
Editorial
Select search scope: search across all journals or within the current journal
We performed a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the efficacy and safety of direct oral anticoagulation (DOAC) compared with antiplatelet therapy for secondary stroke prevention in adult patients with embolic stroke of undetermined source (ESUS).
We searched major databases (Embase, MEDLINE, CINAHL, CENTRAL, and Web of Science) for RCTs published until March 2021. The primary outcome was recurrent stroke, and the main safety outcomes were major bleeding and clinically relevant non-major bleeding (CRNB). We assessed risk of bias using the Cochrane Risk of Bias tool. We used a random-effects model to determine pooled risk ratios and 95% confidence intervals in the datasets and key subgroups.
Our search identified two RCTs, involving a total of 12,603 patients with ESUS. Anticoagulation with dabigatran or rivaroxaban compared with aspirin did not reduce the risk of recurrent stroke (RR, 0.96 [0.76–1.20]) or increase major bleeding (RR, 1.77 [0.80–3.89]) but significantly increased the composite of major or clinically relevant non-major bleeding (RR, 1.57 [1.26–1.97]). Prespecified subgroup analysis demonstrated consistent results according to age and sex. Additional post-hoc subgroup analyses demonstrated consistent results according to prior stroke and presence of a patent foramen ovale but suggested that DOACs reduced recurrent stroke in patients with an estimated glomerular filtration rate (eGFR) <50 and 50-80 ml/min but not in those with eGFR >80 ml/min (interaction
Direct oral anticoagulations are not more effective than aspirin in preventing stroke recurrence in patients with ESUS and increase bleeding.
PROSPERO ID: CRD42019138593
Low blood pressure (BP) in acute ischaemic stroke (AIS) is associated with poor functional outcome, death, or severe disability. Increasing BP might benefit patients with post-stroke hypotension including those with potentially salvageable ischaemic penumbra. This updated systematic review considers the present evidence regarding the use of vasopressors in AIS.
We searched the Cochrane Database of Systematic Reviews, MEDLINE, EMBASE and trial databases using a structured search strategy. We examined reference lists of relevant publications for additional studies examining BP elevation in AIS.
We included 27 studies involving 1886 patients. Nine studies assessed increasing BP during acute reperfusion therapy (intravenous thrombolysis, mechanical thrombectomy, intra-arterial thrombolysis or combined). Eighteen studies tested BP elevation alone. Phenylephrine was the most commonly used agent to increase BP (n = 16 studies), followed by norepinephrine (n = 6), epinephrine (n = 3) and dopamine (n = 2). Because of small patient numbers and study heterogeneity, a meta-analysis was not possible. Overall, BP elevation was feasible in patients with fluctuating or worsening neurological symptoms, large vessel occlusion with labile BP, sustained post-stroke hypotension and ineligible for intravenous thrombolysis or after acute reperfusion therapy. The effects on functional outcomes were largely unknown and close monitoring is advised if such intervention is undertaken.
Although theoretical arguments support increasing BP to improve cerebral blood flow and sustain the ischaemic penumbra in selected AIS patients, the data are limited and results largely inconclusive. Large, randomised controlled trials are needed to identify the optimal BP target, agent, duration of treatment and effects on clinical outcomes.
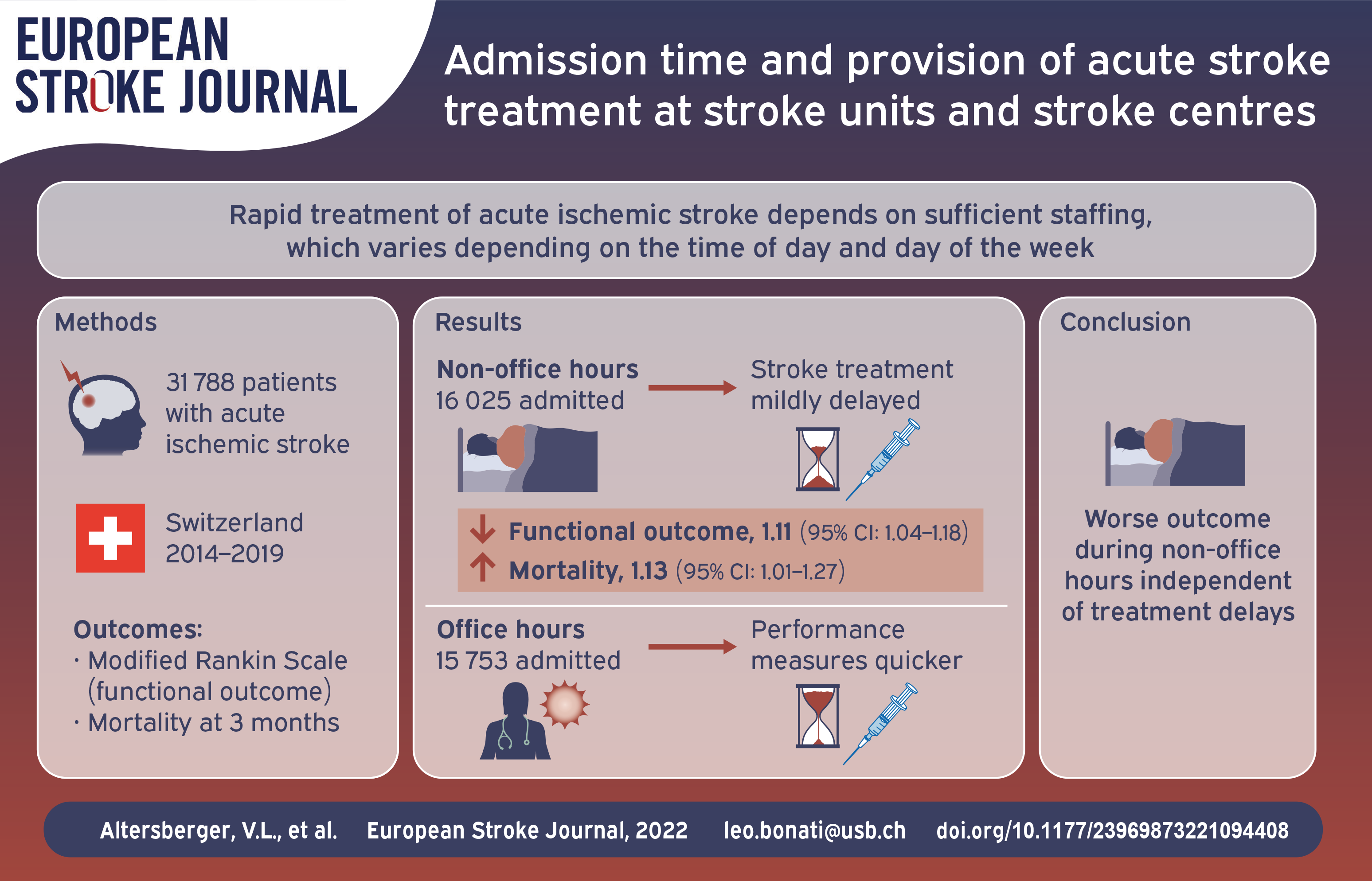
Rapid treatment of acute ischemic stroke (AIS) depends on sufficient staffing which differs between Stroke Centers and Stroke Units in Switzerland. We studied the effect of admission time on performance measures of AIS treatment and related temporal trends over time.
We compared treatment rates, door-to-image-time, door-to-needle-time, and door-to-groin-puncture-time in stroke patients admitted during office hours (Monday–Friday 8:00–17:59) and non-office hours at all certified Stroke Centers and Stroke Units in Switzerland, as well as secular trends thereof between 2014 and 2019, using data from the Swiss Stroke Registry. Secondary outcomes were modified Rankin Scale and mortality at 3 months.
Data were eligible for analysis in 31,788 (90.2%) of 35,261 patients. Treatment rates for IVT/EVT were higher during non-office hours compared with office hours in Stroke Centers (40.8 vs 36.5%) and Stroke Units (21.8 vs 18.5%). Door-to-image-time and door-to-needle-time increased significantly during non-office hours. Median (IQR) door-to-groin-puncture-time at Stroke Centers was longer during non-office hours compared to office hours (84 (59–116) vs 95 (66–130) minutes). Admission during non-office hours was independently associated with worse functional outcome (1.11 [95%CI: 1.04–1.18]) and increased mortality (1.13 [95%CI: 1.01–1.27]). From 2014 to 2019, median door-to-groin-puncture-time improved and the treatment rate for wake-up strokes increased.
Despite differences in staffing, patient admission during non-office hours delayed IVT to a similar, modest degree at Stroke Centers and Stroke Units. A larger delay of EVT was observed during non-office hours, but Stroke Centers sped up delivery of EVT over time. Patients admitted during non-office hours had worse functional outcomes, which was not explained by treatment delays.
The Stockholm Stroke Triage System (SSTS) is a prehospital triage system for detection of patients eligible for endovascular thrombectomy (EVT). Assessment of hemiparesis combined with ambulance-hospital teleconsultation is used to route patients directly to the thrombectomy centre. Some patients are not identified and require secondary transport for EVT (undertriage) while others taken to the thrombectomy centre do not undergo EVT (overtriage). The aims of this study were to characterize mistriaged patients, model for and evaluate alternative triage algorithms.
Patients with suspected stroke transported by priority 1 ground ambulance between October 2017 and October 2018 (n = 2905) were included. Three triage algorithms were modelled using prehospital data. Decision curve analysis was performed to calculate net benefit (correctly routing patients for EVT without increasing mistriage) of alternative models vs SSTS.
Undertriage for EVT occurred in n = 35/2582 (1.4%) and overtriage in n = 239/323 (74.0%). Compared to correct thrombectomy triages, undertriaged patients were younger and had lower median NIHSS (10 vs 18), despite 62.9% with an M1 occlusion. In overtriaged patients, 77.0% had a stroke diagnosis (29.7% haemorrhagic). Hemiparesis and FAST items
Undertriaged patients had lower NIHSS, likely due to better compensated proximal occlusions. SSTS was superior to other models for identifying EVT candidates, but lacked information allowing comparison to other prehospital scales.
Using prehospital data, alternative models did not outperform the SSTS in finding EVT candidates.
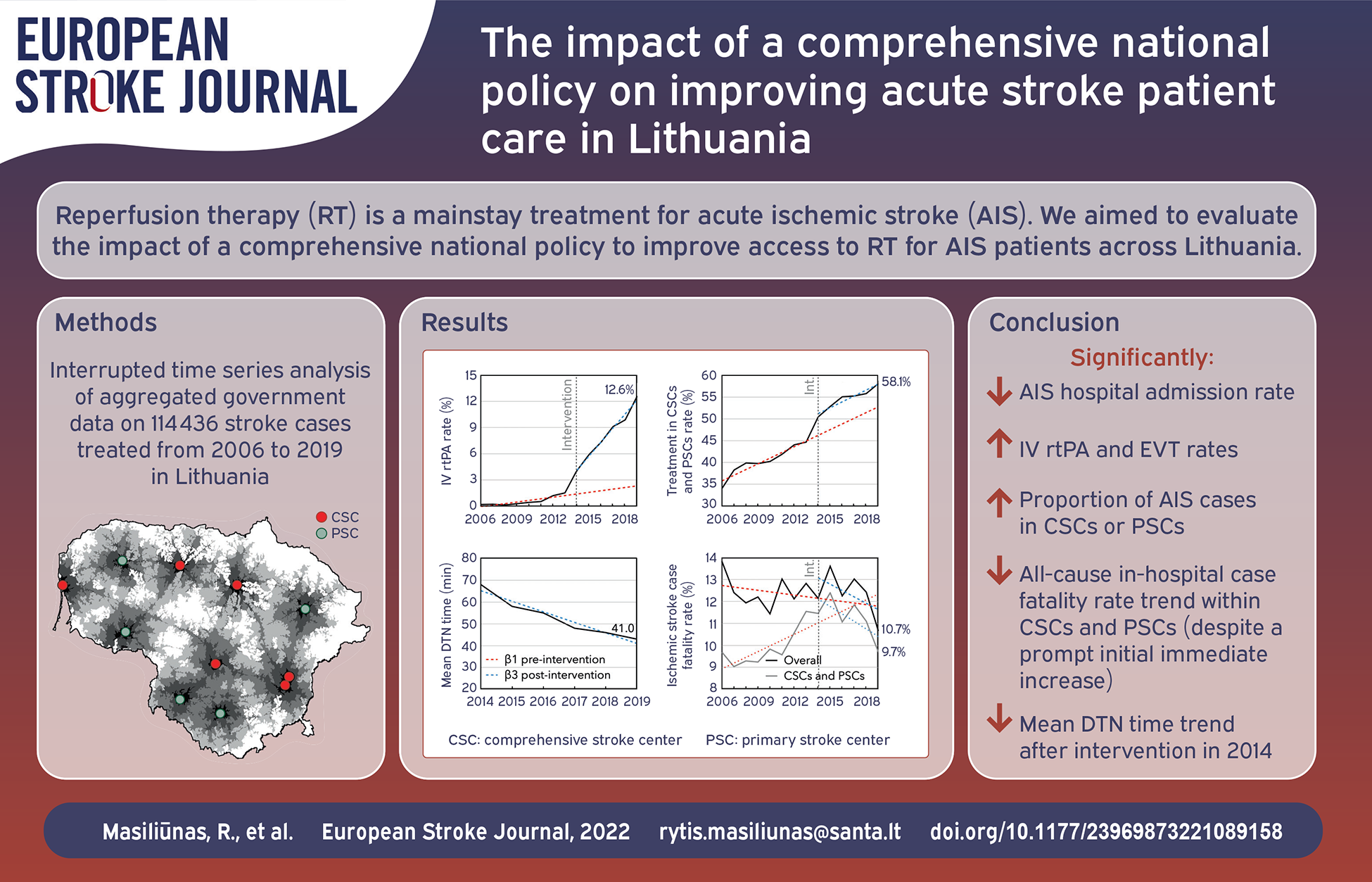
Reperfusion therapy (RT) is a mainstay treatment for acute ischemic stroke (AIS). We aimed to evaluate the impact of a comprehensive national policy (CNP) to improve access to RT for AIS patients across Lithuania.
Aggregated anonymized data on AIS cases treated in Lithuanian hospitals between 2006 and 2019 were retrospectively obtained from the Institute of Hygiene and the Stroke Integrated Care Management Committee. Through an interrupted time series analysis, we examined the trends in AIS hospital admissions, RT, and in-hospital case fatality rates prior to the enactment of CNP in 2014, changes immediately after the intervention, and differences in trends between the pre- and post-intervention periods. Mean yearly door-to-needle times were calculated post-intervention.
114,436 cases were treated for AIS in Lithuanian hospitals before, and 65,084 after the government intervention. We observed a significant decreasing post-intervention trend change in AIS hospital admission rate per 100,000 population (regression coefficient ± standard error: β = –16.47 ± 3.95,
The comprehensive national stroke patient care policy could be associated with an immediate increase in stroke center treatment rate, increased access to RT, and improved stroke care performance measures.
Population-based knowledge of the characteristics of wake-up stroke and unknown-onset stroke is limited. We compared occurrence and characteristics of ischaemic and haemorrhagic wake-up stroke, unknown-onset stroke and known-onset stroke in a nationwide register-based study.
We included patients registered in the Norwegian Stroke Register from 2012 through 2019. Age, sex, risk factors, clinical characteristics, acute stroke treatment and discharge destination were compared according to stroke type and time of onset.
Of the 60,320 patients included, 11,451 (19%) had wake-up stroke, 11,098 (18.4%) had unknown time of onset and 37,771 (62.6%) had known symptom onset. The proportion of haemorrhagic stroke was lower among wake-up stroke patients (1107/11,451, 9.7%, 95% CI: 9.1–10.2) than for known-onset stroke (5230/37,771, 13.8%, 95% CI: 13.5–14.2) and for unknown-onset stroke (1850/11,098, 16.7%, 95% CI: 16.0–17.4). Mild stroke (NIHSS <5) was more frequent in ischaemic wake-up stroke (5364/8308, 64.6%, 95% CI: 63.5–65.5) than in known-onset (16,417/26,746, 61.4%, 95% CI: 60.8–62.0) and unknown-onset stroke (3242/5853, 55.4%, 95% CI: 54.1–56.7), while baseline characteristics were otherwise similar to known-onset stroke. Unknown-onset stroke patients were more often female, lived alone and had more severe strokes compared to wake-up stroke and known-onset stroke patients. Unknown-onset stroke patients were more often in need of community-based health care on discharge and had a higher in-hospital mortality.
Ischaemic wake-up strokes shared baseline characteristics with known-onset strokes, but tended to be milder. Ischaemic unknown-onset stroke patients differed significantly from wake-up stroke, emphasising the importance of considering them as separate entities.
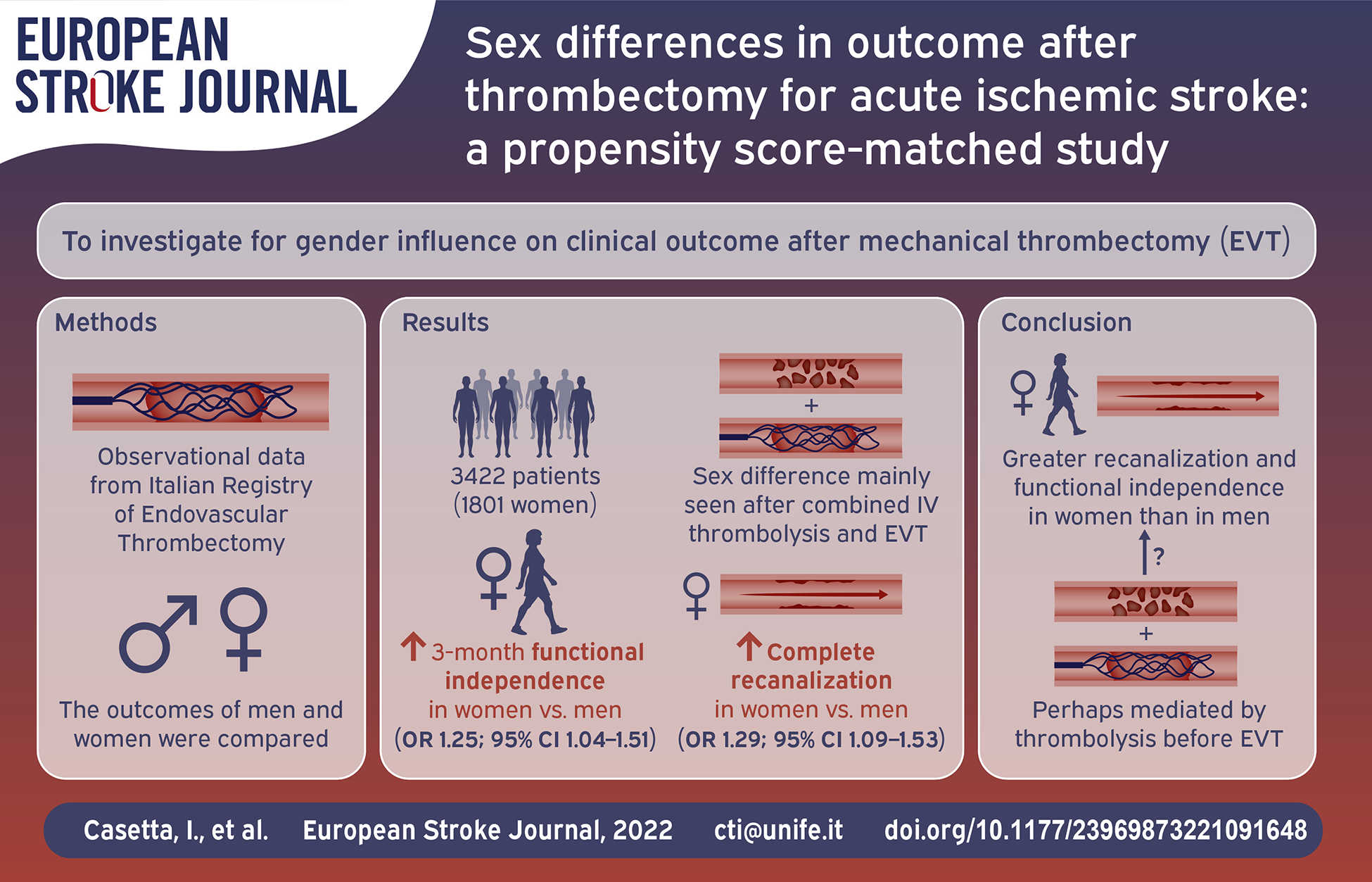
We sought to investigate whether there are gender differences in clinical outcome after stroke due to large vessel occlusion (LVO) after mechanical thrombectomy (EVT) in a large population of real-world patients.
From the Italian Registry of Endovascular Thrombectomy, we extracted clinical and outcome data of patients treated for stroke due to large vessel occlusion. We compared clinical and safety outcomes in men and women who underwent EVT alone or in combination with intravenous thrombolysis (IVT) in the total population and in a Propensity Score matched set.
Among 3422 patients included in the study, 1801 (52.6%) were women. Despite older age at onset (mean 72.4 vs 68.7;
Subject to the limitations of a non-randomized comparison, women with stroke due to LVO treated with mechanical thrombectomy had a better chance to achieve complete recanalization, and 3-month functional independence than men. The results could be driven by women who underwent combined treatment.
We investigated 92 blood biomarkers implicated in the pathophysiological pathways of ischemic injury, inflammation, hemostasis, and regulation of vascular resistance to predict post-stroke mortality.
Based on the most promising markers, we aimed to create a novel Biomarker Panel Index (BPI) for risk stratification.
In this prospective study, we measured 92 biomarkers in 320 stroke patients. The primary outcome measure was mortality within 90 days. We estimated the association of each biomarker using logistic regression adjusting for multiple testing. The most significant 16 biomarkers were used to create the BPI. We fitted regression models to estimate the association and the discriminatory accuracy of the BPI with mortality and stroke etiology.
Adjusted for demographic and vascular covariates, the BPI remained independently associated with mortality (odds ratio (OR) 1.68, 95% confidence interval (CI): 1.29–2.18) and cardioembolic stroke etiology (OR 1.38, 95% CI: 1.10–1.74), and improved the discriminatory accuracy to predict mortality (area under the receiver operating characteristic curve (AUC) 0.93, 95% CI: 0.89–0.96) and cardioembolic stroke etiology (AUC 0.70, 95% CI: 0.64–0.77) as compared to the best clinical prediction models alone (AUC 0.89, 95% CI: 0.84–0.94 and AUC 0.66, 95% CI: 0.60-0.73, respectively).
We identified a novel BPI improving risk stratification for mortality after ischemic stroke beyond established demographic and vascular risk factors. Furthermore, the BPI is associated with underlying cardioembolic stroke etiology. These results need external validation.
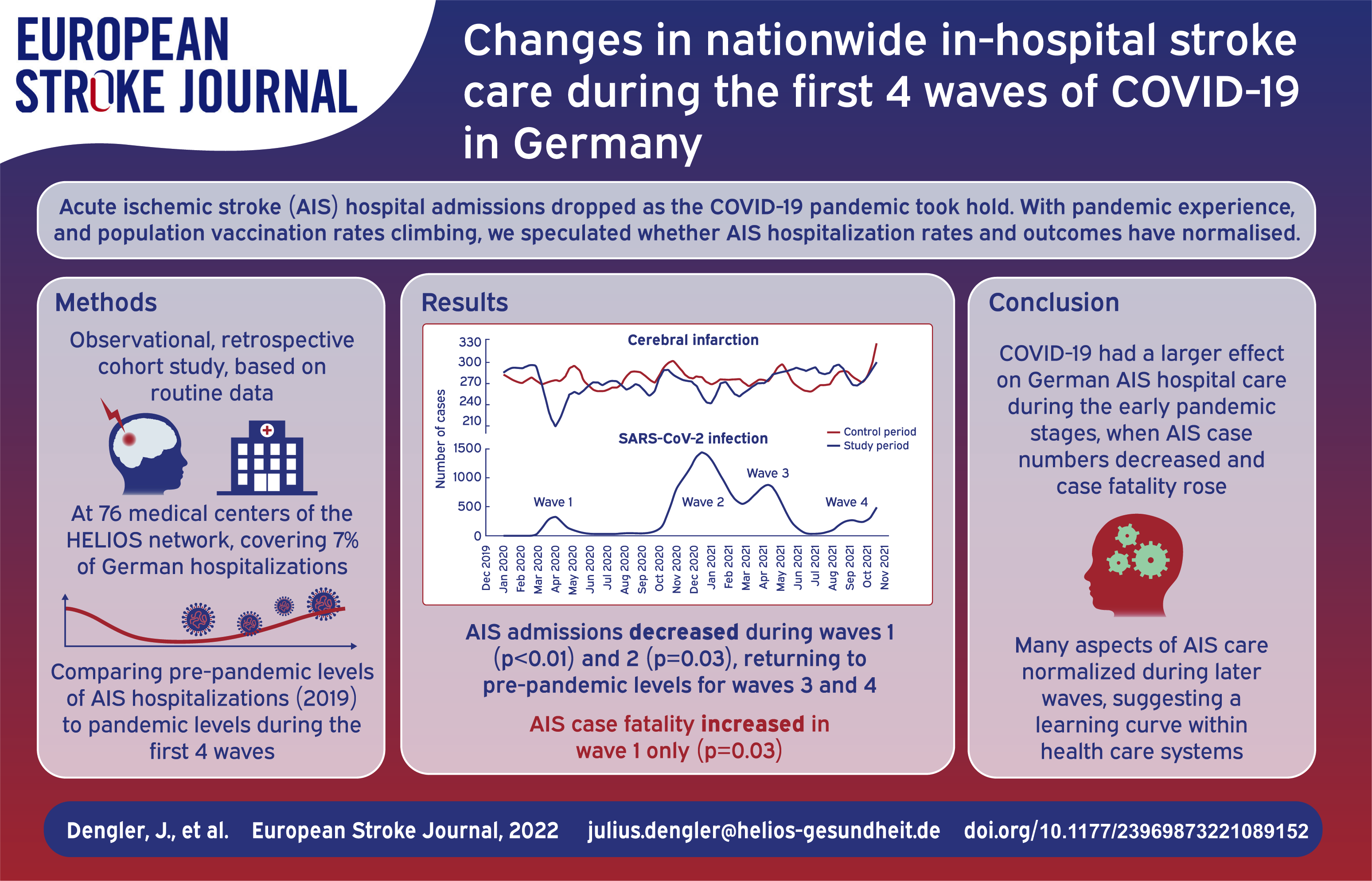
In the early stages of the global COVID-19 pandemic hospital admissions for acute ischemic stroke (AIS) decreased substantially. As health systems have become more experienced in dealing with the pandemic, and as the proportion of the population vaccinated rises, it is of interest to determine whether the prevalence of AIS hospitalization and outcomes from hospitalization have returned to normal.
In this observational, retrospective cohort study, we compared the prevalence and outcomes of AIS during the first four waves of the pandemic to corresponding pre-pandemic periods in 2019 using administrative data collected from a nationwide network of 76 hospitals that manages 7% of all in-hospital cases in Germany.
We included 25,821 AIS cases in the study period (2020/2021) and used 26,295 AIS cases as controls (2019). Compared to pre-pandemic numbers, mean daily AIS admissions decreased only during wave 1 (from 39.6 to 34.1; p < 0.01) and wave 2 (from 39.9 to 38.3; p = 0.03) and returned to normal levels during waves 3 and 4. AIS case fatality increased in wave 1 only (from 6.0% to 7.6%; p = 0.03). We observed a consistent decrease in the prevalences of arterial hypertension, diabetes, and obesity among AIS cases throughout the pandemic and no changes in rates of systemic thrombolysis, mechanical thrombectomy, or decompressive craniectomy. The rate of transfer to stroke units increased only during waves 2 (by 4.6%; p < 0.01) and 3 (by 3.0%; p < 0.01). The proportion of patients with coinciding SARS-CoV-2 and AIS was low, peaking at 3.4% in wave 2 and subsequently decreasing to 0.4% in wave 4.
In Germany, the COVID-19 pandemic seems to have had a larger effect on nationwide in-hospital AIS care during the early pandemic stages, in which AIS case numbers decreased and case fatality rose. This may reflect a nationwide “learning curve” within health care systems in providing AIS care in times of a pandemic.
The aim of our study was to determine whether the severity of the COVID-19 pandemic affected the quality of acute care of stroke.
Data from the stroke register at the National Health Information Centre were analysed. Clinical data from two time periods (the first wave: March–April 2020; the second wave: October–November 2020) were compared using an independent sample
The total number of patients admitted with stroke during the second wave of COVID-19 was 1848, versus 1698 in the first wave. The proportion of patients treated by IVT was similar in both waves (275 (20.7%) vs 333 (22.1%),
The severity of the COVID-19 outbreak did not affect the quality of acute stroke care in Slovakia.
COVID-19 is often complicated by thrombo-embolic events including ischemic stroke. The underlying mechanisms of COVID-19-associated ischemic stroke, the incidence and risk factors of silent cerebral ischemia, and the long-term functional outcome in these patients are currently unknown.
CORONavirus and Ischemic Stroke (CORONIS) is a multicentre prospective cohort study investigating the prevalence, risk factors and long-term incidence of (silent) cerebral ischemia, and the long-term functional outcome among patients with COVID-19. We aim to include 200 adult patients hospitalized with COVID-19 without symptomatic ischemic stroke to investigate the prevalence of silent cerebral ischemia compared with 60 (matched) controls with MRI. In addition, we will identify potential risk factors and/or causes of cerebral ischemia in COVID-19 patients with (
The CORONIS study is designed to add further insight into the prevalence, long-term incidence and risk factors of cerebral ischemia, and the long-term functional outcome in hospitalized adult patients with COVID-19.
Computed tomography perfusion (CTP) is variably considered to assess eligibility for endovascular thrombectomy (EVT) in acute ischemic (AIS) stroke patients. Although CTP is recommended for patient selection in later (6–24 h) time window, it is currently not recommended in the earlier (0–6 h) time window and the costs and health effects of including CTP for EVT selection remain unknown. We aim to estimate the costs and health effects of using CTP for EVT selection in AIS patients compared to conventional selection.
CLEOPATRA is a healthcare evaluation study using clinical and imaging data from multiple, prospective EVT trials and registries in both the earlier and later time windows. To study the long-term health and cost effects, we will construct a (“Markov”) health state transition model simulating the clinical outcome over a 5-year follow-up period for CTP-based and conventional selection for EVT. Clinical data acquired within the current study and estimates from the literature will be used as input for probabilities of events, costs, and Quality-Adjusted Life Years (QALYs) per modified Rankin Scale (mRS) subscore. Primary outcome for the cost-effectiveness analysis will be the Incremental Cost-Effectiveness Ratio (ICER) in terms of costs per QALY gained over the simulated follow-up period.
Outcome measures will be reported as cumulative values over a 5-year follow-up period.
This study will provide preliminary insight into costs and health effects of including CTP in the selection for EVT for AIS patients, presenting between 0 and 24 h after time last known well. The results may be used to develop recommendations and inform further implementation projects and studies.
Pregnancy, postpartum and menopause are regarded as periods women are more vulnerable to ischaemic events. There are conflicting results regarding stroke risk and hormone replacement therapy (HRT) during menopause. Stroke in pregnancy is generally increasing with serious consequences for mother and child; therefore, recommendations for acute treatment with intravenous thrombolysis (IVT) and/or mechanical thrombectomy (MT) are needed. The aim of this guideline is to support and guide clinicians in treatment decisions in stroke in women. Following the “Grading of Recommendations and Assessment, Development and Evaluation (GRADE)” approach, the guidelines were developed according to the European Stroke Organisation (ESO) Standard Operating Procedure. Systematic reviews and metanalyses were performed. Based on available evidence, recommendations were provided. Where there was a lack of evidence, an expert consensus statement was given. Low quality of evidence was found to suggest against the use of HRT to reduce the risk of stroke (ischaemic and haemorrhagic) in postmenopausal women. No data was available on the outcome of women with stroke when treated with HRT. No sufficient evidence was found to provide recommendations for treatment with IVT or MT during pregnancy, postpartum and menstruation. The majority of members suggested that pregnant women can be treated with IVT after assessing the benefit/risk profile on an individual basis, all members suggested treatment with IVT during postpartum and menstruation. All members suggested treatment with MT during pregnancy. The guidelines highlight the need to identify evidence for stroke prevention and acute treatment in women in more vulnerable periods of their lifetime to generate reliable data for future guidelines.