients with AF who suffered an acute ischemic stroke with a follow-up of 90 days. Our outcomes were the combined endpoint, including stroke, transient ischemic attack, systemic embolism, symptomatic intracerebral hemorrhage, and major extracranial bleeding. Furthermore, both ischemic and hemorrhagic outcomes were evaluated separately.
A total of 1742 patients were included (46% male), and 898 (52%) received statins after the index event, of whom 436 (48.6%) were already taking statins before the index event, 462 (51.4%) started treatment after. At multivariable analysis, statin use was statistically associated with age (OR 0.92, 95% CI 0.97–0.99,
Statins protect cerebral arterial vessels (particularly small vessels) from subacute damage due to hypertension, diabetes, and other harmful agents (such as reactive oxygen species, proinflammatory cytokines, etc.) due to their systemic anti-inflammatory and endothelium-protective effects.
Our data show that statins seem to protect against global bleeding events in cardioembolic stroke patients; this may be due to the pleiotropic effect of statins. More data are warranted to confirm these findings.

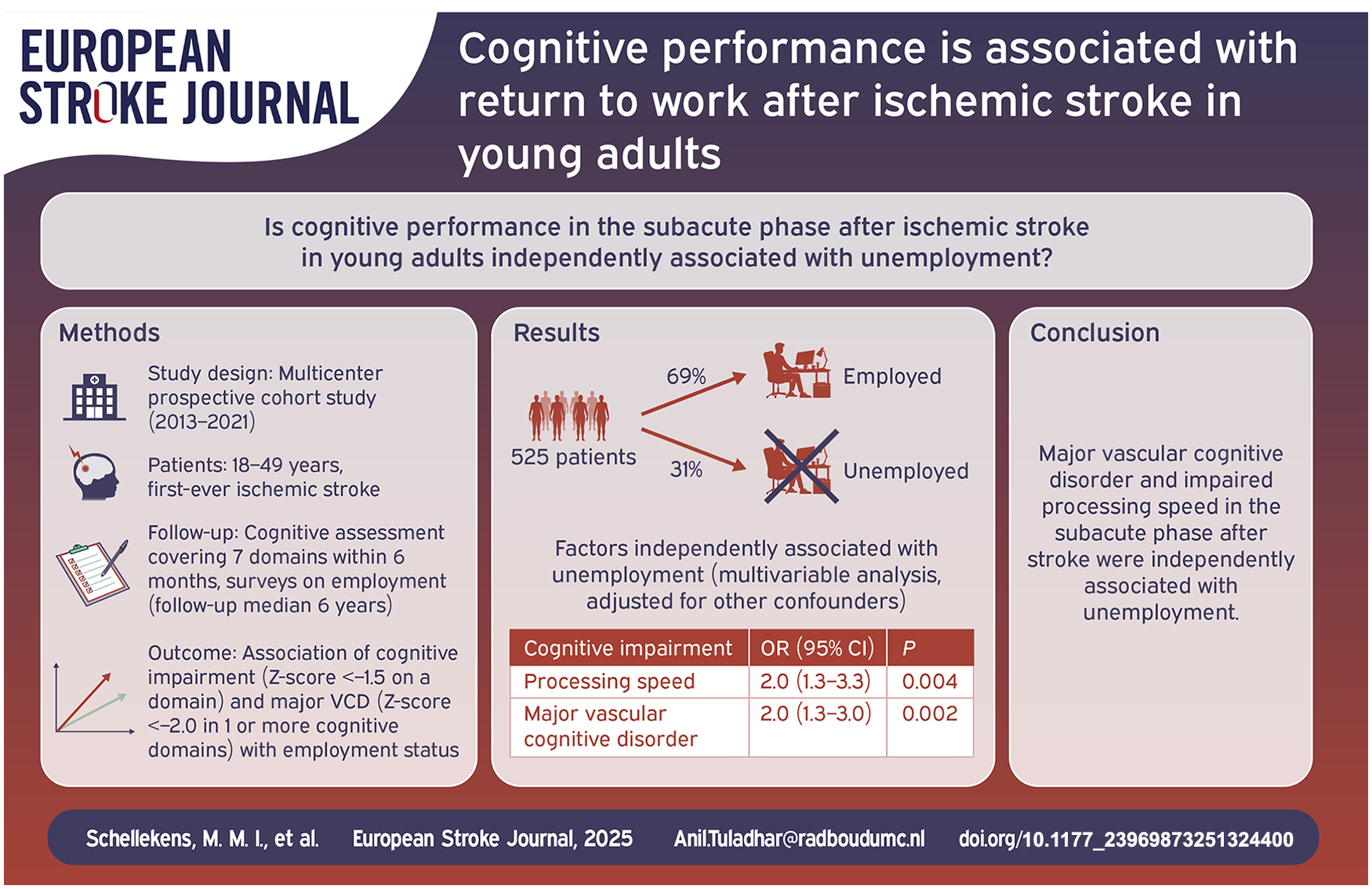
Limited data exist on cognitive performance and return to work after ischemic stroke, especially in patients under 50 years. We investigated whether cognitive performance in the subacute phase after ischemic stroke in young adults was associated with unemployment and the inability to retain their jobs among those who returned to work.
We conducted a multicenter prospective cohort study between 2013 and 2021, enrolling patients aged 18–49 years with first-ever ischemic stroke. Cognitive assessments were performed within 6 months following the index event, covering seven cognitive domains. We categorized patients with cognitive impairment (
Of 525 patients (median age 44.3 [IQR 38.0–47.4] years; 243 women [46.3%]); median follow-up of 6.6 [IQR 4.5–8.2] years), 426 patients (81.1%) returned to work. Sixty-five patients (15.3%) were unable to maintain employment. In multivariable logistic regression analysis, major VCD (OR = 2.0; 95% CI 1.3–3.0;
In young patients after a first-ever ischemic stroke, major VCD and impaired processing speed in the subacute phase after stroke were independently associated with unemployment, but not with the inability to maintain employment.
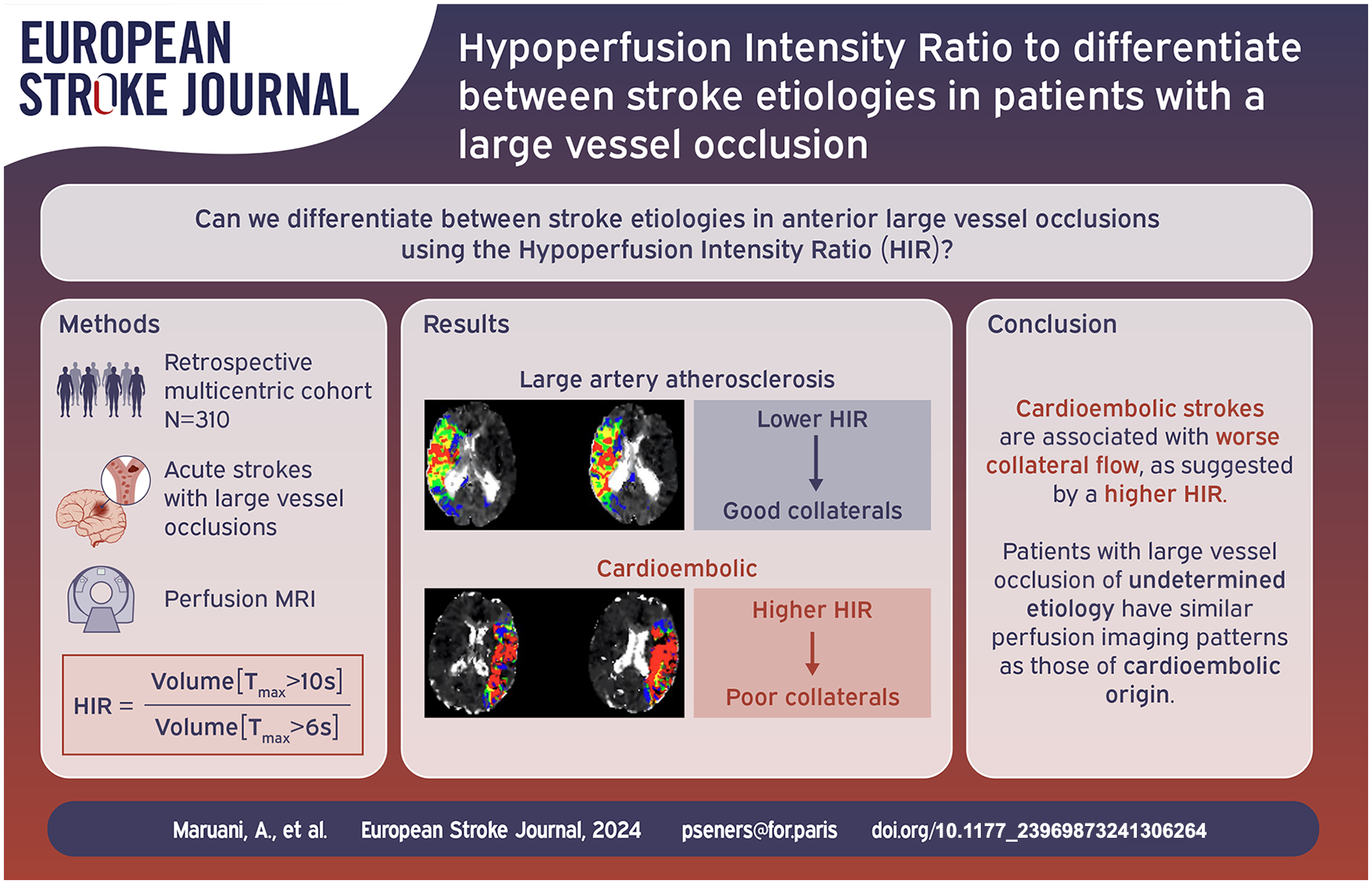
Collateral circulation plays a key role in acute ischemic stroke. We sought to determine the association between the arterial collateral status, estimated by the Hypoperfusion Intensity Ratio (HIR) on perfusion MRI, and stroke etiology in anterior circulation large vessel occlusion (LVO).
We retrospectively analyzed anterior circulation LVO acute stroke patients with a baseline perfusion MRI performed within 24 h from symptom onset. To avoid selection bias, patients were chosen from (1) the prospective registry of one comprehensive stroke center that included both thrombectomy-treated and untreated patients with systematic use of perfusion MRI and (2) one prospective thrombectomy study where perfusion MRI was acquired per protocol, but treatment decisions were made blinded to the results. Stroke etiology was evaluated according to the TOAST classification. HIR, defined as the proportion of time-to-maximum (Tmax) > 6 s with Tmax > 10 s volume, was measured on perfusion imaging. The relationship between stroke etiology (large artery atherosclerosis [LAA]) versus cardioembolism [CE]) and HIR was assessed by bivariate then multivariable binary logistic regression analyses.
Among the 310 included patients, stroke etiology was CE in 178 (57%) and LAA in 51 (16%). Patients with CE stroke etiology had higher HIR (0.43 vs 0.31,
CE etiology is associated with worse collateral circulation in LVO-related acute stroke patients.
Hypertension is a major risk factor of structural brain changes, including atrophy and cerebral small vessel disease. Intracranial arteriosclerosis could be an underlying mechanism between hypertension and structural brain changes. This study investigated whether intracranial carotid artery calcification (ICAC), as a proxy for intracranial arteriosclerosis, explains the association between hypertension and structural brain changes in patients with TIA or ischemic stroke.
About 968 patients (mean age 62.7 years) with TIA or ischemic stroke from a registry who underwent non-contrast CT (NCCT) and CT-angiography (CTA) were included in this study. Presence and volume (mm3) of ICAC were assessed on CTA. Subtypes of ICAC were assessed on NCCT, where ICAC was categorized into intimal and internal elastic lamina (IEL) type calcification. Structural brain changes, indicated by atrophy, periventricular and deep white matter lesions (WML), and lacunes were assessed on NCCT. Mediation analysis was performed using ICAC, ICAC volume, and ICAC subtypes as mediators.
ICAC was prevalent in 67.8% of patients, with 52.6% of them exhibiting intimal calcification, and 26.5% exhibiting IEL calcification. Atrophy, periventricular WML, deep WML, and lacunes were present in 48.1%, 56.4%, 43.0% and 17.1% of patients respectively. The presence of ICAC explained 7.1% of the association of hypertension with periventricular WML, 3.6% with deep WML, and 17.6% with lacunes. Hypertension was associated with increased atrophy through ICAC (OR: 1.02, 95% CI: 1.00–1.05). In subgroup analyses, IEL calcification partly explained the association between hypertension and periventricular WML (16.8%), and atrophy (OR: 1.12, 95% CI: 1.02–1.27). Intimal calcification did not explain any association.
ICAC partially explained the association between hypertension and atrophy, periventricular and deep WML, and lacunes. Although intimal calcification was more prevalent in ischemic stroke patients, IEL calcification takes the leading role in explaining the association between hypertension and structural brain changes.

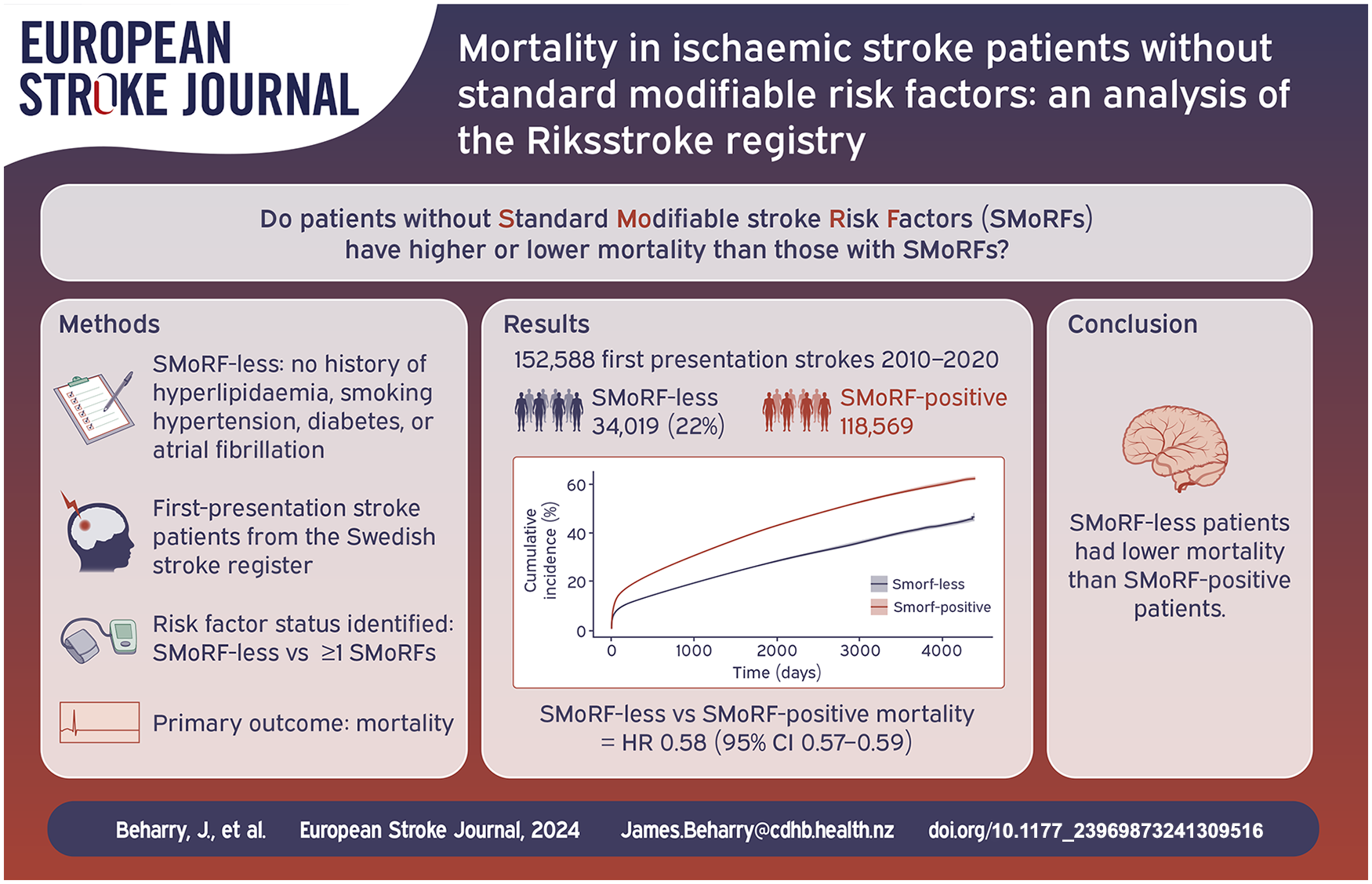
Little is known of the long-term prognosis of patients with acute ischaemic stroke in the absence of standard modifiable stroke risk factors (SMoRFs). In acute coronary syndromes, patients without modifiable risk factors have a higher mortality rate. We analysed data from the Swedish Stroke Register to determine survival of patients without SMoRFs following an ischaemic stroke.
We identified adult patients with first-presentation acute ischaemic stroke between 2010 and 2020. Patients were considered to possess a SMoRF if they had one of: hypertension, diabetes, hyperlipidaemia, atrial fibrillation or an active smoking history. We compared mortality in patients with and without SMoRFs following first-presentation ischaemic stroke using cox regression models. We also assessed the combined endpoint death and dependency (mRS 3–6) at 3 months via logistic regression models.
Of 152,588 patients with ischaemic stroke, hypertension (58.7%) and atrial fibrillation (27.3%) were the most common risk factors. 34,019 patients (22.3%) had no SMoRFs. After a first-presentation ischaemic stroke, patients without SMoRFs had a lower risk of death than patients with one or more SMoRFs (HR 0.58 [95% CI 0.57–0.59]). The absence of SMoRFs was associated with lower odds of death and dependency at 3 months in logistic regression models (OR 0·60 [95% CI 0.58–0.62]).
One in five patients with acute ischaemic stroke had no standard modifiable stroke risk factors. These patients have lower risk of death compared to patients with one or more SMoRFs.
The progression of diabetes status in post-stroke patients remains under-investigated, particularly regarding new treatments for type II diabetes mellitus (DM II), like glucagon-like peptide 1 receptor agonists (GLP-1-RA) and sodium-glucose co-transporter-2 (SGLT-2) inhibitors, which have not been studied in the post-stroke setting.
Eight hundred eighty-four consecutive ischemic stroke patients recruited to our prospective STROKE-CARD Registry were assessed concerning their glycemic status at baseline (normoglycemia, prediabetes, DM II) and change over time within 1 year follow-up. Multivariate logistic regression was performed to identify factors associated with transitioning from normoglycemia to prediabetes or DM II. Additionally, we reviewed ongoing clinical trials for GLP-1-RA and SGLT-2 inhibitors in the context of acute ischemic stroke.
At baseline, 44.6% (
GPrediabetes and DM II are frequent in ischemic stroke patients. Even within an intensified post-stroke disease management setting, a considerable amount of stroke survivors convert to prediabetes or DM II within the first year. Our results demonstrate a notable proportion of patients qualifying inclusion in studies examining the efficacy of GLP-1-RA agonists and SGLT-2 inhibitors in secondary prevention.
Given the high prevalence and progression of prediabetes and DM II in stroke survivors, there is a need for clinical trials evaluating the use of GLP-1-RA and SGLT-2 inhibitors in this population.

Population level tracking of post-stroke functional outcomes is critical to guide interventions that reduce the burden of stroke-related disability. However, functional outcomes are often missing or documented in unstructured notes. We developed a natural language processing (NLP) model that reads electronic health records (EHR) notes to automatically determine the modified Rankin Scale (mRS).
We included consecutive patients (⩾18 years) with acute stroke admitted to our center (2015–2024). mRS scores were obtained from the Get With the Guidelines registry and clinical notes (if documented), and used as the gold standard to compare against NLP-generated scores. We used text-based features from notes, along with age, sex, discharge status, and outpatient follow-up to train a logistic regression for prediction of good (0–2) versus poor (3–6) mRS, and a linear regression for the full range of mRS scores. The models were trained for prediction of mRS at hospital discharge and post-discharge. The models were externally validated in a dataset of patients with brain injuries from a different healthcare center.
We included 5307 patients, 5006 in train and test and 301 in validation; average age was 69 (SD 15) and 65 (SD 17) years, respectively; 47% female. The logistic regression achieved an area under the receiver operating curve (AUROC) of 0.94 [CI 0.93–0.95] (test) and 0.94 [0.91–0.96] (validation), and the linear model a root mean squared error (RMSE) of 0.91 [0.87–0.94] (test) and 1.17 [1.06–1.28] (validation).
The NLP-based model is suitable for use in large-scale phenotyping of stroke functional outcomes and population health research.

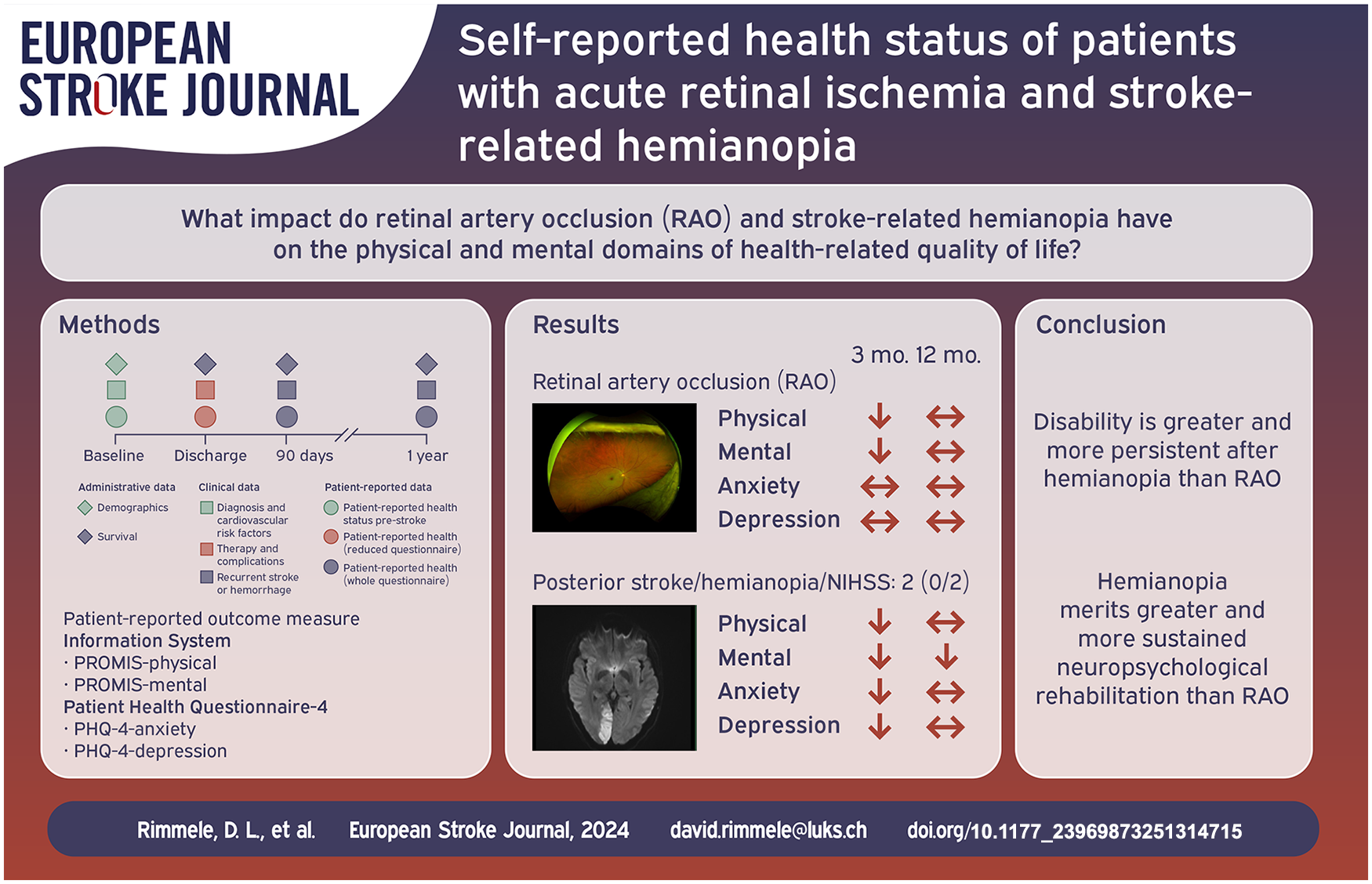
We aimed to assess impairments on health-related quality of life, and mental health resulting from Retinal artery occlusion (RAO) with monocular visual field loss and posterior circulation ischemic stroke (PCIS) with full or partial hemianopia using patient-reported outcome measures (PROMs).
In a prospective study, consecutive patients with acute RAO on fundoscopy and PCIS on imaging were recruited during their surveillance on a stroke unit over a period of 15 months. Baseline characteristics were determined from medical records and interviews. Health-related quality of life (PROM Information System 10-Question-Short-Form, PROMIS-10), and mental health symptoms (Patient-Health-Questionnaire-4, PHQ-4) were assessed 3 and 12 months after admission postally and via phone.
Ffity-seven patients with RAO and 19 with isolated full or partial hemianopia determined by the NIHSS (median = 2; IQR:0/2) according to PCIS were included. Characteristics of cardiovascular risk factors, and functional status pre-stroke were comparable between the groups. At 3 months, mean ± standard deviation
RAO led only to partial and to less persistent mental impairments than PCIS. This suggests that a different approach involving complex visual and neuropsychological treatment over a longer period of time needs to be considered for post-stroke care of PCIS.
The trial was submitted at http://www.clinicaltrials.gov, under NCT03795948.
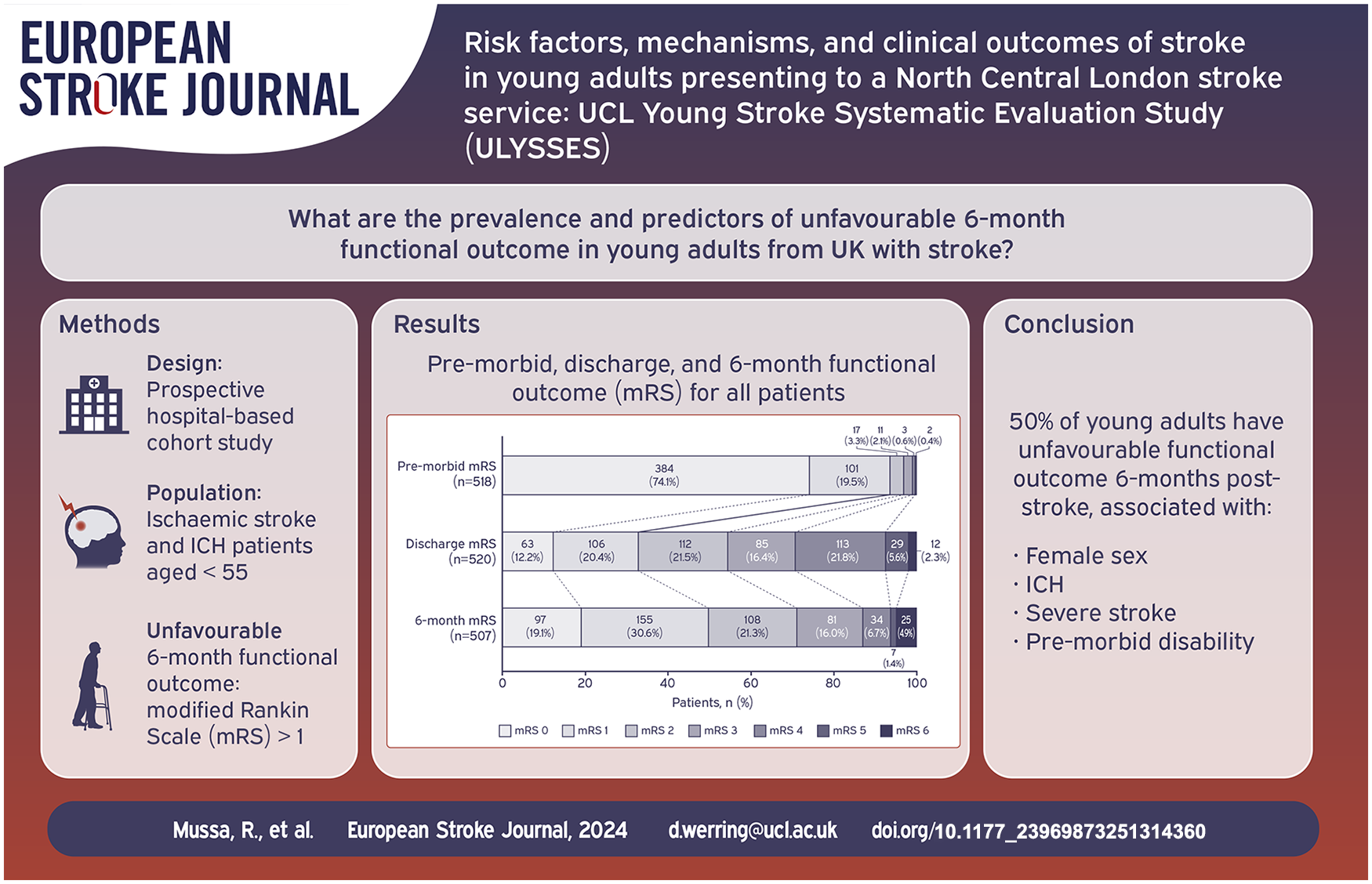
Stroke incidence in younger adults is increasing worldwide yet few comprehensive studies exist from a UK population. We investigated the risk factors, mechanisms, functional outcome and stroke recurrence rate in a cohort of young adults with stroke.
We included consecutive patients (<55 years) with ischaemic stroke or intracerebral haemorrhage (ICH) admitted to the University College London Hospitals Hyperacute Stroke Unit between 2017 and 2020. Ischaemic stroke was classified using Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria and ICH using modified CLAS-ICH criteria. Multivariable logistic regression was performed to identify predictors of unfavourable functional outcome (modified Rankin Scale [mRS] > 1) at 6 months.
Five hundred fifty-two patients were included (median age 47, IQR 41–51; 33% female; 76% ischaemic stroke). Common risk factors included dyslipidaemia (57%), hypertension (40%), and cigarette smoking (34%). Ischaemic stroke was mostly due to cardioembolism (22%). Probable cerebral small vessel disease was the most frequent ICH aetiology (53%). Unfavourable functional outcome was prevalent in 50% at 6 months and was associated with ICH (OR 2.02, 95%CI 1.14–3.58,
Traditional cardiovascular risk factors are common in young adults with stroke. Unfavourable functional outcome is associated with female sex, ICH, severe stroke and pre-morbid disability. These findings can inform national stroke prevention and rehabilitation strategies.
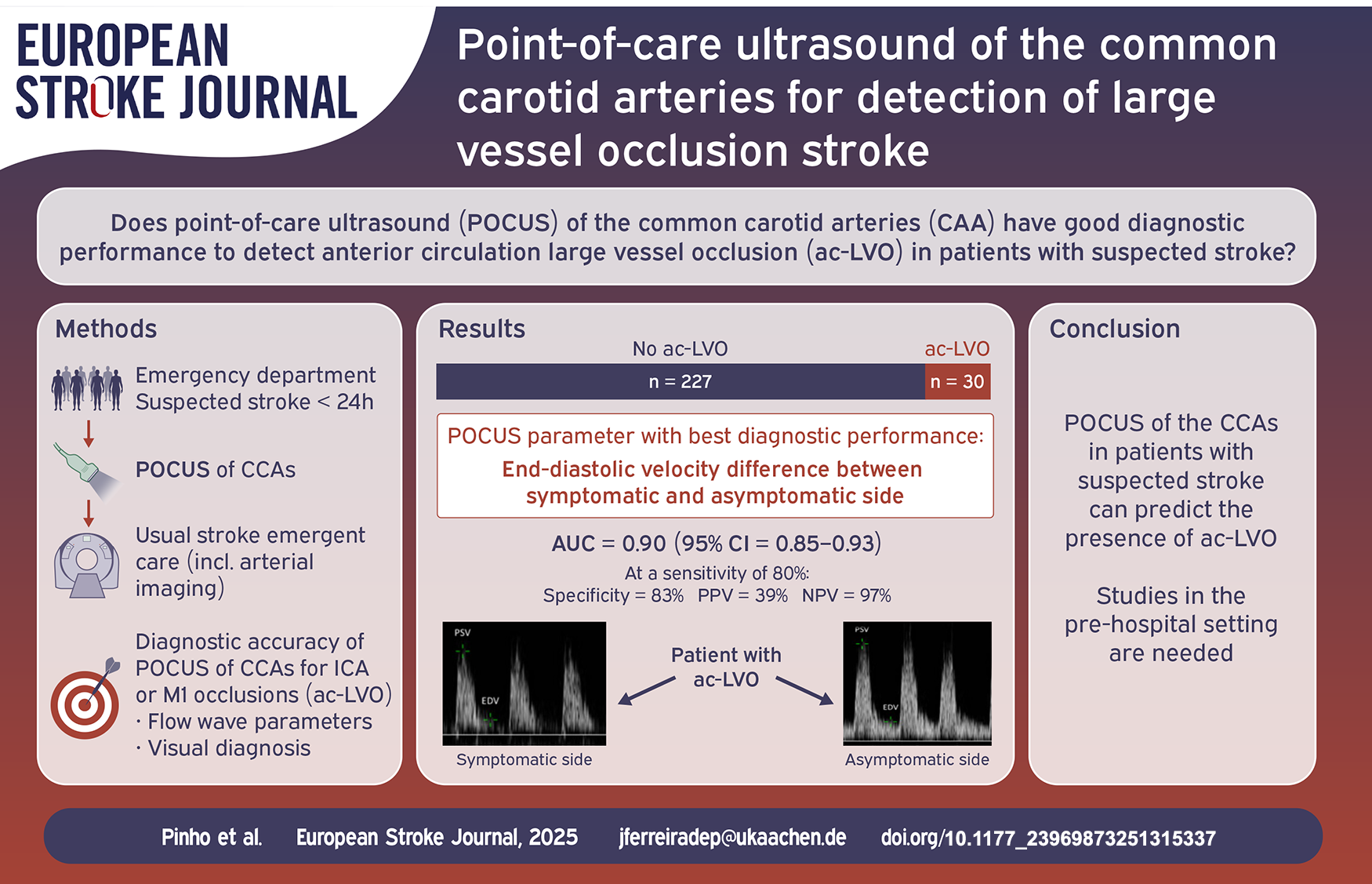
Distal arterial occlusions can cause measurable changes in the flow wave profile in proximal segments of the feeding artery. Our objective was to study the diagnostic accuracy of point-of-care ultrasound (POCUS) of the common carotid arteries (CCA) for detection of anterior circulation large vessel occlusion (ac-LVO) in patients with suspected stroke.
We conducted a prospective, single-center, observational study of adult patients with suspected stroke admitted in the emergency department. Flow wave profiles of both CCAs were generated by non-specialists using POCUS as soon as possible after admission. ac-LVO was defined as an internal carotid artery or M1 occlusion in CT- or MR-angiography. The diagnostic performances for detection of ac-LVO using flow wave parameters were calculated.
Among 283 patients recruited during a 10-month period, 257 patients (91%) had CCA ultrasound images of sufficient quality and were included for analysis. The mean age was 75 years (IQR 62–83), 131 were female (51.0%), median baseline NIHSS was 2 (IQR 0–5). The most frequent final diagnosis was ischemic stroke (49.4%), ac-LVO was present in 30 patients (11.9%). The median duration of POCUS was 3 min (IQR 2–5). Among all flow wave parameters, the highest diagnostic accuracy for ac-LVO detection was found for end-diastolic velocity difference between sides (AUC = 0.90, 95%CI = 0.85–0.93), with a specificity of 83% (95%CI = 78–88%) at a predefined sensitivity threshold of 80%.
POCUS of the CCA in patients with suspected stroke can predict the presence of ac-LVO. These results need to be replicated in a prehospital setting.
Eccentric vessel wall enhancement (EVWE) and high-sensitivity C-reactive protein (hs-CRP) are inflammatory biomarkers associated with atherosclerotic disease. We investigated their prognostic value in patients with acute ischemic stroke receiving guideline-adherent medical treatment.
In this prospective observational cohort study, patients with acute ischemic stroke attributed to intracranial arterial disease (ICAD) underwent vessel wall MRI and hs-CRP testing. The study included intracranial cases of both large artery atherosclerosis (LAA) and small vessel occlusion (SVO). The primary outcome was subsequent ischemic stroke during the follow-up period. The median follow-up duration was 21 months. Kaplan-Meier survival and Cox regression analysis was used to determine the associations between EVWE, hs-CRP levels, and subsequent ischemic stroke.
Among 191 patients, 81 (42.4%) had EVWE. EVWE positivity showed a trend toward a lower risk of subsequent ischemic stroke compared to EVWE negativity (HR 0.32, 95% CI 0.12–0.87;
In this observational study of patients with intracranial atherosclerotic stroke receiving optimal medical therapy, EVWE positivity appeared to be associated with a trend toward lower risk of recurrent stroke, though this relationship requires further validation.
The combination of EVWE and hs-CRP status might potentially offer prognostic information, with preliminary data suggesting that EVWE positivity and low hs-CRP levels could be associated with more favorable outcomes in patients receiving guideline-adherent medical treatment. These preliminary findings suggest a possible role for combining imaging and serum inflammatory biomarkers in risk stratification, though larger prospective studies are needed to confirm these associations.

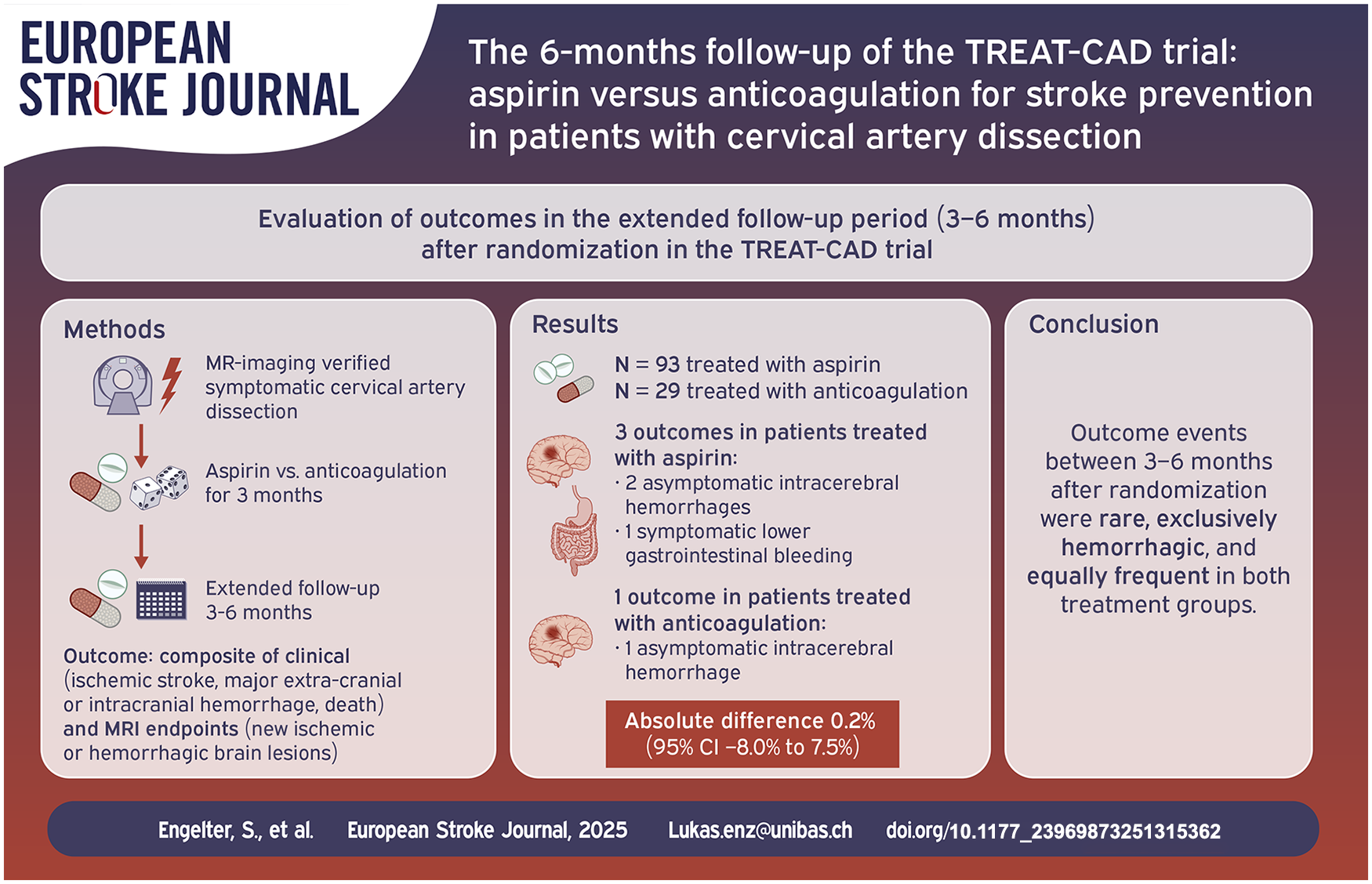
Cervical artery dissection is a major cause of stroke in the young. The optimal choice and duration of antithrombotic treatment for stroke prevention are debated, particularly beyond 3 months after symptom onset.
TREAT-CAD (
Among the 122 participants in the as-treated analysis, 3/93 (3.2%) aspirin-treated participants had new clinical (
During the extended follow-up period of a controlled randomized trial comparing aspirin to anticoagulation in cervical artery dissection, outcomes between 3 and 6 months after randomization occurred rarely, similarly often in both groups and were exclusively hemorrhagic events. Thus, studies balancing benefits versus harms of antithrombotic treatment beyond 3 months are warranted. Registration: ClinicalTrials.gov: NCT02046460. https://clinicaltrials.gov/ct2/show/NCT02046460.
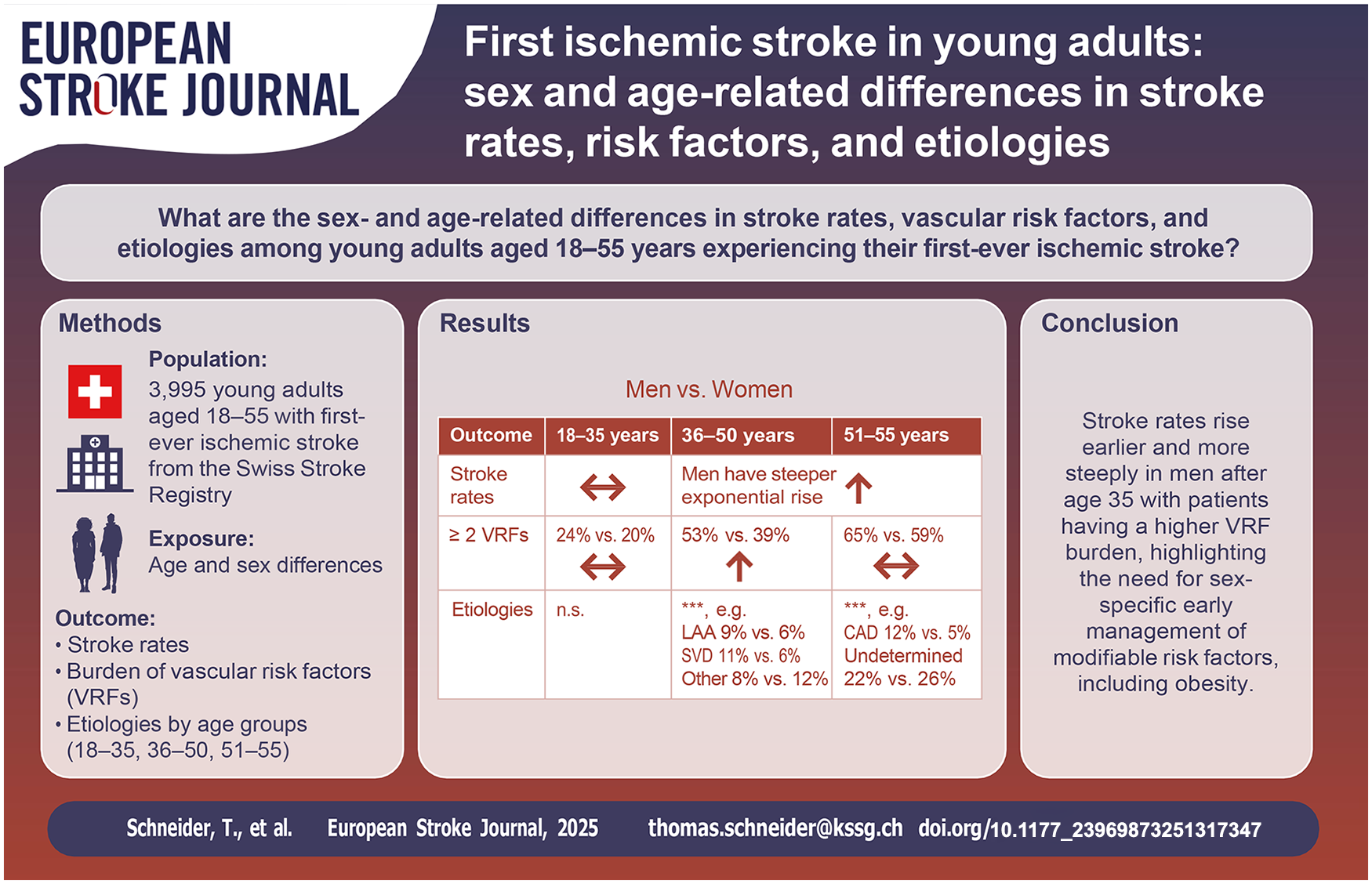
Sex differences in stroke incidence, vascular risk factors (VRFs), and etiologies among young adults remain underexplored, particularly regarding age-related patterns.
We retrospectively analyzed young adults (18–55 years) with first-ever ischemic stroke treated at certified acute stroke units/centers between 2014 and 2022, using Swiss Stroke Registry data. Stroke rates (per 100,000 person-years), VRFs, and etiologies were assessed by age and sex.
Among 3,995 stroke patients, stroke rates were similar between sexes until age 35, after which men showed a more pronounced exponential increase. This rise was particularly notable in patients with elevated BMI and ⩾2 VRFs. The proportion of patients with ⩾2 VRFs rose with age (18–35: 22%; 36–50: 48%; 51–55: 63%). While no statistically significant differences in VRF profiles were observed between men and women aged 18–35, men accumulated VRFs about five years earlier than women, leading to a higher prevalence of multiple VRFs in men aged 36–50, with the gap narrowing in the 51–55 group. Stroke etiologies shifted with age: patent foramen ovale and cervical artery dissection predominated in younger patients, while large artery atherosclerosis, small vessel disease, and strokes of undetermined etiology increased with age, with notable sex differences.
This study highlights sex and age differences in ischemic stroke rates, VRFs, and etiologies among adults under 55 years. After 35, stroke rates rose more sharply in men, paralleling their higher VRF burden. These findings emphasize the importance of early management of VRFs—including overweight—to mitigate stroke risk.
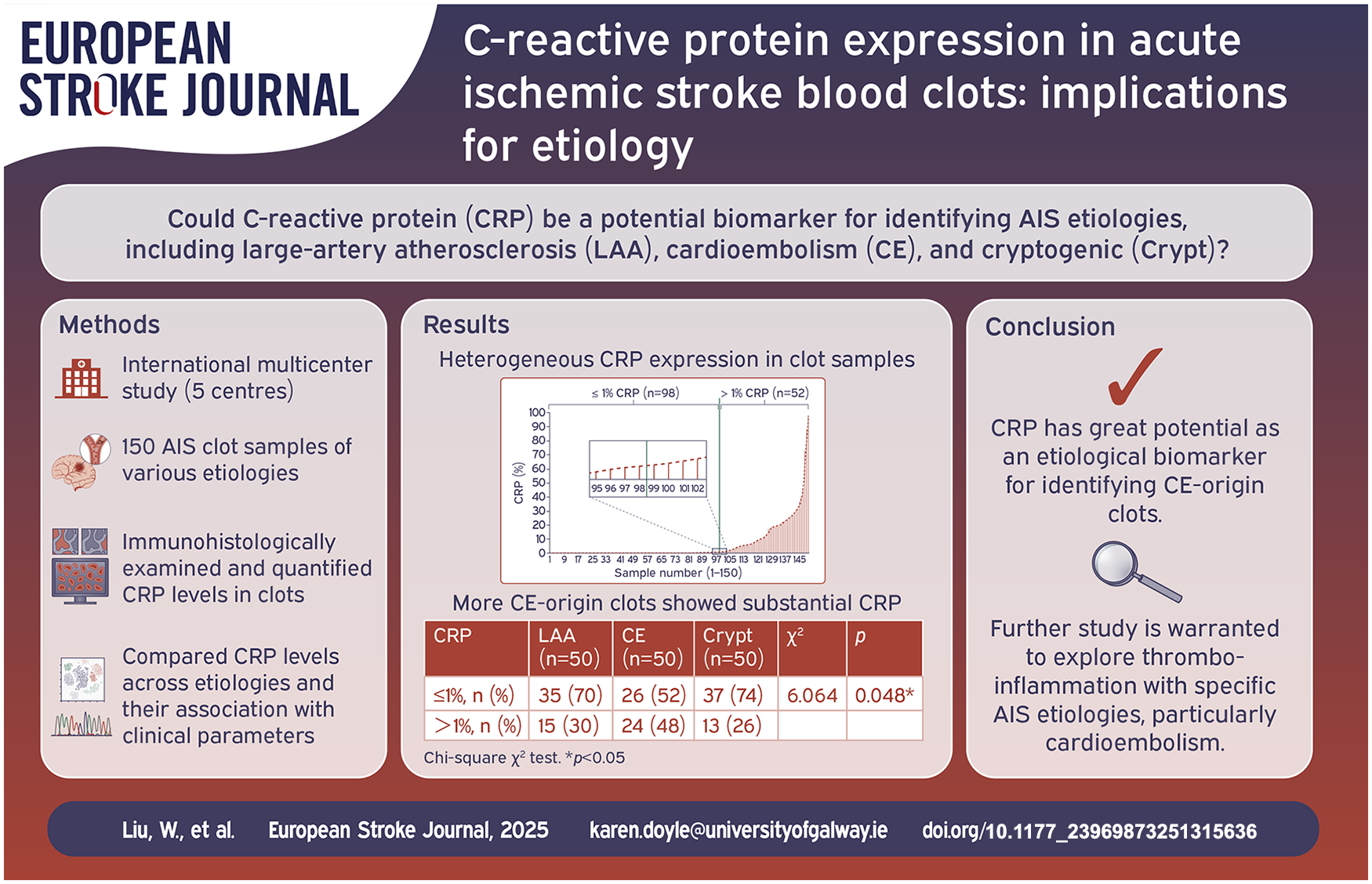
C-reactive protein (CRP) is a prototypic inflammation marker, with elevated levels associated with an increased risk of cerebrovascular events. To determine whether CRP could be a useful biomarker of stroke etiology, we investigated CRP expression in acute ischemic stroke (AIS) clots from large-artery atherosclerosis (LAA), cardio-embolism (CE) and cryptogenic (Crypt) subtypes.
We analysed clot samples from AIS patients (LAA, CE, Crypt;
CRP expression varied significantly among clots. Most clots (65%) had minimal (⩽1%) CRP and 35% showed substantial (>1%) CRP. CE group had significantly more clots with substantial CRP than LAA and Crypt (48% vs 30% and 26%;
Significantly more AIS clots of CE expressed substantial CRP compared to those of LAA and Crypt, suggesting CE strokes may be more strongly linked to inflammation. Clots with substantial CRP expression displayed significantly more fibrin compared to those with minimal CRP expression, suggesting a potential association between inflammation and fibrin-rich clots. Further study of the relationship between CRP, fibrin and WBCs in clots may improve our understanding of the processes of thrombo-inflammation.
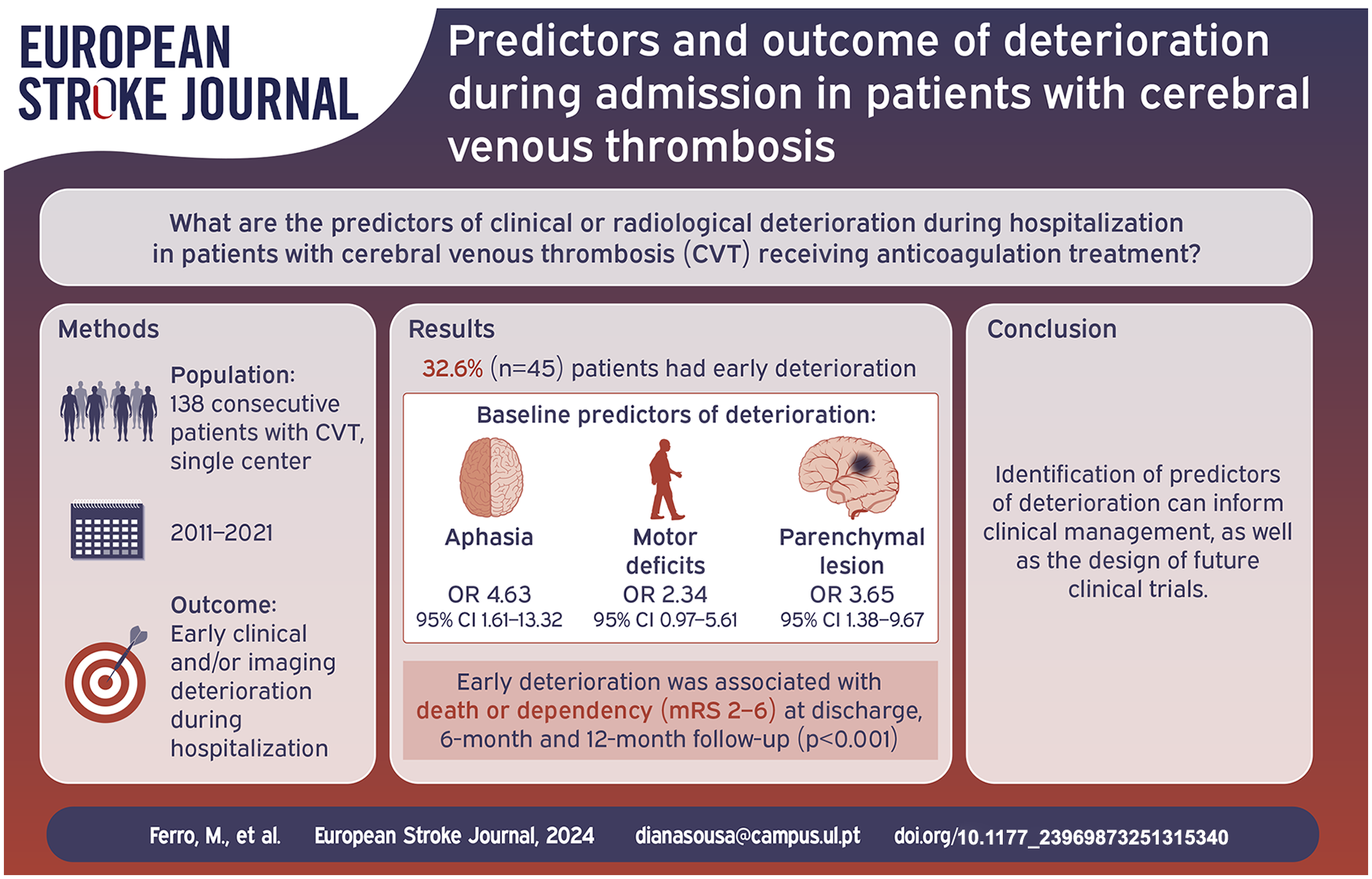
Cerebral venous thrombosis (CVT) is a less common stroke subtype. While long term outcome factors have been extensively studied, short term deterioration remains poorly understood.
We conducted a 10-years retrospective analysis at a high-volume tertiary center, including consecutive patients diagnosed with CVT. The primary outcome was early deterioration (ED), defined as decrease in Glasgow Coma Scale,
We included 138 patients (81.2% female, median age 42.0 years (IQR 29.3–49.0)). Forty-five (32.6%) patients had ED, with 33 (23.9%) showing clinical deterioration and 35 of 104 (33.7%) imaging worsening. Variables selected from the multivariate model for association with ED were aphasia (OR 4.63, 95% CI 1.61–13.32), motor deficits (OR 2.34, 95% CI 0.97–5.61), and parenchymal lesion (OR 3.65, 95% CI 1.38–9.67). Twenty-seven patients underwent endovascular treatment after deterioration. Patients in the ED group had worse functional outcome at discharge, 6 and 12 months (
One third of patients in this cohort experienced ED. Patients with aphasia, motor deficit, or parenchymal brain lesion at baseline were at higher risk. These patients performed worse at long term follow-up.
We identified predictors of ED in patients with CVT. These patients should be carefully monitored. These findings may inform the design of future clinical trials aimed at evaluating additional therapeutic interventions in the acute phase.
Contemporary estimates of the impact of type 2 diabetes (T2D) on stroke outcomes are important for care planning and resource allocation. This retrospective cohort study compared the incidence of stroke and subsequent clinical and economic outcomes following stroke among people with and without T2D.
Data were extracted from a subset of the French Système National des Données de Santé database. Stroke incidence as well as post-stroke clinical outcomes, healthcare resource utilization (HCRU), use of stroke preventative treatments, and costs were compared among people with and without T2D.
The study included 10,906 patients hospitalized for stroke including 2141 (19.6%) people with T2D. Age-standardized stroke incidence rates were 3.3 (95% confidence interval [CI] 3.1; 3.6) per 1000 person-years and 2.2 (2.1; 2.3) in people with and without T2D, respectively. Patients with T2D had significantly higher risk of stroke recurrence (adjusted hazard ratio [HR] 1.14, 95% CI: 1.01; 1.30) and mortality (HR 1.16, 95% CI: 1.08; 1.25) than patients without T2D. The proportion of patients with T2D treated with statins decreased from 27.3% pre-stroke to 20.6% post-stroke but remained relatively stable among patients without T2D (from 13.4% to 13.1%). The mean healthcare costs in the 12 months following stroke were higher among patients with T2D than those without (€22,635 vs €18,629).
The incidence and clinical and economic burden of stroke is considerably higher among people with T2D. Further efforts are needed to reduce this disparity.
This is a visual representation of the abstract.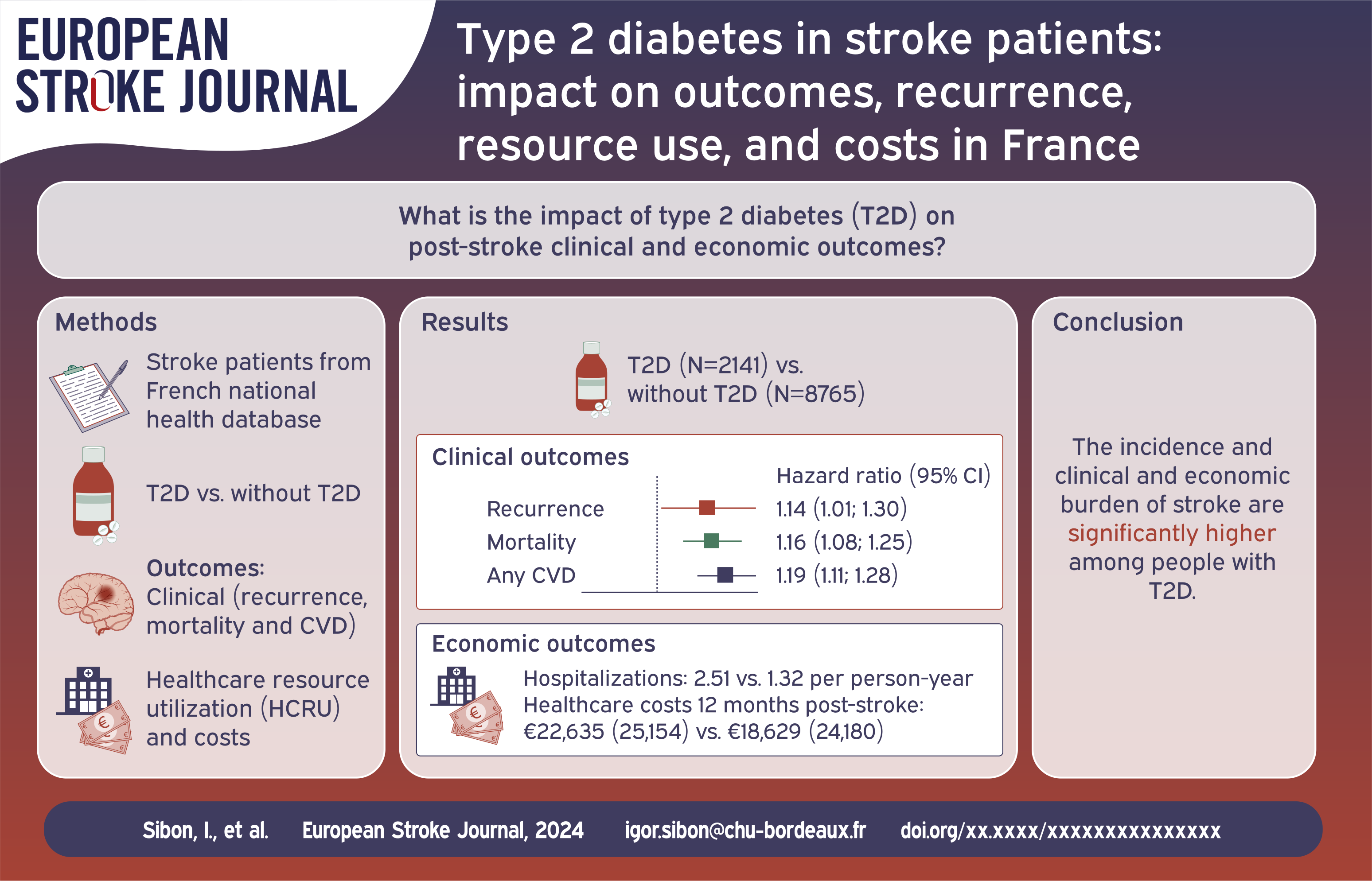
The degree of culprit artery stenosis affects the risk of early neurological deterioration (END) after acute ischemic stroke (AIS). The TREND trial demonstrated the efficacy of tirofiban in preventing END in patients with AIS. We aimed to investigate whether the degree of intracranial artery stenosis affects the efficacy of tirofiban in preventing END in patients with AIS.
We conducted a post hoc analysis of the TREND trial, which enrolled patients within 24 h of onset and randomly allocated to receive intravenous tirofiban or oral aspirin. We stratified the stenosis degrees into three subgroups: no stenosis, mild-to-moderate stenosis (stenosis <70%), and severe stenosis or occlusion (stenosis ⩾70%). The primary endpoint is END4 defined as an increase of the NIHSS ⩾4 within 72 h after randomization. Secondary outcomes include END2 (defined as an increase of NIHSS ⩾2) within 72 h after randomization, the proportion of mRS 0–1 and 0–2 at 90 days.
A total of 296 patients were analyzed. In patients with severe stenosis or occlusion, tirofiban significantly reduced the incidence of END4 (5.7% vs 30.8%, adjusted OR 0.156, 95% CI 0.028–0.873, adjusted
Tirofiban may significantly reduce the incidence of END in patients with severe arterial stenosis or occlusion. Further studies are required to confirm the effects of intracranial artery stenosis on the benefits of intravenous tirofiban.
ClinicalTrials.gov; identifier: NCT04491695.
This is a visual representation of the abstract.
Infective endocarditis (IE) is a life-threatening condition and a rare cause of ischemic stroke (IS). This study aimed to evaluate the utility of analyzing cerebral thrombi, obtained through endovascular thrombectomy in IS, for the pathological diagnosis of IE.
Cerebral thrombi from three groups of IS patients were compared: definite IE (
Median age of included patients was 73 years and 50% were females. Hematoxylin & Eosin and Grocott-Gomori Methenamine Silver stains detected microorganisms in all IE cerebral thrombi, and none in the control groups. Thrombus PCR detected relevant microorganism in n = 2/7 IE. Compared to control groups, IE thrombi were characterized by significant lower content of red blood cells (median [IQR]: IE = 7.4 [4.2–26.7], CE-I− = 49.3 [17–62.6], CE-I+ = 57.5 [40.7–60.8], % over thrombus section area [%TSA],
Multimodal analysis of cerebral thrombi in IS with suspected IE supports early and definite pathological diagnosis by detecting pathogens and assessing changes in thrombus composition.
This is a visual representation of the abstract.
While adiposity is an established risk factor for incident ischemic stroke, its influence on functional recovery after stroke is uncertain. We leveraged Mendelian randomization (MR) to examine the causal effects of body mass index (BMI) and waist-to-hip ratio (WHR) on post-stroke motor, cognitive, and global recovery.
Genetic proxies for BMI and WHR were obtained from a genome-wide association study (GWAS) meta-analysis of the GIANT consortium and the UK Biobank (
A 1-standard deviation (SD) increase (~4.8 kg/m2) in genetically predicted BMI associated with lower odds of post-stroke motor improvement (OR = 0.37, 95% CI = 0.19-0.72;
Human genetic evidence suggests that elevated adiposity negatively impacts multiple post-stroke outcomes, including motor function, cognition, and overall recovery. The biological pathways underlying these associations warrant further investigation.
This is a visual representation of the abstract.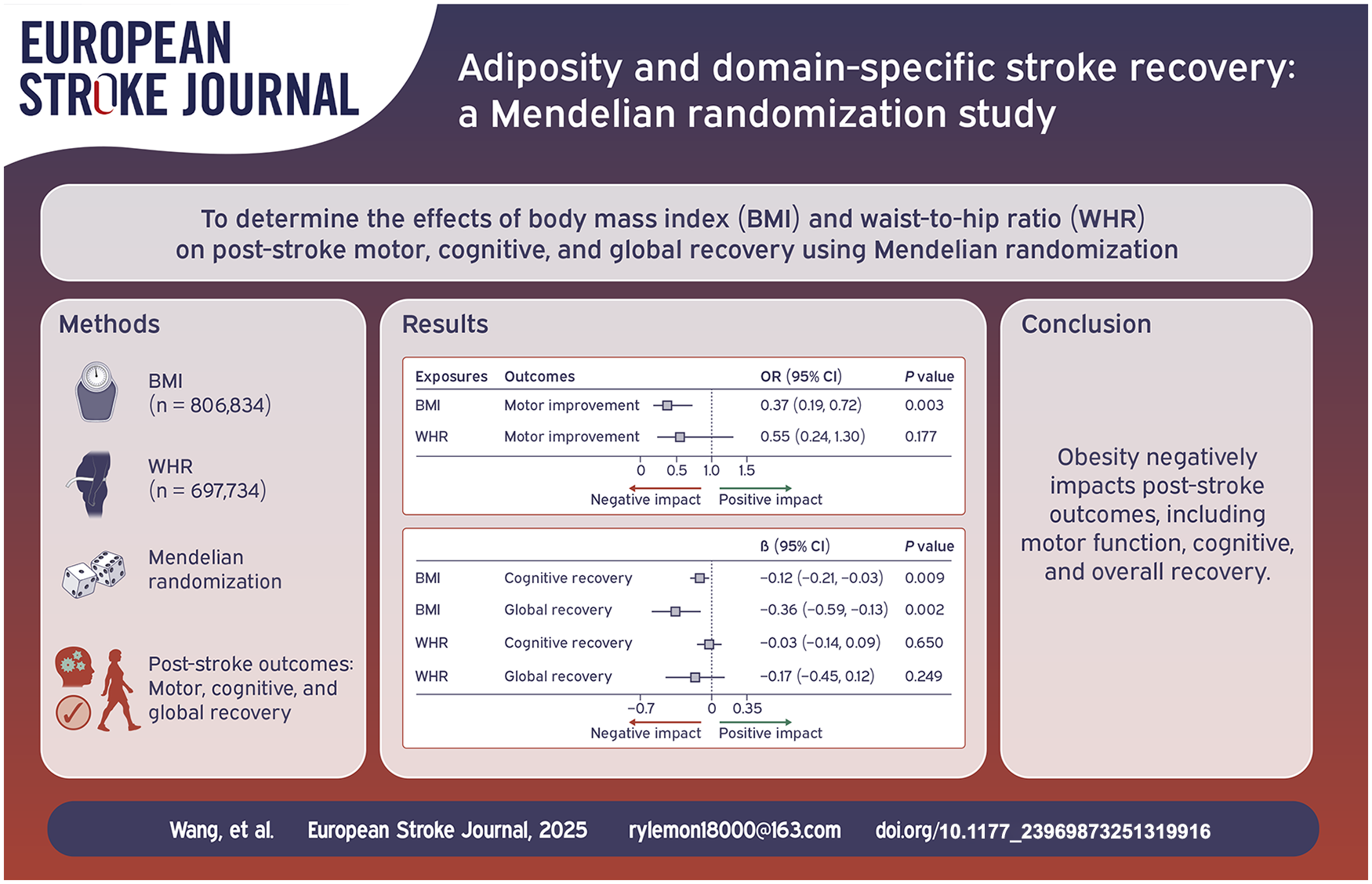
The impact of multiple feeding arteries on clinical outcomes of cerebral arteriovenous malformations (AVMs) is not well understood. This study aims to compare outcomes between AVMs with multiple versus single feeding arteries.
Data from the Multicenter International Study for Treatment of Brain AVMs (MISTA) consortium were analyzed. Propensity score matching (PSM) was used to balance cohorts. Subgroup analysis was conducted for ruptured and unruptured AVMs and different treatment options, and multivariable logistic regression was applied to assess the impact of feeding artery origin.
Among 953 patients, 661(69.4%) had multiple feeding arteries, and 292 (30.6%) had a single feeding artery. After PSM, which included 422 matched patients (211 in each group), the differences in obliteration rates (68.7% vs 74.8%, OR 0.73, 95% CI: 0.48–1.12,
AVMs with a single feeding artery were more likely to present with rupture, but no significant differences in obliteration rates or complications were observed between the groups after PSM. These findings suggest that while the number of feeding arteries may influence the initial presentation, it does not appear to impact overall treatment success or patient prognosis. Further prospective studies are needed to confirm these findings.
This is a visual representation of the abstract.
The modified Rankin Scale (mRS) is the most frequently used primary outcome measure in acute stroke research despite significant interobserver variability in assigning grades. We assessed the use of central blinded adjudication of the mRS based on a video recording of an interview in the PRECIOUS trial.
PRECIOUS was an international, randomized, open-label, clinical trial with blinded outcome assessment of preventive treatment with metoclopramide, paracetamol, and ceftriaxone in elderly patients with acute stroke. Trained local investigators interviewed patients or their representatives and graded functional outcome at 90 days after stroke with the mRS. In each participating country, a video recording of the interview was assessed by three blinded, independent adjudicators. The primary outcome of the present substudy was interobserver agreement between the local mRS score and the median score of the three central adjudicators for patients alive at 90 days, assessed with Cohen’s kappa and quadratic weighted kappa statistics. The difference between treatment effect estimates based on local and central adjudication was a secondary outcome.
Of 1493 patients enrolled in PRECIOUS, 1471 were included in this analysis. At 90 days, 1117 patients (75.9%) were alive and had both a central and local assessment; 28 participants did not have a central mRS score. Interobserver agreement was seen in 829 (74.2%) patients and was substantial (kappa of 0.68; 95% CI 0.65–0.71). Disagreement occurred more often in patients with a central mRS score of 0–2 (OR 2.24; 95% CI 1.14–4.24). Treatment effects were neutral for all three study drugs and did not differ between central and local adjudication.
Central adjudication of the mRS based on a video recording is feasible in a large international, randomized stroke trial. This ensures blinding of the outcome assessment. In this neutral trial, the impact of central adjudication on the precision of effect size estimates could not be assessed.

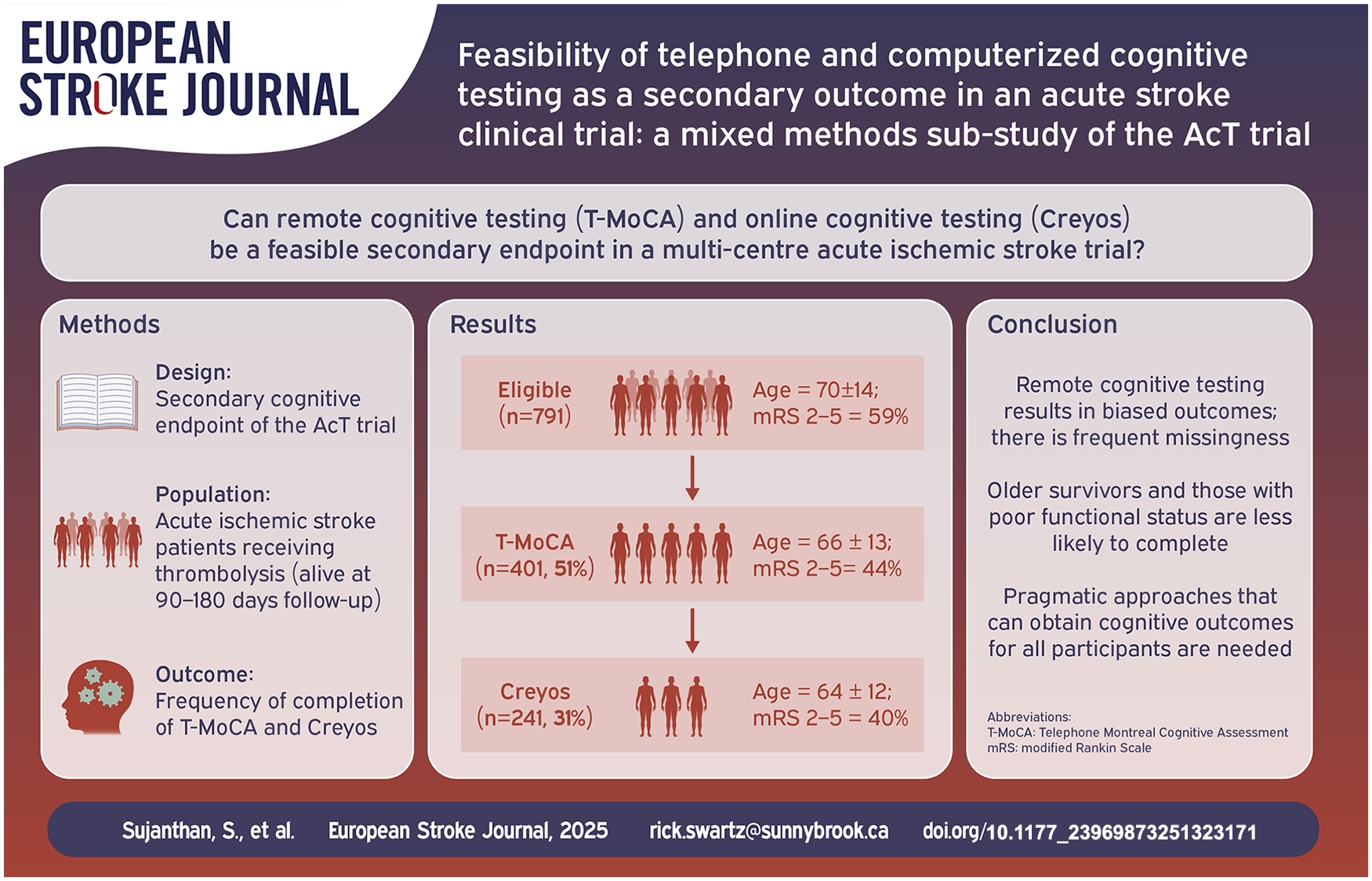
Post-stroke cognitive impairment is associated with impaired quality of life. Remote testing provides a potential avenue to measure cognitive outcomes efficiently.
Prospective cognitive outcomes were collected at 90–180 days using both telephone MoCA (T-MoCA; range 0–22; <17 impairment) and Creyos, a computerized cognitive battery. Key variables associated with completion were assessed using logistic regressions. Mixed methods brief structured interviews and exit survey were performed to explore barriers to completing computer testing.
Of 791 potentially eligible patients (mean age 70 ± 14 years), there was low feasibility of remote cognitive testing, with only 401 (51%) completing the T-MoCA, and 242 (31%) completing Creyos. Our regression models show that age (ORT-MoCA: 0.95 (95% Confidence Interval (CI): 0.94–0.97); ORCreyos: 0.95 (95% CI: 0.94–0.96)), functional impairment (mRS 2–5; ORT-MoCA: 0.55 (95% CI: 0.37–0.81); ORCreyos: 0.66 (95% CI: 0.44–0.98)), quality of life (EQ-VAS; ORT-MoCA: 1.02 (95% CI: 1.01–1.03); ORCreyos: OR:1.02 (95% CI: 1.01–1.03)) and length of hospital stay (ORT-MoCA: 0.98 (95% CI: 0.96–0.99); ORCreyos: 0.97 (95% CI: 0.94–0.99)) predicted both telephone and computer cognitive test completion; computer literacy predicted computer test completion (ORCreyos: 1.12 (95% CI: 1.04–1.21)). In interviews, a preference for accessibility of computerized testing was reported.
Remote cognitive testing has limited feasibility as a secondary outcome in large acute stroke trials. Patients who are older, with worse quality of life, or severe functional impairment post-stroke are less likely to complete remote cognitive outcomes.
Innovative approaches to post-stroke cognitive outcomes in acute stroke trials are needed.
Data available upon request.
A better understanding of who will develop dementia can inform patient care. Although MRI offers prognostic insights, access is limited globally, whereas CT-imaging is readily available in acute stroke. We explored the prognostic utility of acute CT-imaging for predicting dementia.
We included stroke or transient ischaemic attack (TIA) survivors from participating stroke centres in Scotland. Acute CT-scans were rated using ordinal scales for neurodegenerative and cerebrovascular changes (old infarcts, white matter lesions (WMLs), medial temporal lobe atrophy (MTA), and global atrophy (GA)) and combined together to a ‘brain-frailty’ score. Dementia status was established at 18-months following stroke or TIA.
Among 195 participants, 33% had dementia after 3 years of follow-up. High brain-frailty score (⩾2/4) correlated with higher risk of dementia (HR (95% CI) 6.02 (1.89–19.21)). As individual predictor, severe MTA was most strongly associated with dementia (adjusted HR (95% CI) 2.09 (1.07–4.08)). Other predictors associated with dementia included older age, higher prestroke morbidity (mRS), WMLs, and GA. Integrated in a prediction model with clinical parameters, prestroke mRS, cardiovascular disease, GA, MTA and Abbreviated-Mental-Test were the strongest predictors of dementia (c-statistic: 0.77).
Increased brain-frailty, and its individual components (WMLs, MTA, and GA) are associated with a higher risk of dementia in participants with stroke. Combining clinical and brain-frailty parameters created a moderate dementia prediction model but added little value over clinical parameters in combination with cognitive testing. CT-based brain-frailty may provide better prognostic insights when cognitive testing isn’t feasible and for identifying highest-risk individuals for dementia prevention trials to increase trial efficiency.

Data is limited on the safety of early initiation of direct oral anticoagulation (DOAC) treatment after acute ischemic stroke (AIS) receiving reperfusion therapy in patients with atrial fibrillation (AF). We investigated the timing of DOAC initiation and its association with safety and outcomes.
We included AIS patients receiving reperfusion therapy with AF diagnosis (prevalent or new) registered in the Safe Implementation of Treatments in Stroke international registry during 2013–2024. Safety outcomes were hemorrhage and death. Secondary outcomes were recurrent AIS, any embolism and functional independence (modified Rankin Scale [mRS] 0–2) at 3 months. We performed descriptive statistics and multivariable analysis for DOAC initiation time as an ordinal variable (0–3, 4–7, and 8–100 days after stroke onset) and its association with outcomes. Explorative analyses were performed to investigate factors associated with DOAC initiation time, as a continuous or ordinal variable.
In total, 13,389 patients had data on DOAC initiation time, and 7861 patients had new event data by 3-month follow-up. We observed 0.1% intracranial hemorrhage, 0.4% major extracranial hemorrhage, 1.1% recurrent ischemic stroke, and 0.2% systemic embolism. At 3 months, 4.8% patients had died, and functional independence was seen in 60.9%. In multivariable analyses, DOAC initiation after stroke onset was not associated with any outcomes. Higher 24 h NIHSS and lower pre-stroke mRS score were associated with delayed DOAC initiation.
DOAC initiation time was not associated with any outcomes in AIS patients who received reperfusion therapy. Severe stroke symptoms at 24 h were associated with delayed DOAC initiation. The low incidence of safety outcomes and missing data in this study should lead to cautious interpretations of these results.

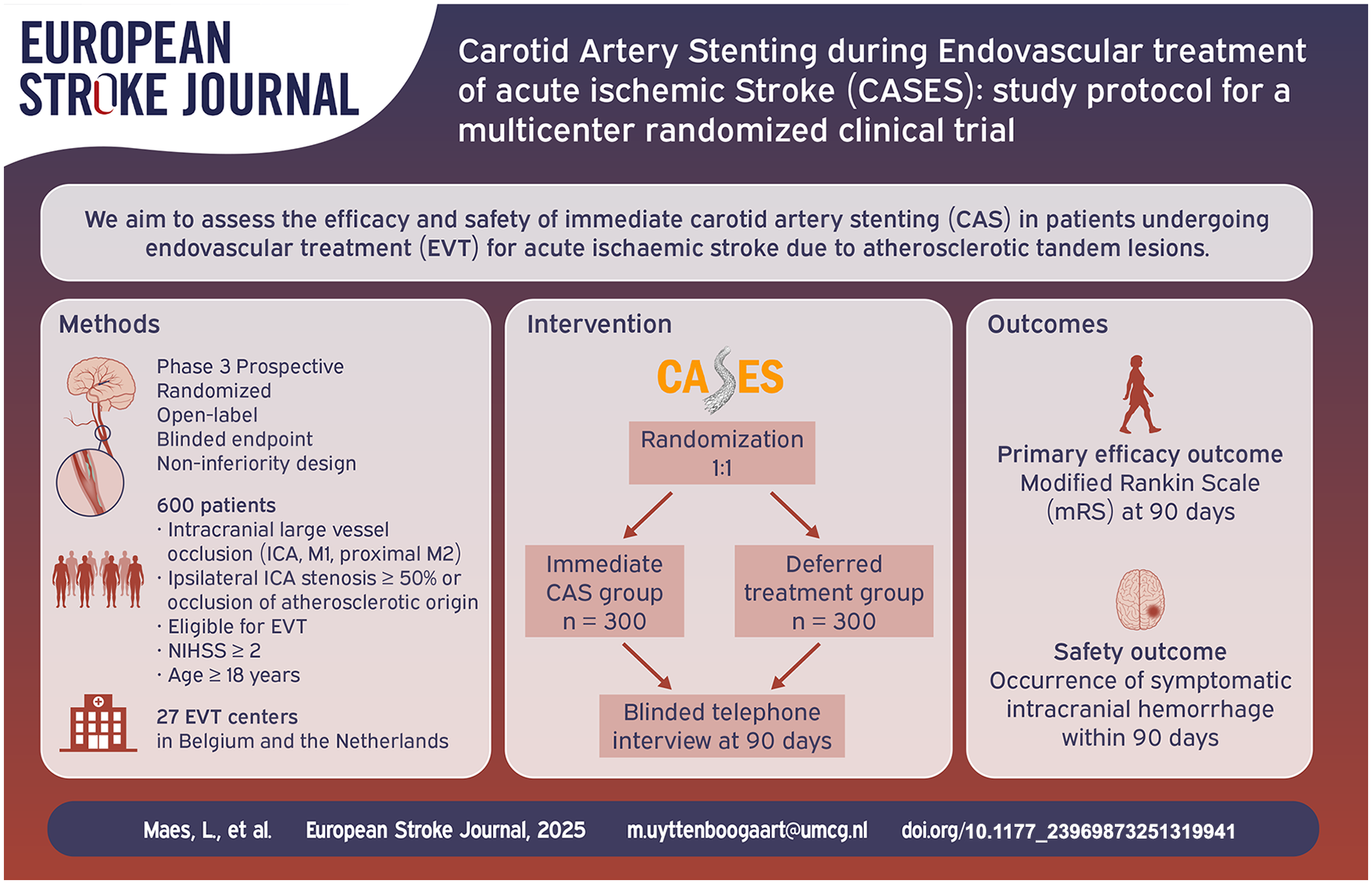
The optimal acute management of patients with acute ischemic stroke and a tandem lesion, defined as intracranial large vessel occlusion (LVO) with concomitant carotid artery stenosis or occlusion, remains unclear. Our aim is to assess the efficacy and safety of immediate carotid artery stenting (CAS) compared to delayed management in patients undergoing endovascular treatment (EVT) for acute ischemic stroke due to tandem lesions.
CASES is a phase 3 multicenter prospective randomized open-label blinded endpoint (PROBE) non-inferiority clinical trial. Patients with a computed tomography angiography proven intracranial LVO in the anterior circulation and ipsilateral proximal carotid artery stenosis (⩾50%) or occlusion of presumed atherosclerotic origin will be randomized to either immediate CAS during EVT or to EVT followed by a deferred strategy, which may include carotid endarterectomy (CEA), CAS, or medical management. CASES will be conducted in 27 EVT centers in Belgium and the Netherlands. A total of 600 patients will be included.
The primary outcome is the score on the modified Rankin Scale (mRS) at 90 days. Secondary outcomes include excellent (mRS 0–1) and good (mRS 0–2) functional outcome at 90 days, stroke severity measured with the National Institutes of Health Stroke Scale (NIHSS) at 24 h and 5–7 days, recanalization, infarct volume at 24 h, ischemic stroke recurrence, carotid artery re-occlusion, symptomatic intracranial hemorrhage, and mortality.
This study will provide high-quality randomized data on the efficacy and safety of immediate CAS in patients undergoing EVT for acute ischemic stroke due to a tandem lesion.
ClinicalTrials.gov NCT06511089; ISRCTN 14956654
This is a visual representation of the abstract.